
The Effect of Sitagliptin on Carotid Artery Atherosclerosis in Type 2 Diabetes: The PROLOGUE Randomized Controlled Trial
In a randomized controlled trial, Koichi Node and colleagues assess the efficacy of sitagliptin in limiting atherosclerosis among patients over 29 years of age living in Japan.
Published in the journal:
. PLoS Med 13(6): e32767. doi:10.1371/journal.pmed.1002051
Category:
Research Article
doi:
https://doi.org/10.1371/journal.pmed.1002051
Summary
In a randomized controlled trial, Koichi Node and colleagues assess the efficacy of sitagliptin in limiting atherosclerosis among patients over 29 years of age living in Japan.
Introduction
Atherosclerosis, often caused by hypertension, diabetes mellitus, or dyslipidemia, causes ischemic diseases of the brain, heart, and kidney, which increase mortality and morbidity worldwide. Above all, diabetes mellitus is a critical factor in the development of vascular injury. The global prevalence of type 2 diabetes mellitus (T2DM) has been estimated to be 171 million cases, and it is projected to reach double this estimate or more by 2030 [1]. Epidemiological studies have shown that the mortality caused by T2DM is equivalent to that resulting from coronary artery disease (CAD) [2–4].
Noninvasive assessment of carotid artery intima-media thickness (IMT) is widely used to estimate not only carotid but also systemic atherosclerosis, because carotid IMT is independently associated with both the presence of CAD [5–8] and the occurrence of cardiovascular events [9,10], including after adjustment for conventional cardiovascular risk factors. It has also been suggested that an increased carotid IMT is strongly associated with the presence of CAD in people with T2DM [11]. Therefore, evaluation of carotid IMT is helpful when treating people with T2DM.
Dipeptidyl peptidase-4 (DPP-4) inhibitors are antihyperglycemic drugs that stimulate insulin release from pancreatic β-cells by sparing incretin hormones, such as glucagon-like peptide-1 (GLP-1), from degradation by DPP-4. GLP-1 analogues and DPP-4 inhibitors have also been shown to have extra-pancreatic effects beyond glycemic control, including anti-atherosclerotic properties [12,13]. Previous meta-analyses of DPP-4 inhibitors in cardiovascular diseases have demonstrated decreases in cardiovascular events [14,15], while large-scale clinical trials have found that DPP-4 inhibitors neither increased nor decreased the onset of cardiovascular events [16–18]. The SAVOR-TIMI 53 trial reported a significant 27% increase in the incidence of hospitalization for heart failure [16], indicating that it is unclear whether DPP-4 inhibitors have a cardioprotective effect in the clinical setting. Moreover, the anti-atherosclerotic effects of DPP-4 inhibitors are not yet fully clarified. We designed the PROLOGUE (Program of Vascular Evaluation under Glucose Control by DPP-4 Inhibitor) study to investigate the effect of sitagliptin on carotid IMT in people with T2DM.
Methods
Study Design and Participants
The rationale and design of the PROLOGUE study have already been described [19]. The study was a multicenter PROBE (prospective, randomized, open label, blinded endpoint) trial carried out in 48 Japanese medical centers. The study protocol and all amendments were reviewed and approved by each center’s ethics committee (S1 and S2 Texts). The study was conducted in accordance with the ethical principles of the Declaration of Helsinki and conformed with good clinical practices and applicable regulatory requirements. All participants gave written consent to participate after having been informed about the nature and purpose of the study, the participation/termination conditions, and the possible risks and benefits of treatment.
We enrolled 463 people with T2DM between November 2010 and September 2012. The inclusion criteria were age ≥ 30 y and presence of T2DM with HbA1c ≥ 6.2% and < 9.4% despite treatment with diet, exercise, and/or conventional antidiabetic agents. The exclusion criteria were as follows: type 1 diabetes mellitus; undergoing insulin treatment; administration of DPP-4 inhibitors and/or GLP-1 analogues before randomization; heart failure with New York Heart Association functional class III or IV; a history of diabetic ketoacidosis or diabetic coma within the 6 mo prior to randomization; a history of myocardial infarction, angina pectoris, percutaneous transluminal coronary angioplasty, or bypass surgery; a history of cerebral infarction, cerebral hemorrhage, subarachnoid hemorrhage, or transient ischemic attack within the 3 mo prior to randomization; serious renal dysfunction (estimated glomerular filtration rate < 30 ml/min/1.73 m2 or dialysis); pregnancy or possible pregnancy; lack of informed consent; and judgment of the investigator that an individual is ineligible for inclusion in the study.
Following the initial echocardiographic estimation of carotid IMT, eligible participants were randomly assigned (ratio 1:1) either to receive conventional therapy plus sitagliptin (sitagliptin group) or to continue with only conventional therapy (diet, exercise, and/or antidiabetic agents, except for DPP-4 inhibitors, GLP-1 analogues, and insulin; conventional therapy group). The randomization was done at the PROLOGUE data center using a modified minimization method with a biased-coin assignment balancing on age (<65 or ≥65 y), sex, use of statins, use of antidiabetic agents (nonpharmacological or pharmacological), HbA1c (<7.0% or ≥7.0%), office systolic blood pressure (<135 or ≥135 mm Hg), and maximum IMT (<1.0 or ≥1.0 mm). The random allocation with a stratified technique was generated automatically by a centralized web-based tool that could not be influenced by the researchers. The treatment target level of HbA1c in both groups was <6.2%. All participants were followed annually for 2 y until September 2014 (S1 Fig).
Measurement of Carotid Intima-Media Thickness
Carotid ultrasound examinations were performed within 1 mo prior to study inclusion, and at 12 and 24 mo after randomization. High-resolution carotid ultrasonography was performed in each ultrasound laboratory in a blinded manner using standardized imaging protocols by expert sonographers trained in the measurement of carotid IMT [20]. All ultrasound systems were equipped with linear transducers of more than 7.5 MHz. Longitudinal B-mode images, perpendicular to the ultrasound beam, with a 4-cm imaging depth, were obtained from the distal common carotid arteries (CCAs), bulbs, and proximal internal carotid arteries (ICA) on both sides. The lateral probe incidence was used to obtain CCA images, using external landmarks with an original semicircular protractor developed for the purpose. The IMT primary parameter measured and calculated was change in the mean far wall CCA IMT in the right and left CCAs 10 mm from the bulb. In addition, the following far wall IMTs were measured: the maximum IMT of the CCA, the mean of the mean IMTs of the CCA, bulb, and ICA, and the mean of the maximum IMTs of the CCA, bulb, and ICA. We used the method recommended by the Mannheim carotid IMT consensus [21]. Plaque was defined as the presence of focal wall thickening at least 50% greater than that of the surrounding vessel wall, or as a focal region with IMT > 1.1 mm protruding into the lumen and distinct from the adjacent boundary. The plaque gray scale median [22] and plaque area far and near to the wall were also measured. If there were multiple carotid plaques in participants, the most echolucent one was selected for measurement of plaque area and gray scale value. The optimized R-wave-gated still frames of the carotid IMT were stored as JPEG files, and all parameters were measured in a core laboratory (University of Tsukuba). A single expert analyst who was unaware of the clinical information of the participants measured all the IMT values using an automatic IMT measurement software program in a blinded manner (Vascular Research Tools 5, Medical Imaging Applications) [23]. The analyst selected the best images of the right and left CCA, bulb, and ICA. In this region, the software identified the lumen/intima and the media/adventitia borders, and calculated the distance between them.
Endpoints
The primary endpoint was the percentage change in mean CCA IMT at 24 mo after randomization. The secondary endpoints, at 12 and 24 mo, were (1) the mean and maximum IMT values and changes at the CCA, bulb, and ICA (except for the primary endpoint); (2) plaque area and plaque gray scale median; (3) the values and changes in glycemic profiles (HbA1c, fasting glucose level, insulin concentration, 1,5-anhydroglucitol,1,4-anhydro-D-glucitol, HOMA-β, HOMA-R); lipoprotein profiles (total cholesterol, high-density lipoprotein cholesterol, triglyceride, small dense low-density lipoprotein, malondialdehyde-modified low-density lipoprotein, remnant-like particle cholesterol); renal function (creatinine, cystatin C, urinary albumin/creatinine ratio, estimated glomerular filtration rate); high molecular weight adiponectin; physiological parameters (body weight, blood pressure); and (4) adjudicated clinical events and adverse events.
