
Analysis of the epidemiologic, clinical, laboratory, ultrasonographic, and anatomopathological profile of women with hydatidiform mole at two referral centers in Northeastern Brazil
Analýza epidemiologického, klinického, laboratorního, ultrasonografi ckého a anatomicko-patologického profilu žen s hydatidiformní molou ve dvou referenčních centrech v severovýchodní Brazílii
Cíl: Zjistit profil žen podstupujících evakuaci dělohy pro podezření na hydatidiformní molu (HM) podle jejich klinických, laboratorních, ultrazvukových a anatomicko-patologických charakteristik ve dvou referenčních centrech v severovýchodní Brazílii. Metody: Retrospektivní kohortová studie byla provedena ve dvou referenčních centrech v období od října 2016 do prosince 2022 u žen podstupujících evakuaci dělohy pro podezření na HM. Hodnotily se sociodemografické charakteristiky, klinické parametry, biochemie, ultrazvuk, anatomická patologie a výsledky. Výsledky: Celkem bylo přijato 507 žen s klinickým podezřením na gestační trofoblastickou nemoc, u 334 z nich byla HM potvrzena, u 107 pacientek v centru 1 a 227 v centru 2. Průměrná vzdálenost mezi referenčním centrem a domovem pacientky byla 88 km. Průměrný věk žen byl 27 ± 9 let, s převahou 19–39 let (72 %), a přibližně 60 % případů bylo diagnostikováno v ≤ 12 týdnu těhotenství. Vaginální krvácení bylo pozorováno u 79 % žen. Transvaginální ultrazvuk vykazoval typický vzhled u 90 % vyšetření. Makroskopický aspekt byl popsán jako vezikula v 70 % případů. Evakuace dělohy byla prováděna především děložní kyretáží (43 %). Většina žen neměla žádné komplikace (69 %). Výsledek považovaný za remisi byl dosažen v 37,1 % případů, ale 38,9 % žen přestalo docházet na kontroly a 9 % nebylo po propuštění z nemocnice sledováno. Závěr: Vzdálenost, kterou ženy urazily do referenčních center, byla významná, ale většina žen neměla žádné komplikace. Remise byla pozorována u 37,1 % žen, ale byl zde vysoký podíl žen (38,9 %), které přestaly na kontroly docházet.
Klíčová slova:
výsledky – hydatidiformní mola – klinické parametry – ultrazvuk –anatomická patologie
Authors:
Eveline Valeriano Moura Linhares 1,2
![]() ; Francisco Edson de Lucena Feitosa 3
; Francisco Edson de Lucena Feitosa 3
![]() ; Antônio Braga 4
; Antônio Braga 4
![]() ; Edward Araujo Júnior 1
; Edward Araujo Júnior 1
![]() ; Evelyn Traina 1
; Evelyn Traina 1
![]() ; Cecília Maria Ponte Ribeiro 3
; Cecília Maria Ponte Ribeiro 3
![]() ; Sue Yazaki Sun 1
; Sue Yazaki Sun 1
![]()
Authors place of work:
Department of Obstetrics, Paulista School of Medicine – Federal University of São Paulo (EPM-UNIFESP), São Paulo-SP, Brazil
1; Department of Gynecology and Obstetrics, Federal University of Ceará (UFC), Sobral-CE, Brazil
2; Department of Gynecology and Obstetrics, Federal University of Ceará (UFC), Fortaleza-CE, Brazil
3; Department of Obstetrics and Gynecology, Federal University of Rio de Janeiro (UFRJ), Rio de Janeiro-RJ, Brazil
4
Published in the journal:
Ceska Gynekol 2025; 90(2): 129-140
Category:
Původní práce
doi:
https://doi.org/10.48095/cccg2025129
Summary
Objective: To determine the profile of women undergoing uterine evacuation for suspected hydatidiform mole (HM) according to their clinical, laboratory, ultrasound, and anatomopathological characteristics at two referral centers in Northeastern Brazil. Methods: Retrospective cohort study was performed in two referral centers between October 2016 and December 2022 with women undergoing uterine evacuation for suspected HM. Socio-demographic characteristics, clinics, biochemistry, ultrasound, anatomopathology, and outcome were evaluated. Results: A total of 507 women were admitted with clinical suspicion of gestational trophoblastic disease, of which 334 were confirmed, with 107 being in Center-1 and 227 being in Center-2. Mean distance between the referral center and the patient‘s home was 88 km. Mean age of the women was 27 ± 9 years, with a predominance of 19 to 39 years (72%), and approximately 60% of the cases were diagnosed ≤ 12 weeks of gestation. Vaginal bleeding was observed in 79% of women. Transvaginal ultrasound showed a typical appearance in 90% of the examinations. The macroscopic aspect was described as a vesicle in 70% of cases. Uterine evacuation was mainly performed by uterine curettage (43%). The majority of women had no complications (69%). The outcome considered to be remission was achieved in 37.1% of cases, but 38.9% abandoned follow-up, and 9% did not start follow-up after hospital discharge. Conclusion: The distance traveled by women to the referral centers was significant, but the majority of women had no complications. Remission was observed in 37.1% of women, but there was a high abandonment rate of 38.9%.
Keywords:
ultrasound – outcomes – hydatidiform mole – clinics – anatomopathology
Introduction
Gestational trophoblastic disease (GTD) is characterized by abnormal proliferation of various types of trophoblasts, including benign forms such as molar pregnancy, complete hydatidiform mole (CHM), and partial hydatidiform mole (PHM), as well as malignant forms, collectively referred to as gestational trophoblastic neoplasia (GTN) [1]. The incidence of GTD, especially HM, is low in the population and varies according to geographic distribution. HM is estimated to occur in 1 in 1,000 pregnancies in North America and Europe; however, the incidence of the disease is thought to be at least two to three times higher in Brazil [2]. In the Cariri region, State of Ceará, Northeastern Brazil, the estimated incidence of GTD is 1.015% of pregnancies [3].
