
Results of the first 12 months treatment of macular edema complicating BRVO in patients treated with ranibizumab
Authors:
L. Lalinská; J. Krásný; P. Studený; M. Veith
Authors place of work:
Oftalmologická klinika Fakultní nemocnice Královské Vinohrady a 3. lékařské fakulty Univerzity Karlovy v Praze, přednosta kliniky: doc. MUDr. Pavel Studený, PhD., MHA
Published in the journal:
Čes. a slov. Oftal., 74, 2018, No. 2, p. 62-67
Category:
Původní práce
doi:
https://doi.org/10.31348/2018/1/3-2-2018
Summary
The aim of the study:
Retrospective evaluation of the first 12 months treatment of macular edema in BRVO with ranibizumab based on anatomical and functional parameters.
Methods:
54 eyes with macular edema complicating BRVO were included in the study, with an average initial best corrected visual acuity 4/16 ETDRS charts, an average central retinal thickness 512.3 μm, and in average 4 months till the beginning of treatment with ranibizumab. After 3 initial injections of 0.5 mg ranibizumab treatment was performed in pro re nata regimen, with adjuvant laser (grid laser photocoagulation) as an additional treatment option. The number of injections administered, the number of eyes where grid laser photocoagulation was provided, functional parameters as a letter gain and BCVA (eyes with final BCVA ≥ 4/8 ETDRS, final BCVA in according to initial BCVA) and anatomical parameters as a mean CRT and CRT ≤ 250 μm, respectively ≤ 300 μm were evaluated.
Results:
In the whole group, an average of 4.8 injections of ranibizumab were administered in the first 12 months. Grid laser photocoagulation was performed in 42 eyes: in 8 eyes prior to the beginning of treatment with ranibizumab, 7 eyes before and during the treatment, 29 eyes only during the treatment. The main gain of letters after 12 months of treatment was +16.5 letters, with 63¨% (n = 34) eyes earning ≥ 15 letters. In the whole group 72 % (n = 39) eyes achieved the resulting BCVA ≥ 4/8 ETDRS after 12 months of treatment. The eyes with initial BCVA ≥ 4/10 ETDRS resulted in BCVA ≥ 4/8 ETDRS in 96 % (n = 23 eyes) and 11 eyes even achieved BCVA ≥ 4/4. The mean CRT after 12 months of treatment was 290.3 μm, 33.3 % of eyes had final CRT ≤ 250 μm, and 64.8 % had final CRT ≤ 300 μm.
Conclusion:
When applying a relatively low number of injections in the first year of treatment with ranibizumab, the final best corrected visual acuity was very good at the end of the observation period, and its dependence on the initial best corrected visual acuity was confirmed. Satisfactory results of central retinal thickness were found as well.
Key words:
branch retinal vein occlusion, macular edema, ranibizuma
INTRODUCTION
Branch retinal vein occlusion (BRVO) is one of the 2 main forms of retinal vein occlusion (RVO), which after diabetic retinopathy is the second most common vascular pathology of the retina. At present, the incidence is estimated at approximately 520 new cases of RVO per million people, in which 442 cases concern BRVO (16). Occlusion of the temporal venous branch in connection with affliction of the macular landscape and the development of macular edema is accompanied as a rule by varying degrees of deterioration of visual acuity, whereas occlusion of the nasal branch may remain undetected.
A typical location for the occurrence of vein occlusion in BRVO is arteriovenous crossing (AV crossing), with subsequent venous stasis of blood (4, 24) and formation of thrombosis (8, 13). In the case of voluminal overload of the venous channel as a consequence of an imbalance between the arterial and venous volume (A/V imbalance), the vascular auto-regulatory mechanisms of the retina are activated, the effectiveness and capacity of which are variable. In the case of exhaustion of these mechanisms, a deepening of macular edema (ME) takes place, with a substantial deterioration of central visual acuity (17, 18). The influence of hypoxia is accentuated in the pathogenesis of ME in RVO. A decisive role in the development of ME is played by vascular endothelial growth factor A (VEGF-A), the levels of which under hypoxic conditions are elevated in the chamber fluid and in the vitreous body (11, 22). Of other mediators generating ME the role of interleukins (IL-1ꞵ and IL-6) has been demonstrated, as well as tumour necrosis factor and a range of prostaglandins (1, 11).
