
MRI signal intensity as a predictor of osteoporotic fractures?
Predikcia osteoporotických zlomenín na základe intenzity signálu MR?
Hyperintenzita pozorovaná na T1 vážených obrazoch (T1vo) magnetickej rezonancie (MR) môže indikovať pokles počtu buniek kostnej drene a zvýšenie obsahu tuku. Okrem parametrov z dvojenergetickej röntgenovej absorpciometrie (dual-energy X-ray absorptiometry, DEXA) bolo našim cieľom v tejto štúdii posúdiť využitie M-skóre z MR pre včasnú detekciu osteoporózy. Piatim novodiagnostikovaným osteoporotickým ženám boli stanovené: hustota kostného tkaniva (bone mass density, BMD), T-skóre a trabekulárne kostné skóre (trabecular bone score, TBS ) v oblasti lumbálnej chrbtice prostredníctvom DEXA, ktoré následne podstúpili MR vyšetrenie za účelom určenia hodnôt pomer signál-šum (signal-to-noise-ratio, SNR) z T1vo pre výpočet M-skóre. Medzi SNR/M-skóre verzus TBS sa zistila pozitívna korelácia a priblíženie sa k štatistickej významnosti pravdepodobne pre nižší počet probandov. Interakcia zobrazovacích metód ponúka predpoklad, žeby sa MR mohla stať neinvazívnou oportúnnou skríningovou modalitou pri diagnostike a skorej liečbe osteoporózy, vrátane včasnej predikcie osteoporotických zlomenín.
Klíčová slova:
DEXA, zlomenina, M-skóre, MR, TBS.
Authors:
Mikulová Udmila 1; Gičová Daša 2; Špakovská Tatiana 3; Lorinczová Zuzana 4; Kalafu-Tová Soňa 1; Blaščáková Mydlárová Marta 5
Authors place of work:
Department of Medical and Technical Disciplines in Health Care, Faculty of Health Care, University of Prešov, Prešov
1; Department of Radiology, Trnava University Hospital, Trnava
2; Clinic of Radiology, AGEL Košice-Šaca Hospital, Košice-Šaca
3; Osteocentre, AGEL Košice-Šaca Hospital, Košice-Šaca
4; Department of Biology, Faculty of Humanities and Natural Sciences, University of Prešov in Prešov, Prešov
5
Published in the journal:
Clinical Osteology 2025; 30(1): 36-40
Category:
Původní práce
Summary
Hyperintensity observed on T1 weighted images (T1WI) of magnetic resonance imaging (MRI) may indicate a decrease in bone marrow cell count and an increase in fat content. In addition to parameters from dual-energy X-ray absorptiometry (DEXA), our study aimed to assess the use of M-scores from MRI for early detection of osteoporosis. Five newly diagnosed osteoporotic women were determined: bone mass density (BMD), T-score and trabecular bone score (TBS) in the lumbar spine region by DEXA, who subsequently underwent MR examination to establish signal-to-noise-ratio (SNR) values from T1WI for M-score calculation. There was a positive correlation between SNR/M-score versus TBS, but this was only close to statistical significance, probably due to the lower number of probands. The interaction of imaging modalities suggests that MR could become a non-invasive opportunistic screening modality in the diagnosis and early treatment of osteoporosis, including the early prediction of osteoporotic fractures.
Keywords:
DEXA, fracture, M-score, MRI, TBS.
Introduction
Osteoporosis is a worldwide health problem. It is considered the most common multifactorial metabolic bone disease (1) and a frequent cause of fractures. Estrogen deficiency is a key cause of bone loss during menopause (2). The disease requires early and correct diagnosis. Appropriate treatment depends on an accurate assessment of bone health. DEXA is the gold standard in the diagnosis of osteoporosis (3). Due to the asymptomatic nature of osteoporosis, despite the need for bone mineral density (BMD) testing, many patients do not undergo early diagnosis by DEXA while attending for MRI scan due to lumbar spine pain and osteoporosis-related complications (4).
