
Quantifying the Number of Pregnancies at Risk of Malaria in 2007: A Demographic Study
Background:
Comprehensive and contemporary estimates of the number of pregnancies at risk of malaria are not currently available, particularly for endemic areas outside of Africa. We derived global estimates of the number of women who became pregnant in 2007 in areas with Plasmodium falciparum and P. vivax transmission.
Methods and Findings:
A recently published map of the global limits of P. falciparum transmission and an updated map of the limits of P. vivax transmission were combined with gridded population data and growth rates to estimate total populations at risk of malaria in 2007. Country-specific demographic data from the United Nations on age, sex, and total fertility rates were used to estimate the number of women of child-bearing age and the annual rate of live births. Subregional estimates of the number of induced abortions and country-specific stillbirths rates were obtained from recently published reviews. The number of miscarriages was estimated from the number of live births and corrected for induced abortion rates. The number of clinically recognised pregnancies at risk was then calculated as the sum of the number of live births, induced abortions, spontaneous miscarriages, and stillbirths among the population at risk in 2007. In 2007, 125.2 million pregnancies occurred in areas with P. falciparum and/or P. vivax transmission resulting in 82.6 million live births. This included 77.4, 30.3, 13.1, and 4.3 million pregnancies in the countries falling under the World Health Organization (WHO) regional offices for South-East-Asia (SEARO) and the Western-Pacific (WPRO) combined, Africa (AFRO), Europe and the Eastern Mediterranean (EURO/EMRO), and the Americas (AMRO), respectively. Of 85.3 million pregnancies in areas with P. falciparum transmission, 54.7 million occurred in areas with stable transmission and 30.6 million in areas with unstable transmission (clinical incidence <1 per 10,000 population/year); 92.9 million occurred in areas with P. vivax transmission, 53.0 million of which occurred in areas in which P. falciparum and P. vivax co-exist and 39.9 million in temperate regions with P. vivax transmission only.
Conclusions:
In 2007, 54.7 million pregnancies occurred in areas with stable P. falciparum malaria and a further 70.5 million in areas with exceptionally low malaria transmission or with P. vivax only. These represent the first contemporary estimates of the global distribution of the number of pregnancies at risk of P. falciparum and P. vivax malaria and provide a first step towards a more informed estimate of the geographical distribution of infection rates and the corresponding disease burden of malaria in pregnancy.
: Please see later in the article for the Editors' Summary
Published in the journal:
. PLoS Med 7(1): e32767. doi:10.1371/journal.pmed.1000221
Category:
Research Article
doi:
https://doi.org/10.1371/journal.pmed.1000221
Summary
Background:
Comprehensive and contemporary estimates of the number of pregnancies at risk of malaria are not currently available, particularly for endemic areas outside of Africa. We derived global estimates of the number of women who became pregnant in 2007 in areas with Plasmodium falciparum and P. vivax transmission.
Methods and Findings:
A recently published map of the global limits of P. falciparum transmission and an updated map of the limits of P. vivax transmission were combined with gridded population data and growth rates to estimate total populations at risk of malaria in 2007. Country-specific demographic data from the United Nations on age, sex, and total fertility rates were used to estimate the number of women of child-bearing age and the annual rate of live births. Subregional estimates of the number of induced abortions and country-specific stillbirths rates were obtained from recently published reviews. The number of miscarriages was estimated from the number of live births and corrected for induced abortion rates. The number of clinically recognised pregnancies at risk was then calculated as the sum of the number of live births, induced abortions, spontaneous miscarriages, and stillbirths among the population at risk in 2007. In 2007, 125.2 million pregnancies occurred in areas with P. falciparum and/or P. vivax transmission resulting in 82.6 million live births. This included 77.4, 30.3, 13.1, and 4.3 million pregnancies in the countries falling under the World Health Organization (WHO) regional offices for South-East-Asia (SEARO) and the Western-Pacific (WPRO) combined, Africa (AFRO), Europe and the Eastern Mediterranean (EURO/EMRO), and the Americas (AMRO), respectively. Of 85.3 million pregnancies in areas with P. falciparum transmission, 54.7 million occurred in areas with stable transmission and 30.6 million in areas with unstable transmission (clinical incidence <1 per 10,000 population/year); 92.9 million occurred in areas with P. vivax transmission, 53.0 million of which occurred in areas in which P. falciparum and P. vivax co-exist and 39.9 million in temperate regions with P. vivax transmission only.