In the pathogenesis of RVO it is not possible to overlook the influence of systemic risk factors (6, 7, 12, 23) supporting the progression of atherosclerotic vascular changes. In the group of patients with a positive anamnesis of thrombotic episodes and in patients younger than 50 years without systemic risk factors, it is furthermore recommended to conduct an examination for congenital blood coagulation disorders (14).
The prognosis of BRVO is fairly favourable. In the natural course, in 50-60% of cases of BRVO, resulting best corrected visual acuity (BCVA) is 6/12 of Snellen's optotype and better. In the remaining 40% resulting BCVA is 6/18 and worse, in which 20% of the total number have resulting BCVA of 6/60 and worse (5, 10).
As regards prognostic factors, initial BCVA is considered highly significant. As a result it is recommended upon analysis of the results to take into account the influence of initial BCVA on final vision. Occlusion with initial BCVA of 6/24 Snellen's optotype and worse has been defined as prognostically unfavourable occlusion (19).
The aim of treatment in BRVO is to resolve the 2 main complications threatening sight, namely chronic ME and ischaemia manifesting itself in the formation of neovascularisations (NV). In the great majority of cases in BRVO, treatment is focused precisely on the treatment of ME.
Grid laser photocoagulation (grid LPC) has been the long-term therapeutic standard for ME on a background of BRVO. Another laser technique – arteriolar constriction (“crimping technique”) in the occluded region improves drainage of ME as a consequence of the reduction of inflow into the place of occlusion (L'Esperance, 1975), and is suitable for the treatment of haemodynamically severe occlusions with extensive retinal haemorrhages, with high macular ischaemia and thus also poor initial BCVA (20).
At present an already verified therapeutic modality is intravitreal application of ranibizumab, a humanised fragment of a monoclonal antibody with non-selective binding to all isoforms of vascular endothelial growth factor A (VEGF-A). This prevents VEGF-A from binding to receptors VEGFR-1 and VEGFR-2 localised on the endothelial cells of the retinal capillaries. A further possibility is intravitreal application of aflibercept, the effect of which is based on a blockade of VEGF-A and placental growth factor (PIGF).
Of the group of corticosteroids, in therapy it is possible to use dexamethasone depot with progressive release into the vitreous body over a period of up to six months.
COHORT AND METHOD
In our cohort we evaluated 54 eyes (29 right and 25 left) of 54 patients (27 men and 27 women) with an average age of 65 years (range 42-88 years), who were classified for treatment with ranibizumab at the Department of Ophthalmology at Královské Vinohrady University Hospital in the period from May 2103 to December 2016.
All the patients in the evaluated cohort underwent a comprehensive ocular examination before the actual commencement of treatment. BCVA was examined on an ETDRS optotype from 4 metres. There followed a biomicroscopic examination of the anterior segment of the eye and the fundus in artificial mydriasis, supplemented by quantification of macular edema (CRT-central retinal thickness) by OCT scan on a Cirrus HD-OCT instrument (Carl Zeiss Meditec, Dublin, CA). At the conclusion fluorescence angiography (FAG) was performed for an assessment of the presence of ischaemic changes of the retina.
In the above-stated period a total of 63 eyes were classified for treatment with ranibizumab. In the cohort of 54 eyes which was evaluated, the following were not included: a) patients with advanced cataract (n=1) or substantial secondary cataract (n=1) upon entry, b) patients in whom no improvement of BCVA by at least 5 letters of ETDRS and a reduction of CRT by a minimum of 100 µm or beneath 250 µm was recorded following the initial 3 injections of 0.5 mg of ranibizumab, on the basis of which a change of therapeutic preparation was selected (n=3), c) patients with affiliated diabetic ME or macular traction (n=2) and d) patients who had been treated in the preceding period by another intravitreal preparation (n=2).
In the case of patients in the evaluated cohort, of systemic risk factors the most frequently appearing was arterial hypertension (n=35 patients), followed by dyslipidemia (n=22 patients) and type 2 diabetes mellitus (n=12 patients). In 6 patients BRVO was the initial manifestation of an untreated systemic pathology. Of ocular factors glaucoma was present in 6 patients.
A condition for classification for treatment with ranibizumab was that all indication restrictions for payment were met.
