
Real-world PD-L1 testing, fi rst-line therapy for advanced NSCLC, and fi rst-line pembrolizumab monotherapy utilization and outcomes for metastatic NSCLC in the Czech Republic
Testování PD-L1 v reálné praxi, první linie léčby pokročilého NSCLC a výsledky a využití první linie léčby metastatického NSCLC pembrolizumabem v monoterapii v České republice
Východiska: Cílem této studie bylo popsat testování PD-L1 a schéma léčby první linie (1L) u pokročilého nemalobuněčného karcinomu plic (non-small cell lung cancer – NSCLC) a klinické výsledky u metastatického NSCLC v reálné praxi po zavedení úhrady monoterapie pembrolizumabem v České republice (únor 2019). Pacienti a metody: Tato deskriptivní neintervenční studie čerpala z dvou českých registrů plicních nádorů. Zkoumali jsme schéma testování PD-L1 a výsledky v registru KELLY u vzorků od dospělých pacientů s pokročilým NSCLC odeslaných 1. února 2019 nebo později. Pomocí registru TULUNG jsme shrnuli výsledky cílené léčby první linie u pokročilého NSCLC zahájené 1. února 2019 nebo později, kromě charakteristik a výsledků u pacientů léčených v první linii pembrolizumabem v monoterapii pro metastatický NSCLC se skóre nádorového podílu (tumor proportion score – TPS) ≥ 50 % a bez známých alterací EGFR/ALK. Skutečná doba léčby (real-world time on treatment – rwToT) a celkové přežití (overal survival – OS) byly stanoveny pomocí Kaplan-Meierovy metody. Data byla shromážděna k 16. září 2021. Výsledky: Procento vzorků NSCLC v registru KELLY testovaných na expresi PD-L1 se zvýšilo ze 70,5 % v roce 2019 na 84,4 % v roce 2021. U pacientů s pokročilým NSCLC a PD-L1 TPS ≥ 50 % (n = 315) byla v letech 2019–2021 nejčastější cílenou léčbou první linie monoterapie pembrolizumabem, podávaná každoročně 70–80 % pacientů. Z 235 pacientů s metastatickým NSCLC, kteří byli v první linii léčeni pembrolizumabem v monoterapii, byl medián věku 69 let, 54 % byli muži, 52 % byli aktuální kuřáci a 28 % mělo skvamózní NSCLC. Medián rwToT byl 8,5 měsíce (95% CI 6,7–10,1), přičemž OS po 6 a 12 měsících léčby u 199 pacientů bylo 59 % a 36 % při ≥ 6 měsících sledování. Po přidání údajů o úmrtnosti z národního registru byl odhadovaný medián OS 13,7 měsíce (12,3–17,7); po 6 a 12 měsících byla míra OS 70% a 59 %. Závěry: Míra testování PD-L1 se v letech 2019–2021 zvýšila. Medián OS u pacientů s metastatickým NSCLC a PD-L1 TPS ≥ 50 % léčených pembrolizumabem byl nižší než v klinických studiích, pravděpodobně kvůli rozdílům mezi pacienty v reálné praxi a účastníky studií, a to z hlediska věku, kouření, výkonnostním stavu a skvamózní histologie.
Klíčová slova:
Česká republika – karcinom plic – imunoterapie – monoterapie – pembrolizumab – nemalobuněčný – ligand programované buněčné smrti 1 – data z reálné praxe
Authors:
M. L. Santorelli 1; M. Chrápavá 2; K. Hrabcová 2; G. Bencina 3; J. Blažek 4; M. Bratová 5; O. Fibigr 6; #; O. Fischer 7; L. Koubková 8; J. Krejčí 9; A. Ryška 10; P. Zemanová 11; T. Burke 12
Authors place of work:
Value & Implementation Outcomes Research, Oncology, Merck & Co., Inc., 126 East Lincoln Ave., Rahway, NJ 07065, USA
1; Institute of Biostatistics and Analyses, Czech Republic, ¨
2; Value & Implementation Outcomes Research, MSD, Madrid, Spain
3; Department of Pneumology and Phthisiology, University Hospital Plzen, Medical Faculty in Pilsen, Charles University in Prague, Prague, Czech Republic
4; Clinic of Pulmonary Dis eases and Tuberculosis, University Hospital Brno, Czech Republic
5; Pulmonology Department, Masaryk Hospital in Ústí nad Labem, Czech Republic
6; Department of Pulmonary Dis eases and Tuberculosis, University Hospital Olomouc, Czech Republic
7; Department of Pulmonology, 2nd Faculty of Medicine, Charles University and University Hospital, Motol, Prague, Czech Republic
8; Pulmonology Clinic, Na Bulovce Hospital, Prague, Czech Republic
9; The Fingerland Department of Pathology, University Hospital Hradec Králové, and Charles University Medical Faculty, Hradec Králové, Czech Republic
10; Department of Oncology, General University Hospital in Prague, Czech Republic
11; Outcomes Research, Merck Research Labs, Merck & Co. Inc., USA, # Current affi liation for Ondřej Fibigr is Department of Pneumology and Phthisiology, University, Hospital Plzeň, Medical Faculty in Pilsen, Pilsen, Czech Republic
12
Published in the journal:
Klin Onkol 2025; 38(3): 192-200
Category:
Původní práce
doi:
https://doi.org/10.48095/ccko2025192
Summary