Increased bone marrow (BM) fat serves as a compensatory mechanism for the cellular content in the trabecular microarchitecture that is associated with osteoporosis. Bone marrow adipose tissue has been shown to indicate a significant increase in patients with osteoporosis, and there is an inverse relationship between BMD and adipose tissue in the vertebral bone marrow (5–7). The appearance of bone marrow is determined by its relative amounts of protein, fat, water, and cells on the MR pulse sequence. T1 weighted spin-echo images are the most accurate for evaluating BM cellular content due to their good detection of fat content. A decrease in bone marrow cell number and an increase in fat content are indicated by the hyperintensity observed on T1WI, which is associated with osteoporosis (4, 7, 8).
MRI of the lumbar spine is nowadays a frequently indicated examination. It has a prospective role in the diagnosis of osteoporosis and could be used as a screening tool (4). Koyama et al. (2013) concluded that routine MRI, particularly the SNR value from T1WI, has the potential to assess osteoporosis and may become a reliable diagnostic indicator through M-score (9). Quantitative M-scores and SNR evaluated from MR scans are suitable modalities for the detection of lumbar spine osteoporosis. Several studies have introduced the M-score, an analogue to the T-score from DEXA, based on the average signal-to-noise ratio of the L1–L4 vertebral bodies on T1WI (5–8).
The main aim of this pilot study, which was conducted in Slovak postmenopausal women diagnosed with osteoporosis, was to evaluate the correlation between lumbar spine SNR examined by MRI versus BMD from DEXA scanning and to observe the association between M-score (from MRI) versus T-score (from DEXA). Subsequently, through these correlations, confirm whether MRI as an imaging modality is appropriate/useful for early diagnosis of osteoporosis in the spine.
Material and methods
Research set
Five postmenopausal women of Slovak nationality, mean age 57 ± 5 years, were confirmed to have osteoporosis based on medical screening (personal and family history, biochemical and DEXA examination). After being instructed by an osteologist, they were recommended to undergo MRI of the L spine. Inclusion criteria for patients in the study included: women > 50 years, menopausal ≥ 12 months, newly diagnosed patients who had not been previously treated with any drugs affecting bone metabolism. The control group consisted of five women with a mean age of 23 ± 2 years who underwent MRI of the L spine for low back pain. All participating patients signed an informed consent to participate in this study and completed a questionnaire designed by us. This pilot study was approved by the Ethics Committee 1/2024 of the AGEL Hospital in Košice-Šaca.
DEXA examination
DEXA scanning of the lumbar spine was performed using a device - Hologic Discovery A (S/N 84182), which generated all the investigated values: T-score, Z-score, BMD and TBS (Fig. 1) according to the guidelines of the International Society for Clinical Densitometry (ISCD). A minimum of two consecutive levels are used to evaluate the lumbar T-score, after excluding vertebrae with structural degenerative abnormalities. All probands examined by DEXA scan had confirmed osteoporosis (T-score < -2.5).
MR imaging
Lumbar MR imaging was performed on a 1.2T Hitachi open magnet in the SAG T1vo and T2WI, AXIAL and STIR COR planes at the L1–L4 level. Assessment was obtained from the SAG T1 weighted spin-echo sequence (ETR = 2, TR = 700, TE = 12, pixel size = 0.586 mm, dfov = 55.57 × 30.00 cm) - the most suitable sequence for BM assessment.
Patient exclusion criteria were as follows:
1. MRI with contrast,
2. traumatic injury of the dorso-lumbar vertebrae,
3. absolute contraindications to MR,
4. patients refusing to participate.
In our study, 10 women underwent lumbar spine MRI: 5 women diagnosed with postmenopausal osteoporosis and 5 young women who were not diagnosed with osteoporosis but underwent MRI based on unknown low back pain in the sacral region. The examinations were performed at the AGEL Košice-Šaca Hospital and the time interval between DEXA and MR examination was maximum 1 month.
After the MR examination, the results were transferred to an off-line workstation (Radiant DICOM Viewer (64 -bit)) for post-processing. The region of interest (ROI) was manually placed in the form of a rectangle in the vertebral bodies of L1–L4, excluding cortical bone, subchondral abnormalities, focal lesions (e.g. hemangioma), and the posterior venous plexus. Another ROI was localized outside the patient’s body - to a location free of artifacts, for noise recording. The area of all manually placed ROIs was 0.40 cm2 (Fig. 2).
