
Association between the 2008–09 Seasonal Influenza Vaccine and Pandemic H1N1 Illness during Spring–Summer 2009: Four Observational Studies from Canada
Background:
In late spring 2009, concern was raised in Canada that prior vaccination with the 2008–09 trivalent inactivated influenza vaccine (TIV) was associated with increased risk of pandemic influenza A (H1N1) (pH1N1) illness. Several epidemiologic investigations were conducted through the summer to assess this putative association.
Methods and Findings:
Studies included: (1) test-negative case-control design based on Canada's sentinel vaccine effectiveness monitoring system in British Columbia, Alberta, Ontario, and Quebec; (2) conventional case-control design using population controls in Quebec; (3) test-negative case-control design in Ontario; and (4) prospective household transmission (cohort) study in Quebec. Logistic regression was used to estimate odds ratios for TIV effect on community - or hospital-based laboratory-confirmed seasonal or pH1N1 influenza cases compared to controls with restriction, stratification, and adjustment for covariates including combinations of age, sex, comorbidity, timeliness of medical visit, prior physician visits, and/or health care worker (HCW) status. For the prospective study risk ratios were computed. Based on the sentinel study of 672 cases and 857 controls, 2008–09 TIV was associated with statistically significant protection against seasonal influenza (odds ratio 0.44, 95% CI 0.33–0.59). In contrast, estimates from the sentinel and three other observational studies, involving a total of 1,226 laboratory-confirmed pH1N1 cases and 1,505 controls, indicated that prior receipt of 2008–09 TIV was associated with increased risk of medically attended pH1N1 illness during the spring–summer 2009, with estimated risk or odds ratios ranging from 1.4 to 2.5. Risk of pH1N1 hospitalization was not further increased among vaccinated people when comparing hospitalized to community cases.
Conclusions:
Prior receipt of 2008–09 TIV was associated with increased risk of medically attended pH1N1 illness during the spring–summer 2009 in Canada. The occurrence of bias (selection, information) or confounding cannot be ruled out. Further experimental and epidemiological assessment is warranted. Possible biological mechanisms and immunoepidemiologic implications are considered.
: Please see later in the article for the Editors' Summary
Published in the journal:
. PLoS Med 7(4): e32767. doi:10.1371/journal.pmed.1000258
Category:
Research Article
doi:
https://doi.org/10.1371/journal.pmed.1000258
Summary
Background:
In late spring 2009, concern was raised in Canada that prior vaccination with the 2008–09 trivalent inactivated influenza vaccine (TIV) was associated with increased risk of pandemic influenza A (H1N1) (pH1N1) illness. Several epidemiologic investigations were conducted through the summer to assess this putative association.
Methods and Findings:
Studies included: (1) test-negative case-control design based on Canada's sentinel vaccine effectiveness monitoring system in British Columbia, Alberta, Ontario, and Quebec; (2) conventional case-control design using population controls in Quebec; (3) test-negative case-control design in Ontario; and (4) prospective household transmission (cohort) study in Quebec. Logistic regression was used to estimate odds ratios for TIV effect on community - or hospital-based laboratory-confirmed seasonal or pH1N1 influenza cases compared to controls with restriction, stratification, and adjustment for covariates including combinations of age, sex, comorbidity, timeliness of medical visit, prior physician visits, and/or health care worker (HCW) status. For the prospective study risk ratios were computed. Based on the sentinel study of 672 cases and 857 controls, 2008–09 TIV was associated with statistically significant protection against seasonal influenza (odds ratio 0.44, 95% CI 0.33–0.59). In contrast, estimates from the sentinel and three other observational studies, involving a total of 1,226 laboratory-confirmed pH1N1 cases and 1,505 controls, indicated that prior receipt of 2008–09 TIV was associated with increased risk of medically attended pH1N1 illness during the spring–summer 2009, with estimated risk or odds ratios ranging from 1.4 to 2.5. Risk of pH1N1 hospitalization was not further increased among vaccinated people when comparing hospitalized to community cases.
Conclusions:
Prior receipt of 2008–09 TIV was associated with increased risk of medically attended pH1N1 illness during the spring–summer 2009 in Canada. The occurrence of bias (selection, information) or confounding cannot be ruled out. Further experimental and epidemiological assessment is warranted. Possible biological mechanisms and immunoepidemiologic implications are considered.
: Please see later in the article for the Editors' Summary
Introduction
On 17 April 2009 a novel swine-origin influenza A (H1N1) virus was identified as the cause of two pediatric cases of febrile respiratory illness in California [1],[2]. Shortly thereafter, this virus was also identified as the cause of an outbreak of severe respiratory illness occurring among young people in Mexico in March and April [3],[4]. Subsequent spread throughout North America and elsewhere resulted in the declaration, on 11 June, of a phase 6 pandemic of the novel influenza A (H1N1) (now called pandemic influenza A (H1N1) [pH1N1]) by the World Health Organization (WHO) [5]. Early surveillance and immunogenicity data and global summary by the WHO emphasized increased risk among young people <50 years of age [2],[6],[7].
Influenza vaccine is recommended and provided free in Canada to children 6–23 months of age, elderly people, people of all ages with designated high-risk conditions, and their household contacts and care providers [8]. In Ontario, all residents ≥6 months of age can access the influenza vaccine annually free of charge via a universal immunization program initiated in 2000. Residents of other provinces who are not among the high-risk or their contacts are also encouraged to receive influenza vaccine, and this may be provided free by their employers or they must purchase it. In its annual update, WHO recommended changes to all three components of the influenza vaccine for the 2008–09 season [8]. GlaxoSmithKline (GSK Fluviral; domestically manufactured) and Sanofi Pasteur (Vaxigrip; imported) supply approximately 75% and 25%, respectively, of the split trivalent inactivated influenza vaccine (TIV) distributed each year in Canada; Quebec generally receives a higher proportion of GlaxoSmithKline product (∼95% for 2008–09 and 2007–08) while Ontario generally receives less (∼67% for 2008–09 and 2007–08). Live attenuated influenza vaccine is not yet approved for use in Canada.
During the last week of April, a school pH1N1 outbreak was reported in a rural community of northern British Columbia (BC) [9]. During outbreak investigation, an unexpected signal of association between prior vaccination with TIV and fever/cough illness was noted. Because these unexpected results were based on a nonspecific outcome defined by clinical syndrome, separate follow-up studies were arranged to investigate this initial signal using more stringent methodologies based on laboratory-confirmed outcomes. We report the results of four epidemiologic studies conducted during the summer of 2009 in Canada to assess the putative association between vaccination with seasonal 2008–09 TIV and pH1N1 illness.
Methods
The design, sample size, and outcomes evaluated in each of the four studies to assess the association between prior 2008–09 TIV receipt and risk of pH1N1 illness are summarized in Table 1.

Ethics Statement
The studies described were approved by the relevant institutional review boards of participating agencies/provinces as well as nationally for the sentinel study, or were conducted as legally mandated public health investigations for the Quebec and Ontario case-control studies. Patients provided written informed consent for the prospective cohort study and oral consent for the other three studies.
National Sentinel Monitoring System
The four most populated provinces of Canada—BC, Alberta, Ontario, and Quebec—conduct annual (November through April) vaccine effectiveness (VE) monitoring through linked community-based sentinel physician surveillance networks. Study methods, implemented annually since 2004 and described in detail in prior publications, are approved each year by ethics boards provincially and nationally [10]–[12]. Designated sentinel sites in participating provinces are provided kits with which clinicians submit respiratory specimens (nasal or nasopharyngeal [NP]) for influenza testing along with epidemiologic information collected in a standardized way from eligible consenting patients presenting within 7 days of onset of influenza-like illness (ILI). Following the emergence of pH1N1 in mid-April, sentinel physicians in participating provinces were instructed to continue their routine VE monitoring activities, regardless of other testing guidelines to clinicians.