Background: This study aimed to describe real-world PD-L1 testing and first-line (1L) treatment patterns for advanced non-small cell lung cancer (NSCLC), and clinical outcomes for metastatic NSCLC after 1L pembrolizumab monotherapy became reimbursed in the Czech Republic (February 2019). Patients and methods: This descriptive noninterventional study drew on two Czech lung cancer registries. We examined PD-L1 testing patterns and results in the KELLY registry for samples submitted on/after 1-Feb-2019 from adult patients with advanced NSCLC. Using the TULUNG registry, we summarized 1L targeted therapies initiated on/after 1-Feb-2019 for advanced NSCLC, in addition to characteristics and outcomes for patients treated with 1L pembrolizumab monotherapy for metastatic NSCLC, PD-L1 tumor proportion score (TPS) ≥ 50%, and no known EGFR/ALK alterations. Real-world time on treatment (rwToT) and overall survival (OS) were determined using Kaplan-Meier curves. The data cutoff was 16-Sept-2021. Results: The percentage of NSCLC samples in the KELLY registry tested for PD-L1 expression increased from 70.5% in 2019 to 84.4% in 2021. Pembrolizumab monotherapy was the most common 1L targeted therapy in 2019–2021 for patients with advanced NSCLC and PD-L1 TPS ≥ 50% (N = 315), administered to 70–80% each year. Of 235 patients with metastatic NSCLC who received 1L pembrolizumab monotherapy, median age was 69 years, 54% were men, 52% were current smokers, and 28% had squamous NSCLC. Median rwToT was 8.5 months (95% CI; 6.7–10.1), with 6 - and 12-month on-treatment rates of 59% and 36%, respectively, for 199 patients with ≥ 6 months of follow-up. With added national registry mortality data, estimated median OS was 13.7 months (12.3–17.7); 6 - and 12-month OS rates were 70% and 59%, respectively. Conclusions: The rates of PD-L1 testing increased from 2019 to 2021. Median OS among patients with metastatic NSCLC and PD-L1 TPS ≥ 50% treated with pembrolizumab was lower than in clinical trials, likely due to differences between real-world patients and trial participants in age, smoking status, performance status, and squamous histology.
Keywords:
immunotherapy – Czech Republic – programmed death-ligand 1 – carcinoma – real-world data – non-small-cell lung – pembrolizumab monotherapy
Introduction
Lung cancer continues to be the most common cause of cancer death globally. Non-small cell lung cancer (NSCLC) accounts for about 80–85% of all lung cancers and has a 28% 5-year relative survival rate [1]. The age-standardized death rate for lung cancer is the highest in Europe compared with other continents, estimated in 2022 as 21.4 per 100,000 standard population, and varying widely by country. In the Czech Republic (Czechia), a central European country, the rate is 19.8, similar to the surrounding countries, namely, Austria (19.5), Germany (21.4), and Slovakia (19.3), and lower than in Poland (30.5) [2].
The diagnosis of NSCLC is most common at an unresectable advanced or metastatic stage of disease when the 5-year relative survival rate is only 9% [1]. The European Society of Medical Oncology (ESMO) clinical practice guidelines for metastatic NSCLC provide targeted treatment algorithms for patients with specific molecular alterations, such as ALK, ROS1, or EGFR genomic alterations [3,4]. For patients with NSCLC without these alterations, the standard of care was platinum-based therapy until the treatment landscape shifted after the authorization of first-line (1L) immunotherapy for patients with metastatic NSCLC and programmed death-ligand 1 (PD-L1) tumor proportion score (TPS) ≥ 50% [4]. In 2016, results of the KEYNOTE-024 study, a randomized phase III trial investigating pembrolizumab monotherapy vs. platinum-based doublet chemotherapy regimens in patients with previously untreated metastatic NSCLC whose tumors expressed PD-L1 TPS ≥ 50% without EGFR/ALK alterations, showed pembrolizumab was superior to platinum chemotherapy for both the primary endpoint of progression-free survival and the secondary endpoint of overall survival (OS) [5]. On the basis of results from this trial, pembrolizumab became the first immunotherapy approved by the European Medicines Agency (EMA) in January 2017 for the 1L treatment of metastatic NSCLC with PD-L1 TPS ≥ 50% and no EGFR mutations or ALK translocations [6]. Subsequently, the EMA approved pembrolizumab in combination with chemotherapy as 1L treatment for metastatic nonsquamous (September 2018) and squamous (March 2019) NSCLC, independent of PD-L1 expression [7,8].
In most European countries, patients with NSCLC were able to access pembrolizumab in 2017–2018. Accessibility was suboptimal in Central and Eastern European countries where initial access to pembrolizumab spanned from 2019 to 2020 [9]. In the Czech Republic, eligible patients with NSCLC continued receiving platinum doublet therapy until pembrolizumab became accessible via public insurance reimbursement in 2019. For nonsquamous NSCLC in patients with PD-L1 TPS ≥ 50%, pembrolizumab was reimbursed in the 1L setting in combination with pemetrexed and platinum chemotherapy in March 2021.
Observational studies can complement findings from clinical trials by describing the implementation and effectiveness of new treatments once they become accessible to patients in real-world clinical settings. Real-world patient populations are more heterogeneous and often differ from clinical trial populations in terms of prognostic patient and clinical characteristics. The need for real-world observational research is especially relevant in Europe where the lung cancer survival rate shows high variation. Several data-rich registries are maintained for Czech patients with cancer. The TULUNG and KELLY registries are unique data sources providing the opportunity to study biomarker testing, treatment patterns, and associated clinical outcomes in routine clinical practice in central Europe [10,11].