Statistical Analysis
Based on previous reports, we assumed that the annual change in mean CCA IMT would be −0.005 mm/y in the sitagliptin group and +0.005 mm/y in the conventional therapy group [24,25]. The necessary sample size was calculated on the assumption of a 0.01-mm group difference in the primary endpoint at the final assessment, with a standard deviation (SD) of 0.06 for individual differences and 80% power for a two-sided, two-sample t-test at a 0.05 significance level. The target sample size was set at 567 participants per group in anticipation of a 20% dropout rate, with total sample size at 1,200 participants. However, as there has been increasing evidence that DPP-4 inhibitors can reduce HbA1c safely and adequately, they have been quite widely prescribed in Japan. As a consequence, it was difficult to recruit participants who were not taking them, and also to continue the trial without prescribing them. Based on these circumstances, we recalculated the necessary sample size assuming that DPP-4 inhibitors have protective effects similar to those of thiazolidine derivatives, which were reported to prevent carotid intima-media thickening in the CHICAGO study [26]. In the sample size recalculation, we assumed a 0.02-mm group difference with an SD of 0.06 for individual differences and 80% power for a two-sided, two-sample t-test at a 0.05 significance level. The target sample size was re-estimated at 238 participants per group in anticipation of a 20% dropout rate, and the total sample size was set at 500 in June 2012. An interim analysis was done for the purpose of investigating futility or overwhelming efficacy of the study and was performed by an independent data monitoring committee at 1 y after the completion of enrollment. The investigators and participants remained blinded to the results of this interim analysis. Significance was evaluated using the Pocock method (with the stopping boundary p ≤ 0.0311 at the first interim analysis), resulting in approval of study continuation.
The data for the primary and secondary endpoints were collected at each time point. The statistical analysis and reporting of this trial were conducted in accordance with the CONSORT guidelines, with the primary analyses based on the intention to treat principle (S3 Text). For the baseline variables, summary statistics were constructed employing frequencies and proportions for categorical data and mean and SD for continuous variables. The baseline variables were compared using Fisher’s exact test for categorical outcomes and unpaired t-tests for continuous variables, as appropriate.
For the primary analysis comparing the treatment effects, the baseline-adjusted means and their 97.2% CIs, estimated by analysis of covariance (ANCOVA), for the change in average carotid IMT at 24 mo were compared between the treatments (sitagliptin group versus conventional therapy group). This analysis was carried out taking into account the variation caused by treatment effects, and using age, sex, statin use, prerandomization treatment type, baseline HbA1c, baseline office systolic blood pressure, and baseline maximum IMT as covariates. The significance level of the final analysis was set at 0.0277 (two-sided). We did not impute missing observations