The M-score was calculated using the difference of the values: the signal-to-noise ratio (SNR) of L1–L4 in a postmenopausal woman diagnosed with osteoporosis and the SNR of the control group (ref). We then divided this difference by the SD of the control group (7, 10).


Statistical analysis
Statistical analysis and tests were selected according to the type of variable. Available statistical software IBM® SPSS® Statistics 29. 0. 2. 0 was used to calculate correlations. Graphs were created using RStudio 2023. 12. 1 software. Because the study contains a small sample of patients, Spearman’s Rho correlation calculator was preferred to Pearson’s correlation coefficient calculator to evaluate the correlations. Statistical tests were used to analyze the differences between the MRI results (calculated SNR and M-score) and the results from the DEXA scan (T-score, BMD, TBS).

Results and discussion
The DEXA scan is currently the best tool available for measuring bone density in terms of BMD (g/cm2). Although this examination is the unit of choice in the diagnosis of osteoporosis, it is less performed in patients who do not have fragility fractures even if they are confirmed to be at risk of fracture. These patients are not screened and treated for osteoporosis promptly. The DEXA scan has a high specificity but a low detection rate. Mechanical properties and bone quality depend on bone microarchitecture and mineral content. Therefore, it is advisable to measure TBS values of bone and other parameters undetectable by DEXA.
With increasing age, fat in the BM progressively increases and there is a proportional decrease in bone strength, thus TBS also changes. This is the basic principle on which MR evaluation is based. Shah LM and co-authors (2011) found that T1WI helps to assess cellular content in BM. Fat content due to its hydrophobic groups leads to T1 short relaxation time and causes diffusely increased hyperintensity at T1WI (11).
MRI of the lumbar spine is a routine examination, especially in the elderly due to low back pain, in this respect it can be used as a screening method to detect osteoporosis. The SNR and M-score values depend on the instrument on which the examination is performed. Each MRI technique is calibrated differently and has its threshold. It has been confirmed that BM signal intensity on standard T1WI is negatively correlated with BMD (5, 7). Jain M and co-authors (2023) found in their study that M-score negatively correlated with T score. Spearman’s correlation coefficient for spine T-score was -0.651 with p-value < 0.001. Thus, they demonstrated that fragility fractures related to osteoporosis could be accurately detected through MRI (6).
The limitations of our study are covered in the following points:
- Our study group, due to time limitation, was very small (5 patients) compared to foreign studies (ranging from 40–150 patients) (5–8). The difference in the M-score threshold may be due to the sample size and sample type, as our study group deliberately included postmenopausal women with hormonal changes.
- MRI examinations were performed using a 1.2T machine. In foreign literatures, a technique with at least 1.5T magnetic induction, and even the highest 7T, has been applied to MR examinations (5, 12, 13). Higher inductions are recommended to achieve more intense signal, higher spatial resolution and sensitivity.
On the plus side, our examinations were performed within one month of each other, and thus did not create a long time between examinations that could affect correlations between DEXA and MRI values.
SNR and M-score results were evaluated from the T1WI images. The SNR was obtained by dividing the mean signal intensity determined for the L1–L4 vertebrae by the standard deviation of the noise (Tab. 1).
In Tab. 2, we list all observed parameters related to MRI and DEXA examination.
Diagnostic SNRL1–L4 was calculated for each patient and applied to obtain an M-score (based on MRI) for a possible diagnosis of osteoporosis. The averaged SNRL1–L4 values of the control group (SNRref) and standard deviation (SDref) were also entered into the formula for calculating the M-score.
When comparing the values from the two imaging modalities in our study (Tab. 2), the highest T-scores and significantly high TBS from the DEXA scans (patient 3) were confirmed by the highest MRI intensity values (SNR and M-score). The lowest T-score and TBS from DEXA also showed lower values from the MRI scan, but not the lowest (patient 4).
When applying the correlations, SNR was found to be positively correlated with M-score (r = 1.000**), with no statistical significance, which differs from the 2019 Egyptian study where SNR was negatively correlated with M-score (r = -0.74, p < 0.0001) (7). Which can be justified by their larger patient sample studied (50) and by the fact that both quantitative SNR and M-score values will vary for each MR department according to the machine settings.