Conclusions:
In 2007, 54.7 million pregnancies occurred in areas with stable P. falciparum malaria and a further 70.5 million in areas with exceptionally low malaria transmission or with P. vivax only. These represent the first contemporary estimates of the global distribution of the number of pregnancies at risk of P. falciparum and P. vivax malaria and provide a first step towards a more informed estimate of the geographical distribution of infection rates and the corresponding disease burden of malaria in pregnancy.
: Please see later in the article for the Editors' Summary
Introduction
Malaria in pregnancy can have devastating consequences to a pregnant woman and the developing fetus, but comprehensive estimates of the annual number of women who become pregnant each year in malaria endemic areas and are therefore at risk of malaria are not available, particularly for Latin America and the Asia-Pacific regions. These figures are an important first step towards informing policy makers and for estimating the regional needs for therapeutic and disease prevention tools for malaria in pregnancy. The most cited global estimate is from the Roll Back Malaria Partnership, which states that “each year approximately 50 million women living in malaria endemic countries throughout the world become pregnant” [1]. However, an explanation of the methods used to derive these estimates is not provided. More comprehensive estimates exist for Africa and are provided by the Africa Regional Office (AFRO) of the World Health Organization (WHO) in their widely quoted strategic framework document for malaria prevention and control during pregnancy in the African region [2]. Their estimate of 24.6 million pregnancies at risk of malaria (predominantly P. falciparum), is based on the number of live born babies delivered in malarious areas of Africa in the year 2000 using a combination of malaria risk maps [3] and estimates of the number of live births from UNICEF [4]. A more recent estimate by the WHO states that “In Africa, 30 million women living in malaria endemic areas become pregnant each year” [5]. Estimates for outside of Africa are less clear, particularly for P. vivax. P. vivax is the most widely distributed human malaria parasite and co-occurs with P. falciparum in tropical areas but also occurs in temperate regions outside the limits of P. falciparum transmission. It is the major cause of malaria in much of Asia and Latin America [6],[7], and recent evidence has shown that P. vivax infections are far from benign and can result in significant morbidity in pregnant women with serious consequences for maternal and infant health [8]–[10].
Here we define a global estimate of the number of pregnancies at risk of P. falciparum and P. vivax malaria in 2007 by combining malaria spatial limits developed by the Malaria Atlas Project (MAP; www.map.ox.ac.uk), which define the total population at risk of malaria [11], with country-specific demographic data on women of childbearing age provided by the United Nations and published data on induced abortions and spontaneous pregnancy loss.
Methods
Data Sources
The global limits of P. falciparum malaria
The initial focus of the Malaria Atlas Project has been P. falciparum [12] due to its global epidemiological significance [13] and better prospects for its control and local elimination [14]. The global spatial limits of P. falciparum malaria transmission in 2007 have recently been mapped. This was done by triangulating data on transmission exclusion using biological rules based on temperature and aridity limits on the bionomics of locally dominant Anopheles vectors, data on nationally reported case incidence rates, and other medical intelligence [15]. The resulting map stratifies the malaria endemic world by stable and unstable transmission in 2007 [15]. Unstable transmission refers to areas where transmission is plausible biologically, but limited, with a clinical incidence of less than one case per 10,000 population per year. Stable transmission refers to areas with a minimum of one clinical case per 10,000 population per year [15].