for the primary analysis, but the mixed-effects model for repeated measures was applied as a sensitivity analysis to examine the effect of missing data. The secondary analyses were performed in the same manner as the primary analysis. The baseline-adjusted means of the secondary endpoints at each time point were estimated by ANCOVA with treatment effects, age, sex, statin usage, pre-randomization treatment type, baseline HbA1c, baseline office systolic blood pressure, and the baseline value of the secondary efficacy parameter as covariates.
All comparisons were planned, and all p-values were two-sided. A p-value < 0.05 was considered statistically significant. All statistical analyses were performed using SAS, version 9.4 (SAS Institute).
Study Management
The organization of the study is detailed in S4 Text. A steering committee was responsible for the study design and scientific execution. An independent efficacy and safety evaluation committee, consisting of six members blinded to any information related to group allocation, evaluated each clinical and adverse event. The independent data monitoring committee, composed of three members, independently reviewed the interim analysis to advise whether it was appropriate to continue the study. An independent audit team inspected several main medical centers to ensure the quality of the data. All medical centers participating in this study are listed in S4 Text. Changes in the protocol, including definition of the primary endpoint, change of sample size, and enforcement of interim analysis, are described in S2 Text.
Data for this study were deposited in the Dryad Digital Repository [27].
Results
Study Population
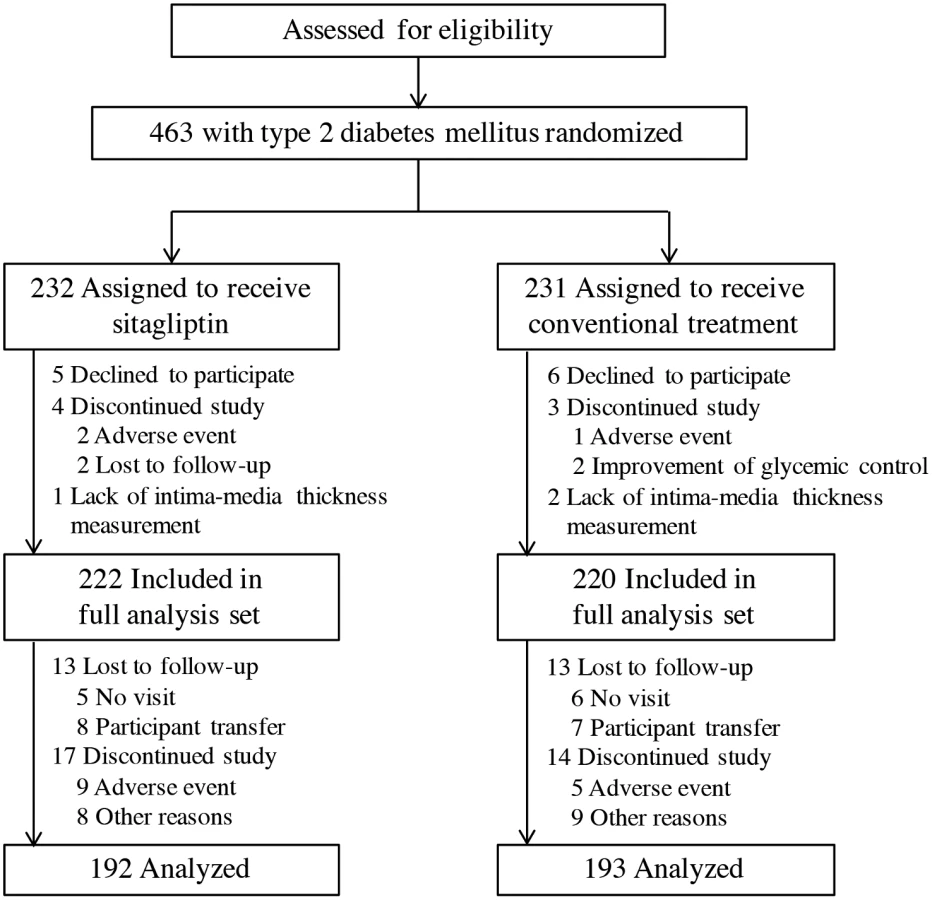
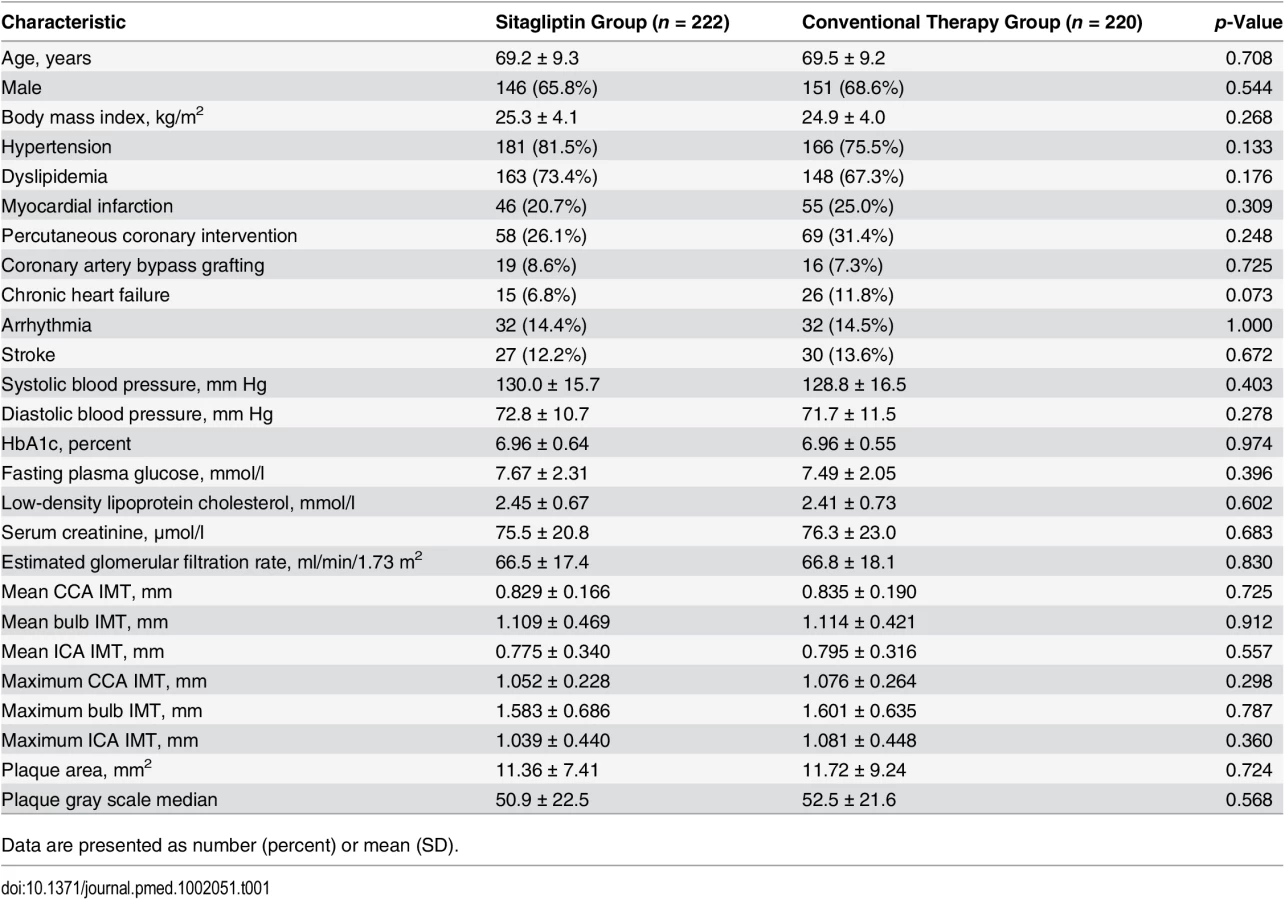
In all, 463 people with T2DM were enrolled and randomly assigned to the two groups (232 and 231 to the sitagliptin and conventional therapy groups, respectively). We obtained complete endpoint information at the end of the study for 222 participants in the sitagliptin group and 220 participants in the conventional therapy group (Fig 1). There were no significant differences in baseline characteristics between the two groups (Table 1).
Carotid Intima-Media Thickness
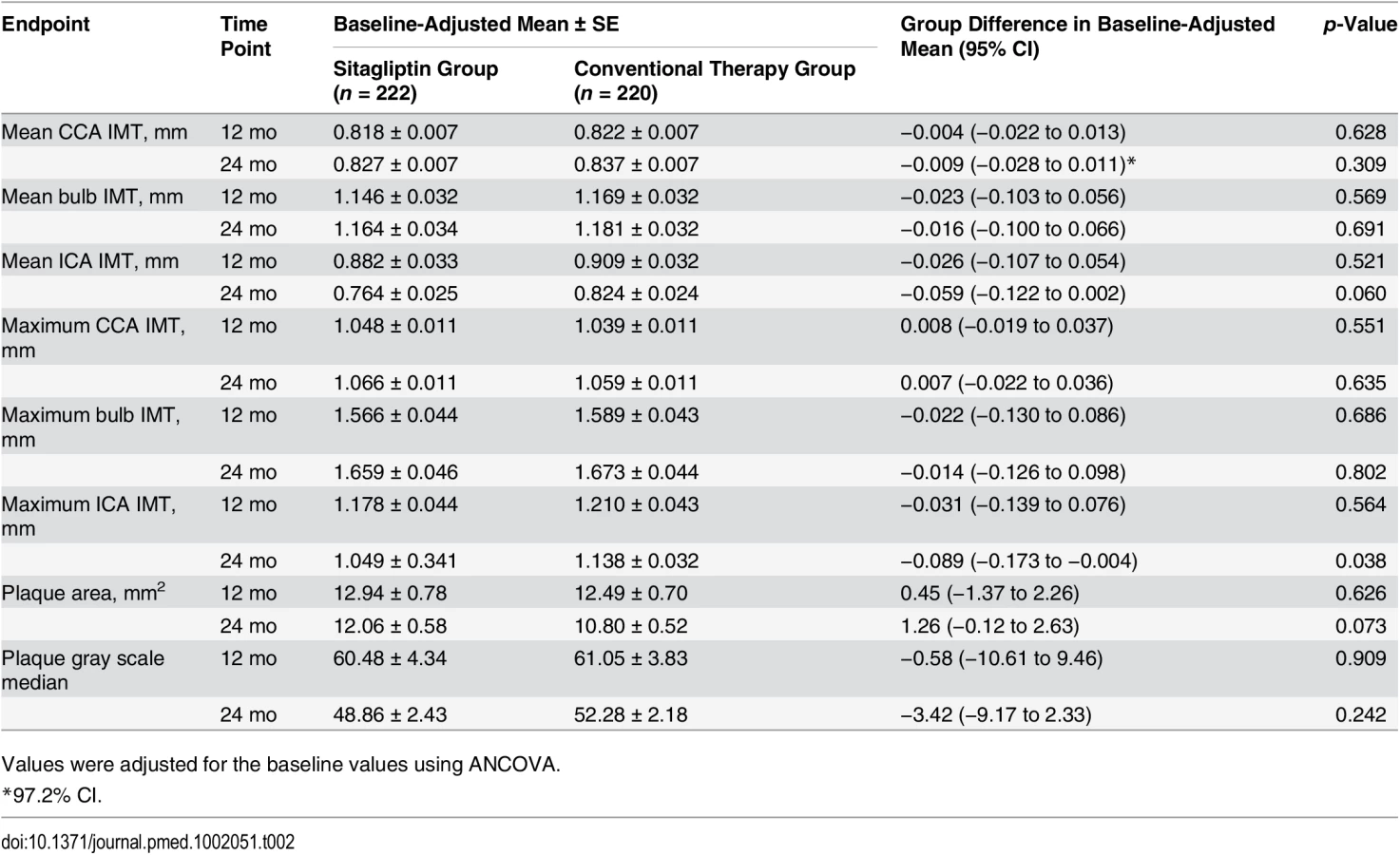
At baseline, the mean CCA IMT (± SD) was 0.829 ± 0.166 mm in the sitagliptin group and 0.835 ± 0.190 mm in the conventional therapy group (Table 1). The baseline-adjusted mean (± standard error [SE]) CCA IMT at 24 mo in the sitagliptin and conventional therapy groups was 0.827 ± 0.007 mm and 0.837 ± 0.007 mm, respectively, with a mean difference of −0.009 mm (97.2% CI −0.028 to 0.011, p = 0.309). Although the change in maximum ICA IMT at 24 mo was significantly greater in the sitagliptin group (p = 0.038), the values of mean bulb IMT, mean ICA IMT, maximum CCA IMT, maximum bulb IMT, plaque area, and plaque gray scale median at 24 mo did not differ significantly between the two groups at any time point (Table 2).
The effect of sitagliptin on carotid IMT in older participants (≥70 y) was evaluated (S1 Table). However, there was no statistically significant difference in effect between the older and younger participants. Accordingly, the results did not depend on the age of the participants.