This study aimed to describe real-world PD-L1 testing, treatment patterns, and clinical outcomes in patients with advanced NSCLC or metastatic NSCLC and PD-L1 TPS ≥ 50% without EGFR or ALK genomic alterations after 1L pembrolizumab monotherapy became reimbursed in the Czech Republic in February 2019.
Patients and methods
Data sources
This was a descriptive noninterventional study using the KELLY and TULUNG cancer registries in the Czech Republic [10–12]. Retrospective analysis of each registry database was conducted independently. No primary data collection, testing, or evaluations were performed in conjunction with the study.
Both TULUNG and KELLY registries are managed and rigorously monitored by the Institute of Biostatistics and Analyses (IBA), a spin-off company of Masaryk University that provides management, monitoring, and other services to the registries [13]. In this study, we used the KELLY registry to examine PD-L1 testing patterns from pathology records and the TULUNG registry to analyze targeted therapy utilization and pembrolizumab utilization with associated outcomes from medical records. Ethical review and approval were waived for this study because both the KELLY and TULUNG cancer registries are anonymized and operate independently without the option to merge data at the patient level.
Launched by IBA in 2014, the KELLY registry has been used as a source of anonymized data to monitor the number of Czech patients with NSCLC and their diagnostic testing [11,14]. Records include all newly diagnosed and microscopically verified NSCLC cases, histological parameters of each tumor, information about all morphological examinations, and EGFR and ALK testing performed in participating laboratories. Diagnostic data are entered in the registry once under a unique code. If a patient is re-examined, each sample is entered in the registry under a new unique code; therefore, the registry contains data at the sample level, not at the patient level. The registry is organized by type of material, i.e., small samples, small surgical specimens, and resection specimens. All small surgical and resection specimens can be tested for PD-L1 expression, whereas a small sample can be tested for PD-L1 expression only on cytoblock and biopsy.
The KELLY registry covers all laboratories authorized to perform PD-L1 immunohistochemistry (IHC) testing, as well as small laboratories that perform basic morphology and then send samples for further testing to the authorized laboratories. Since 2017, the registry has contained information on ~80% of all NSCLC samples in the Czech Republic. The PD-L1 IHC 22C3 pharmDx (Agilent Technologies, Carpinteria, CA, USA), Anti-PD-L1 antibody [28-8] (abcam, Cambridge, UK), and VENTANA PD-L1 (SP263) Assay (Roche, Basel, Switzerland) are currently used as testing assays in the Czech Republic. The assays differ in the definition of PD-L1 positivity, which depends on the cells, tissue compartments, and staining thresholds for the specific PD-L1 assay.
The TULUNG registry is a noninterventional post-registration database collecting epidemiological and clinical data of patients with NSCLC who have been treated with selected therapies, primarily targeted therapies, including immunotherapy (e. g., alectinib, afatinib, atezolizumab, bevacizumab, ceritinib, crizotinib, dabrafenib, durvalumab, erlotinib, gefitinib, lorlatinib, nintedanib, nivolumab, osimertinib, pembrolizumab, pemetrexed, and trametinib). New therapies are added after their regulatory approvals, while platinum use (carboplatin or cisplatin) and generic drug use (e. g., docetaxel generic) are not recorded in TULUNG. The database covers all centers authorized to prescribe targeted therapies, including immunotherapies, in the Czech Republic. Clinicians enter the data voluntarily; however, they are reimbursed for their efforts. The TULUNG project was initiated in July 2011 by the Czech Society for Oncology, and data from the TULUNG registry can be enriched with mortality data from the national registry of death certificates.
Patients
We identified patients with primary diagnostic samples or those who started 1L advanced or metastatic NSCLC treatment on or after February 1, 2019. Data were extracted from both registries on September 16, 2021. Since data are collected continuously in the TULUNG registry, the data collection period was from February 1, 2019, to September 16, 2021. In the KELLY registry, there is a lag of about 4 weeks between diag - nostic testing (the reported date on the request form) and data input in the registry, so the data collection period was from February 1, 2019, to approx. August 19, 2021.
Three adult patient populations were included in this study to meet the three study aims, namely: (1) to describe PD-L1 testing patterns using the KELLY registry; (2) to describe therapy for advanced NSCLC as recorded in the TULUNG registry; and (3) to evaluate 1L pembrolizumab monotherapy utilization and outcomes for patients with metastatic NSCLC, using the TULUNG registry.
PD-L1 testing patterns: KELLY registry
We included sample results from patients aged 18 years and older at the time of advanced NSCLC diagnosis, with histologically or cytologically confirmed diagnosis derived from the submitted sample and the primary diagnostic testing for NSCLC initiated on or after February 1, 2019, as recorded in the KELLY registry. Data from surgical resection specimens were excluded.
Therapy for advanced NSCLC: TULUNG registry
Patients eligible for descriptive analyses of targeted therapy including immunotherapy were ≥18 years old at the time of advanced NSCLC diagnosis, histologically or cytologically confirmed as at least stage IIIB NSCLC, and who initiated 1L therapy for advanced NSCLC on or after February 1, 2019.