Seasonal influenza analysis spanned ILI onset between 1 November 2008 and 31 March 2009. pH1N1 analysis spanned ILI onset between 17 April and 22 July 2009. Testing for seasonal influenza at designated provincial laboratories in BC, Ontario, and Quebec consisted of real time reverse transcription PCR (RT-PCR) screening for influenza A and B, followed by real time RT-PCR subtyping (A/H1 or A/H3). In Alberta, all specimens were tested by Luminex RVP Assay, which detects seasonal influenza, pH1N1, and influenza B viruses and directly subtypes as A/H1 or A/H3. Testing was modified in all provinces after 17 April to detect pH1N1 using a conventional (end point) RT-PCR assay (Text S1, Appendix A1). Sequence analysis was performed on a subset of the PCR product in each province to validate specificity of pH1N1 detection.
We used the test-negative case-control design: cases presented with ILI and tested positive for seasonal or pH1N1 influenza, depending upon the analysis period; controls presented with ILI and tested negative for both seasonal and pH1N1 influenza. Medically attended, laboratory-confirmed influenza is uncommon, and thus case subjects are a small fraction of the total source population. In addition, control subjects are a proportion of the total population that reflects vaccine coverage and is anticipated to be stable over both the seasonal and the pH1N1 analysis periods. In that context, the odds ratio (OR) is appropriate to estimate the risk ratio (RR) [13]. Logistic regression was thus used to estimate ORs for a 2008–09 TIV effect on laboratory-confirmed influenza through sequential models with adjustment for age, chronic conditions, province, and timeliness of medical visit (sex was also explored but was not influential in final models). Per above, stratification at age 50 was decided a priori because of age-related differences generally observed in the epidemiology of pH1N1. VE is typically calculated as 1 – OR; here, we report ORs directly [14]. Additional methodological detail, including laboratory testing procedures, is provided in Text S1, Appendix A1.
Quebec Population Case-Control Study
A legally mandated public health investigation was launched in Quebec on 15 July 2009. Eligible cases included community (medically attended, nonhospitalized) and hospitalized (≥24 hours) laboratory-confirmed detections of pH1N1 illness with onset from 25 May to 1 July among residents of one of four regions of Quebec together comprising 83% of community cases and 78% of hospitalized cases in Quebec during that period. All tests for pH1N1 were conducted at the provincial laboratory by specific RT-PCR assay. The study sampling plan included all hospitalized cases, approximately the same number of community cases and a number of controls similar to the sum of the hospitalized and community cases. The initial study plan was to use a test-negative case-control approach. Results from this test-negative approach was consistent with increased risk of pH1N1 illness among prior TIV recipients, but more in-depth examination of participant profiles showed test-negative specimens to be inadequate as controls for reasons outlined in Text S2, Appendix B1a–B1e, notably because of early restrictions placed on testing in Quebec. Quebec therefore moved to conventional sampling of population controls from the community. Population controls were selected by random-digit-dial to homes in numbers proportionate to the number of cases per age group and region. Trained interviewers conducted the survey from 17 July to 10 August 2009 using a standardized questionnaire. ORs were derived through sequential logistic regression for a 2008–09 TIV effect on pH1N1 cases compared to community controls with adjustment for relevant covariates (Tables 1 and 5).
Ontario Test-Negative Case-Control Study
An urgent public health investigation was also conducted in Ontario based on test-negative case-control design. A sample size of 300 cases and 600 controls was estimated to be required a priori based on TIV prevalence in controls of 30%–35%, an alpha value of 0.05, and statistical power of 80% to detect an OR of at least 1.5 for increased risk of medically attended pH1N1 illness. Respiratory specimens (nasal, throat, or NP swabs) submitted for influenza testing between 13 April and 20 July 2009 at the provincial laboratory or the Mount Sinai Hospital/University Health Network were identified as representing a community (medically attended, non-hospitalized) or hospitalized case (pH1N1-specific RT-PCR positive) or a control (RT-PCR negative for all influenza). Hospitalized cases were identified through linkage to the public health surveillance database. Test-negative controls were medically attended community-based patients. A sample of cases and controls was randomly selected and frequency-matched by age group and week of specimen collection. A standardized telephone survey of consenting cases and controls was administered between 1 August and 4 September 2009 by trained interviewers from the Institute for Social Research (ISR), York University, Toronto. In the analysis, test date before versus after 11 June was incorporated as a binary variable into all models since Ontario clinicians (outside the sentinel system) were instructed after that date to submit specimens only from high-risk patients and/or patients with severe illness. ORs were derived through sequential logistic regression for a 2008–09 TIV effect on pH1N1 cases compared to test-negative community controls with adjustment for relevant covariates (Tables 1 and 5).
Quebec Household Transmission Study
A prospective study to assess household pH1N1 transmission and secondary attack rates (SARs) was conducted in Quebec City, Canada from 27 May to 10 July 2009. The effect of TIV on pH1N1 risk was thus also explored in this cohort. The household primary case was the first laboratory-confirmed patient to present with symptoms of respiratory illness in the household. Primary cases were excluded as were symptomatic household members without laboratory-confirmation of pH1N1 whose symptom onset preceded that of the primary case. NP swabs were collected at home from all household members as soon as possible after identification of the primary case. Clinical information and self-reported 2008–09 TIV status were collected using a standardized questionnaire. NP swabs were tested by RT-PCR assay. SARs were compared across vaccination groups by Chi-square (or Fisher exact as appropriate) for children (<18 years) and adults (≥18 years), and RRs were computed.
Results
National Sentinel Monitoring System
Inclusion/exclusion criteria and final participation in the seasonal and pH1N1 sentinel study analysis periods are shown in Text S1, Appendix A2. Influenza subtype and pH1N1 detection by province are shown in Text S1, Appendix A3a/b, and the epidemic curve of influenza test results by subtype and week of ILI onset is shown in Text S1, Appendix A4. There were 1,529 specimens included in the overall seasonal analysis, of which 672 (44%) were influenza positive; by subtype these included 253 A/H3 (38%), 249 B (38%), and 160 A/H1 (24%). Ten were non-subtypeable. There were 711 specimens included in pH1N1 analyses, of which 175 (25%) were influenza positive, 144 (82%) for pH1N1 (20% pH1N1 positivity), 29 (17%) for seasonal influenza, and two of unknown subtype. Seasonal influenza viruses were detected in 28 sentinel specimens with ILI onset between 20 April and 10 May 2009, including 14 A/H3 (50%), 11 B (39%), and three A/H1 (11%); A/H1 was detected in one specimen thereafter.