The average time from the beginning of subjective complaints until the application of the first injection of 0.5 mg ranibizumab was 4 months on average (1 month n=7 eyes, 2 months n=6 eyes, 3 months n=10 eyes, 4 months n=8 eyes, 5 months n=13 eyes, 6 months n=5 eyes, 7 months n=3 eyes, 10 months n=1 eye, 11 months n=1 eye). Before the commencement of treatment with ranibizumab, grid LPC was performed in 13 eyes in the drainage area of the afflicted vein, and in 2 eyes arteriolar constriction was performed. Average initial BCVA in the evaluated cohort was 4/16 ETDRS optotype and average initial CRT was 512.3 µm. According to FAG this concerned a non-ischaemic type of occlusion in all the affected eyes.
In all the eyes in the evaluated cohort, at the beginning of treatment an initial 3 injections of 0.5 mg ranibizumab were applied at an interval of one month. Further injections were then applied in a pro re nata (PRN) regimen with regard to the conditions of reapplication stipulated by the SPC. In the case of stable visual acuity or disappearance of ME on the OCT scan patients were observed, if applicable in the interim period grid LPC was supplemented in the drainage area of the afflicted vein, on the precondition that no retinal haemorrhages were present in the area in question and the performance of laser treatment of the retina was therefore safe.
During the course of the observation period of 12 months (the beginning was determined by the date of application of the 1st injection), evaluation of treatment was conducted after 3, 6, 9 and 12 months. We evaluated change of the number of letters read, and BCVA was furthermore evaluated in relation to initial BCVA, specifically in 3 smaller subgroups according to initial BCVA: 1) 4/8-4/10, 2) 4/12-4/25 and 3) 4/32-4/40 ETDRS optotype. We also evaluated change of CRT in relation to the initial CRV value, the average resulting CRT and the proportion of patients with attained CRT < 250 and 300 µm respectively. At the conclusion of the observation period, the number of administered injections and the use of adjuvant grid LPC were also evaluated.
RESULTS
Functional results
The average gain of letters throughout the entire cohort following the application of the initial 3 doses of 0.5 mg ranibizumab was +15.9 letters, during the course of the observation period this remained without significant fluctuations, and at the end of the first year of treatment the gain reached +16.5 letters (graph 1).

6 M: after 6 months of treatment
9 M: after 9 months of treatment
12 M: after 12 months of treatment
A gain of at least 5 letters of ETDRS optotype was attained in all the evaluated eyes in the cohort following the initial 3 injections, in which 26 eyes (48%) gained > 15 letters. After 12 months of treatment a gain of > 15 letters was recorded in 34 eyes (63%), as shown in table 1.

6 M: after 6 months of treatment
9 M: after 9 months of treatment
Resulting BCVA was evaluated throughout the entire observation period with focus on the representation of eyes with resulting BCVA of > 4/8 ETDRS optotype (table 2), and evaluation of resulting BCVA was expressed also in the subgroups according to initial BCVA (table 3). After 12 months of treatment, a total of 39 eyes (72.2%) attained resulting BCVA of > 4/8 ETRDS optotype. The best results of BCVA were recorded in eyes with a prognostically favourable BCVA of 4/8-4/10 ETDRS optotype. In this group 23 eyes (95.8%) had resulting BCVA of > 4/8 after 12 months of treatment, and 11 of these had BCVA of > 4/4.

6 M: after 6 months of treatment
9 M: after 9 months of treatment
12 M: after 12 months of treatment

Anatomical results
Change of central retinal thickness (CRT), specifically its reduction from its initial value, which throughout the entire cohort was 512.3 µm, was most pronounced after 3 months of treatment, when CRT was reduced by 247.9 µm, attaining a resulting average value of CRT 264.4 µm. At further follow-up examinations (after 6, 9 and 12 months of treatment) this reduction was balanced, but somewhat smaller (graph 2).