First-line pembrolizumab monotherapy for metastatic NSCLC: TULUNG registry
Eligible patients were ≥18 years old at the time of a histologically or cytologically confirmed diagnosis of metastatic (stage IV) NSCLC, with PD-L1 TPS ≥ 50% and no known EGFR sensitizing mutation or ALK translocation (EGFR/ALK wild-type, or missing test results) confirmed before initiating 1L pembrolizumab monotherapy on/after February 1, 2019. Patients who received pembrolizumab for indications other than metastatic NSCLC were excluded, as were those who received 1L therapy in a clinical trial setting.
Outcomes and analyses
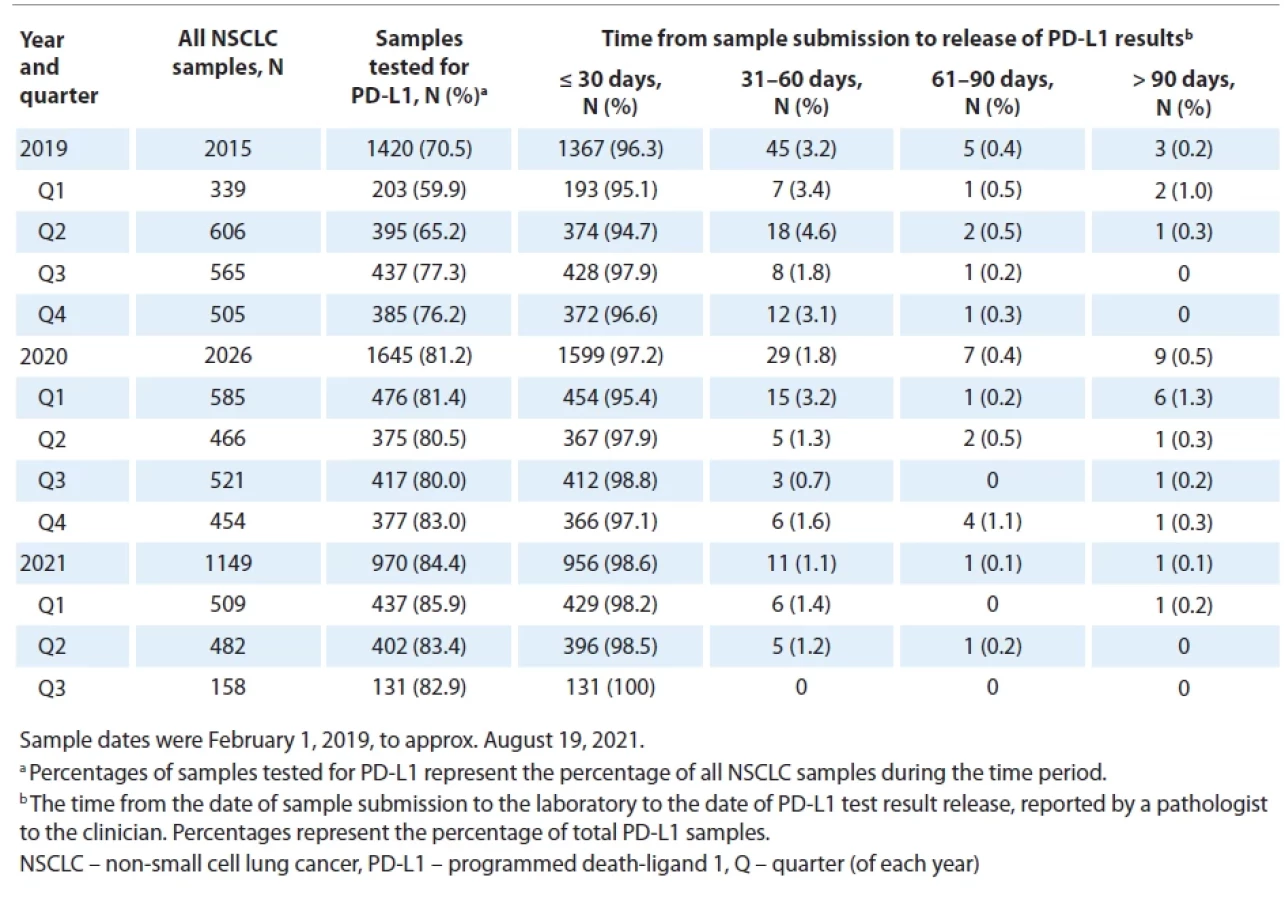
Using the KELLY registry, we calculated the percentages of tests for PD-L1 TPS among advanced NSCLC samples submitted each year and each quarter from February 1, 2019, to data cutoff (September 16, 2021). We also calculated the days from sample submission at the laboratory to availability of PD-L1 test results.
We described the characteristics of patients with advanced NSCLC in the TULUNG registry, in addition to the 1L targeted therapies administered to those with advanced NSCLC with PD-L1 TPS ≥ 50% during the study period. We also summarized characteristics of patients in the TULUNG registry who received 1L pembrolizumab monotherapy for metastatic NSCLC (PD-L1 TPS ≥ 50%, no known EGFR/ALK alteration) and analyzed two primary outcomes for this patient population. The real-world time on treatment (rwToT) was defined as the time from the first dose to the last dose of pembrolizumab (the earliest documented date among end-of-treatment dates, a recorded subsequent line of therapy, or date of death while on therapy). If the date of the last dose was unavailable, the patient was censored on the date of the last structured activity (most recent visit, treatment date, or date of progression). OS was defined as the time from the first dose of pembrolizumab to death from any cause, with censoring on the date of the last structured activity.