The extremes of reproductive age are well recognized as a risk factor for the development of CHM, with adolescents having a 7-fold risk and women > 40 years having a 2-fold risk, while the distribution of PHM cases is uniform [4]. However, changes in the epidemiology of GTD have been observed in several countries [1]. Some studies also report a reduction in the age range and mean gestational age at uterine evacuation in women with CHM, as well as smaller uterine volumes, the latter attributed to an earlier diagnosis [5]. CHM and PHM develop malignancy in 18–28% and 2–4% of cases, respectively, in the United States [6]. In 2010, a study concluded that heterozygous complete moles have a higher risk of progression to GTD than homozygous complete moles. Cytogenetic analysis was performed using a short tandem repeat (STR) polymorphism from molar tissue and parental serum samples. It is important to note that this study involved a small, screened population and further research is needed on this topic [7].
In Brazil, the likelihood of developing GTN after molar pregnancy has been estimated to be 15–25% [8]. From an individual perspective, although almost all women with HM have a normal reproductive future [9], the risk of a repeat molar pregnancy increases up to 5-fold after the first molar pregnancy [6]. As a result of the increased use of ultrasound in the first trimester of pregnancy, the clinical presentation of HM has changed dramatically. In some cases where the clinical course is not very expressive, it will be necessary to wait for more data, such as an elevated blood human chorionic gonadotropin (hCG) level or an ultrasound examination with a more typical pattern, to confirm the clinical suspicion [10].
In Brazil, ultrasound is performed by a physician who may specialize in radiology or gynecology and obstetrics. Ultrasound scans are provided by the public health system, but there are some disparities between different regions of the country, as some cities offer immediate access, such as the first trimester scan, while others offer only one scan during pregnancy. Obstetric care in Brazil is characterized by two models: private (self-funded or through health insurance companies) and public (regulated by SUS, acronym in Portuguese, Brazil’s Unified Health System, at no cost to the user). In the public system, women diag - nosed at an early stage of pregnancy may initially receive care from a multidisciplinary team, including a nurse and a physician, at primary health care facilities. If there is a comorbidity or risk factor, the patient is referred to a secondary level for high-risk prenatal care or to a tertiary level for more complex maternity facilities.
For proper management of HM, it is recommended that the woman be referred to a referral center where she will receive appropriate treatment and guidance to minimize negative outcomes and psychological impact of the disease. The prognosis of patients with GTN improves 9-fold when treatment is performed in trophoblastic reference centers [11]. The only modifiable variable associated with a reduction in the lethality of GTN is its management at reference centers [12]. The care of women with GTD is directed to independent reference centers, supported as needed by the Brazilian Association of Gestational Trophoblastic Disease (ABDTG, acronym in Portuguese). Currently, there are 47 referral centers throughout the country, almost all of which are public services, mainly located in teaching and university hospitals.
The management of GTD after diag - nostic suspicion involves performing uterine evacuation in women with reproductive desire, preferably through uterine vacuum aspiration. Hysterectomy may be an alternative in those of advanced age with offspring [13]. The best described technique for evacuating the uterus is a vacuum or electric aspiration guided by ultrasound. However, because it requires the constant purchase of disposable materials, many hospitals do not have a sufficient supply to sustain its use. The material resulting from molar evacuation is typically sent in for histopathologic analysis when the procedure is performed at reference centers.
After discharge from the hospital, hCG blood level monitoring is essential in order to promote early detection of malignant progression or post-molar GTD. For outpatient follow-up of women with GTD, referrals to reference centers may require transportation from the patients‘ hometowns or they have to be arranged by the women themselves. Public health systems of the cities are responsible for facilitating patient transportation to the reference center, with local health departments responsible for coordinating and providing this support. However, in Brazil, due to the great distances and several socio-economic disparities, it is known that it is more difficult to return weekly for this post-molar follow-up [14].
The objective of this study was to determine the profile of women undergoing uterine evacuation for suspected HM, according to their clinical, laboratory, ultrasound, and anatomopathological characteristics, in two referral services in the state of Ceará, Northeastern Brazil.
Methods
Patients
A retrospective cohort study of women with suspected HM was conducted between October 2016 and December 2022 in two tertiary referral centers in the state of Ceará, Northeastern Brazil. This study was approved by the Ethics Committee of the Federal University of Ceará. Informed consent was not applicable. The two reference public health centers were the Assis Chateaubriand Maternity School in Fortaleza city (Center-2), a reference center for high-risk pregnancies with a specialized GTD outpatient clinic with 94 obstetric beds including an obstetric clinic and maternal intensive care unit beds. The Northern Region Hospital (Center-1) in Sobral city is a general hospital with an obstetric service for suspected cases of GTD with 43 obstetric beds for high-risk pregnancies.
Inclusion criteria were women with a diagnosis of HM, suspected by ultrasound examination in cases of early pregnancy or first trimester vaginal bleeding, who had undergone uterine evacuation. The exclusion criteria were women whose pathology revealed miscarriage or an unknown result, except for those whose clinical, laboratory, and/or ultrasound history maintained a strong suspicion of HM.
Variables
Socio-demographic characteristics
- Municipalities/Services: Fortaleza/Center-2 and Sobral/Center-1.
- Distance in kilometers between the patient‘s home and referral center, measured using Google Maps.
- Age in years, divided into the following age groups: ≤ 15 years, 16 to 18 years, 19 to 39 years, and ≥ 40 years.
- Gestational age: gestational age based on the last menstrual period.
- Total number of pregnancies, including the current one.
- Parity (number of deliveries).
Clinics
Vaginal bleeding;
- Anemia: hemoglobin blood level < 11 mg/dL in a blood count taken before uterine evacuation, and severe anemia hemoglobin ≤ 7.0 mg/dL.
- Preeclampsia: arterial blood pressure ≥ 140 × 90 mmHg on two occasions 4 hours apart and proteinuria (≥ 300mg/dL in 24 hours of collection or protein/creatinine ratio ≥ 0.3 mg/dL or 1+ on two occasions 4–6 hours apart or ≥ 2+ in any single urine sample – qualitative) [15].