6 M: after 6 months of treatment
9 M: after 9 months of treatment
12 M: after 12 months of treatment
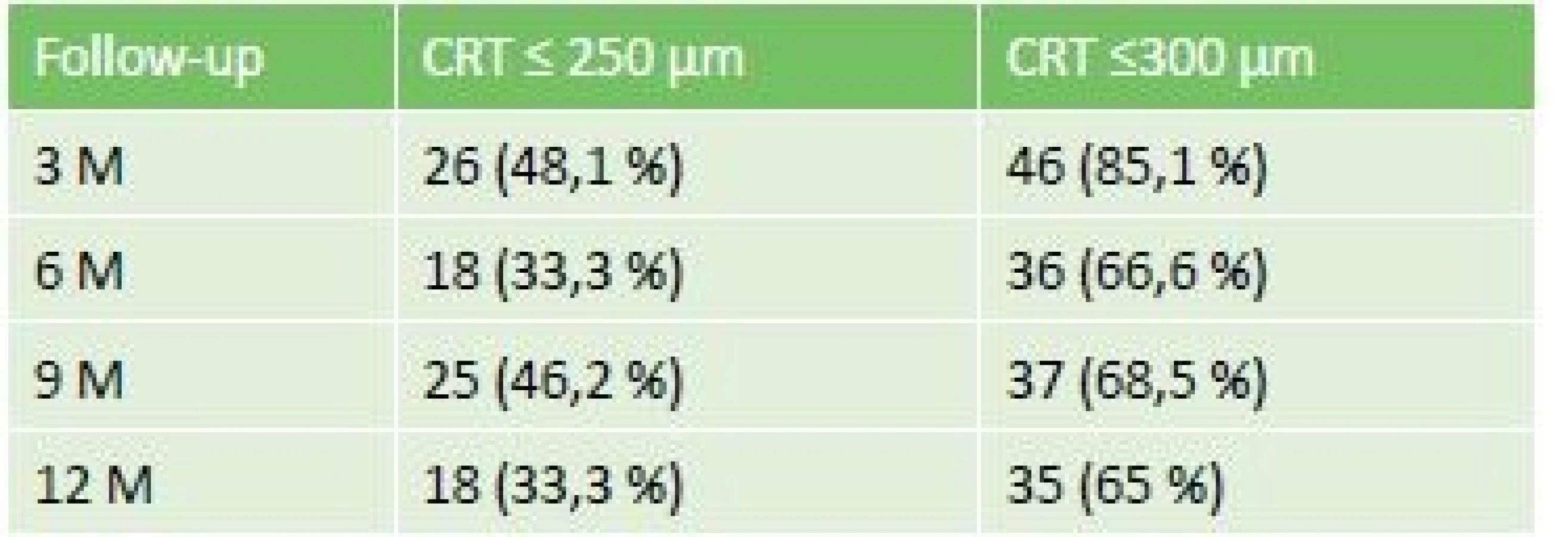
In addition to resulting average CRT for the entire cohort (table 4), which at the end of the first year of treatment attained a value of 290.3 µm, the representation of eyes with CRT of < 250 and < 300 µm was also evaluated (table 5). In the subgroup with resulting CRT of < 300 µm the largest representation of eyes, i.e. 46 eyes (85.1%) was after 3 months of treatment, after 12 months of treatment 35 eyes (64.8%) maintained CRT of < 300 µm. At the end of the observation period 23 eyes (42.6%) had a dry macula for a period of more than 6 months.

6 M: after 6 months of treatment
9 M: after 9 months of treatment
12 M: after 12 months of treatment
6 M: after 6 months of treatment
9 M: after 9 months of treatment
12 M: after 12 months of treatment
INJECTIONS AND ADJUVANT LPC
During the first 12 months of treatment, an average of 4.8 injections of 0.5 mg ranibizumab (3 injections n=15 eyes, 4 injections n=9 eyes, 5 injections n=10 eyes, 6 injections n=16 eyes, 7 injections n=3 eyes, 9 injections n=1 eye) were applied throughout the entire cohort.
Before the commencement of treatment with ranibizumab, 13 eyes were treated with the aid of grid LPC (which in 7 of these eyes was also supplemented during the course of treatment with ranibizumab). Out of the total number of 54 eyes, grid LPC was performed on 42 eyes (77.8%).
DISCUSSION
Anti-VEGF preparations are the pharmaceutical of first choice in the treatment of ME complicating BRVO. In this indication it has been possible to apply ranibizumab in the Czech Republic since 2012. The effectiveness and safety of ranibizumab has been clinically verified by the prospective study BRAVO (2), in which patients were divided into 3 branches according to the applied active agent (0.3 mg ranibizumab, 0.5 mg ranibizumab or sham injection). The group treated with 0.5 ranibizumab comprised 131 eyes. Average initial BCVA was 4/16 ETDRS and average CRT 520.5 µm. In the first (therapeutic) phase a total of 6 intravitreal injections were applied to all eyes. There then followed a six month observation phase, in which treatment was administered in a PRN regimen, if BCVA was < ETDRS or CRT > 250 µm. Laser treatment could be supplemented once during the course of the treatment period and once during the course of the observation period upon the fulfilment of the defined criteria.