We used descriptive statistics for continuous variables, namely, mean, standard deviation (SD), median, interquartile range (IQR), and range. Categorical variables were described using frequency and proportions. We calculated relative frequencies based on the number of patients/samples in the relevant subgroup. Time-to-event variables (OS, rwToT) were estimated using the Kaplan-Meier method. A minimum of 6 months of follow-up time from the start of 1L pembrolizumab and the cutoff date was required for the assessment of time-to-event variables.
Results
PD-L1 testing patterns: KELLY registry
We identified 5,190 NSCLC samples submitted to the KELLY registry from February 1, 2019, to approx. August 19, 2021. The median age of patients with samples was 70 years (range, 20–99) and almost two-thirds were men (3,265; 63%); 3,000 samples (58%) were of nonsquamous NSCLC histology (supplementary Tab. S1).
The percentage of NSCLC samples tested for PD-L1 increased over time from 71% in 2019 to 84% in 2021. Most PD-L1 results were released within 30 days (Tab. 1), and most samples were tested using the PD-L1 IHC 22C3 pharmDx assay, regardless of sampling year (supplementary Tab. S2). During the study period, 93% of samples (> 90% of samples during each quarter of each year) were associated with a primary diagnosis rather than a repeat examination (data not shown).
Targeted therapy for advanced NSCLC: TULUNG registry
In the TULUNG registry, we identified 1,134 patients with advanced NSCLC who received targeted therapies including immunotherapy. Their median age was 68 years, over half (57%) were men, and the majority (81%) were current or former smokers. Other demographic and clinical characteristics of these patients are summarized in supplementary Tab. S3.

A total of 315 patients with advanced NSCLC and PD-L1 TPS ≥ 50% received 1L targeted therapy in 2019, 2020, and 2021. Most of these patients (70–80% each year) received 1L pembrolizumab monotherapy (Tab. 2). In 2021, 10% of patients received 1L pembrolizumab and pemetrexed.
1L pembrolizumab monotherapy for metastatic NSCLC: TULUNG registry
A total of 235 patients included in the TULUNG registry received 1L pembrolizumab monotherapy for stage IV NSCLC with PD-L1 TPS ≥ 50% and no known EGFR or ALK genomic alteration [15,16]. Their median age was 69 years (range 38–84); 126 (54%) patients were men; 232 (99%) were Caucasian; and 206 (88%) were current or former smokers (Tab. 3). All patients had Eastern Cooperative Oncology Group performance status (ECOG PS) of 0 or 1 (reimbursement criteria), and 170 (72%) had nonsquamous NSCLC.
First-line pembrolizumab monotherapy was initiated with a median of 1 month after the NSCLC diagnosis (Tab. 3). The median follow-up period was 4.3 months (range 0–28) from the start of pembrolizumab to death or last structured activity before data cutoff.
The median number of pembrolizumab doses was 10 (range, 1–41; Tab. 4). The 213 patients (91%) with no recorded subsequent treatment included 125 patients (53%) who were still receiving pembrolizumab monotherapy at the end of the follow-up period and 88 patients (37%) who discontinued treatment. Twenty-two patients (9%) treated with pembrolizumab monotherapy had subsequent therapy, most commonly pemetrexed, documented in the TULUNG registry (Tab. 4).



We evaluated OS and pembrolizumab rwToT for 199 patients (85%) with at least 6 months of follow-up. The median rwToT was 8.5 months, and the estimated on-treatment rates at 6 and 12 months were almost 60% and 36%, respectively (Fig. 1A). The median OS was not reached due to the low number of events (35, 18%).
We performed post hoc OS analyses in which we enriched data from the TULUNG registry with mortality data from the national registry of death certificates. (No changes other than adding dates of death were made in the dataset.) The minimum follow-up period was at least 6 months, and if a patient had a longer follow-up, their data were censored on the cutoff date (September 16, 2021). The median OS was 13.7 months (95% CI 12.3–17.7), and the estimated OS rates at 6 and 12 months were 70% and 59%, respectively (Fig. 1B).
Discussion
Our study leveraged two population-based registries in the Czech Republic to describe real-world PD-L1 testing, treatment patterns, and clinical outcomes following access to 1L pembrolizumab monotherapy for metastatic NSCLC via public insurance reimbursement in 2019. Using data from the KELLY registry, we found that the percentage of advanced NSCLC samples tested for PD-L1 was high already at the study start and further increased during the study period. In 1Q 2019, shortly after pembrolizumab was made available to patients, the testing rate was nearly 60%. As PD-L1 testing was available in the Czech Republic (in January 2018) before access to pembrolizumab, hence, testing preceded therapy reimbursement by 13 months. This situation may explain why the testing percentages were high shortly after pembrolizumab became accessible. The percentage of advanced NSCLC samples tested for PD-L1 increased to nearly 83% in 3Q 2021 when this study ended.
Using data from the TULUNG registry, we found that among Czech patients with advanced NSCLC who received therapies of interest for the registry and had tumors with PD-L1 TPS ≥ 50%, about 70–80% were treated with 1L pembrolizumab monotherapy each year during the study period. This percentage was the lowest in 2021 when 10% of patients received pembrolizumab with pemetrexed instead of monotherapy, a shift consistent with the reimbursement date for pembrolizumab with pemetrexed and platinum chemotherapy on March 1, 2021.