Glucose Metabolism and Other Parameters
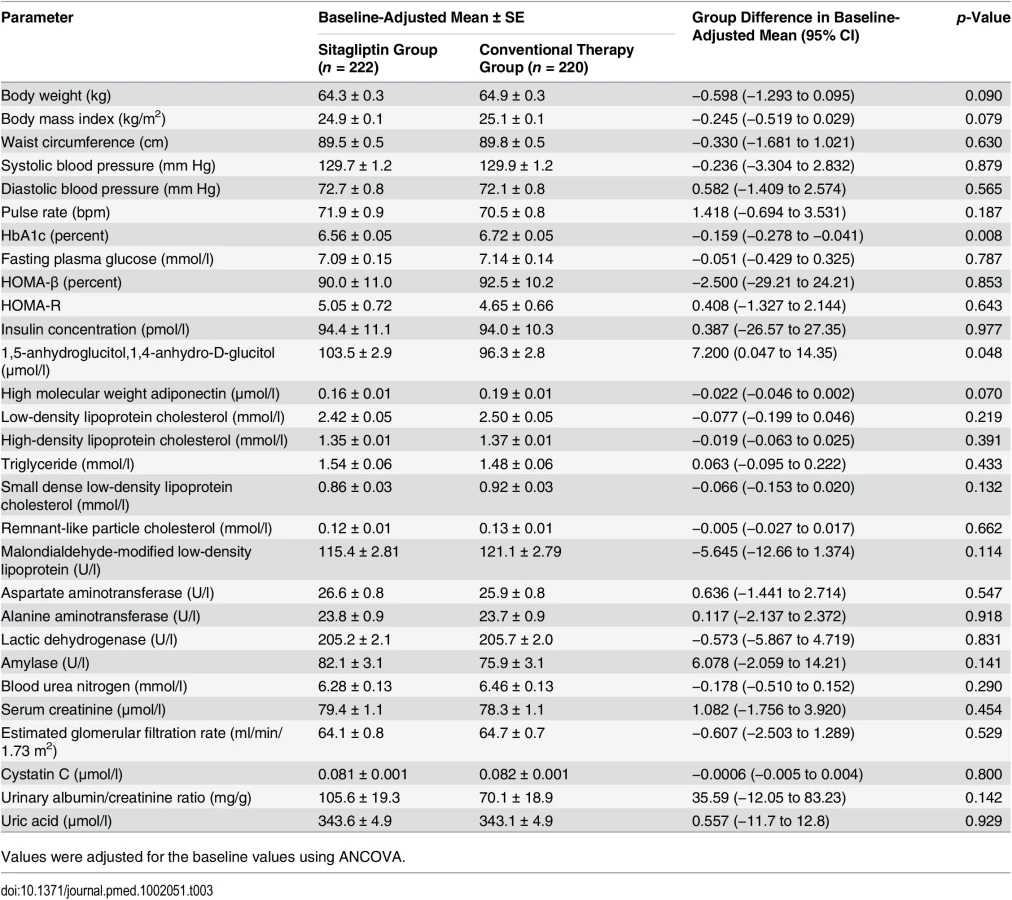
The baseline levels of HbA1c were 6.96% ± 0.64% and 6.96% ± 0.55% in the sitagliptin and conventional therapy groups, respectively (mean ± SD; Table 1). The baseline-adjusted mean (± SE) at each time point and the change in HbA1c level are shown in Tables S2 and 3. HbA1c level decreased to 6.56% ± 0.04% in the sitagliptin group and to 6.67% ± 0.04% in the conventional therapy group at 12 mo (p = 0.047), and to 6.56% ± 0.05% in the sitagliptin group and 6.72% ± 0.05% in the conventional therapy group at 24 mo (p = 0.008). While the change in 1,5-anhydroglucitol,1,4-anhydro-D-glucitol at 24 mo in the conventional therapy group was significantly greater than that in the sitagliptin group (p = 0.048), there was no significant difference between the groups in fasting plasma glucose at 24 mo (p = 0.787). There were no significant differences between the two groups in changes in the other parameters, including body weight, blood pressure, renal function, and metabolic and lipid profiles.
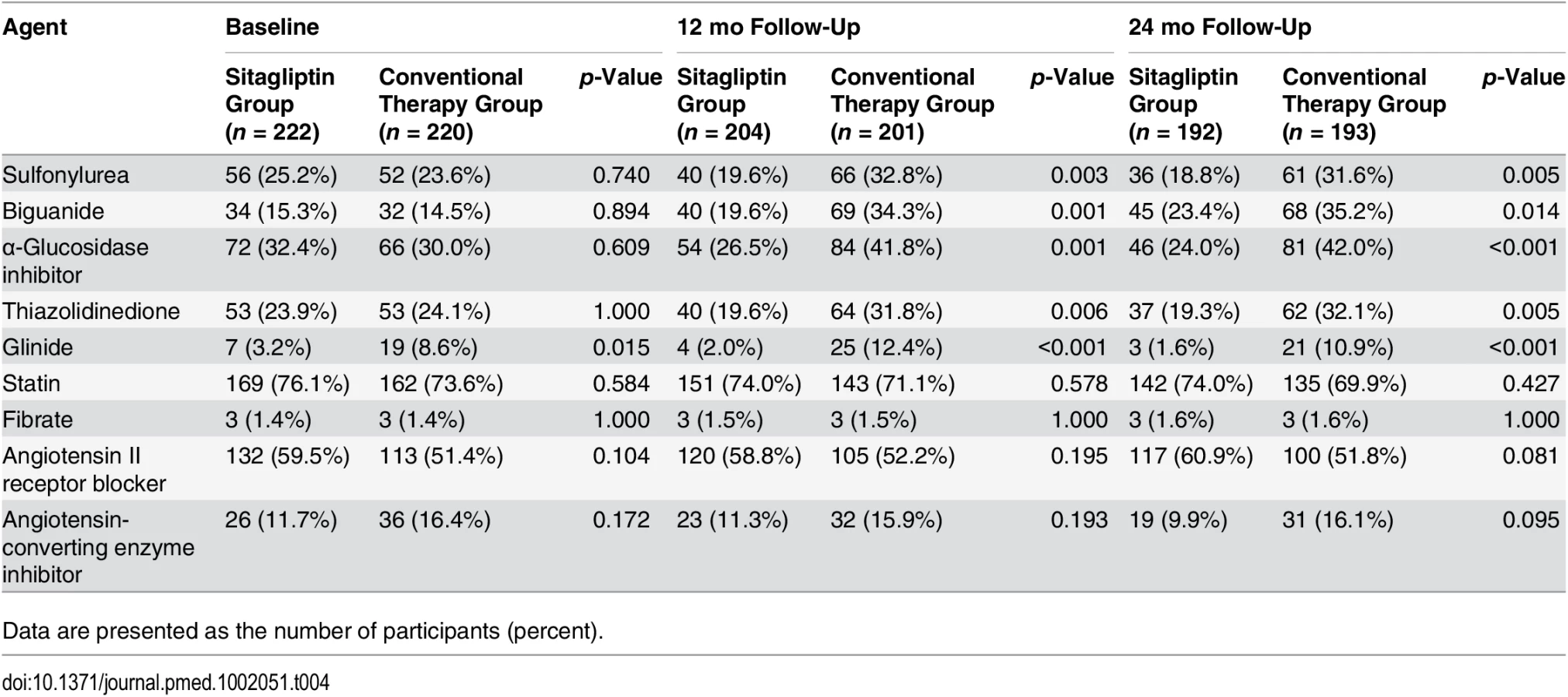
In the conventional therapy group, the additional use of a sulfonylurea, biguanide, α-glucosidase inhibitor, or thiazolidinedione for the management of glycemic control increased during the 24-mo observation period. Conversely, the usage of other antidiabetic agents, except for biguanide drugs, did not increase in the sitagliptin group (Table 4). The average dose of sitagliptin was 48 ± 8 mg at baseline, 62 ± 24 mg at 12 mo, and 64 ± 26 mg at 24 mo (S3 Table).