The global limits of P. vivax malaria
Initial attempts to map the limits of P. falciparum and P. vivax transmission were made by Guerra et al. [16],[17]. The resulting maps and “masks” (mapped areas that are filtered and excluded from analyses) used were later tested against the Malaria Atlas Project parasite prevalence database to assess their feasibility [18],[19]. This testing revealed that the accuracy to define areas of zero transmission risk due to very low population densities was limited because of the coarse spatial resolution of the initial map. Moreover, in the initial mapping [16],[17], a high density population mask was used on the basis of the assumption that no transmission occurs in areas where the population density is so high that conditions become unsuitable for transmission through the process of urbanization. However, recent analyses [19] provide evidence suggesting that high density population masks and urban extent maps should not be used to map zero risk because some transmission can occur in high density urban areas, although this is significantly lower than in rural areas [18],[19]. Therefore, for the current analyses, the P. vivax limits were redefined using the same methods as in Guerra et al. [16],[17], but without applying the population-based masks. Also, previously excluded P. vivax endemic countries have now been added after a more extensive review of the literature; these include Comoros, Djibouti, Madagascar, and Uzbekistan. This refinement of the spatial limits of transmission for P. vivax accounted for an approximate 19% increase in the population at risk (PAR) compared with previous estimates [16],[17], principally (18%) due to the inclusion of major cities.
Gridded population data
The Global Rural-Urban Mapping Project (GRUMP) alpha version provides gridded population counts and population density estimates for the years 1990, 1995, and 2000, both adjusted and unadjusted to the United Nations' national population estimates [11],[20]. The adjusted population counts for the year 2000 were projected to 2007 by applying national, medium variant, intercensal growth rates by country [21] using methods described previously [22].
Annual number of pregnancies per country
The number of pregnancies was calculated as the sum of the number of live births, induced abortions, and spontaneous pregnancy loss (including miscarriages and stillbirths) in 2007.
Live births
The annual number of live births in 2007 was estimated per country using demographic data on the proportion of women of childbearing age (WOCBAs) within a population and the total fertility rates. The data were abstracted from the United Nations' national population estimates, which provide publicly accessible demographic information by year, age, sex, and country for Africa, Asia, and the Americas [23]. The number of WOCBAs in each country, defined as the mid-year resident number of women aged between 15 and 49y, was obtained for the years 2005 and 2010 (interim years are not available), and the number of WOCBAs for 2007 was calculated as the midpoint between the 2005 and 2010 estimates. The fraction of WOCBAs per country was then calculated as the number of WOCBAs in 2007 divided by the mid-year resident population at risk in 2007 (available by year).
The total fertility rate (TFR) is an age-standardised measure of fertility and corresponds to the total number of children that would be born alive to a woman entering her childbearing years at age 15y if she lived to the end of her childbearing years (age 49y) and if her fertility during these 35 reproductive years was the same as the average woman of childbearing age. The total fertility rate divided by 35 is the average number of live births per WOCBA per year and when multiplied by 1,000 this is expressed as the rate of live births per 1,000 WOCBAs per year.
Induced abortions, miscarriages, and stillbirth rates
Subregional data on induced abortion rates were obtained from a recently published review that calculated the worldwide, regional, and subregional incidence of safe and unsafe abortions in women of child bearing age in 2003 by use of reports from official national reporting systems, nationally representative demographic health surveys, hospital data, other surveys, and published studies [24].
Country-specific information on stillbirth rates was abstracted from model-based estimates published by Stanton et al. [25] that derived data from vital registration, demographic and health surveys (DHS), and data from study reports integrated into a regression model. Regional estimates were used for three malaria endemic countries for which country-specific estimates were not available (French Guiana, Mayotte, and Timor-Leste).
Country-specific data on miscarriages (spontaneous abortions) are not available. To calculate the proportion of pregnancies resulting in miscarriage, a method was applied that uses multipliers to work backwards from the (known) number of live births and induced abortions to recover the (unknown) underlying number of pregnancies that “produced” them, as described in detail previously [24],[26]–[28]. The method takes account of pregnancies that are terminated voluntarily during the period of risk for miscarriage and estimates the number of spontaneous pregnancy loss (stillbirths and miscarriages) as 10% of induced abortions plus 20% of live births. It is based on clinical studies of rates of pregnancy loss by gestational age that indicate that for each 100 induced abortions an additional ten clinically recognised pregnancies will have aborted spontaneously prior to the average gestational age of induced abortions in that population, and that approximately 120 additional clinically recognised pregnancies are required to “produce” 100 live births [27],[28]. For example, in Afghanistan it was estimated that in 2007 1.182 million live births occurred among a population of 27 million and a further 0.284 million induced abortions occurred. The number of spontaneous pregnancy losses (the sum of the number of stillbirths and miscarriages) was therefore estimated at 0.2×1,182 plus 0.1×0.284 = 0.265 million, and the total number of pregnancies as 1.731 million. The reported number of miscarriages used in this manuscript represents the number of spontaneous pregnancy losses calculated through the multiplier method as described above, minus the country-specific number of stillbirths obtained from the review by Stanton et al. [25]. The estimates provided in this study refer to clinically recognised pregnancies and do not take into account the potentially large but unknown rates of embryonic loss that may occur in the first 4–6 wk of gestation.