More than half of the 235 patients (58%) with metastatic NSCLC who received 1L pembrolizumab monotherapy were treated for more than 6 months and one-quarter (26%) were treated for 12 months or longer. The Kaplan-Meier median pembrolizumab rwToT was 8.5 months (95% CI 6.7–10.1), with estimated on-treatment rates at 6 and 12 months of almost 60% and 36%, respectively. This result is generally consistent with the median treatment duration for patients treated with 1L pembrolizumab monotherapy in clinical trials, namely, 7.9 months in KEYNOTE-024 [17,18], 6.6 months in patients with metastatic NSCLC and PD-L1 TPS ≥ 50% in the KEYNOTE-042 trial [19], and 9.7 months in the control group of patients with metastatic NSCLC and PD-L1 TPS ≥ 50% in the KEYNOTE-598 trial [20].
After supplementing mortality data from the TULUNG registry with records from the national registry of death certificates, we estimated median OS of 13.7 months (95% CI 12.3–17.7). The estimated OS rate at 6 and 12 months was almost 70% and 59%, respectively. This 12-month rate was lower than in the KEYNOTE-024, KEYNOTE-042, and KEYNOTE-598 trials, with 12-month rates of 70.3%, 63.5%, and 67.9%, respectively [17,20,21]. These differences can be explained by prognostic patient characteristics in our real-world study compared with the clinical trial patient populations and/or differences in subsequent lines of therapy. Our patients were older, with median age of 69 years, while the median ages of patients in the trial pembrolizumab arms were 64.5 years in KEYNOTE-024, 63 years in KEYNOTE-042, and 65 years in KEYNOTE-598.
Our patient population also included more current smokers, 123 (52%), compared with 34 (22%) in KEYNOTE-024 and 76 (27%) in KEYNOTE-598 trials. In the pembrolizumab group with TPS ≥ 50% in the KEYNOTE-042 trial, 57 (19%) patients were current smokers [22], considerably fewer than in our study. A recent meta-analysis concluded that quitting smoking “at or around” the diagnosis improves survival in patients with lung cancer [23]. Squamous NSCLC histology was reported in 29 patients (19%) in KEYNOTE-024, while squamous histology percentage in our study was greater (65; 28%) and similar to 89 (33%) in KEYNOTE-042 and 77 (27%) in KEYNOTE-598.
Most patients in our study (188, 80%) had baseline ECOG PS of 1, while this performance status was reported in 99 (64%) in KEYNOTE-024, 187 (69%) in KEYNOTE-042, and 180 (63%) in KEYNOTE-598 [17,19,20]. In the KEYNOTE-024, KEYNOTE-042, and KEYNOTE-598 trial patient populations, life expectancy was required to be at least 3 months [5,20,22], whereas there was no such inclusion criterion in the real-world clinical setting.
As in any retrospective observational study, we cannot exclude an inherent bias mostly due to missing data. The data extracts were performed from live databases; thus, a data entry backlog or incomplete records might have occurred. It is not possible to identify patients included in both registries, so we could not associate records of the same patients. Reasons for not testing were unavailable for the samples that were not tested. We cannot exclude the possibility of misclassification, especially for ECOG PS. In the population treated with 1L pembrolizumab monotherapy, we found that all patients had ECOG PS of 0 or 1. Since ECOG PS is a subjective clinical measure and is tied to reimbursement in the Czech Republic, there is the possibility of misclassification if treated patients had a worse ECOG PS. The TULUNG registry includes only patients treated with targeted therapies; therefore, the information about subsequent treatment with chemotherapy was unavailable. As a result, we could not evaluate the time to next treatment (TTNT), which was an outcome of interest. Pembrolizumab in combination regimens approved by the EMA became only partially accessible during the study period; therefore, we were unable to evaluate outcomes for these regimens.
Our study adds to the paucity of literature on treatment patterns and real-world outcomes in patients with metastatic NSCLC treated in Central Europe after the EMA approval and pembrolizumab access roll-out [24]. A recent study compared the characteristics of patients in the German CRISP registry with metastatic NSCLC, PD-L1 TPS ≥ 50%, and treated with pembrolizumab monotherapy who would be potentially eligible with those who would not be eligible in the KEYNOTE-042 and -024 studies. The authors concluded that potentially eligible patients had better prognostic factors and better outcomes than potentially ineligible patients representing the real-world population [25]. In 2021, Frost et al. published results of a German retrospective multicentric study aiming to validate clinical trial results in real-world patients. They concluded that outcomes in frail patients with worse ECOG PS, brain metastases, and receiving corticosteroids were worse than in clinical trials [26]. The OS in both German studies was higher than in ours, likely because of different baseline characteristics of the studied populations; however, all three studies demonstrate the effect of baseline characteristics on real-world patient outcomes.
Conclusion
In real-world patients with metastatic NSCLC and PD-L1 TPS ≥ 50% treated with pembrolizumab monotherapy, the estimated OS rate at 12 months was 59%. This is lower than in the KEYNOTE-024, KEYNOTE-042, and KEYNOTE-598 trials, in which the 12-month rates were 70.3%, 63.5%, and 67.9%, respectively. Clinical trial patient populations are homogeneous per defined eligibility criteria, while real-world patient populations are heterogeneous. Differences in baseline patient characteristics in disease registries compared with randomized clinical trials should be considered when evaluating real-world clinical outcomes. Findings of this study highlight variations in patient characteristics in real-world settings compared with randomized clinical trials and their impact on clinical outcomes.