- Hyperemesis gravidarum: nausea and vomiting requiring medication.
- Thyrotoxic crisis: TSH blood levels < 0.5 mUI/mL associated with the need for beta-blockers for clinical improvement [16].
- Pulmonary symptoms.
Biochemistry, Ultrasound, and Anatomopathology
- Typical image of HM: hyperechoic endometrial echo filled with hypoanechoic, irregular images [1].
- Non-developing pregnancy:
- incomplete miscarriage: partial expulsion of the products of pregnancy with an endometrial echo ≥ 16 mm;
- anembryonic pregnancy: retention of pregnancy material, closed uterine cervix, mean gestational sac diameter > 20 mm without an embryo, or mean gestational sac diameter < 20 mm with an embryo without growth in 7 days;
- retained miscarriage: crown-rump length (CRL) > 6 mm without cardiac activity or CRL < 6 mm without growth in 7 days;
- tecalutein cyst: multiple simple anechogenic cysts (4 to 8 cm), usually bilateral.
- hCG blood levels: pre-evacuation levels.
- Hemoglobin and hematocrit blood levels: pre-evacuation levels recorded in medical records.
- Chest X-ray: record of findings such as ground-glass infiltrates, pleural effusion, pulmonary nodules.
- Macroscopic aspect: vesicles, ovular/placental remnants.
- Anatomopathology: PHM, CHM, unclassified HM, miscarriage/decidual remnants, and GTN.
Outcomes
- Spontaneous remission: three normal weekly hCG blood levels ≤ 5 mUI/mL – followed by 6 normal monthly tests for HCM and 1 test in 1 month for HPM.
- GTN, post-treatment discharge: progression to GTN (hormonal or anatomopathological diagnosis), surgical and/or chemotherapy treatment, and follow-up to outpatient discharge.
- Abandonment of follow-up: started outpatient follow-up but did not complete it, with hCG blood levels > 5 mUI/mL at the last evaluation.
- Incomplete follow-up: started outpatient follow-up but did not complete follow-up, with hCG blood levels at the last evaluation < 5 mUI/mL.
- No follow-up: no outpatient returns after discharge.
- Prenatal care: new pregnancy during outpatient follow-up.
Statistical analysis
Variables were presented as mean and standard deviation, median, percentiles, Min. and Max., frequency, and prevalence. The Mann-Whitney U-test was used to analyze the characteristics of the women and to check that the data did not follow a Gaussian distribution. Pearson‘s chi-squared test and Fisher‘s exact test were used to investigate associations between categorical variables. A 5% significance level was used. Statistical analyses were performed using the R statistical program version 3.2.2 and Excel 2016 (Microsoft Corp., Redmond, WA, USA).
Results
During the study period, 507 women with clinical suspicion of HM were admitted to both referral centers. We initially excluded 5 cases whose pathology was unknown (2 Center-1 and 3 Center-2) and 168 that turned out to be miscarriages (101 Center-1 and 67 Center-2). Of the 334 patients selected, 107 were from Center-1 and 227 were from Center-2. Among the 107 women from Center-1 : 64 HCM, 27 HPM, 8 unclassified HM, 4 miscarriage/decidual remnants, 4 GTN (1 invasive mole and 3 choriocarcinomas). In the 227 women in Center-2 : 136 HCM, 78 HPM, 5 unclassified HM, 3 miscarriages/decidual remnants, and 5 GTN (2 invasive moles and 3 choriocarcinomas). It should be noted that the 7 women with pathology of miscarriage/decidual remnants (4 Center-1 and 3 Center-2) who remained in the analysis were kept because they had a strong suspicion of HM (clinical, laboratory, and ultrasound findings). The ratio between the types of HM followed up in each service was as follows for Center-2 : 227 HM (136/59.9% HCM; 78/34.4% HPM; 5/2.2% unclassified HM; 5/2.2% GTN; 3/1.3% miscarriages/decidual remnants); Center-1 : 107 HM (64/59.8% HCM; 27/25.2% HPM; 8/7.5% unclassified HM; 4/3.7% GTN; 4/3.7% miscarriages/decidual remnants) (Scheme 1).
During the evaluation period, the services had the following number of deliveries: Center-2 33,222 deliveries (19,922 cesarean sections and 13,300 vaginal deliveries), and Center-1 10,752 deliveries (7,866 cesarean sections and 2,886 vaginal deliveries). The ratio of the number of deliveries to the incidence of HM between the services was as follows: 62 per 1,000 deliveries at Center-2 and 99 per 1,000 deliveries at Center-1. Regarding the referral center where the women were seen, more than half were seen in Center-2 (227/68%) and another half in Center-1 (107/32%). The mean total distance traveled between the referral center and the patient‘s home was 88 ± 106 km. This distance was approximately 2 km greater in Center-1 than in Center-2, and there was statistical significance (P = 0.029) (Tab. 1).
As for the year in which the women were seen in the two services, there was a predominance of the years 2022 (82/25%), 2020 (74/22%), and 2019 (71/21%). Mean age of the women seen at the two centers was 27 ± 9 years, with a predominance of 19 to 39 years (242/72%). Gestational age could not be determined in 26% of the women. Considering the available gestational age, the mean was 12.6 ± 4.2 weeks and 60% of the cases occurred in the period ≤ 12 weeks of gestation (148/334) (Tab. 1).
Regarding parity, the majority of women were multiparous with at least one previous delivery (185/55%), with a higher percentage of multiparous in Center-1 (63/58.9%) compared to Center-2 (122/53.7%) (P = 0.032). Regarding the number of pregnancies, ≥ 1 pregnancies predominated (201/60%) with a higher percentage of the number of pregnancies in Center-1 (68/63.6%) compared to Center-2 (133/58.6%) (P = 0.031). Regarding the history of GTD, only 8/2.4% reported this disease in the obstetric history (Tab. 1).