Estimating the annual number of pregnancies exposed to malaria
To obtain the total population at risk, the limits of stable and unstable P. falciparum transmission and the limits of P. vivax transmission described above were overlaid onto the Global Rural-Urban Mapping Project (GRUMP) alpha surface, projected to 2007. For every malaria endemic country of the world, the population within each set of limits was extracted, following approaches described previously [13]. The number of pregnancies at risk of malaria was then calculated from the total annual number of pregnancies estimated to have occurred in 2007 in the entire country multiplied by the fraction of the total resident population living within the spatial limits of malaria transmission in that country.
Results
Tables 1 and 2 provide a summary of the total population living within the global spatial limits of malaria transmission in 2007, and the corresponding number of total population, pregnancies, and live births, stratified by species and transmission patterns (within areas of assumed unstable and stable P. falciparum transmission), globally and by WHO region.


The compiled data showed that, globally, 125.2 million women living in areas with P. falciparum and/or P. vivax transmission became pregnant in 2007 : 77.4 million (61.8%) in the countries that fall under the regional office of the WHO for the South East Asian (SEARO) and the Western Pacific Region (WPRO); 30.3 million (24.2%) in AFRO; 13.1 million (10.5%) in the Eastern Mediterranean and European Region (EMRO and EURO); and only 4.3 million (3.4%) in the American Region (AMRO) (Table 3). Figures 1 and 2 display the same analysis by species, but depicted by continent rather than by WHO region. Of the 125.2 