BMD values were positively correlated with T-scores (r = 0.975**) without statistical significance. In a 2018 Iranian study (1.5 T), the authors also confirmed a positive correlation (r = 0.943), however, in their case with statistical significance (4).
When comparing the values from DEXA scan (T-score, BMD) versus the values from MRI scan (M-score, SNR), the following findings were observed in our study:
- The modality values obtained from MRI (SNR/M-score) were similar when correlated with the values calculated by DEXA technique. M-score was negatively correlated with BMD (r = -0.300, p = 0.68) and with T-score (r = -0.36, p = 0.55).
- SNR was negatively correlated with BMD (r = - 0.300, p = 0.68) and with T-score (r = - 0.36, p = 0.55).
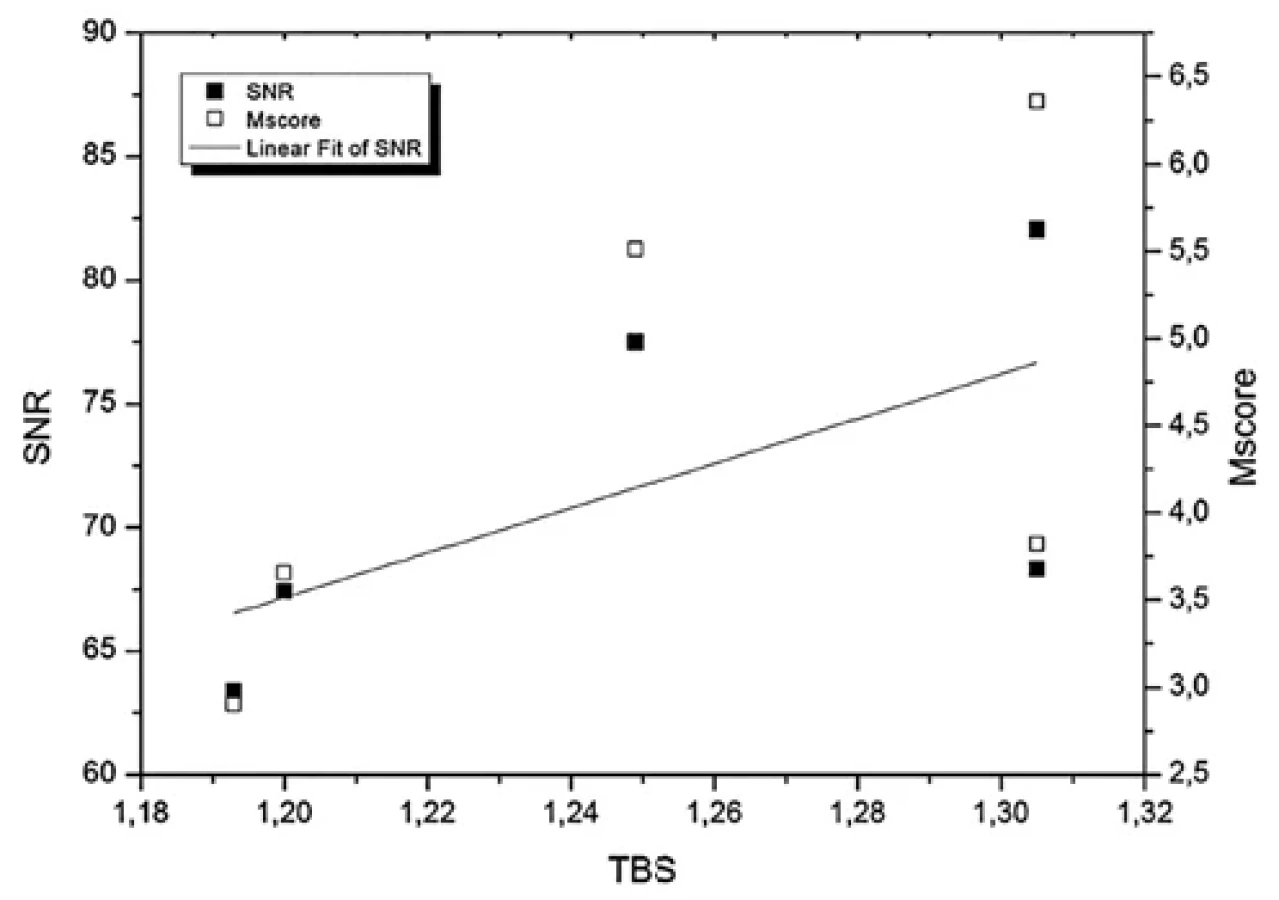
The graphs with SNR and M-score values correspond to the same result because M-score was calculated from SNR, which is confirmed in figure 3 when comparing these values with TBS.