With regard to vaginal bleeding at admission, 79% (264/334) of the women seen reported this complaint. The percentage of women with vaginal bleeding was higher in Center-2 (195/86.3%) compared to Center-1 (64/64.5%) (P < 0.001). Among symptomatic women, hyperemesis gravidarum (25/7.5%), pre-eclampsia (14/4.2%), and thyrotoxic crisis (2/0.6%) were more frequently detected. Preeclampsia was more frequent in Center-2 (13/5.7%) compared to Center-1 (1/0.9%) (P = 0.043) (Tab. 2).
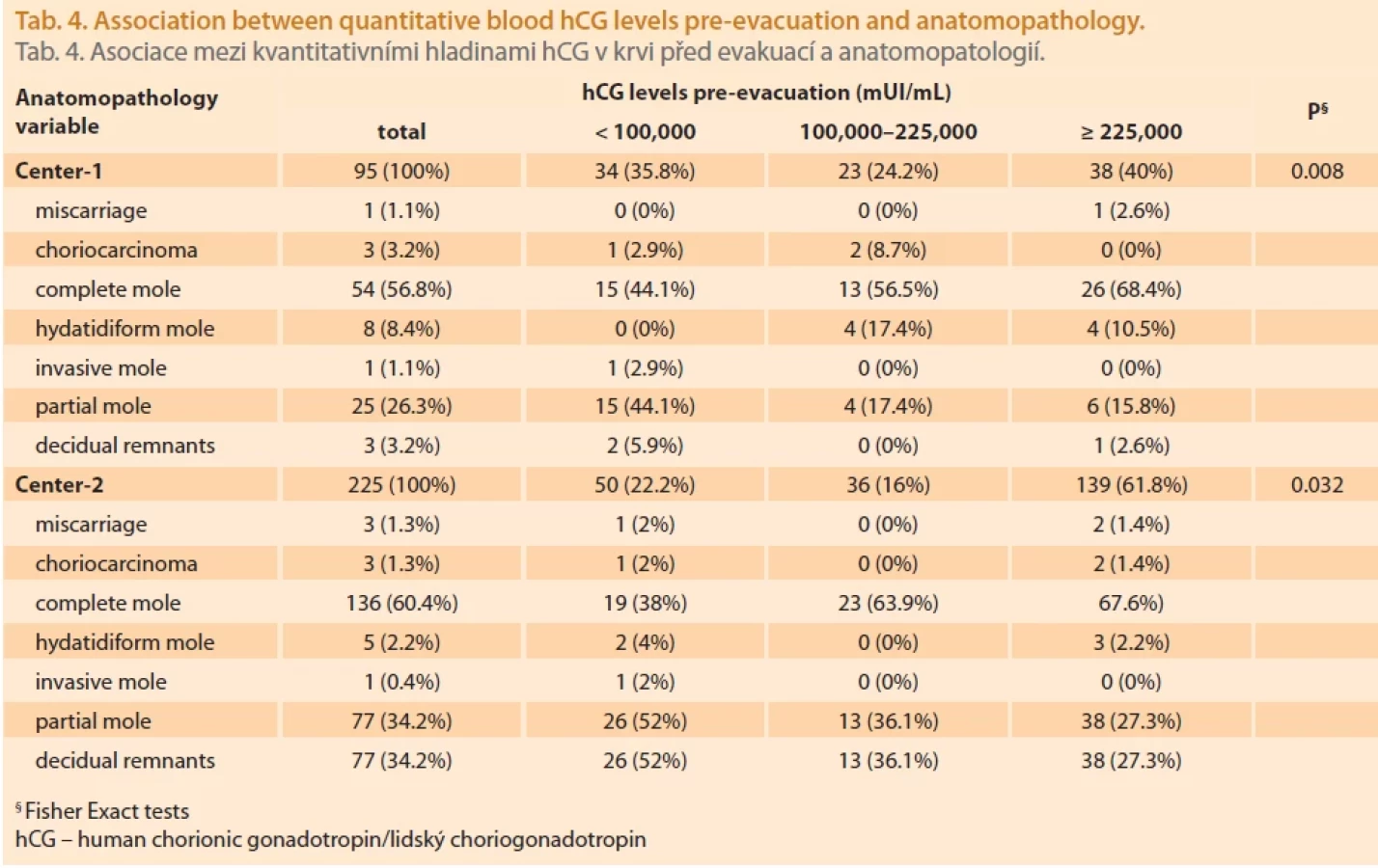
The mean pre-evacuation hCG blood levels were 196,046 ± 163,007 mUI/mL, and this value was unknown in 14/4.19% of the women. Blood hCG levels upon admission were as follows: < 100,000 (26.3%), 100,000 to 225,000 (18.4%), and > 225,000 mUI/mL (55.3%). There was a statistical difference when categorized quantitative hCG blood levels were evaluated (P < 0.001). When transvaginal ultrasound was performed, all were performed upon arrival and 301/90% had a typical HM appearance. A total of 26/7.8% had theca lutein cysts. Regarding chest X-rays, 313/93.7% of the women did not perform this examination and of those who underwent this examination, 11 (3.3%) had X-ray findings that varied between nodules, opacities, effusions, and signs of congestion. There was statistical significance in the inter-center comparison analysis (P = 0.002). Regarding the type of uterine evacuation, conventional uterine curettage predominated (144/43%), followed by manual vacuum aspiration (110/33%). However, when the services were analyzed separately, manual vacuum aspiration was used more often in Center-2 (94/41.8%) than in Center-1 (16/15.8%) (P < 0.001). Of the women studied, one was admitted at 22 weeks of gestation with PHM and acute pulmonary edema. After an unsuccessful attempt at labor induction and curettage, she underwent cesarean section due to her acute condition (Tab. 2).
Regarding the macroscopic aspect, majority of specialists described the presence of vesicles in the operative report (233/70%), with this description dominating in Center-2 (179/78.9%), whereas in Center-1 there was a greater balance between the presence of vesicles (54/50.5%) and ovular/placental remnants (47/43.9%) (P < 0.001). Regarding complications from admission to follow-up, a total of 229/69% had no complications. Among those with complications, the following were identified: vaginal bleeding (3/0.9%); perforation (1/0.3%); and anemia (20/5.9%), of which 5 were severe anemia. In terms of anatomopathology, a total of 200 (60%) had CHM, 105 (31%) had PHM, and 13 (3.9%) had an unclassified HM. The percentage of HCM was similar between the services, with 64.0/59.8% in Center-1 and 136.0/59.9% in Center-2 (P = 0.018) (Tab. 3).