In each participant, adherence to medications was monitored by counting the residual number of tablets at each clinic visit. If the average daily consumption of all tablets combined in a participant was less than 75% of that prescribed, the participant was defined as having “poor adherence” at the end of the study. There were seven such participants in the sitagliptin group, and nine in the conventional therapy group.
Adjudicated Clinical and Adverse Events
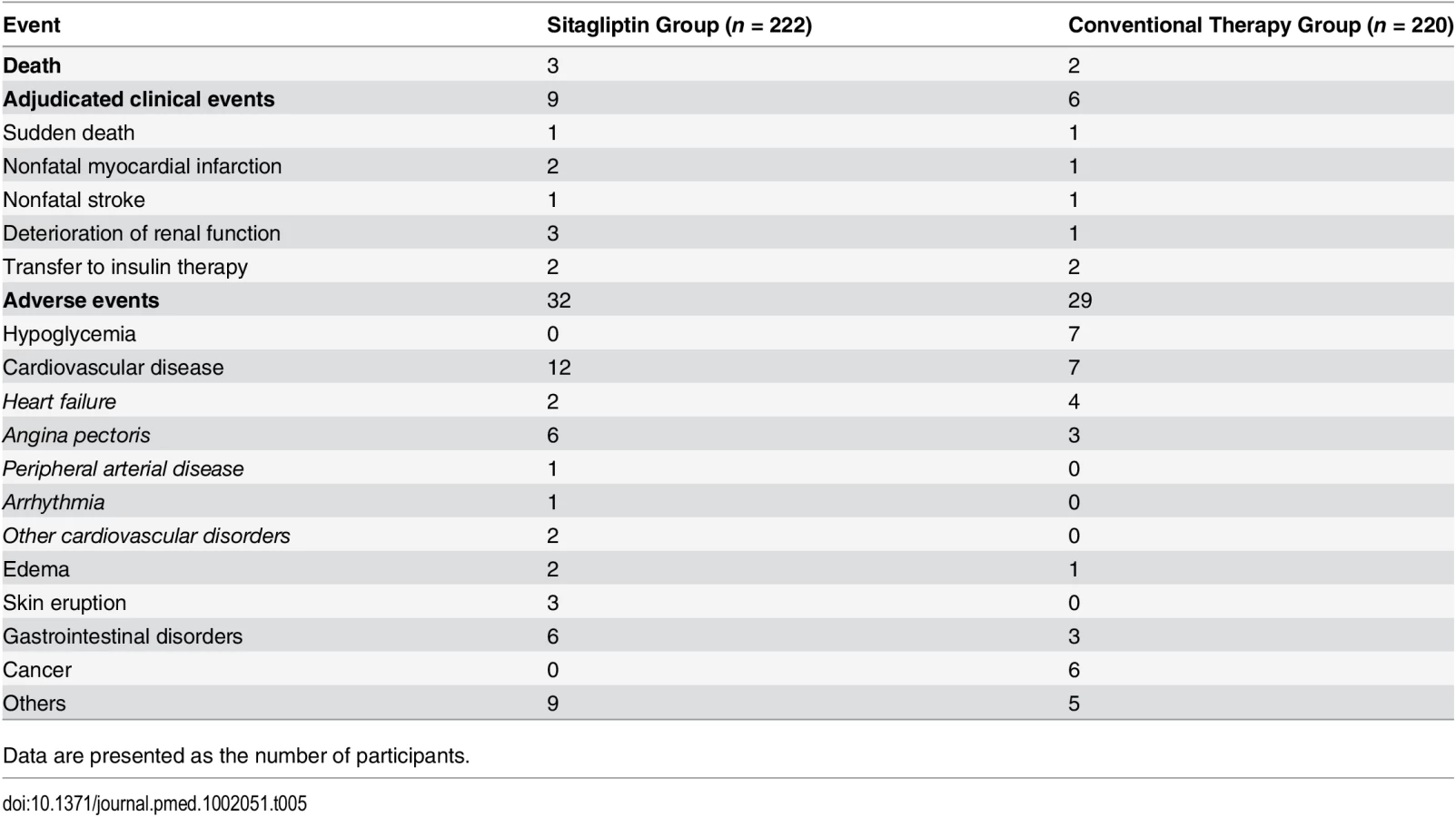
During the 24 mo of follow-up, five participants died, three in the sitagliptin group and two in the conventional therapy group (nontuberculous mycobacterial infection, multiple organ failure following bone fracture, coma of unknown cause, or sudden death); sudden death occurred in one participant in each group. Nonfatal myocardial infarction occurred in two participants in the sitagliptin group and in one in the conventional therapy group. Nonfatal stroke occurred in one participant in each group. Two participants in each group initiated insulin therapy. Deterioration of renal function, defined as a greater than 2-fold increase in serum creatinine level, was seen in three participants in the sitagliptin group and in one in the conventional therapy group. Hypoglycemia, which is one of the most clinically important adverse events, was recorded only in the conventional therapy group. Heart failure occurred in two participants in the sitagliptin group and in four in the conventional therapy group. Acute pancreatitis and pancreatic cancer were not observed in either group (Table 5).
Discussion
Main Findings
To our knowledge, the PROLOGUE study is the largest trial to investigate whether DPP-4 inhibitors slow the progression of carotid IMT in participants with T2DM. The major finding of the study is that the serial change in mean CCA IMT was not significantly different between conventional treatment plus sitagliptin and conventional treatment alone. The change in HbA1c was significantly greater in the sitagliptin group. These results suggest that sitagliptin failed to inhibit IMT progression relative to conventional therapy despite its glucose-lowering effect.
Intima-Media Thickness in People with Type 2 Diabetes Mellitus
The primary endpoint of carotid IMT in this study, which can be evaluated noninvasively using ultrasonography, reflects atherosclerotic status and has been used to predict the risk of myocardial infarction and stroke [28]. A positive association exists between carotid IMT and subsequent cardiovascular events in the general population, independent of other major risk factors [29]. A single measurement of carotid IMT and assessment of carotid plaque increases the predictive power of cardiovascular disease risk assessment [30–35]. Accordingly, the American College of Cardiology Foundation/American Heart Association guidelines [36] give carotid IMT and plaque measurement for cardiovascular risk stratification as a class IIA recommendation. Repeated carotid IMT measurements are an accepted approach to test the effects of interventions on carotid IMT progression. The Multi-Ethnic Study of Atherosclerosis [31] showed a positive association between carotid IMT progression and stroke incidence. Although two meta-regression analyses of clinical trial data [37,38] reported conflicting results on the relationship between carotid IMT progression and cardiovascular events, many reports have supported its use in pathophysiological studies and clinical trials, such that the perception of carotid IMT has shifted from that of a secondary endpoint to that of a surrogate marker of the risk of cardiovascular events for evaluating therapeutic interventions in atherosclerotic disease [39,40]. It was on this basis that we undertook the PROLOGUE study to determine whether treatment with a DPP-4 inhibitor, sitagliptin, is more effective than conventional therapy at inhibiting atherosclerotic progression in Japanese people, using carotid IMT as a surrogate marker. Measurement of carotid IMT in a blinded manner and in a core laboratory—as done in this study—avoids bias, improves accuracy, enhances the credibility of image assessments, and ensures consistency. A highly standardized imaging acquisition protocol in a fully blinded manner is recommended [41].