million pregnancies, 82.6 million (66.0%) are estimated to result in live births; 48.8 million (63.0%), 22.1 million (72.7%), 9.0 million (68.8%), and 2.7 million (63.1%) in the SEARO/WPRO, AFRO, EMRO/EURO, and AMRO regions, respectively (Table 4). It illustrates that the proportional distribution of pregnancies at risk resulting in live births is slightly different from the distribution of total pregnancies at risk, primarily reflecting the differences in the proportion of pregnancies ending in induced abortions, which is much lower in the AFRO region (11.9%) compared to the global average in the malaria endemic countries of 19.5% [24].
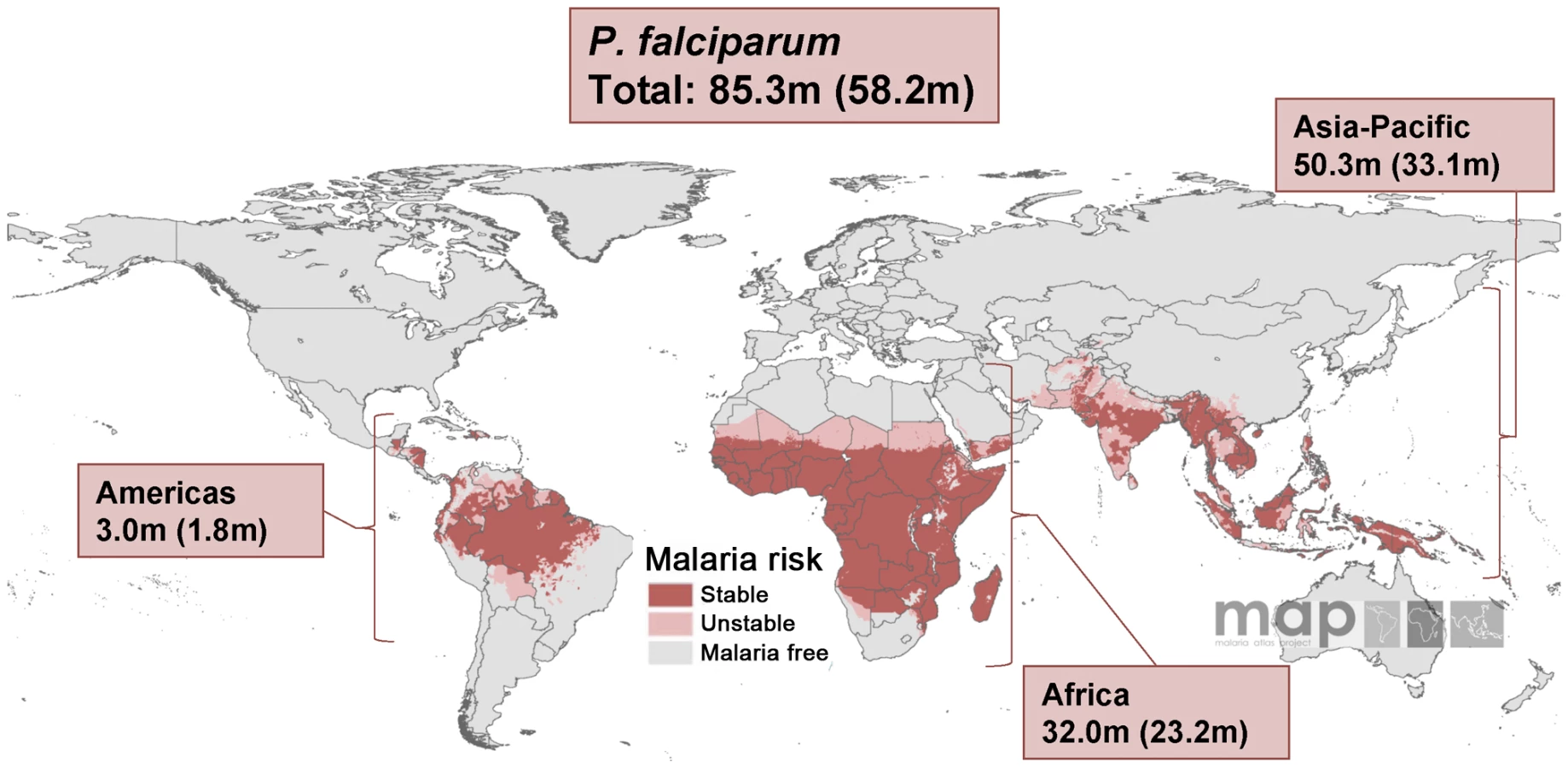


P. falciparum Malaria
Of the 125.2 million pregnancies defined above, 85.3 million occur in areas with P. falciparum transmission, 51.8% of them (44.2 million) are in the combined SEARO-WPRO regions and 35.1% (30.0 million) in the AFRO region. The remainder live in the EMRO-EURO (9.6%) and AMRO regions (3.5%) (Figure 3; Table 3). As expected, the top five ranked countries with the highest number of pregnancies at risk of P. falciparum malaria were the malaria endemic countries with the largest overall populations: India (28.2 million), Nigeria (6.5 million), Indonesia (4.4 million), Pakistan (3.7 million), and the Democratic Republic of the Congo (3.3 million). Overall, 64.1% of 85.3 million pregnancies at risk of P. falciparum malaria live in areas with assumed stable transmission (Figure 3). However, this varies widely by region; from 98.7% in the AFRO region to none in the EURO region. As depicted in Figure 3, 55.3% of the 44.2 million pregnancies at risk of P. falciparum in the WPRO/SEARO region occur in areas of very low and unstable transmission.