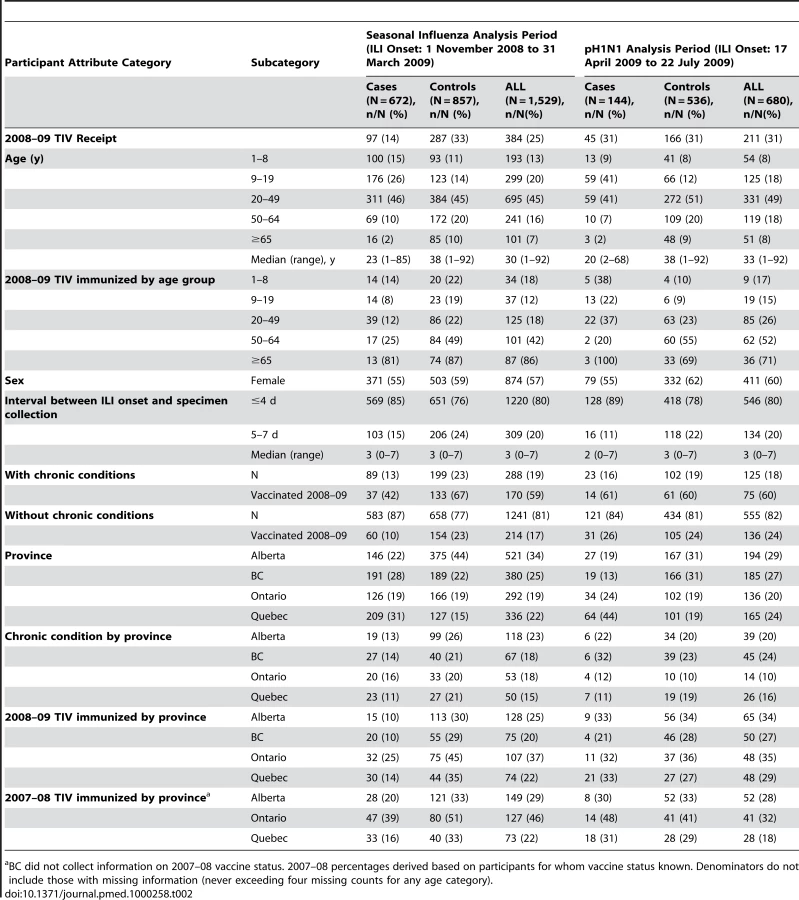
The profile of participants is comparable between seasonal and pH1N1 analysis periods (Table 2; more detail in Text S1, Appendix A5a/b). Young adults aged 20–49 years contributed most to the sentinel study during both seasonal and pH1N1 analysis periods. In participating provinces, 9% of the general population 12–19 years, and 10% aged 20–49 years, are estimated from publicly available data to have vaccine-eligible chronic conditions [15]. These proportions are comparable to those found among seasonal and pH1N1 test-negative controls in the sentinel study. Compared to population estimates of ∼20%–25% for 50 - to 64-year-olds and ∼35%–40% for those ≥65 years, the report of chronic conditions was substantially higher among older adult controls for both seasonal (64/172 [37%] and 57/85 [67%], respectively) and pH1N1 (34/109 [31%] and 27/48 [56%]) analysis periods (Text S1, AppendixA5a/A5b) [15]. The proportion immunized in 2008–09 among test-negative controls was comparable for seasonal and pH1N1 analysis periods both overall (287/857 [33%] and 166/536 [31%], respectively) and among controls ages 20–49 years (86/384 [22%] and 63/272 [23%], respectively). Overall, immunization coverage estimates among controls were similar to those derived from the 2007–08 Canadian Community Health Survey (CCHS), particularly among young adults (Text S3, Appendix C) [16].
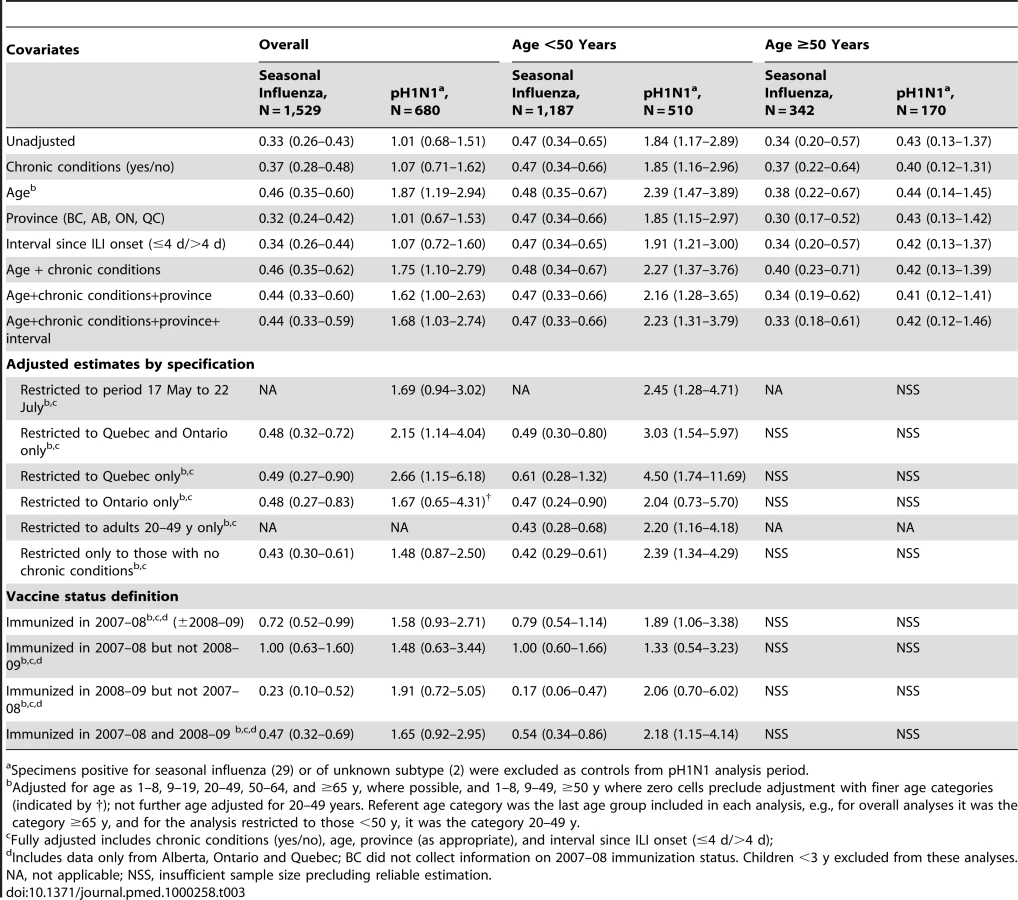
As in previous seasons, we found that prior vaccination with TIV significantly reduced the risk of medically attended seasonal influenza in 2008–09, with ORs consistently and significantly <1 (Figure 1, Table 3). Conversely, receipt of TIV was associated with significantly increased risk of medically attended pH1N1 illness with fully adjusted OR (95% CI) of 1.68 (1.03–2.74) overall and 2.23 (1.31–3.79) for participants <50 years (Figure 1, Table 3). Fully adjusted sensitivity analyses, further restricted to participants 20–49 years of age, to those with ILI onset after mid-May (the period of greatest indigenous pH1N1 circulation), or to the provinces of Quebec and Ontario (more intense pH1N1 activity) gave consistent results (Table 3). ORs were highest for a vaccine effect on pH1N1 risk in Quebec. Caution is required in the interpretation of a TIV effect for the age stratum >50 years owing to small sample size, wide confidence intervals spanning 1, and further anticipated variation of effect with advancing age and immune status among older individuals [17],[18]. Estimates for crude and fully adjusted ORs for 2008–09 TIV effect on seasonal influenza for the period 17 April to 30 May 2009 remained <1, although sample size was again small and statistical significance was not achieved. In overall analyses, the crude and fully adjusted ORs for 2008–09 TIV in preventing seasonal influenza during the pH1N1 analysis period 17 April to 30 May were 0.48 (0.18–1.30) and 0.73 (0.25–2.16), respectively, and for the age stratum <50 years were 0.55 (0.16–1.93) and 0.87 (0.23–3.32), respectively. Crude and adjusted ORs for TIV effect on seasonal influenza were also <1 for the full pH1N1 analysis period spanning 17 April to 22 July.