In the CHICAGO (Carotid Intima-Media Thickness in Atherosclerosis Using Pioglitazone) trial, the inhibitory effect of 15–45 mg/d of pioglitazone on mean CCA IMT progression was evident during 18 mo of observation, in comparison with 1–4 mg/d glimepiride [26]. Other investigators also demonstrated that pioglitazone slowed the progression of carotid IMT compared with glimepiride [35,42]. In addition to pioglitazone, a biguanide that has been suggested to inhibit DPP-4 activity and increase GLP-1 concentration [43,44] also reduced the progression of carotid IMT [45,46]. In studies of small numbers of people, DPP-4 inhibitors including sitagliptin were reported to inhibit the progression of carotid IMT [47,48]. The SPEAD-A study revealed that treatment with alogliptin, the other DPP-4 inhibitor, attenuated the progression of carotid IMT compared with conventional treatment during 24 mo of follow-up [49]. More recently, the SPIKE trial demonstrated that sitagliptin attenuated carotid IMT in people with T2DM who were under treatment with insulin [50]. However, compared with these studies showing positive results, in the PROLOGUE study the change in mean CCA IMT in the sitagliptin group did not differ significantly from that in the conventional therapy group. Participants on insulin treatment were excluded from the present study, HbA1c values at baseline were lower (PROLOGUE study: 6.96% [sitagliptin], 6.96% [conventional]; SPEAD-A study: 7.3% [alogliptin], 7.2% [conventional]; SPIKE trial: 8.1% [sitagliptin], 8.0% [conventional]), and the difference between the treatment groups in the change in HbA1c over 24 mo was smaller (PROLOGUE study: 0.14%; SPEAD-A study: 0.2%; SPIKE trial: 0.3%). In addition, the prevalence of statin use was higher in the PROLOGUE study than in the SPEAD-A study and the SPIKE trial (PROLOGUE study: 76.1% [sitagliptin], 73.6% [conventional]; SPEAD-A study: 38% [alogliptin], 46% [conventional]; SPIKE trial: 48% [sitagliptin], 46% [conventional]) [49,50]. Thus, it may not be appropriate to directly compare these different results, as the baseline characteristics of the participants, such as severity of T2DM, HbA1c level, and carotid IMT, differed between them. In the PROLOGUE study, even in the conventional therapy group mean CCA IMT had increased only slightly at 24 mo, which seems to be lower than values reported previously. It has been reported that the annual progression of carotid IMT in Japanese people with T2DM is 0.016 to 0.035 mm [25,51] even with aggressive antidiabetic treatment. In the CHICAGO study, the glimepiride arm showed a 0.012-mm increase in mean CCA IMT during 18 mo of follow-up. Interestingly, in the PROLOGUE study additional use of both pioglitazone and biguanides increased in the conventional therapy group, possibly contributing to the suppression of IMT progression. Additionally, both the sitagliptin and conventional treatment groups achieved strict overall management of risk factors, including glycemic control, although the reduction of HbA1c was greater in the sitagliptin group than in the conventional therapy group. On these grounds, the progression of carotid IMT might be inhibited in both groups, in contrast to previous reports [25,26,47–51].
DPP-4 Inhibitors and Cardiovascular Disease
There are published experimental data showing that incretin therapy, including treatment with GLP-1 analogues or DPP-4 inhibitors, attenuates atherosclerosis. GLP-1 and its analogues inhibit the inflammatory and atherogenic pathways induced by exogenous stimulation with oxidative stress and/or inflammation in vitro [52–55]. In vivo studies have revealed that the administration of GLP-1 analogues or DPP-4 inhibitors reduces high-fat-diet-induced atherosclerosis and stabilizes plaques in apoE knockout mice [55–57]. In the clinical setting, several investigators have demonstrated that GLP-1 analogues or DPP-4 inhibitors improve endothelial function in people with T2DM [58,59]. These lines of evidence suggest that sitagliptin may have beneficial effects on atherosclerosis in humans. Large-scale randomized clinical trials found that DPP-4 inhibitors were safe and effective in the treatment of T2DM. However, they did not reduce cardiovascular events in participants with T2DM who were at high risk for cardiovascular disease or who had a recent onset of acute coronary syndrome [16–18]. In the TECOS trial [18], sitagliptin had no effect on cardiovascular events in participants with T2DM. The discrepancy between the experimental data and recent clinical results requires explanation. One possibility is that the period of observation in clinical studies may have been too short to evaluate the clinical effects of sitagliptin. Efficacy against cardiovascular events can be demonstrated over several years, according to the VADT study and the UK Prospective Diabetes Study. The TECOS trial was designed to show noninferiority for cardiovascular events with sitagliptin. Therefore, we had to clarify the precise effects of sitagliptin on atherosclerosis directly to evaluate carotid IMT. In the PROLOGUE study, intima-media thickening did not differ significantly between the sitagliptin and conventional therapy groups during 24 mo of follow-up.
In experimental research in patients with T2DM, comparisons of drugs are relatively simple and their doses are sometimes much greater than those used in clinical practice. Usually people are also taking other drugs, including antidiabetic, antihypertensive, or lipid-lowering drugs, and it is difficult to exclude their influence. Indeed, the use of thiazolidinediones and biguanides increased as co-therapies in the conventional therapy group in our study (Table 4), which may have diminished the effect of the DPP-4 inhibitor. Moreover, better glycemic control can now be achieved compared with several years ago. This may be the reason why carotid IMT in the conventional therapy group did not increase as much as anticipated. We emphasize that the true purpose of the present study was not to elucidate whether sitagliptin can prevent carotid IMT compared with a placebo, but to investigate whether sitagliptin can confer an additional beneficial effect on carotid IMT in clinical practice.
Study Limitations
The PROLOGUE study has a few limitations. First, it was conducted with a PROBE design, which might have introduced bias in the assessment of outcomes. Although the primary endpoint was measured by a single observer in a core laboratory who was blinded to the treatment assignments, open-label treatments might affect physicians’ choices of therapy. Second, baseline HbA1c level and carotid IMT were not very high—probably because participants’ diabetes was well-controlled without insulin treatment—in comparison with previous clinical studies that assessed the additional effects of sitagliptin on carotid atherosclerosis relative to conventional antidiabetic drugs [50].
In conclusion, the PROLOGUE study did not provide evidence that treatment with sitagliptin has an additional effect on the progression of carotid IMT in participants with T2DM beyond that achieved with conventional treatment.
Supporting Information
{kind=link}
Zdroje
1. Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care. 2004;27:1047–1053. 15111519
2. Juutilainen A, Lehto S, Rönnemaa T, Pyörälä K, Laakso M. Type 2 diabetes as a “coronary heart disease equivalent”: an 18-year prospective population-based study in Finnish subjects. Diabetes Care. 2005;28:2901–2907. 16306552
3. Haffner SM, Lehto S, Rönnemaa T, Pyörälä K, Laakso M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med. 1998;23;339:229–234. 9673301
4. Whiteley L, Padmanabhan S, Hole D, Isles C. Should diabetes be considered a coronary heart disease risk equivalent?: results from 25 years of follow-up in the Renfrew and Paisley survey. Diabetes Care. 2005;28:1588–1593. 15983305
5. Craven TE, Ryu JE, Espeland MA, Kahl FR, McKinney WM, Toole JF, et al. Evaluation of the associations between carotid artery atherosclerosis and coronary artery stenosis. A case-control study. Circulation. 1990;82:1230–1242. 2205416
6. Handa N, Matsumoto M, Maeda H, Hougaku H, Ogawa S, Fukunaga R, et al. Ultrasonic evaluation of early carotid atherosclerosis. Stroke. 1990;21:1567–1572. 2237950