All foreign publications studied report, as we do, negative correlations of these values: (M-score x T-score => r = -0.48 (6,7), r = -0.651 (6), r = -0.067 (5)), (M-score x BMD => r = -0.37 (7)), (SNR x T-score => r = -0.42 (7), r = -0.067 (5)), (SNR x BMD => r = -0.31(7)). In their case, probably due to the large sample of patients studied and the stronger magnetic induction (1.5–3 T), statistical significance (p < 0.0001) was confirmed, which is absent in our study.
However, the present work is the only pilot study to investigate the correlation of SNR and M-score (MR) with TBS (DEXA). The TBS index from DEXA examination, assesses bone texture and microarchitecture and has been an increasingly studied parameter in the field of osteology in recent years. Therefore, with the expansion of the study sample, this correlation could be beneficial in terms of highlighting the importance of MRI in osteoporosis of the spine and in the prediction of fractures.
When correlating SNR/M-score versus TBS, a positive correlation was found (r = 0.82; p = 0.089) (Fig. 4). Although statistical significance was not confirmed for these parameters either, it is close to p < 0.05. This may indicate that with an increase in the number of patients and the implementation of higher magnetic induction MRI scans, this comparison between DEXA and MRI values could become important for radiologists and osteologists when investigating osteoporosis.
The limitations of our study are as follows:
- Our cohort was very small (5 patients) due to time limitation compared to foreign studies (ranging from 40–150 patients) (5–8). There is a need to expand this study sample in the future to represent the population. The difference in the M score cut-off may be due to the sample size, but also to the type of sample, as our study group deliberately included postmenopausal women with hormonal changes.
- The MRI scans were performed on a 1.2T machine. In the foreign literature, MRI examinations are performed with a magnetic induction of at least 1.5T and as high as 7T (5, 12, 13). Higher inductions are recommended to obtain a more intense signal, higher spatial resolution and sensitivity.
- Due to the small number of patients studied, it was not possible to include ROC curves that would show the relevance of osteoporosis screening using the open 1.2T Hitachi magnet, in particular the specificity and sensitivity of the MRI device.
- The observed values from DEXA and MRI scans (Tab. 2) indicate a slight deviation from the expected values and confirm that the study sample is not large enough to exclude a single case with a deviation, which could lead to the establishment of MRI signal thresholds also indicating a high risk of fractures. To propose such values, it would be necessary to continue this pilot study, expand the studied sample of probands and to propose a ROC curve.
On the plus side, our examinations were performed within one month of each other, and thus did not create a long time between examinations that could affect correlations between DEXA and MRI values.
The present study, as well as other foreign studies (5–8), suggests that MRI scanning could become useful in the evaluation of osteoporosis, allowing the patient to avoid even low-level ionizing radiation.
Although MRI cannot replace DEXA in the diagnosis of osteoporosis, it may have prognostic value (function) and serve as a useful tool in clinical practice to better understand the pathophysiology of this metabolic disease. This study is specific because we only followed postmenopausal women. In the future, it is necessary to include men in similar studies, as men over 50 years of age are also at increased risk of developing osteoporosis.



Conclusion
The integration of several imaging modalities shows the potential to improve osteoporosis treatment and patient outcomes as this area develops. It might be beneficial to include SNR and M-score as part of routine lumbar spine MRI evaluation, which is considered a simple, reliable and reproducible screening method for osteoporosis. MRI does not pose a radiation burden, which is particularly beneficial for postmenopausal women and elderly patients at risk for osteoporosis. This fact could become a useful tool for early detection of individuals requiring medical - orthopaedic/osteological assistance. This could prevent osteoporosis, fractures, improve outcomes and reduce the economic burden caused by expenditure on medication and ongoing health care.