Quebec Population Case-Control Study
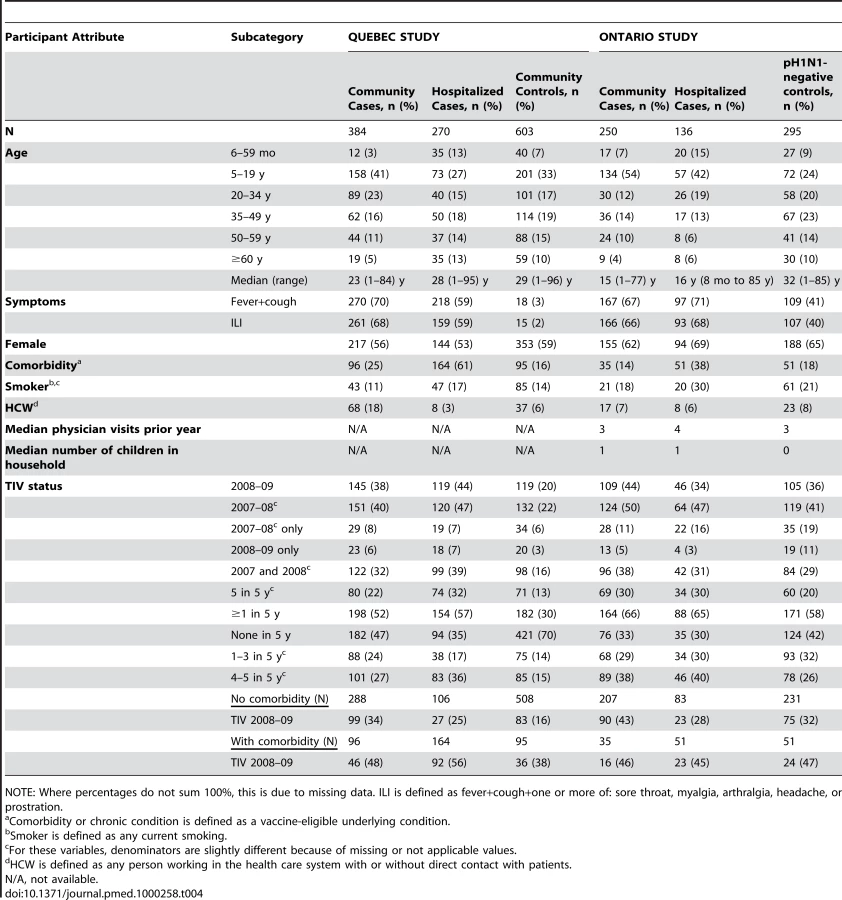
Among community members who answered the telephone survey as potential controls, the participation rate before applying exclusions was 62% (630/1,014) for the Quebec case-control study (details provided in Text S4, Appendix D1). After exclusion criteria were applied, 384 community cases, 270 hospitalized cases, and 603 community controls were available for the Quebec case-control analysis (Text S4, Appendix D1). Participant profiles are shown in Table 4 and in more detail in Text S4, Appendix D2. In community controls aged 12–19, 20–34, 35–44, and 45–64 years, TIV coverage for the 2008–09 season were 6% (8/125), 16% (16/101), 18% (13/71), and 24% (35/144), respectively, similar to estimates from the CCHS for Quebec as measured for the 2007–08 season (Text S3, Appendix C) [16]. The proportion of controls with underlying medical conditions eligible for TIV was also comparable to population estimates by age (Text S4, Appendix D2) [15].
The crude OR for a 2008–09 TIV effect on pH1N1 community cases was significant compared to controls (2.47 [1.85–3.30]) (Table 5). Crude OR was also significant for hospitalized (3.20 [2.34–4.38]) cases (Table 5). After adjustment for age, chronic conditions, sex, and HCW status, the OR for community cases was 2.48 (1.80–3.42) and for hospitalized cases was 2.16 (1.47–3.17) (Figure 1, Table 5). TIV receipt did not appear to increase the risk when comparing hospitalized to community cases (adjusted OR of 0.97 [0.66–1.42]).

Ontario Test-Negative Case-Control Study
Text S5, Appendix E1 outlines inclusion and exclusion criteria resulting in 250 community cases, 136 hospitalized cases, and 288 test-negative community controls available for analysis in the Ontario test-negative case-control study. Baseline characteristics of community or hospitalized cases and controls are shown in Table 4 and in more detail in Text S5, Appendix E2. Community and hospitalized cases were younger than controls but reported similar health care–seeking behavior as measured by the median number of physician visits in the prior 12 months (Table 4). Among participants reporting any “flu-like” symptoms at the time of influenza testing, 72% (166/230) of community and 73% (93/130) of hospitalized cases reported symptoms consistent with ILI, compared to 41% (106/256) of controls (59 participants were unable to recall specific symptoms). Among controls 20–49 years of age, 31% (38/123) had received TIV, slightly higher (by ∼5%-10%) compared to people 20–44 years from the 2007–08 CCHS for Ontario (Text S3, Appendix C) [16]. The proportion of controls aged 12–49 years with a chronic condition (18/143; 11%) was within the expected range based on available population estimates [15].
After adjustment for age, chronic conditions, sex, and HCW status, the OR for TIV effect on pH1N1 was 1.95 [1.27–2.99] for community cases compared to controls (Figure 1, Table 5). For hospitalized cases, the OR was 1.19 [0.61–2.32] (Table 5). Adjustment for neither the number of primary care visits in the previous 12 months (marker for health care–seeking behavior) nor number of children in the household (marker for exposure risk) had influence except to slightly increase ORs. Interval between symptom onset and specimen collection was available for 141/250 (56%) of the community cases and 171/229 (60%) of the test-negative controls. With restriction to only community cases and controls known to be tested within 4 days of symptom onset, the fully adjusted OR for TIV effect on pH1N1 increased to 2.37 (1.22–4.60). Restriction to only participants known to have had ILI gave consistent results, but with reduced power owing to small sample size. TIV receipt did not appear to increase the individual risk of hospitalization when hospitalized and community cases were compared (adjusted OR of 0.68 [0.41–1.13]).
Household Transmission Study
Forty-seven households participated in the Quebec household transmission study. This included 47 primary cases, six members who were symptomatic before the primary case, and 120 other members. Among these 120 household members (median age 29 years, range 0–61 years), 32/120 (27%) had received the 2008–09 TIV, 8/48 (17%) of children and 24/72 (33%) of adults. Timeline to the first specimen collection after identification of the primary case was similar between vaccinated and unvaccinated participants at a median of 3 (range 1–14) versus 3 (range 1–16) days. The proportion of children with chronic conditions was 0% (0/8) for the vaccinated and 15% (6/40) for the unvaccinated, whereas for adults it was 21% (5/24) and 23% (11/48), respectively.
SARs by outcome category for vaccinated compared to unvaccinated children and adults are presented in Table 6. TIV was not associated with increased risk of nonspecific respiratory symptoms (p = 0.40) for any age category. No increased risk was found in children for any outcome category, but with only eight vaccinated pediatric participants, no definitive conclusions should be drawn. Among the larger sample of adults, TIV was associated with significantly increased risk for more specific outcomes of ILI syndrome (RR 3.20 [95% CI 1.17–8.74]) and laboratory-confirmed pH1N1 regardless of symptoms (RR 2.18 [1.13–4.20]). Results were essentially unchanged and remained significant with adjustment for sex. Comparison of syndrome severity among vaccinated versus unvaccinated laboratory-confirmed cases overall showed no significant differences, with similar mean number of days during which the patient was unable to carry on daily activities (2.7 versus 2.4) and during which the patient was bedridden (1.4 versus 1.5).