In our observation a total of 54 eyes were evaluated. The average time from the beginning of the complaints until the first application of injection was 4 months. Average initial BCVA was 4/16 ETDRS and average CRT was 512.3 µm, which is very similar baseline data in comparison with the BRAVO study. However, the therapeutic regimen differed. In the first 3 months, 3 injections were applied to all eyes, and further applications were then conducted within a PRN regimen. Out of the total number of eyes classified for treatment with ranibizumab (n=63), the response to treatment was insufficient in only 3 of these after the initial 3 doses of ranibizumab, and for this reason there was an early change of the pharmaceutical preparation to dexamethasone depot. The initial parameters and attained results of these 3 patients were not included as a part of our evaluation.
In our cohort, the PRN regimen after 3 initial injections reduced the average number of injections for the entire observation period of 12 months to an average of 4.8 injections, in comparison with 8.8 injections in the BRAVO study, and the number of follow-up examinations was also reduced (in the BRAVO study these were conducted once per month). In our cohort there were 15 eyes which did not require further application of treatment after the initial 3 injections. Grid LPC was performed on 77.8% of eyes (42 eyes), which within the framework of the evaluated cohort represents a higher proportion than in the BRAVO study, in which only 23.7% of eyes underwent laser treatment.
The average gain of letters in the BRAVO study after 6 months of treatment was +18.3 letters, which was maintained at the same value also after 12 months of treatment. Of this, 60% of eyes recorded a gain of > 15 letters after 12 months, and 66.4% of eyes recorded BCVA of > 4/8 ETDRS. In our cohort the average gain of letters was slightly smaller – after 12 months of treatment it reached +16.5 letters, in which 63% of eyes (n=34) recorded a gain of > 15 letters after 12 months. BCVA of > 4/8 was recorded in 39 eyes (72.2%) after 12 months of treatment. With regard to initial BCVA, the best results of resulting BCVA were attained in eyes with initial BCVA of > 4/10, in which 23 eyes (out of a total number of 24 eyes) attained BCVA of > 4/8 after 12 months of treatment, and of these 11 eyes recorded BCVA of > 4/4 ETDRS.
As regards the anatomical results, reduction of CRT from the initial values in our cohort was most pronounced after 3 months of treatment, when CRT was reduced by 247.9 µm to an average value of CRT 264.4 µm. After 12 months of treatment average CRT was 290.3 µm. In the subgroup with resulting CRT of < 250 µm, the largest representation of eyes (n=26, 48.1%) was after 3 months of treatment, after 12 months of treatment 18 eyes (33%) retained this CRT value. In the BRAVO study these anatomical results were better, as many as 86.3% of eyes attained CRT < 250 µm after 12 months of treatment. If we were to consider CRT < 300 µm to be satisfactory resulting CRT, then 35 eyes (64.8%) in our cohort belonged to this group at the end of the observation period.
However, regular practice differs from the ideal, strictly controlled conditions of trials.
In 2014 a collective of authors from Denmark published annual results of patients with BRVO treated with ranibizumab (3). 57 eyes were evaluated at a follow-up examination after 6 months, and 38 eyes after 12 months of observation. A gain of more than 15 letters of ETDRS and CRT less than 275 µm was considered a successful functional result. Average initial BCVA was identical to the BCVA in our cohort, but average initial CRT was higher (638 µm). During the course of the first year of treatment, an average of 5 injections were administered, 3 initial doses at the beginning and then further until the disappearance of macular edema. In the case of an unsatisfactory response to ranibizumab, therapy was supplemented with adjuvant LPC of the macula. The average gain of letters was +9.4 letters after 6 months (31.6% with gain of > 15 letters) and +11.6 letters after 12 months (26.3% gain of > 15 letters); average reduction of CRT was -217 µm with average CRT of 421 µm after 6 months; reduction of CRT was -248 µm with average CRT of 373 µm after 12 months. In comparison with these results, in our cohort average initial and resulting CRT was lower, which would explain the greater gain of letters in our cohort. This correlation between retinal thickness and BCVA has been statistically significantly demonstrated – according to the regression model a reduction of BCVA by 1.9 letters from initial BCVA corresponds to each 100 µm of thickening of CRT of the macula (21). The results may generally be distorted by the representation of eyes with prognostically worse initial BCVA and the number of eyes with very good BCVA (4/10-4/8), due to the “ceiling effect” (lower potential to achieve a gain of more than 15 letters). The results of the Danish study may have been influenced also by the different number of eyes which were evaluated after 6 and 12 months of treatment, as well as by the inconsistent observation period, which at the end was variable (9-15 months).