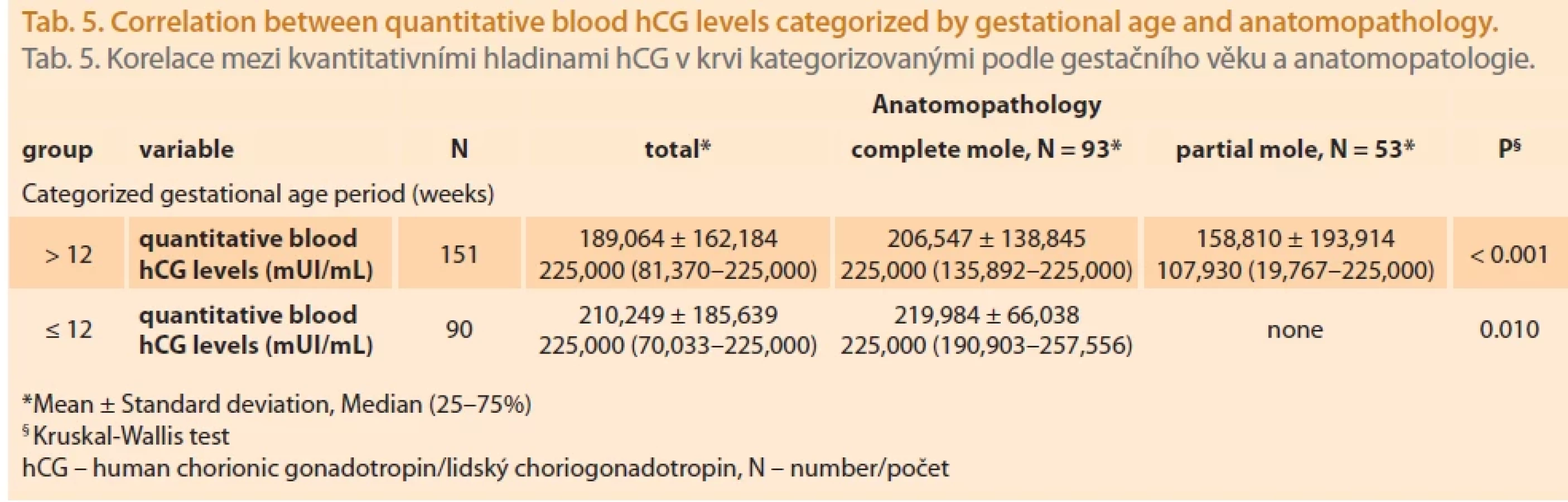
Categorization of quantitative blood hCG levels into parameters: > 100,000; 100,000–225,000; and > 225,000 mUI/mL. It was observed that the highest pre-evacuating quantitative blood hCG levels (> 225,000 mUI/mL) were found in women with HCM – 71.4% (Graph 1, Tab. 4). Tab. 5 shows the correlation between quantitative blood hCG levels categorized by gestational age and anatomopathology.
Regarding the outcome, spontaneous remission, defined as normal blood hCG levels during the 6 months following the first normal blood hCG levels after uterine evacuating, was achieved in 124/37.1%. The percentage of follow-up to spontaneous remission was higher in Center-2 (93/41%) than in Center-1 (31/29%). It was found that 73/21.9% did not complete follow-up (18/16.8% in Center-1 and 55/24.2% in Center-2). The loss to follow-up was higher in Center-1 (26/24.3%) than in Center-2 (31/13.7%). Another 30/9.0% never started follow-up (15/14.0% in Center-1 and 15/6.6% in Center-2). Two women became pregnant again during follow-up (one patient in each Center). There was a statistically significant difference between the two Centers in terms of outcome (Tab. 6).
Of the 334 women included in the study, a total of 73 were diagnosed as GTN. Of these, 9 were characterized as GTN based on the pathology report (6 choriocarcinomas and 3 invasive moles). Another 64/21% were diagnosed as GTN, identified after laboratory follow-up as they evolved with a plateau for at least 3 weeks, elevation of hCG blood levels for at least 2 weeks, or persistence of hCG blood levels for ≥ 6 months after uterine evacuation according to the FIGO classification. In this population, 35 (54.6%) were CHM, 19 (29.6%) were PHM, 3 (4.68%) were unclassified HM, and 7 (10.9%) women were followed up even with pathology of miscarriage/decidual remnants due to the high clinical suspicion having been treated for GTN. Of the 73 women followed up for GTN (9 by anatomopathological diagnosis and 64 by biochemical diagnosis during post-molar follow-up), 66% of women (48/73) were followed up to outpatient discharge, while another 34% of women (25/73) abandoned the follow-up before outpatient discharge, and of those who abandoned, 9 were still positive for hCG blood levels. The mean follow-up time between uterine evacuation and outpatient discharge was 335 ± 224 days (216–369), with the mean time being longer in Center-2 (353 ± 236 days) compared to Center-1 (240 ± 108 days) (P = 0.008).

* Ženy se silným podezřením na hydatidiformní molu (klinický, laboratorní a/nebo ultrazvukový nález), které zůstaly mezi hodnocenými případy.





Discussion
This study identified 334 cases of GTD, 107 from Center-1 and 227 from Center-2. It is important to note that the cases evaluated may not reflect the total number of women affected by GTD in the state of Ceará, Northeastern Brazil. The reason for this could be the fragility of the assertive diagnosis, leading to procedures aimed at non-evolving pregnancies of another classification (miscarriage or anembryonic pregnancy) in women in whom GTD was not suspected in the first trimester. In addition, women admitted with a less typical history or with irregular vaginal bleeding, who had already undergone uterine evacuation at other services and who did not have a new surgical procedure in these centers and therefore did not have histopathologic material for analysis, may also be underreported.