Discussion
To assess the association between TIV and pH1N1 risk that was first identified in Canada during the late spring of 2009, several observational designs were pursued through the summer, a period when pH1N1 continued to circulate in Canada. As reported here, this included incident (sentinel network) and retrospective case-control methods with both test-negative and conventional community controls as well as a prospective cohort study. In this paper we report the expected finding that 2008–09 TIV was associated with a significant (56%) reduction in the risk of medically attended illness due to seasonal influenza. However, we also report the unexpected finding that TIV receipt was subsequently associated with a statistically significant (1.4 - to 2.5-fold) increased risk of medically attended illness due to the novel pH1N1 virus (Figure 1). Because the latter result is contrary to established knowledge, greater scrutiny is required to determine whether these associations are more likely on balance to be real (causal) or due to a methodological flaw (bias). Reliance on observational methods means that even careful study design, implementation, and analysis cannot rule out the possibility of random variation (chance) or bias (selection, information) or confounding in explaining results. Consistency of results across different designs in various populations and with substantial sample sizes provides some reassurance against random variation, but the possible contributions of bias or confounding still warrant careful consideration.
Several methodological issues have thus been considered in assessing these findings. The sentinel test-negative approach provides estimates of TIV association with both seasonal and pH1N1 risk and offers several methodological advantages. The well-established and rehearsed sentinel system in Canada has consistently shown TIV protection against seasonal strains over the several years of its application, higher with better vaccine matches and lower with relative antigenic mismatches [10]–[12]. Canada's sentinel system has not previously found an increased risk of illness associated with TIV, even at the component-specific level in the context of substantial vaccine mismatch to circulating seasonal strains. With the emergence of the novel pH1N1 virus in mid-April we were able to extend routine 2008–09 sentinel monitoring activities into the spring and summer without changes in protocol. Canada has a publicly funded health care system that is free to patients at use, thus removing restrictions on access that may apply elsewhere. Sentinel physicians were specifically notified that they were exempt from limitations on respiratory specimen testing applied to other ambulatory care clinicians. Although patients may have themselves altered their usual patterns of physician visits, in accordance with protocol only submissions meeting the ILI definition were included in sentinel analyses, thereby standardizing in part, although not fully, for health care–seeking or illness severity. Influenza immunization registries do not exist in participating provinces, so all vaccine uptake estimates rely upon patient self-reports and cannot be further confirmed. Although imperfect recall may have introduced misclassification of vaccine status, immunization history was recorded by the clinician at the time of test submission, before the test result was known, thus helping to attenuate possible differential in recall by outcome. We also excluded submissions with unknown vaccine status. Unlike the Ontario and Quebec case-control studies, the sentinel approach did not collect information on occupation. Adjustment for HCW status, however, did not meaningfully influence ORs in the Ontario test-negative or Quebec population case-control studies, and when they were excluded in the Quebec test-negative approach, ORs were unchanged or slightly increased.
To further address the possible influence of health care–seeking behavior, we adjusted for the timeliness of medical visits in the sentinel and Ontario case-control studies and for chronic conditions in all studies. Comorbidity was analyzed as a dichotomous variable. Although all chronic conditions may not exert the same influence, further stratification on select categories of chronic conditions did not influence ORs in subanalyses (not shown; available upon request). It is possible that misclassification of comorbidity may have biased our results. If this effect exists in the sentinel study, however, it should be minor; underlying conditions were also recorded before test results were known, and our findings mainly reflect the experience of healthy young adults and school-aged children. It is important to note that subanalyses within the stratum of participants without any chronic conditions showed a consistent vaccine effect. The lower ORs and apparent absence of TIV effect on pH1N1 risk in the older stratum of sentinel study participants are noteworthy. During both analysis periods, the proportion of controls ≥50 years of age, and especially ≥65 years of age, who reported chronic conditions and who received TIV were higher than expected based on community surveys, flagging a possible concern with the controls in that stratum. Given the small sample size and the expected variation in important characteristics such as pre-existing pH1N1 immunity across advancing years of life, no specific conclusions can be drawn for older individuals based on these data [17],[18].
A strength of the sentinel study is that it enabled a direct comparison of participant profiles and vaccine effect using the same methods for seasonal and pH1N1 analysis periods. With similar methods and participant profiles for the two analysis periods, we found very different TIV associations with influenza risk, notably among younger persons. We found significant TIV protection against seasonal influenza and a protective trend against seasonal strains that persisted during the pH1N1 analysis period. ORs<1 for seasonal influenza that persisted after April 17 make it more difficult to attribute the ORs>1 for pH1N1 using the same methods during the same period to newly introduced bias.
With its randomly selected community controls, the Quebec population case-control study likely provides the upper bound of a risk estimate for pH1N1 associated with TIV, since standardization of health care–seeking behavior between cases and controls was not afforded. Results from this design may be affected by differential characteristics among those who sought care or testing compared to community controls. The initial Quebec experience with the test-negative case-control design also provides an important caution regarding the potential for selection bias with this approach. This caution applies especially to test-negative designs when specimens are drawn from general laboratory submissions and/or when limitations are placed on testing, such as to individuals with chronic conditions or severe illness (see Text S2, Appendix B1a). Careful assessment of participant profiles showed that the test-negative controls in the initial Quebec study were not adequately representative of the source population from which the cases arose, although with appropriate adjustment for relevant covariates and restriction to patients with similar clinical presentation, the same increased risk of pH1N1 illness in association with 2008–09 TIV was found (Text S2, Appendix B1a–B1e).
Ontario applied a later restriction on laboratory testing compared to Quebec (11 June versus 15 May), and the Ontario dataset showed test-negative controls to be representative of the case source population. Both cases and controls sought care and had similar health care–seeking behavior, as evidenced by the rate of physician visits in the previous 12 months and by the proportion with chronic conditions. Immunization rates among test-negative controls may have slightly exceeded population estimates for Ontario in young adults (tending to decrease the OR) but a statistically significant effect was still observed. Adjustment for other relevant covariates generally increased ORs among vaccinated participants. Sample sizes in Ontario were smaller than planned, especially for hospitalized cases, and confidence intervals surrounding ORs were wide, particularly among stratified analyses. Point estimates, however, remained consistent with other studies. A comparison between hospitalized and community cases in both the Quebec and the Ontario designs suggests that once pH1N1 illness was acquired, the risk of pH1N1 hospitalization was not further increased among TIV recipients. An increase in the absolute number of hospitalizations, however, would nevertheless still occur with this association, since that number is determined by the risk of becoming ill (increased) multiplied by the risk of hospitalization once ill (unchanged). Finally, with its active and prospective follow-up of all household members, the Quebec household transmission study provided corroborating evidence that was able to avert the potential for health care–seeking and other selection biases known to affect case-control studies. The results were consistent with other findings, and statistical significance was observed. A limitation of that study, however, is the small sample size that precluded further stratification.
Confounding by indication may spuriously lower VE estimates in observational studies because influenza vaccine is administered to people at greater risk of clinical illness and more likely to seek care (such as those with chronic conditions) [19]. More recent publications have also reported overestimation of influenza vaccine protection against serious outcomes among elderly persons as a result of better general health status among vaccinated compared to unvaccinated people (healthy user bias) [20],[21]. Influences on immunization status can thus skew estimates in either direction. It may be that in young people chronic conditions exert a greater influence in decreasing VE estimates (increasing ORs) than the counterforce of healthy user bias. Our national sentinel study population, however, included few participants with chronic conditions, and to further address this possible influence we applied recognized analysis techniques of restriction, stratification, and adjustment to all studies. We cannot rule out that these efforts were incomplete and that an unmeasured bias or residual confounding remains.