Funding
This work was supported by Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA. Although the sponsors formally reviewed a penultimate draft, the opinions expressed are those of the authors and may not necessarily reflect those of the sponsors. All co-authors approved the final version of the manuscript.
Acknowledgments
The authors thank Kamila Novak, MSc, of KAN Consulting MON. I.K.E., Athens, Greece, for providing medical writing support, which was funded by Merck & Co., Inc., 126 East Lincoln Ave., p. o. Box 2000, Rahway, NJ 07065, USA, in accordance with Good Publication Practice (GPP3) guidelines and position of the European Medical Writers Association [27]. Editorial assistance was provided by Elizabeth V. Hillyer, DVM (freelance). This assistance was funded by Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA.
The authors thank the Czech centers and physicians for consistent provision of patients’ data into the TULUNG and KELLY registries. The project would not have been completed without the centers’ data contribution, namely, Radoslav Matěj (Department of Pathology and Molecular Medicine, Thomayer University Hospital, Prague), Linda Čapková (Department of Pathology and Molecular Medicine, 2nd Faculty of Medicine, Charles University and Motol University Hospital, Prague), Tomáš Jirásek (Regional Hospital Liberec – Department of Pathology), Dušan Žiak (EUC Laboratoře CGB a. s., Prague).
Potential conflicts of interest
Melissa L. Santorelli and Thomas Burke are full-time employees of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA, and hold stock of Merck & Co., Inc., Rahway, NJ, USA.
Goran Bencina was a full-time employee of Merck Sharp & Dohme LLC (MSD) at the time of the study and holds stock of Merck & Co., Inc., Rahway, NJ, USA.
Ondřej Fibigr has received speaker honoraria from GSK, Astra Zeneca, MSD, Sanofi.
Leona Koubková has received support for attending meetings and speaker honoraria from Pfizer, Bristol Myers Squibb, MSD, Astra Zeneca, Roche, Sanofi, Amgen, Merck and has served on advisory boards for Merck, MSD, Roche, Amgen.
Aleš Ryška has received consulting fees from Amgen, MSD, AstraZeneca, Boehringer-Ingelheim, Sanofi and speaker honoraria from Amgen, AstraZeneca, BMS, Eli-Lilly, Janssen-Cilag, MSD, Roche, Gilead, Novartis, Sanofi, Merck Serono, Bayer; has served on advisory boards for Amgen, MSD, AstraZeneca, Sanofi; and has received support to his institution for attending meetings or travel from Sanofi, Gilead, Roche.
All other authors have declared no conflicts of interest.
Employees of the funder participated in the design of the study; in the interpretation of data; in the writing of the manuscript; and in the decision to publish the results.
Zdroje
1. American Cancer Society. Key statistics for lung cancer. [online]. Available from: https: //www.cancer.org/cancer/types/lung-cancer/about/key-statistics.html.
2. WHO. Cancer today. [online]. Available from: https: //gco.iarc.fr/today/home.
3. Hendriks LE, Kerr KM, Menis J et al. Oncogene-addicted metastatic non-small-cell lung cancer: ESMO clinical practice guideline for diagnosis, treatment and follow-up. Ann Oncol 2023; 34 (4): 339–357. doi: 10.1016/j.annonc.2022.12.009.
4. Hendriks LE, Kerr KM, Menis J et al. Non-oncogene-addicted metastatic non-small-cell lung cancer: ESMO clinical practice guideline for diagnosis, treatment and follow-up. Ann Oncol 2023; 34 (4): 358–376. doi: 10.1016/j.annonc.2022.12.013.
5. Reck M, Rodriguez-Abreu D, Robinson AG et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N Engl J Med 2016; 375 (19): 1823–1833. doi: 10.1056/NEJMoa1606774.
6. European Medicines Agency. Keytruda. [online]. Available from: https: //www.ema.europa.eu/en/medicines/human/EPAR/keytruda.
7. Merck. European Commission approves Merck’s KEYTRUDA® (pembrolizumab) in combination with pemetrexed and platinum chemotherapy for the first-line treatment of patients with metastatic nonsquamous NSCLC, with no EGFR or ALK genomic tumor aberrations. [online]. Available from: https: //www.merck.com/news/european-commission-approves-mercks-keytruda-pembrolizumab-in-combination-with-pemetrexed-and-platinum-chemotherapy-for-the-first-line-treatment-of-patients-with-metastatic - nonsquamou/.
8. Merck. European Commission approves Merck’s KEYTRUDA® (pembrolizumab) in combination with chemotherapy for first-line treatment of adults with metastatic squamous non-small cell lung cancer (NSCLC). [online]. Available from: https: //www.merck.com/news/european-commission-approves-mercks-keytruda-pembrolizumab-in-combination-with-chemotherapy-for-first-line-treatment-of-adults-with-metastatic-squamous-non-small-cell-lung-cancer-nsc/.
9. Cufer T, Ciuleanu TE, Berzinec P et al. Access to novel drugs for non-small cell lung cancer in central and southeastern Europe: a Central European Cooperative Oncology Group analysis. Oncologist 2020; 25 (3): e598–e601. doi: 10.1634/theoncologist.2019-0523.
10. TULUNG. [online]. Available from: https: //tulung.registry.cz/index-en.php.
11. Kelly. [online]. Available from: https: //kelly.registry.cz/index-en.php.
12. Bratova M, Skrickova J, Matusikova M et al. Effectiveness of first-line anticancer treatment may predict treatment response in further lines in stage III/IV patients with non-small cell lung cancer. J Cancer Res Clin Oncol 2023; 149 (19): 17123–17131. doi: 10.1007/s00432-023-05431-5.