Considering the two Centers, 200 women had CHM (60%), 105 had PHM (31%), 13 had unclassified HM (3.9%), and 9 had histopathologic GTN (2.7%). In a previous study in 10 reference centers in Brazil with 5,250 women, 63.2% had CHM and 29.5% had PHM [17]. Nadhan et al. [18] reported that the most common form of GTD, HM, has an incidence of 1 case per 1,000 pregnancies in North America and Europe. In Brazil, HM is estimated to occur in 1 in 200 to 1 in 400 pregnancies, approximately 5 to 10 times more commonly than in North America and Europe [19].
This study showed a long distance between the patient’s home and the referral center, with a mean of 88 km, and the presence of women from other Brazilian states. Silva et al. [20] and Clark et al. [21] highlighted the 80 km cut-off point as a negative factor in the clinical condition, making it difficult to access specialized centers and worsening the clinical condition of GTD. On the other hand, another study considered that 50 km would already be a distance with a potentially unfavorable outcome, including death from GTD [14]. A retrospective historical cohort study of GTN women followed at 8 Brazilian referral centers showed that when the distance between the patient’s home and the referral center was ≥ 56 km, there was also an increase in the occurrence of metastatic disease, the need for multi-agent chemotherapy, loss to follow-up during chemotherapy, the occurrence of chemoresistance, relapse, and death from GTN [22].
Regarding age, we found that the mean age of the women was 27 years. It should be noted that we did not observe a significant difference in the age of the women between the two centers. Yuk et al. [23] and Taye et al. [24] observed that women > 40 years had a higher risk of developing GTD, while Mulisya et al. [25] observed this profile in women younger than 25 years. Regarding gestational age at diagnosis of GTD, the women had a mean of 12.6 weeks, with minimal difference between the two centers. The mean gestational age at diagnosis is currently around 10 to 12 weeks, which is in line with our results [26]. It should be noted that both centers are located in the Northeast of Brazil, a region with great socio-economic and public health disparities. In addition, previous history of GTD was low (8/2.4%) in both centers, confirming the literature indicating that the risk of GTD following a molar pregnancy is low (0.6 to 2.0%) [27].
When the clinical complaints of the two centers were evaluated, it was found that a total of 79.3% of the women had vaginal bleeding. This finding is consistent with a study that found 90.1% of women with HM had abnormal vaginal bleeding [28]. Early diagnosis of HM confirms a lower frequency of associated symptoms such as hyperemesis gravidarum (7.5%), preeclampsia (4.2%), and thyrotoxic crisis (0.6%), which was confirmed in this study and is consistent with the findings in the literature [29,30]. A systematic review of data available between 2002 and 2010 found that the incidence of preeclampsia ranged from 1.2 to 4.2% and that of eclampsia ranged from 0.1 to 2.7%, with higher rates in regions with lower socioeconomic status [31]. The most severe form of vomiting in pregnant women, known as hyperemesis gravidarum, accounts for 1.1% of all cases of nausea and vomiting in pregnancy [32]. Transient gestational thyrotoxicosis (TGT) or transient gestational hyperthyroidism is the main differential diagnosis of Graves‘ disease and the most common clinical presentation, occurring in up to 5% of pregnancies and limited to the first half of pregnancy. There is an increased risk of TGT in conditions with elevated hCG levels, such as twin pregnancies, hydatidiform mole, and choriocarcinoma [33].
It has been shown that early miscarriages often mimic GTD on transvaginal ultrasound because hydropic and cystic images are seen that simulate HM [34]. This may also explain the high percentage of ultrasound examinations (90%) with a mole-like appearance found in this study. A meta-analysis aimed at evaluating the diagnostic value and accuracy of ultrasound in the diagnosis of HM in all trimesters of pregnancy high - -lighted that although the sensitivity was relatively low at 52.2%, the specificity was high at 92.6% [36].
Regarding the type of uterine evacuation, in Center-2, manual vacuum aspiration predominated in 41.8% of cases, with another 20.4% using a combination of techniques. In a study by Matos et al. [35], 51.9% underwent uterine curettage and 30.4% underwent manual vacuum aspiration. In a retrospective study comparing manual vacuum aspiration with electrical aspiration in women with GTD in Rio de Janeiro, Brazil, similar results were observed between the two groups, with manual vacuum aspiration being associated with a lower rate of synechiae [36]. Padrón et al. [36] described that in women who underwent vacuum aspiration, whether electrical or manual, it was associated with uterine curettage to ensure complete uterine evacuation, which may explain the combination of techniques used in 65/19.9% of women in our study.
Regarding the macroscopic aspect of GTD, we observed that in Center-2 there was a predominance of vesicles (179.0/78.9 vs. 44.0/19.4%), while in Center-1 there was a greater balance between ovular/placental remnants and vesicles (47.0/43.9 vs. 54.0/50.5%), with a statistical difference. This finding highlights the subjectivity of macroscopic evaluation of uterine evacuation material reinforcing the importance of histopathologic analysis to confirm the disease [37].
Regarding the outcome, it was observed that remission predominated in both centers; however, there were still high rates of abandonment of follow-up and of women not being followed up. These data are of particular concern because they reveal a number of women who were lost to follow-up with a positive hCG serum, and who were unknown to the centers. Timely diagnosis of recurrent GTN is challenging because in most cases women are asymptomatic and the new increase in hCG serum is insidious. Otherwise, in the absence of follow-up, women return with signs and symptoms of metastases [38]. On the other hand, we observed that a total of 51.4% of women, including both benign and malignant forms of GTD, completed adequate follow-up and were safely discharged. In the analysis of the 325 women followed up for HM, 64 were diagnosed with GTN after biochemical follow-up (21.8%). A previous study also showed that although the majority of CHM are benign, the risk of developing GTN can be as high as 18–19% [39].