Several studies from Australia [22], Mexico [23],[24], and the US [25],[26] have instead reported null or protective effects of 2008–09 TIV against pH1N1 illness based on test-negative case-control [22]–[25], case-cohort [25], or ILI outbreak investigations [26]. One other test-negative case-control analysis from a US outbreak found a statistically significant increased risk, with an unadjusted OR of 2.9 (95% CI 1.8–4.69) for pH1N1 illness among military beneficiaries who received influenza vaccine within the previous 12 months [27]. Unlike in Canada, however, this association was driven primarily by receipt of live attenuated vaccine. Discrepant results across studies may reflect either differences in methods or real variation in the effect of specific vaccines, immunization programs, or population immunity. Most of the studies published to date, however, have not presented sufficient participant characteristics to properly assess methodological issues, sources of bias or confounding, or the validity of results. As previously highlighted, the importance of the public health and scientific implications requires that analyses of TIV effect on pH1N1 risk be more rigorous [28],[29]. At a minimum, a detailed profile of cases and controls specifically included in vaccine effectiveness analyses should be displayed by vaccine status, age, and chronic conditions, as well as timeliness of specimen collection and other recognized influences. Where participant characteristics have been presented by investigators, conspicuous evidence of selection bias can be seen to explain opposite findings of TIV protection against pH1N1 [23],[28]. In the detailed participant profiles we display for each of the four studies we report, evidence for this type of bias is not obvious, but that does not rule it out. We also cannot rule out the possibility that the increased risk of pH1N1 found in Canada was an effect specific to the Canadian vaccine: it is noteworthy that ORs were highest in Quebec, where a greater proportion of domestically produced vaccine is distributed than in the rest of Canada. However, even if our findings are considered a “Canadian problem,” if causal in nature they would still have wider implications for our understanding of influenza immunopathogenesis.
In the event that our findings are valid and reflect a causal association by which prior receipt of TIV increased the risk of PCR-positive pH1N1 illness, several biological mechanisms have been considered to explain them. These proposed mechanisms must each be viewed as speculative since our epidemiologic studies were not designed to assess them. One hypothesis is that repeat immunization effectively blocks the more robust, complex, and cross-protective immunity afforded by prior infection. This mechanism was suggested by Hoskins et al. in the mid-1970s in evaluating the risk of A/H3N2 drift variants among previously infected versus immunized boys during successive boarding school outbreaks, with the consideration of other factors (such as viral neuraminidase [NA]) in addition to HA antibody [30]. Bodewes et al. have more recently shown in mice that effective vaccination against human influenza A/H3N2 virus prevents virus-induced (cell-mediated) heterosubtypic immunity against severe (lethal) infection with avian influenza of a different subtype (A/H5N1) [31],[32]. That one influenza subtype may influence the risk of infection by another is also suggested by the subtype replacement that followed the pandemics of 1918, 1957, and 1968, although the mechanism for that is unknown [33]. A BLAST sequence analysis demonstrates that pH1N1 and human influenza strains (A/H1N1 and A/H3N2, recent [since 2000] and historical [since 1974]) are nearly identical (95%–98%) with respect to their polymerase proteins, at both the overall and the antigenic levels, and other internal components, including M1 (94%–97%) and NP (85%–92%) are also well-conserved (Text S6, Appendix F). Conversely, both the HA and the NA surface proteins of recently circulating seasonal H1N1 influenza viruses and pH1N1 are more divergent, particularly with respect to their antigenic regions (Text S6, Appendix F). With a greater likelihood of seasonal influenza infection, unvaccinated people may have had a greater opportunity to develop cross-protective cell-mediated immunity to the more conserved internal viral components of pH1N1. Since those immunized in a given season may have been repeatedly immunized over several seasons, they may have lost multiple opportunities for infection-induced cross-immunity. TIV recipients may have boosted antibody to HA/NA (the only TIV components), effectively protecting against seasonal influenza, but without a cross-protective effect against the markedly different surface antigens of pH1N1.
If this hypothesis explains our results, it also reassuringly implies that the TIV effect we have observed on pH1N1 risk would be induced again only if seasonal influenza circulates before pH1N1 and TIV blocks the potential cross-protection of that heterologous infection. There are, however, at least two considerations that oppose this hypothesis. First, the risk of laboratory-confirmed influenza illness per se—the outcome reported by our studies—is believed to be determined primarily by protective antibodies to viral surface proteins. As indicated above, the antigenic distance between the HA and NA surface proteins of pH1N1 and recently circulating human H1N1 strains is large, making cross-protection on that basis less likely. Differences in severe outcomes may be explained by cross-protective cell-mediated immunity, as shown by Bodewes et al. to be induced by prior infection with heterologous virus, but we did not detect differences in severe outcomes by vaccine status and that is not what we are trying to explain. The role of cell-mediated or other immune correlates of cross-protection against influenza illness per se likely warrants further study. Second, in order to show a 2-fold increase in pH1N1 illness, this hypothesis would require implausible assumptions of unreasonably high prior seasonal influenza attack rates, cross-protection against pH1N1 illness, and/or the effective block of that cross-protection by TIV (see Text S7 Appendix G).
We have also considered the possibility of a direct immune mechanism to explain our results. One such mechanism is based on the induction of low-affinity/non-neutralizing but cross-reactive antibodies by TIV to the major surface proteins. Such antibodies are typically identified within an “original antigenic sin” response [34]–[36], the relevance of which has long been debated for influenza, but for which Kim and colleagues have recently provided evidence in the mouse model [37]. In a related concept, antibody-dependent enhancement (ADE) of virus replication may occur when preexisting low levels of weakly heterotypic antibodies (cross-reactive but not cross-protective) bind to virus but instead of neutralizing the virus, form bridging complexes that facilitate enhanced uptake and increased virus production by the target cell [38]–[40]. Original antigenic sin and ADE of virus replication have been described for secondary heterotypic dengue infections, but also in vitro for other viruses such as respiratory syncytial virus, Ebola, HIV, etc. [38]–[40]. ADE has also been shown in vitro for influenza uptake by macrophages, although these are not generally considered the main target cell for influenza replication [41]–[44]. Interestingly, vaccine-potentiated pneumonia has been reported following heterologous swine influenza challenge in pigs, and enhanced pneumonia due to heterologous swine influenza has also been reported in piglets vaccinated in the presence of maternal antibody, with ADE invoked by authors to possibly explain these findings [45],[46]. In further support of a direct vaccine-induced effect to explain our findings, a recent pH1N1 challenge study of influenza-naïve ferrets has shown that, compared to a nonimmunized control group, prior receipt of 2008–09 seasonal vaccine (notably live attenuated vaccine) was associated with slight worsening of day 3 upper airway viral loads, clinical disease, and mortality, with ADE also invoked by authors as a possible explanation [47]. We did not find increased pH1N1 severity associated with seasonal vaccine in our epidemiologic studies; this observation may reflect intrinsically less virulent virus or, as described above, other intact viral clearance mechanisms [48].