13. Institute of Biostatistics and Analyses. Let’s turn clinical questions to data-driven answers. [online]. Available from: https: //biostatistika.cz/index-en.php.
14. Borilova S, Dusek L, Jakubikova L et al. Lung cancer in the Czech Republic. J Thorac Oncol 2023; 18 (3): 271–277. doi: 10.1016/j.jtho.2022.11.023.
15. Amin M, Edge SB, Greene FL et al. AJCC cancer staging manual, 8th edition, Basel. Switzerland: Springer 2017.
16. Gospodarowicz MK, Wittekind C, Brierley JD. TNM classification of malignant tumours, 8th edition. Geneva 2016.
17. Reck M, Rodriguez-Abreu D, Robinson AG et al. Updated analysis of KEYNOTE-024: pembrolizumab versus platinum-based chemotherapy for advanced non-small-cell lung cancer with PD-L1 tumor proportion score of 50% or greater. J Clin Oncol 2019; 37 (7): 537–546. doi: 10.1200/JCO.18.00149.
18. Reck M, Rodriguez-Abreu D, Robinson AG et al. Five-year outcomes with pembrolizumab versus chemotherapy for metastatic non-small-cell lung cancer with PD-L1 tumor proportion score ≥ 50%. J Clin Oncol 2021; 39 (21): 2339–2349. doi: 10.1200/JCO.21.00174.
19. Velcheti V, Chandwani S, Chen X et al. First-line pembrolizumab monotherapy for metastatic PD-L1-positive NSCLC: real-world analysis of time on treatment. Immunotherapy 2019; 11 (10): 889–901. doi: 10.2217/imt-2019-0061.
20. Boyer M, Sendur MAN, Rodriguez-Abreu D et al. Pembrolizumab plus ipilimumab or placebo for metastatic non-small-cell lung cancer with PD-L1 tumor proportion score ≥ 50%: randomized, double-blind phase III KEYNOTE-598 study. J Clin Oncol 2021; 39 (21): 2327–2338. doi: 10.1200/JCO.20.03579.
21. Velcheti V, Chandwani S, Chen X et al. Outcomes of first-line pembrolizumab monotherapy for PD-L1-positive (TPS ≥50%) metastatic NSCLC at US oncology practices. Immunotherapy 2019; 11 (18): 1541–1554. doi: 10.2217/imt-2019-0177.
22. Mok TSK, Wu YL, Kudaba I et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): a randomised, open-label, controlled, phase 3 trial. Lancet 2019; 393 (10183): 1819–1830. doi: 10.1016/S0140-6736 (18) 32409-7.
23. Caini S, Del Riccio M, Vettori V et al. Quitting smoking at or around diagnosis improves the overall survival of lung cancer patients: a systematic review and meta-analysis. J Thorac Oncol 2022; 17 (5): 623–636. doi: 10.1016/j.jtho.2021.12.005.
24. Bílek O, Bořilová S, Grell P et al. Immunotherapy in the treatment of non-small cell lung cancer. Klin Onkol 2021; 34 (Suppl 1): 54–64. doi: 10.48095/ccko2021S54.
25. Griesinger F, Sebastian M, Brueckl WM et al. Checkpoint inhibitor monotherapy in potentially trial-eligible or trial-ineligible patients with metastatic NSCLC in the German prospective CRISP registry real-world cohort (AIO-TRK-0315). JTO Clin Res Rep 2024; 5 (4): 100626. doi: 10.1016/j.jtocrr.2023.100626.
26. Frost N, Kollmeier J, Misch D et al. Pembrolizumab as first-line palliative therapy in PD-L1 overexpressing (≥50%) NSCLC: real-world results with special focus on PS ≥2, brain metastases and steroids. Clin Lung Cancer 2021; 22 (5): 411–422. doi: 10.1016/j.cllc.2021.02.001.
27. ISMPP. GPP3 Guidelines, 2015. [online]. Available from: http: //www.ismpp.org/gpp3.
Štítky
Dětská onkologie Chirurgie všeobecná OnkologieČlánek vyšel v časopise
Klinická onkologie

2025 Číslo 3
- Diosmin a hesperidin: Co ukazuje farmakokinetika?
- Zkušenosti s axitinibem v léčbě metastatického renálního karcinomu
- Evaluace skóre m7-FLIPI u pacientů s folikulárním lymfomem odhalila slibný prediktivní biomarker k určení vhodné chemoterapie
- Neuropatie výrazně zpomaluje proces hojení u povrchových ran
- Zeolit-jodový komplex pomáhá v péči o infikované rány
Nejčtenější v tomto čísle
- Současná komplexní léčba karcinomu hrdla děložního
- Extravazace (paravazace) protinádorových léčiv – aktualizované doporučení (2025) pro standardní péči v rámci České republiky vycházející z multioborové spolupráce
- Testování PD-L1 v reálné praxi, první linie léčby pokročilého NSCLC a výsledky a využití první linie léčby metastatického NSCLC pembrolizumabem v monoterapii v České republice
- Současný management gastrointestinálních stromálních tumorů
Zvyšte si kvalifikaci online z pohodlí domova
Mazová zátka a její řešení
nový kurzVšechny kurzy