In summary, the prevalence of GTD was 65.8% with a total of 32.1% from Center-1 and 67.9% from Center-2. The distance traveled by women to the referral centers was significant, but the majority of women had no complications. Remission was observed in 37.1% of women with HM. In addition, there was a high abandonment rate of 38.9%, which can be explained by the numerous social and demographic barriers.
Zdroje
1. Ngan HY, Seckl MJ, Berkowitz RS et al. Update on the diagnosis and management of gestational trophoblastic disease. Int J Gynaecol Obstet 2018; 143 (Suppl 2): 79–85. doi: 10.1002/ijgo.12615.
2. Braga A, Lin LH, Maestá I et al. Gestational trophoblastic disease in Brazil. Rev Bras Ginecol Obstet 2019; 41 (4): 211–212. doi: 10.1055/s-0039-1688566.
3. Soares MK, Oliveira JF, Oliveira MA. Incidence gestational trophoblastic disease in the years of 2007 to 2011 in a public hospital in the region of Cariri. Cadernos ESP. Ceará 2015; 9 (1): 35–41.
4. Gockley AA, Melamed A, Joseph NT et al. The effect of adolescence and advanced maternal age on the incidence of complete and partial molar pregnancy. Gynecol Oncol 2016; 140 (3): 470–473. doi: 10.1016/j.ygyno.2016. 01.005.
5. Mangili G, Garavaglia E, Cavoretto P et al. Clinical presentation of hydatiform mole in northern Italy: has it change in the last 20 years? Am J Obstet Gynecol 2008; 198 (3): 302e.1–302.e4. doi: 10.1016/j.ajog.2007.09.036.
6. Garner EL, Goldstein DP, Feltmate CM et al. Gestational trophoblastic disease. Clin Obstet Gynecol 2007; 50 (1): 112–122. doi: 10.1097/GRF.0b013e31802f17fc.
7. Baasanjav, Usui H, Kihara M et al. The risk of post-molar gestational trophoblastic neoplasia is higher in heterozygous than in homozygous complete hydatidiform moles. Hum Reprod 2010; 25 (5): 1183–1191. doi: 10.1093/humrep/deq052.
8. Uberti EM, Diestel MC, Guimarães FE et al. Gestational trophoblastic disease: one more risk in adolescent pregnancy. Acta Obstet Gynecol Scand 2002; 81 (4): 356–363. doi: 10.1034/j.1600-0412.2002.810415.x.
9. Lurain JR. Gestational trophoblastic disease II: classification and management of gestational trophoblastic neoplasia. Am J Obstet Gynecol 2010; 204 (1): 11–18. doi: 10.1016/ j.ajog.2010.06.072.
10. Lima LL, Parente RC, Maestá I et al. Clinical and radiological correlations in patients with gestational trophoblastic disease. Radiol Bras 2016; 49 (4): 241–250. doi: 10.1590/0100-3984.2015.0073.
11. Kohorn EI. The new FIGO 2000 staging and risk factor scoring system for gestational trophoblastic disease description and critical assessment. Int J Gynecol Cancer 2001; 11 (1): 73–77. doi: 10.1046/j.1525-1438.2001.01100 1073.x.
12. Freitas F, Braga A, Viggiano M et al. Gestational trophoblastic neoplasia lethality among Brazilian women: a retrospective national cohort study. Gynecol Oncol 2020; 158 (2): 452–459. doi: 10.1016/j.ygyno.2020.04.704.
13. Elias KM, Berkowitz RS, Horowitz NS. State--of-the-art workup and initial management of newly diagnosed molar pregnancy and postmolar gestational trophoblastic neoplasia. J Natl Compr Canc Netw 2019; 17 (11): 1396–1401. doi: 10.6004/jnccn.2019.7364.
14. Braga Neto AR, França SL. Impact of the distance between the patient’s residence and the reference center on clinical and quality indicators of healthcare provided to women with gestational trophoblastic neoplasia in the State of Rio de Janeiro. J Bras Ginecol 2023; 133: e2313382.
15. Mol BW, Roberts CT, Thangaratinam LA et al. Pre-eclampsia. Lancet 2016; 387 (10022): 999–1011. doi: 10.1016/S0140-6736 (15) 00070-7.
16. de Almeida CE, Curi EF, de Almeida CR et al. Thyrotoxic crisis associated with gestational trophoblastic disease. Rev Bras Anestesiol 2011; 61 (5): 604–609. doi: 10.1016/S0034-7094 (11) 70071-X.
17. Braga A, Uberti EM, Fajardo MC et al. Epidemiological report on the treatment of patients with gestational trophoblastic disease in 10 Brazilian referral centers: results after 12 years since International FIGO 2000 Consensus. J Reprod Med 2014; 59 (5–6): 241–247.
18. Nadhan R, Vaman JV, Nirmala C et al. Insights into dovetailing GTD and cancers. Crit Rev Oncol Hematol 2017; 114 : 77–90. doi: 10.1016/ j.critrevonc.2017.04.001.
19. Braga A, Obeica B, Moraes V et al. Gestational trophoblastic disease – update. Revista HUPE 2014; 13 (3): 55–61.
20. da Silva VA, Maestá I, da Costa RA et al. Geographical health district and distance traveled influence on clinical status at admission of patients with gestational trophoblastic disease. Rev Bras Ginecol Obstet 2023; 45 (7): e384–e392. doi: 10.1055/s-0043-1772179.
21. Clark LH, Staley SA, Barber EL et al. The effect of distance traveled on disease outcomes in gestational trophoblastic neoplasia. Am J Obstet Gynecol 2016; 215 (2): 217.e1–217.e5. doi: 10.1016/j.ajog.2016.02.008.
22. Braga A, Lopes R, Campos V et al. The impact of the distance traveled between residence and gestational trophoblastic neoplasia reference center and clinical outcomes in Brazilian women. Gynecol Oncol 2023; 176 : 130–138. doi: 10.1016/j.ygyno.2023.07. 012.
23. Yuk JS, Baek JC, Park JE et al. Incidence of gestational trophoblastic disease in South Korea: a longitudinal, population-based study. Peer J 2019; 7: e6490. doi: 10.7717/peerj. 6490.