7. Smith GD, Shipley MJ, Rose G. Intermittent claudication, heart disease risk factors, and mortality. The Whitehall Study. Circulation. 1990;82:1925–1931. 2242518
8. Khoury Z, Schwartz R, Gottlieb S, Chenzbraun A, Stern S, Keren A. Relation of coronary artery disease to atherosclerotic disease in the aorta, carotid, and femoral arteries evaluated by ultrasound. Am J Cardiol. 1997;80:1429–1433. 9399716
9. Chambless LE, Heiss G, Folsom AR, Rosamond W, Szklo M, Sharrett AR, et al. Association of coronary heart disease incidence with carotid arterial wall thickness and major risk factors: the Atherosclerosis Risk in Communities (ARIC) Study, 1987–1993. Am J Epidemiol. 1997;146:483–494. 9290509
10. Salonen JT, Salonen R. Ultrasound B-mode imaging in observational studies of atherosclerotic progression. Circulation. 1993;87:II56–II65. 8443925
11. Kasami R, Kaneto H, Katakami N, Sumitsuji S, Yamasaki K, Kuroda T, et al. Relationship between carotid intima-media thickness and the presence and extent of coronary stenosis in type 2 diabetic patients with carotid atherosclerosis but without history of coronary artery disease. Diabetes Care. 2011;34:468–470. doi: 10.2337/dc10-1222 21270201
12. Sivertsen J, Rosenmeier J, Holst JJ, Vilsbøll T. The effect of glucagon-like peptide 1 on cardiovascular risk. Nat Rev Cardiol. 2012;9:209–222. doi: 10.1038/nrcardio.2011.211 22290234
13. Chrysant SG, Chrysant GS. Clinical implications of cardiovascular preventing pleiotropic effects of dipeptidyl peptidase-4 inhibitors. Am J Cardiol. 2012;109:1681–1685. doi: 10.1016/j.amjcard.2012.01.398 22425330
14. Monami M, Ahrén B, Dicembrini I, Mannucci E. Dipeptidyl peptidase-4 inhibitors and cardiovascular risk: a meta-analysis of randomized clinical trials. Diabetes Obes Metab. 2013;15:112–120. doi: 10.1111/dom.12000 22925682
15. Patil HR, Al Badarin FJ, Al Shami HA, Bhatti SK, Lavie CJ, Bell DS, et al. Meta-analysis of effect of dipeptidyl peptidase-4 inhibitors on cardiovascular risk in type 2 diabetes mellitus. Am J Cardiol. 2012;110:826–833. doi: 10.1016/j.amjcard.2012.04.061 22703861
16. Scirica BM, Bhatt DL, Braunwald E, Steg PG, Davidson J, Hirshberg B, et al. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N Engl J Med. 2013;369:1317–1326. doi: 10.1056/NEJMoa1307684 23992601
17. White WB, Cannon CP, Heller SR, Nissen SE, Bergenstal RM, Bakris GL, et al. Alogliptin after acute coronary syndrome in patients with type 2 diabetes. N Engl J Med. 2013;369:1327–1335. doi: 10.1056/NEJMoa1305889 23992602
18. Green JB, Bethel MA, Armstrong PW, Buse JB, Engel SS, Garg J, et al. Effect of sitagliptin on cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2015;373:232–242. doi: 10.1056/NEJMoa1501352 26052984
19. Oyama J, Ishizu T, Sato Y, Kodama K, Bando YK, Murohara T, et al. Rationale and design of a study to evaluate the effects of sitagliptin on atherosclerosis in patients with diabetes mellitus: PROLOGUE study. Int J Cardiol. 2014;174:383–384. doi: 10.1016/j.ijcard.2014.03.204 24768387
20. Stein JH, Korcarz CE, Hurst RT, Lonn E, Kendall CB, Mohler ER, et al. Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: a consensus statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Endorsed by the Society for Vascular Medicine. J Am Soc Echocardiogr. 2008;21:93–111. doi: 10.1016/j.echo.2007.11.011 18261694
21. Touboul PJ, Hennerici MG, Meairs S, Adams H, Amarenco P, Desvarieux M, et al. Mannheim intima-media thickness consensus. Cerebrovasc Dis. 2004;18:346–349. 15523176
22. Sabetai MM, Tegos TJ, Nicolaides AN, Dhanjil S, Pare GJ, Stevens JM. Reproducibility of computer-quantified carotid plaque echogenicity: can we overcome the subjectivity? Stroke. 2000;31:2189–2196. 10978050
23. Lundby-Christensen L, Almdal TP, Carstensen B, Tarnow L, Wiinberg N. Carotid intima-media thickness in individuals with and without type 2 diabetes: a reproducibility study. Cardiovasc Diabetol. 2010;9:40. doi: 10.1186/1475-2840-9-40 20727128
24. Yamasaki Y, Kodama M, Nishizawa H, Sakamoto K, Matsuhisa M, Kajimoto Y, et al. carotid intima-media thickness in Japanese type 2 diabetic subjects. Diabetes Care. 2000;9:1310–1315.
25. Kawasumi M, Tanaka Y, Uchino H, Shimizu T, Tamura Y, Sato F, et al. Strict glycemic control ameliorates the increase of carotid IMT in patients with type 2 diabetes. Endocr J. 2006;53:45–50. 16543671
26. Mazzone T, Meyer PM, Feinstein SB, Davidson MH, Kondos GT, D’Agostino RB Sr, et al. Effect of pioglitazone compared with glimepiride on carotid intima-media thickness in type 2 diabetes. JAMA. 2006;296:2572–2581. 17101640
27. Oyama J, Node K. Data from: the effect of sitagliptin on carotid artery atherosclerosis in patients with type 2 diabetes: the PROLOGUE randomized controlled trial. Dryad Digital Repository. Avaiable: http://dx.doi.org/10.5061/dryad.qt743/2.
28. Chambless LE, Folsom AR, Clegg LX, Sharrett AR, Shahar E, Nieto FJ, et al. Carotid wall thickness is predictive of incident clinical stroke: the atherosclerosis risk in communities (ARIC) study. Am J Epidemiol. 2000;151:478–487. 10707916
29. Lorenz MW, Markus HS, Bots ML, Rosvall M, Sitzer M. Prediction of clinical cardiovascular events with carotid intima-media thickness: a systematic review and meta-analysis. Circulation. 2007;115:459–467. 17242284
30. Nambi V, Chambless L, Folsom AR, He M, Hu Y, Mosley T, et al. Carotid intima-media thickness and presence or absence of plaque improves prediction of coronary heart disease risk: the ARIC (Atherosclerosis Risk In Communities) study. J Am Coll Cardiol. 2010;55:1600–1607. doi: 10.1016/j.jacc.2009.11.075 20378078
31. Polak JF, Pencina MJ, O’Leary DH, D’Agostino RB. Common carotid artery intima-media thickness progression as a predictor of stroke in multi-ethnic study of atherosclerosis. Stroke. 2011;42:3017–3021. doi: 10.1161/STROKEAHA.111.625186 21885840
32. Espeland MA, O’leary DH, Terry JG, Morgan T, Evans G, Mudra H. Carotid intimal-media thickness as a surrogate for cardiovascular disease events in trials of HMG-CoA reductase inhibitors. Curr Control Trials Cardiovasc Med. 2005;6:3. 15760471
33. Künzli N, Jerrett M, Garcia-Esteban R, Basagaña X, Beckermann B, Gilliland F, et al. Ambient air pollution and the progression of atherosclerosis in adults. PLoS ONE. 2010;5:e9096. doi: 10.1371/journal.pone.0009096 20161713
34. Hsue PY, Lo JC, Franklin A, Bolger AF, Martin JN, Deeks SG, et al. Progression of atherosclerosis as assessed by carotid intima-media thickness in patients with HIV infection. Circulation. 2004;109:1603–1638. 15023877
35. Yamasaki Y, Katakami N, Furukado S, Kitagawa K, Nagatsuka K, Kashiwagi A, et al. Long-term effects of pioglitazone on carotid atherosclerosis in Japanese patients with type 2 diabetes without a recent history of macrovascular morbidity. J Atheroscler Thromb. 2010;17:1132–1140. 20686324
36. Greenland P, Alpert JS, Beller GA, Benjamin EJ, Budoff MJ, Fayad ZA, et al. 2010 ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2010;122:e584–e636. doi: 10.1161/CIR.0b013e3182051b4c 21098428
37. Goldberger ZD, Valle JA, Dandekar VK, Chan PS, Ko DT, Nallamothu BK. Are changes in carotid intima-media thickness related to risk of nonfatal myocardial infarction? A critical review and meta-regression analysis. Am Heart J. 2010;160:701–714. doi: 10.1016/j.ahj.2010.06.029 20934565
38. Costanzo P, Perrone-Filardi P, Vassallo E, Paolillo S, Cesarano P, Brevetti G, et al. Does carotid intima-media thickness regression predict reduction of cardiovascular events? A meta-analysis of 41 randomized trials. J Am Coll Cardiol. 2010;56:2006–2020. doi: 10.1016/j.jacc.2010.05.059 21126642
39. Amarenco P, Labreuche J, Lavallee P, Touboul PJ. Statins in stroke prevention and carotid atherosclerosis: systematic review and up-to-date meta-analysis. Stroke. 2004;35:2902–2909. 15514180
40. Riccioni G. Statins and carotid intima-media thickness reduction: an up-to-date review. Curr Med Chem. 2009;16:1799–1805. 19442146
41. US Food and Drug Administration. Clinical trial imaging endpoint process standards guidance for industry. Draft guidance. 2015 Mar [cited 24 May 2016]. Available: http://www.fda.gov/downloads/drugs/guidancecomplianceregulatoryinformation/guidances/ucm268555.pdf.