In a further study conducted by a Viennese team (15), an average of 3 injections were applied within the first 6 months in a group of 14 eyes treated from the beginning in a PRN regimen, and in the second half of the observation only 1 injection was applied on average. Adjuvant laser treatment was supplemented in 4 eyes. All 14 eyes in the cohort recorded a gain of > 15 letters. The average period of duration of ME was short, only 51 days. In this case it is possible to a large extent to attribute the functional improvement with a small number of injections to timely classification for treatment and therefore knowledge of the influence of the duration time of ME on the final results of BCVA, in which the best results can be achieved in the case of duration of ME of less than 3 months (9). In our cohort the average duration of ME before the application of the 1st injection was 4 months, in which 23 eyes out of 54 had a duration of less than 3 months, thus the duration of ME influenced our results altogether positively.
CONCLUSION
Our aim was to retrospectively evaluate the functional and anatomical results of the first year of treatment of ME complicating BRVO with ranibizumab in regular clinical practice. Our observed cohort of patients was distinguished by relatively timely classification for treatment (on average 4 months), PRN treatment regimen after the 3 initial injections, relatively small number of administered injections (4.4 injections) and adjuvant grid LPC in the majority of eyes (77.8%). Our clinical experience at the end of the first year of treatment was positive. Patients with BRVO remain under regular observation, and if applicable, their treatment is continuing according to the finding. The therapeutic approach in the first year of treatment is reflected in the results of further years, and as a result, it is possible to evaluate its effectiveness only after a time interval upon evaluating the long-term results.
The authors of the study declare that no conflict of interest exists in the compilation, theme and subsequent publication of this professional communication, and that it is not supported by any pharmaceuticals company.
MUDr. Lucia Lalinská, FEBO
Oftalmologická klinika Fakultní nemocnice
Královské Vinohrady
a 3. lékařské fakulty Univerzity Karlovy
v Praze
Šrobárova 1150/50, Praha 10, 100 34
lucia.gogorova@gmail.com
Zdroje
1. Bringmann, A., Reichenbach, A., Wiedeman, P.: Pathomechanism of cystoid macular edema. Ophtalmic Res, 36; 2004 : 241-249.
2. Brown, DM., Campochiaro, PA., Bhisitkul, RB., et al.: Sustained benefits from ranibizumab for macular edema following branch retinal vein occlusion: 12-month outcomes of a phase III study. Ophtalmology, 118; 2011 : 1594-1602.
3. Brynskov, T., Kemp, H., Sørensen, TL.: Intravitreal ranibizumab for retinal vein occlusion through 1 year in clinical practice. Retina, 34; 2014 : 1637-1643
4. Duker, JS., Brown, GC.: Anterior location of the crossing artery in branch retinal vein obstruction. Arch Ophtalmol, 107; 1989 : 998-1000.
5. Gutman, FA., Zegarra, H., Zakov, ZN.: The natural course of temporal retinal vein. Trans Am Acad Ophtalmol Otolaryngol, 78; 1974 : 178-192.
6. Hayreh, SS., Zimmermann, B., McCarthy, MJ., et al.: Systemic diseases associated with various types of retinal vein occlusion. Amer J Ophthalmol, 131; 2001 : 61-77.
7. Cheung, N., Klein, R., Wang, JJ., et al.: Traditional and novel cardiovascular risk factors for retinal vein occlusion: the multiethnic study of atherosclerosis. Invest Ophthalmol Vis Sci, 49; 2008 : 4297-4302.
8. Christoffersen, NLB., Larsen, M.: Pathophysiology and hemodynamics of branch retinal vein occlusion. Ophthalmology, 106; 1999 : 2054-2062.
9. Jaissle, GB., Szurman, P., Feltgen, N.: Predictive factors for functional improvement after intravitreal bevacizumab therapy for macular edema due to branch retinal vein occlusion.Graefes Arch Clin Exp Ophthalmol, 249; 2011 : 183-192.
10. Michels, RG., Gass, JD.: The natural course of temporal retinal branch vein obstruction. Trans Am Acad Ophtalmol Otolaryngol, 79; 1974 : 166-177.