In considering the ADE hypothesis, it should be recognized that this proposed mechanism has not been previously linked to epidemiologic observations for influenza in humans. ADE may require a precise balance of antigenic distance and cross-reactive versus neutralizing antibody to be manifest. The 2009 pandemic differs from other influenza epidemics or pandemics in that it has been caused by a novel virus distantly related to but nevertheless within the same HA/NA subtype as recently circulating H1N1 viruses. The role of antibody concentrations in ADE is under debate, so it is difficult to know whether our findings during spring–summer 2009 in Canada, if explained in this way, would have been observed during fall–winter 2009–10 with (or without) repeat administration of TIV, or whether seasonal vaccines may differ in the relative proportion of cross-reactive versus cross-protective antibody induced to pH1N1. In the end, our results may seem counterintuitive, but they cannot be dismissed on the basis that no biological mechanism can plausibly explain them. The mechanism may be a combination of the above or an as-yet unknown pathway. Further empiric evidence would be necessary to support a specific mechanism.
After the substantial autumn 2009 wave of pH1N1 and the mass pH1N1 vaccination campaign, seasonal influenza viruses remain a possible threat to consider for the rest of the 2009–10 winter. The complex benefit–risk analysis for receipt of 2009–10 TIV will ultimately depend upon the extent to which seasonal A/H1N1, A/H3N2, or B viruses contribute to TIV-preventable morbidity this season. It remains uncertain whether the influenza A subtype replacement observed with previous pandemics will also occur with this pandemic. Thus far (to 1 March 2010), seasonal strains have not comprised a substantial proportion of influenza detections in the northern hemisphere's 2009–10 season, with the exception of a recent increase in influenza B in China [49]. For the next season, WHO has recommended that pH1N1 be included in seasonal vaccine formulations, thereby providing direct pH1N1 protection and obviating the possible risk we identified in association with the seasonal vaccine in 2009 [50],[51]. The possible scientific implications of our findings, however, will remain important to consider over the long term. These include questions about influenza immunopathogenesis, the interaction between seasonal and novel pandemic strains, the complex immunoepidemiologic aspects of influenza prevention and control, and how best to assess these issues experimentally and epidemiologically.
In summary, we report findings from four epidemiologic studies in Canada showing that prior receipt of 2008–09 TIV was associated with increased risk of medically attended pH1N1 illness during the spring–summer 2009. Bias cannot be ruled out in observational studies, and therefore these findings cannot be considered conclusive. If these observations do reflect a real biological effect, however, they raise important questions that warrant further scientific investigation.
Supporting Information
Zdroje
1. CDC 2009 Swine influenza A (H1N1) infection in two children - Southern California, March–April 2009. MMWR Morb Mortal Wkly Rep 58 400 402
2. Novel swine-origin influenza A(H1N1) virus investigation team 2009 Emergence of a novel swine-origin influenza A (H1N1) virus in humans. New Engl J Med 361 1 10
3. ChowellG
BertozziSM
ColcheroMA
Lopez-GatellH
Alpuche-ArandaC
2009 Severe respiratory disease concurrent with the circulation of H1N1 influenza. New Engl J Med 361 674 79
4. Perez-PadillaR
de la Rosa-ZamboniD
Ponce de LeonS
HernandezM
Quinones-FalconiF
2009 Pneumonia and respiratory failure from swine-origin influenza A (H1N1) in Mexico. New Engl J Med 361 680 89
5. WHO 11 June 2009 Transcript of statement by Margaret Chan, Director-General of the World Health Organization. Available: http://www.who.int/mediacentre/influenzaAH1N1_presstranscript_20090611.pdf. Accessed 26 February 2010
6. KatzJ
HancockK
VeguillaV
ZhongW
SunH
2009 Serum cross-reactive antibody response to a novel influenza A (H1N1) virus after vaccination with seasonal influenza vaccine. MMWR Morb Mortal Wkly Rep 58 521 524
7. WHO 2009 WHO pandemic (H1N1) briefing note 9: Preparing for the second wave: lessons from current outbreaks. Available at: http://www.who.int/csr/disease/swineflu/notes/h1n1_second_wave_20090828/en/index.html. Accessed 26 February 2010
8. National Advisory Committee on Immunization 2008 Statement on influenza vaccination for the 2008–09 season. Can Commun Dis Rep ACS-3 34 1 46
9. JanjuaNZ
SkowronskiDM
HottesTS
OseiW
PetricM
2010 Seasonal influenza vaccine and increased risk of pandemic H1N1 illness: first detection of the association during outbreak investigation in British Columbia, Canada. 13th Annual Conference on Vaccine Research, Bethesda, MD, 27 April 2010. Abstract # 130
10. SkowronskiDM
GilbertM
TweedSA
PetricM
LiY
2005 Effectiveness of vaccine against medical consultation due to laboratory-confirmed influenza: results from a sentinel physician pilot project in British Columbia, 2004–05. Can Commun Dis Rep 31 181 192
11. SkowronskiDM
MasaroC
KwindtTL
MakA
PetricM
2007 Estimating vaccine effectiveness against laboratory-confirmed influenza using a sentinel physician network: results from the 2005–2006 season of dual A and B vaccine mismatch in Canada. Vaccine 25 2842 2851
12. SkowronskiDM
De SerresG
DickinsonJ
PetricM
MakA
2009 Component-specific effectiveness of trivalent influenza vaccine as monitored through a sentinel surveillance network in Canada, 2006–07. J Infect Dis 199 168 179
13. RodriguesL
KirkwoodBR
1990 Case-control designs in the study of common diseases: updates on the demise of the rare disease assumption and the choice of sampling scheme for controls. Int J Epidemiol 19 205 13
14. OrensteinWA
BernierRH
DonderoTJ
HinmanAR
MarksJS
1985 Field evaluation of vaccine efficacy. Bull WHO 63 1055 1068
15. Statistics Canada 2005 Canadian Community Health Survey (Cycle 3.1). Ottawa, ON
16. Statistics Canada 2009 Influenza Immunization Coverage by Province and age 2007–08. In: Table 105-0502. Health indicator profile, annual estimates, by age group and sex, Canada, provinces, territories, health regions (2007 boundaries) and peer groups, occasional (1209600 series). Available: http://cansim2.statcan.gc.ca/cgi-win/cnsmcgi.pgm?Lang=E&RootDir=CII/&Array_Pick=1&ArrayId=105-0502&C2DB=PRD&ResultTemplate=CII%2FCII
17. ItohY
ShinyaK
KisoM
WatanabeT
SakodaY
2009 In vitro and in vivo characterization of new swine-origin H1N1 influenza viruses. Nature 460 1021 1025
18. HancockK
VeguillaV
XiuhuaL
ZhongW
ButlerEN
2009 Cross-reactive antibody responses to the 2009 pandemic H1N1 influenza virus. 361 1 8
19. HakE
VerheijThJM
GrobbeeDE
NicholKL
2002 Confounding by indication in non-experimental evaluation of vaccine effectiveness: the example of prevention of influenza complications. J Epidemiol Community Health 56 951 955
20. JacksonLA
JacksonML
NelsonJC
NeuzilKM
WeissNS