42. Langenfeld MR, Forst T, Hohberg C, Kann P, Lübben G, Konrad T, et al. Pioglitazone decreases carotid intima-media thickness independently of glycemic control in patients with type 2 diabetes mellitus: results from a controlled randomized study. Circulation. 2005;111:2525–2531. 15883215
43. Green BD, Irwin N, Duffy NA, Gault VA, O’Harte FP, Flatt PR. Inhibition of dipeptidyl peptidase-IV activity by metformin enhances the antidiabetic effects of glucagon-like peptide-1. Eur J Pharmacol. 2005;547:192–199.
44. Lindsay JR, Duffy NA, McKillop AM, Ardill J, O’Harte FP, Flatt PR, et al. Inhibition of dipeptidyl peptidase IV activity by oral metformin in type 2 diabetes. Diabet Med. 2005;22:654–657. 15842525
45. Katakami N, Yamasaki Y, Hayaishi-Okano R, Ohtoshi K, Kaneto H, Matsuhisa M, et al. Metformin or gliclazide, rather than glibenclamide, attenuate progression of carotid intima-media thickness in subjects with type 2 diabetes. Diabetologia. 2004;47:1906–1913. 15565373
46. Matsumoto K, Sera Y, Abe Y, Tominaga T, Yeki Y, Miyake S. Metformin attenuates progression of carotid arterial wall thickness in patients with type 2 diabetes. Diabetes Res Clin Pract. 2004;64:225–258. 15126012
47. Ishikawa S, Shimano M, Watarai M, Koyasu M, Uchikawa T, Ishii H, et al. Impact of sitagliptin on carotid intima-media thickness in patients with coronary artery disease and impaired glucose tolerance or mild diabetes mellitus. Am J Cardiol. 2014;114:384–388. doi: 10.1016/j.amjcard.2014.04.050 24929624
48. Barbieri M, Rizzo MR, Marfella R, Boccardi V, Esposito A, Pansini A, et al. Decreased carotid atherosclerotic process by control of daily acute glucose fluctuations in diabetic patients treated by DPP-IV inhibitors. Atherosclerosis. 2013;227:349–354. doi: 10.1016/j.atherosclerosis.2012.12.018 23375680
49. Mita T, Katakami N, Yoshii H, Onuma T, Kaneto H, Osonoi T, et al. Alogliptin, a dipeptidyl peptidase 4 inhibitor, prevents the progression of carotid atherosclerosis in patients with type 2 diabetes: the Study of Preventive Effects of Alogliptin on Diabetic Atherosclerosis (SPEAD-A). Diabetes Care. 2016;39:139–148. doi: 10.2337/dc15-0781 26628419
50. Mita T, Katakami N, Shiraiwa T, Yoshii H, Onuma T, Kuribayashi N, et al. Sitagliptin attenuates the progression of carotid intima-media thickening in insulin-treated patients with type 2 diabetes: the Sitagliptin Preventive Study of Intima-Media Thickness Evaluation (SPIKE): a randomized controlled trial. Diabetes Care. 2016;39:455–464. doi: 10.2337/dc15-2145 26822324
51. Mita T, Watada H, Ogihara T, Nomiyama T, Ogawa O, Kinoshita J, et al. Eicosapentaenoic acid reduces the progression of carotid intima-media thickness in patients with type 2 diabetes. Atherosclerosis. 2007;191:162–167. 16616147
52. Shiraki A, Oyama J, Komoda H, Asaka M, Komatsu A, Sakuma M, et al. The glucagon-like peptide 1 analog liraglutide reduces TNF-α-induced oxidative stress and inflammation in endothelial cells. Atherosclerosis. 2012;221:375–382. doi: 10.1016/j.atherosclerosis.2011.12.039 22284365
53. Ishibashi Y, Matsui T, Takeuchi M, Yamagishi S. Glucagon-like peptide-1 (GLP-1) inhibits advanced glycation end product (AGE)-induced up-regulation of VCAM-1 mRNA levels in endothelial cells by suppressing AGE receptor (RAGE) expression. Biochem Biophys Res Commun. 2010;391:1405–1408. doi: 10.1016/j.bbrc.2009.12.075 20026306
54. Liu H, Dear AE, Knudsen LB, Simpson RW. A long-acting glucagon-like peptide-1 analogue attenuates induction of plasminogen activator inhibitor type-1 and vascular adhesion molecules. J Endocrinol. 2009;201:59–66. doi: 10.1677/JOE-08-0468 19136619
55. Gaspari T, Liu H, Welungoda I, Hu Y, Widdop RE, Knudsen LB, et al. A GLP-1 receptor agonist liraglutide inhibits endothelial cell dysfunction and vascular adhesion molecule expression in an ApoE-/- mouse model. Diab Vasc Dis Res. 2011;8:117–124. doi: 10.1177/1479164111404257 21562063
56. Matsubara J, Sugiyama S, Sugamura K, Nakamura T, Fujiwara Y, Akiyama E, et al. A dipeptidyl peptidase-4 inhibitor, des-fluoro-sitagliptin, improves endothelial function and reduces atherosclerotic lesion formation in apolipoprotein E-deficient mice. J Am Coll Cardiol. 2012;59:265–276. doi: 10.1016/j.jacc.2011.07.053 22240132
57. Vittone F, Liberman A, Vasic D, Ostertag R, Esser M, Walcher D, et al. Sitagliptin reduces plaque macrophage content and stabilises arteriosclerotic lesions in Apoe (-/-) mice. Diabetologia. 2012;55:2267–2275. doi: 10.1007/s00125-012-2582-5 22648661
58. Nyström T, Gutniak MK, Zhang Q, Zhang F, Holst JJ, Ahrén B, et al. Effects of glucagon-like peptide-1 on endothelial function in type 2 diabetes patients with stable coronary artery disease. Am J Physiol Endocrinol Metab. 2004;287:E1209–E1215. 15353407
59. Kubota Y, Miyamoto M, Takagi G, Ikeda T, Kirinoki-Ichikawa S, Tanaka K, et al. The dipeptidyl peptidase-4 inhibitor sitagliptin improves vascular endothelial function in type 2 diabetes. J Korean Med Sci. 2012;27:1364–1370. doi: 10.3346/jkms.2012.27.11.1364 23166419
Štítky
Interní lékařstvíČlánek vyšel v časopise
PLOS Medicine
2016 Číslo 6
- Není statin jako statin aneb praktický přehled rozdílů jednotlivých molekul
- INFOGRAFIKA: Doporučený postup léčby primární arteriální hypertenze u obecné populace dle guidelines ESC 2024
- Národní kardiovaskulární plán pro roky 2023–2033 v kontextu léčby hypertenze
- INFOGRAFIKA: Hypertoniků přibývá a bude hůř! Co bude následovat kromě epidemie srdečního selhání?
- Průlom ve farmakologické léčbě symptomatických pacientů s obstrukční hypertrofickou kardiomyopatií – kazuistika
Nejčtenější v tomto čísle
- Why Most Clinical Research Is Not Useful
- Agreements between Industry and Academia on Publication Rights: A Retrospective Study of Protocols and Publications of Randomized Clinical Trials
- Inter-pregnancy Weight Change and Risks of Severe Birth-Asphyxia-Related Outcomes in Singleton Infants Born at Term: A Nationwide Swedish Cohort Study
- Strengthening the Reporting of Observational Studies in Epidemiology—Nutritional Epidemiology (STROBE-nut): An Extension of the STROBE Statement
Zvyšte si kvalifikaci online z pohodlí domova
Eozinofilní zánět a remodelace
nový kurzVšechny kurzy