24. Taye A, Jarso H, Ahmed Y. Incidence and clinical profiles of gestational trophoblastic diseases in South West Ethiopia. EC Gynaecology 2019; 8 (2): 40–49.
25. Mulisya O, Roberts DJ, Sengupta ES et al. Prevalence and factors associated with hydatidiform mole among patients undergoing uterine evacuation at Mbarara regional referral hospital. Obstet Gynecol Int 2018; 2018 : 9561413. doi: 10.1155/2018/9561413.
26. Soper JT. Gestational trophoblastic disease: current evaluation and management. Obstet Gynecol 2021; 137 (2): 355–370. doi: 10.1097/AOG.0000000000004240.
27. Ngan HY, Seckl MJ, Berkowitz RS et al. Diagnosis and management of gestational trophoblastic disease: 2021 update. Int J Gynecol Obstet 2021; 155 (Suppl 1): 86–93. doi: 10.1002/ijgo.13877.
28. Zhao P, Chen Q, Lu W. Comparison of different therapeutic strategies of complete hydatidiform mole in women at least 40 years old: a retrospective cohort study. BMC Cancer 2017; 17 (1): 733. doi: 10.1186/s12885-017-3749-8.
29. Braga A, Maestá I, Short D et al. Hormonal contraceptive use before hCG remission does not increase the risk of gestational trophoblastic neoplasia following complete hydatidiform mole: a historical database review. BJOG 2016; 123 (8): 1330–1335. doi: 10.1111/1471-0528. 13617.
30. Ramos MM, Maesta I, Araújo Costa RA et al. Clinical characteristics and thyroid function in complete hydatidiform mole complicated by hyperthyroidism. Gynecol Oncol 2022; 165 (1): 137–142. doi: 10.1016/j.ygyno.2022.01.037.
31. Abalos E, Cuesta C, Grosso AL et al. Global and regional estimates of preeclampsia and eclampsia: a systematic review. Eur J Obstet Gynecol Reprod Biol 2013; 170 (1): 1–7. doi: 10.1016/j.ejogrb.213.05.005.
32. Miller F. Nausea and vomiting in pregnancy: the problem of perception – is it really a disease? Am J Obstet Gynecol 2002; 186 (5): S182–S183. doi: 10.1067/mob.2002.122594.
33. Iijima S. Pitfalls in the assessment of gestational transient thyrotoxicosis. Gynecol Endocrinol 2020; 36 (8): 662–667. doi: 10.1080/09513590.2020.1754391.
34. Newhouse I, Spacey A, Scragg B et al. The diagnostic value and accuracy of ultrasound in diagnosing hydatidiform mole: a systematic review and meta-analysis of the literature. Radiography (Lond) 2022; 28 (4): 897–905. doi: 10.1016/j.radi.2022.06.005.
35. Matos MM, Menezes MP, Rodrigues LM et al. Evaluation of the epidemiological profile of patients with Gestational Trophoblastic Disease treated at the Reference Center of Sergipe. Res Soc Develop 2021; 10 (3): e4110312934. doi: 10.33448/rsd-v10i3.12934.
36. Padrón L, Filho JR, Amim Junior J et al. Manual compared with electric vacuum aspiration for treatment of molar pregnancy. Obstet Gynecol 2018; 131 (4): 652–659. doi: 10.1097/AOG.0000000000002522.
37. Biscaro A, Silveira SK, de Figueiredo Locks G et al. Frequency of hydatidiform mole in tissue obtained by curettage. Rev Bras Ginecol Obstet 2012; 34 (6): 254–258.
38. Li J, Wang Y, Lu B et al. Gestational trophoblastic neoplasia with extrauterine metastasis but lacked uterine primary lesions: a single center experience and literature review. BMC Cancer 2022; 22 (1): 509. doi: 10.1186/s12885-022-09620-2.
39. Sun SY, Melamed A, Joseph NT et al. Clinical presentation of complete hydatidiform mole and partial hydatidiform mole at a regional trophoblastic disease center in the United States over the past 2 decades. Int J Gynecol Cancer 2016; 26 (2): 367–370. doi: 10.1097/IGC.0000000000000608.
ORCID of authors
E. V. Moura Linhares 0000-0001-7897-3724
F. E. de Lucena Feitosa 0000-0001-8396-2990
A. Braga 0000-0002-2942-6182
E. Araujo Júnior 0000-0002-6145-2532
E. Traina 0000-0002-6856-8327
C. M. Ponte Ribeiro 0009-0008-0758-0577
S. Y. Sun 0000-0001-6573-7386
Submitted/Doručeno: 11. 9. 2024
Accepted/Přijato: 6. 1. 2025
Prof. Edward Araujo Júnior, MD, PhD
Rua Belchior de Azevedo
156 apto. 111 Torre Vitoria
Vila Leopoldina
CEP 05089-030
São Paulo-SP, Brazil
araujojred@terra.com.br
Štítky
Dětská gynekologie Gynekologie a porodnictví Reprodukční medicínaČlánek vyšel v časopise
Česká gynekologie
2025 Číslo 2
- Vědecké poznatky rozptylující obavy spojené s používáním nitroděložní antikoncepce i u mladých žen
- Používání intrauterinních tělísek uvolňujících měď a riziko tubární infertility u nuligravidních žen
- Účinnost dlouhodobě působící reverzibilní antikoncepce
- Antikoncepční pilulka přestává být nejpřitažlivější metodou antikoncepce
- Nitroděložní systém s levonorgestrelem by mohl snižovat riziko adenokarcinomu endometria
Nejčtenější v tomto čísle
- Comparison of perinatal outcomes using oral misoprostol, vaginal misoprostol, and intracervical dinoprostone for induction of labor
- Sister Mary Joseph’s nodule – rare umbilical cutaneous metastasis
- Occupational therapy in oncogynecology – a pilot study
- Sclerotherapy of endometrioma and its impact on ovarian reserve – a narrative review
Zvyšte si kvalifikaci online z pohodlí domova
Mazová zátka a její řešení
nový kurzVšechny kurzy