2006 Evidence of bias in estimates of influenza vaccine effectiveness in seniors. Int J Epidemiol 35 337 344
21. JacksonLA
NelsonJC
BensonP
NeuzilKM
ReidRJ
2006 Functional status is a confounder of the association of influenza vaccine and risk of all cause mortality in seniors. Int J Epidemiol 35 345 352
22. KellyH
GrantK
2009 Interim analysis of pandemic influenza (H1N1) 2009 in Australia: surveillance trends, age of infection and effectiveness of seasonal vaccination. Eurosurveillance 14. Available: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19288. Accessed 26 February 2010
23. Garcia-GarciaL
Valdespino-GomezJL
Lazcano-PonceE
Jimenez-CoronaA
Higuera-IglesiasA
2009 Partial protection of seasonal trivalent inactivated vaccine against novel pandemic influenza A/H1N1 2009: case-control study in Mexico City. BMJ 339: b3928. Available: http://www.bmj.com/cgi/content/full/339/oct06_2/b3928 Accessed 26 February 2010
24. Echevarria-ZunoS
Mejia-ArangureJM
Mar-ObesoAJ
Grajales-MunizC
Robles-PerezE
2009 Infection and deaths from influenza A H1N1 virus in Mexico: a retrospective analysis. Lancet 374 2072 2079
25. GargiulloP
ShayD
KatzJ
BramleyA
NowellM
2009 Effectiveness of 2008–09 trivalent influenza vaccine against 2009 pandemic influenza A (H1N1) - United States, May–June 2009. MMWR Morb Mortal Wkly Rep 58 1241 1245
26. IulianoAD
ReedC
GuhA
DesaiM
KuttyP
2009 Notes from the field: outbreak of 2009 pandemic influenza A (H1N1) virus at a large public university in Delaware, April–May 2009. Clin Infect Dis 49 1811 1820
27. Crum-CianfloneNF
BlairPJ
FaixD
ArnoldJ
EcholsS
2009 Clinical and epidemiologic characteristics of an outbreak of novel H1N1 (swine origin) influenza A virus among United States military beneficiaries. Clin Infect Dis 49 1801 1810
28. JanjuaNZ
SkowronskiDM
HottesTS
De SerresG
CrowcroftNS
2009 Seasonal vaccine and H1N1. Selection bias explains seasonal vaccine's protection. BMJ 339 b4972
29. JanjuaNZ
SkowronskiDM
HottesTS
De SerresG
CrowcroftNS
2010 Bias and seasonal vaccine effectiveness against pandemic A/H1N1. Lancet 375 801 802
30. HoskinsTW
DaviesJR
SmithAJ
AlchinA
MillerCL
1976 Influenza at Christ's Hospital: March, 1974. Lancet 1 105 108
31. BodewesR
KreijtzJHCM
BaasC
Geelhoed-MierasMM
de MutsertG
2009 Vaccination against human influenza A/H3N2 virus prevents the induction of heterosubtypic immunity against lethal infection with avian influenza A/H5N1 Virus. PLoS ONE 4 e5538 doi:10.1371/journal.pone.0005538
32. BodewesR
KreijtzJHCM
RimmelzwaanGF
2009 Yearly influenza vaccinations: a double-edged sword? Lancet Infect Dis 9 784 788
33. PaleseP
2004 Influenza: new and old threats. Nat Med 10 S82 7
34. WebsterRG
1966 Original antigenic sin in ferrets: the response to sequential infections with influenza viruses. J Immunol 97 177 183
35. de St. FazekasG
WebsterRG
1966 Disquisitions on original antigenic sin, II: proof in lower creatures. J Exp Med 124 347 361
36. de St. FazekasG
WebsterRG
1966 Disquisitions of original antigenic sin, I: evidence in man. J Exp Med 124 331 345
37. KimJH
SkountzouI
CompansR
JacobJ
2009 Original antigenic sin responses to influenza viruses. J Immunol 183 3294 3301
38. StephensonJR
2005 Understanding dengue pathogenesis: implications for vaccine design. Bull WHO 83 308 314
39. SauterP
HoberD
2009 Mechanisms and results of the antibody-dependent enhancement of viral infections and role in the pathogenesis of coxsackievirus B-induced diseases. Microbes Infect 11 443 451
40. TakadaA
KawaokaY
2003 Antibody-dependent enhancement of viral infection: molecular mechanisms and in vivo implications. Rev Med Virol 13 387 398
41. GotoffR
TamuraM
JanusJ
ThompsonJ
WrightP
1994 Primary influenza A virus infection induces cross-reactive antibodies that enhance uptake of virus into Fc receptor-bearing cells. J Infect Dis 169 200 203
42. OchiaiH
KurokawaM
KurokiY
NiwayamaS
1990 Infection enhancement of influenza A H1 subtype viruses in macrophage-like P388D1 cells by cross-reactive antibodies. J Med Virol 30 258 265
43. OchiaiH
KurokawaM
HayashiK
NiwayamaS
1988 Antibody-mediated growth of influenza A NWS virus in macrophagelike cell line P388D1. J Virol 62 20 26
44. OchiaiH
KurokawaM
MatsuiS
YamamotoT
KurokiY
1992 Infection enhancement of influenza A NWS virus in primary murine macrophages by anti-hemagglutinin monoclonal antibody. J Med Virol 36 217 221
45. VincentAL
LagerKM
JankeBH
GramerMR
RichtJA
2008 Failure of protection and enhanced pneumonia with a US H1N2 swine influenza virus in pigs vaccinated with an inactivated classical swine H1N1 vaccine. Vet Microbiol 126 310 323
46. KitikoonP
NilubolD
EricksonBJ
JankeBH
HooverTC
2006 The immune response and maternal antibody interference to a heterologous H1N1 swine influenza virus infection following vaccination. Vet Immunol Immunopathol 112 117 128
47. KobingerGP
MeunierI
PatelA
PilletS
GreenJ
2010 Assessment of the efficacy of commercially available and candidate vaccines against a pandemic H1N1 2009 virus. J Infect Dis 201 1000 1006
48. GreenbaumJA
KotturiMF
KimY
OseroffC
VaughanK
2009 Pre-existing immunity against swine-origin H1N1 influenza viruses in the general human population. Proc Natl Acad Sci U S A 106 20365 20370 Available: http://www.pnas.org/content/106/48/20365. Accessed 26 February 2010
49. World Health Organization 2010 Pandemic (H1N1) 2009 – update 89. Weekly virological surveillance update. Available at: http://www.who.int/csr/disease/swineflu/laboratory26_02_2010/en/index.html. Accessed 26 February 2010
50. World Health Organization 2010 Recommended composition of influenza vaccines for use in the 2010 southern hemisphere influenza season. Available at: http://www.who.int/csr/disease/influenza/recommendations2010south/en/index.html. Accessed 26 February 2010
51. World Health Organization 2010 Recommended viruses for influenza vaccines for use in the 2010–2011 northern hemisphere influenza season. Available at: http://www.who.int/csr/disease/influenza/recommendations2010_11north/en/index.html. Accessed 26 February 2010
Štítky
Interní lékařstvíČlánek vyšel v časopise
PLOS Medicine
2010 Číslo 4
- Srovnání vlivu omeprazolu a pantoprazolu na antiagregační účinek klopidogrelu
- Fixní kombinace kandesartan/amlodipin v terapii arteriální hypertenze
- Současné postavení a přínos sartanů v klinické praxi
- Prognostický význam hladiny natriuretických peptidů při léčbě empagliflozinem
- Hypertrofická obstrukční kardiomyopatie ve světle moderní farmakoterapie – kazuistika
Nejčtenější v tomto čísle
- Preoperative/Neoadjuvant Therapy in Pancreatic Cancer: A Systematic Review and Meta-analysis of Response and Resection Percentages
- Economic Appraisal of Ontario's Universal Influenza Immunization Program: A Cost-Utility Analysis
- China's Engagement with Global Health Diplomacy: Was SARS a Watershed?
- Laboratory Capacity Building in Asia for Infectious Disease Research: Experiences from the South East Asia Infectious Disease Clinical Research Network (SEAICRN)
Zvyšte si kvalifikaci online z pohodlí domova
Mazová zátka a její řešení
nový kurzVšechny kurzy