11. Noma, H., Funatsu, H., Yamasaki, M., et al.: Pathogenesis of macular edema with branch retinal vein occlusion and intraocular levels of vascular endothelial growth factor and interleukin 6. Am J Ophtalmol, 140; 2005 : 256-261.
12. O’Mahoney, DT., Wong, T., Ray, JG.: Retinal vein occlusion and traditional risk factors for atherosclerosis. Arch Ophthalmol, 126; 2008 : 692-699.
13. Osinbowale, O., Ali, L., Chi, YW.: Venous trombembolism: a clinical review. Postgrad Med, 122; 2010 : 54-65.
14. Rehák, M., Krčová, V.: Poruchy hematokoagulační kaskády. In Řehák, J., Rehák, M., et al., Venózní okluze sítnice. Praha, Grada, 2011, 49-54.
15. Rezar, S., Eibenberger, K., Bühl, W., et al.: Anti-VEGF treatment in branch retinal vein occlusion: a real-world experience over 4 years. Acta Ophtal, 93; 2015 : 719–725.
16. Rogers, S., McIntosh, RL., Cheung, N., et al.: International Eye Consortium: The prevalence of retinal vein occlusion: pooled data from population studies from United States, Europe, Asia, and Australia. Ophtalmology, 117; 2010 : 313-319.
17. Řehák, J.: Branch retinal vein occlusion: Part 1. Pathogenesis, collaterals and visual prognosis. New approach. New Trends Ophtalmol, 12; 1997 : 41-45.
18. Řehák, J.: Venózní okluze sítnice: I. Příspěvek k patogenezi cirkulačních změn. Českoslov. Oftalmol, 49; 1993 : 145-147.
19. Řehák, J., Dušek, L., Chrapek, O. et al.: Initial visual acuity is an important prognostic factor in patients with branch retinal vein occlusion. Ophtalmic Research 45; 2011 : 204-209.
20. Řehák, J., Rehák, M.: Fotokoagulační terapie okluze větve sítnicové vény. In Řehák, J., Rehák, M., et al., Venózní okluze sítnice. Praha, Grada, 2011, 89-93.
21. Šín, M.: Optická koherenční tomografie. InŘehák, J., Rehak, M., et al., Venózní okluze sítnice. Praha, Grada, 2011, 74-75.
22. Vinores, SA., Youssri, AI., Luna, JD.: Upregulation of vascular endothelial growth factor in ischemic and non-ischemic human and experimental retinal disease. Histol Histopathol., 12; 1997 : 99-109.
23. Wong, TY., Larsen, EK., Klein, R., et al.: Cardiovascular risk factors for retinal vein occlusion and arteriolar emboli: the Atherosclerosis Risk in Communities & Cardiovascular Health studies. Ophthalmology, 112; 2005 : 540–547.
24. Zhao, J., Sastry, SM., Sperduto, RD., et al.: Arteriovenous crossing patterns in branch retinal vein occlusion. Ophtalmology, 100; 1993 : 423-428.
Štítky
OftalmologieČlánek vyšel v časopise
Česká a slovenská oftalmologie

2018 Číslo 2
- Selektivní laserová trabekuloplastika nesnižuje nitroční tlak více než argonová laserová trabekuloplastika
- Progresi glaukomu je třeba hodnotit strukturálními i funkčními parametry
- Ztráta centrálního vidění po filtrujících operacích glaukomu
- Od PGF-2 alfa-isopropyl esteru k latanoprostu: přehled vývoje Xalatanu
- Compliance u pacientů s glaukomem
Nejčtenější v tomto čísle
- CHANGE OF CENTRAL AND PERIPHERAL VISION IN PATIENT WITH SYMPTOMATIC CYST OF RATHKE'S CLEFT FOLLOWING TRANSSPHENOIDAL RESECTION.
- The use of micropulse laser in patients with diabetic macular edema at the Department of Ophthalmology, Faculty Hospital Hradec Králové
- Results of the first 12 months treatment of macular edema complicating BRVO in patients treated with ranibizumab
- ACUTE MYOPIA WITH ELEVATION OF INTRAOCULAR TENSION AS AN ADVERSE SIDE EFFECT OF ANTIDEPRESSANT MEDICATION
Zvyšte si kvalifikaci online z pohodlí domova
Mazová zátka a její řešení
nový kurzVšechny kurzy