Zdroje
1. Sözen T, Özışık L, Başaran NÇ. An overview and management of osteoporosis. Eur J Rheumatol. 2017;4(1):46-56.
2. Cheng CH, Chen LR, Chen KH. Osteoporosis Due to Hormone Imbalance: An Overview of the Effects of Estrogen Deficiency and Glucocorticoid Overuse on Bone Turnover. Int J Mol Sci. 2022;23(3):1376.
3. Sangondimath G, Sen RK, T FR. DEXA and Imaging in Osteoporosis. Indian J Orthop. 2023;57(Suppl 1):82-93.
4. Shayganfar A, Khodayi M, Ebrahimian S, et al. Quantitative diagnosis of osteoporosis using lumbar spine signal intensity in magnetic resonance imaging. Br J Radiol. 2019;92(1097):20180774.
5. Atik İ, Atik S, Gül E, et al. Contribution of Lumbar Vertebral Magnetic Resonance Imaging to Diagnosis in Women with Osteoporosis. Turk J Osteoporos. 2022;28(2):77-82.
6. Jain M, Naik S, Prasad Mishra N et al. Correlation of bone mineral density using the dual energy x-ray absorptiometry and the magnetic resonance imaging of the lumbar spine in Indian patients. Journal of Orthopaedics. 2023;40 : 65-69.
7. Saad MM, Ahmed AT, Mohamed KE, et al. Role of lumbar spine signal intensity measurement by MRI in the diagnosis of osteoporosis in post-menopausal women. Egypt J Radiol Nucl Med. 2019;50(35).
8. Naik S, Jain M, Bhoi K, et al. Correlation between Vertebral Marrow Fat Fractionin MRI Using DIXON Technique and BMD in DXA in Patients of Suspected Osteoporosis. Indian J Radiol Imaging. 2023;34 : 239-245.
9. Koyama H, Yoshihara H, Kotera M, et al. The quantitative diagnostic capability of routine MR imaging and diffusion-weighted imaging in osteoporosis patients. Clin Imaging 2013;37(5):925-9.
10. Bandirali M, Di Leo G, Papini JDE. A new diagnostic score to detect osteoporosis in patientsundergoing lumbar spine MRI. Eur Radiol. 2015;25 : 2951-2959.
11. Shah LM, Hanrahan CJ. MRI of spinal bone marrow: part I, techniques and normal age-related appearances. AJR Am J Roentgenol. 2011;197(6):1298-308.
12. Trentadue M, Sozzi C, Idolazzi L, et al. Magnetic resonance imaging at 3.0-T in postmenopausal osteoporosis: a prospective study and review of the literature. Radiol Bras. 2022;55(4):216-224.
13. Berman N, Brent H, Chang G, et al. Transient osteoporosis: Not just the hip to worry about. Bone Reports. 2016;5 : 308-311.
Štítky
Biochemie Dětská gynekologie Dětská radiologie Dětská revmatologie Endokrinologie Gynekologie a porodnictví Interní lékařství Ortopedie Praktické lékařství pro dospělé Radiodiagnostika Rehabilitační a fyzikální medicína Revmatologie Traumatologie OsteologieČlánek vyšel v časopise
Clinical Osteology

2025 Číslo 1
- Diosmin a hesperidin: Co ukazuje farmakokinetika?
- Inkontinence jako důsledek operačního zákroku na prostatě
- Plicní screening v Česku zatím zachytil přes stovku případů karcinomu plic
Nejčtenější v tomto čísle
- Vitamin D – current overview of the issue and specifics in nephrological practice
- Secondary Osteoporosis
- A completely now approach to the issue of bone disease in patients with chronic kidney disease – what KDIGO practice recommendations can we expect? Commentary on the KDIGO 2025 Controversies Conference.
- From despair to results: Clinical experience and effective strategies in the treatment of calciphylaxis
Zvyšte si kvalifikaci online z pohodlí domova
Mazová zátka a její řešení
nový kurzVšechny kurzy