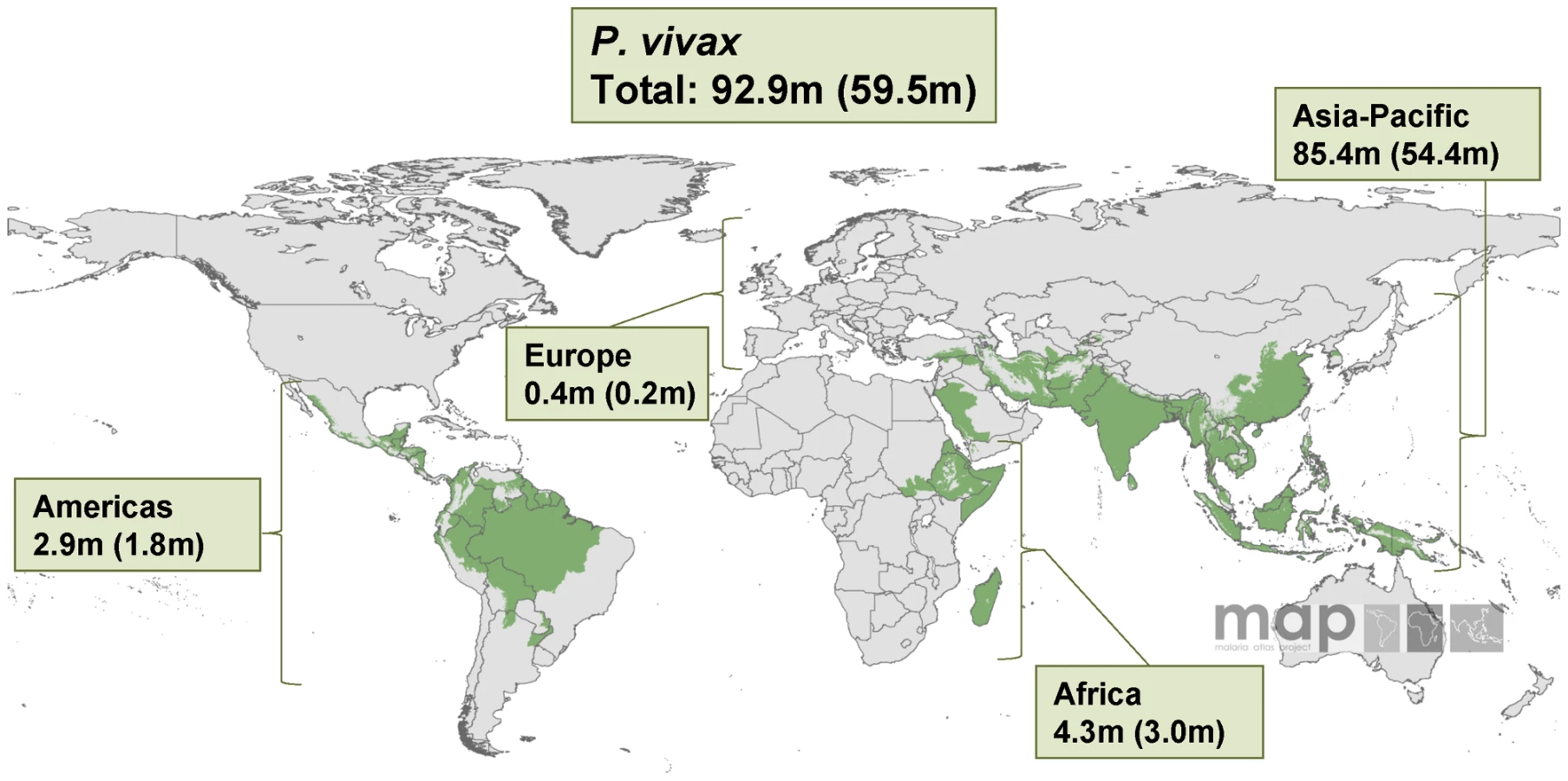
P. vivax Malaria
Globally, an estimated 92.9 million pregnancies occurred in areas endemic for P. vivax in 2007 (including in areas where both P. falciparum and P. vivax co-exist) (Figure 2). The top five ranked countries include: India (32.9 million), China (21.2 million), Indonesia (6.3 million), Pakistan (5.8 million), and Bangladesh (4.7 million). In the WPRO/SEARO region, where the majority of the populations at risk of P. vivax live (Figure 4), approximately 98.2% of those pregnancies in malaria endemic countries occur in areas with P. vivax transmission (alone or combined with P. falciparum). By contrast this was only 11.9% for the AFRO region where P. vivax transmission is principally restricted to the horn of Africa region, Madagascar, and the Comoros islands (Figure 4).

The country-specific demographic data and population at risk estimates (Table S1), as well as total pregnancies at risk and by specific pregnancy outcomes (live births, induced abortions, stillbirths, and miscarriages; Table S2) and summary estimates by other regional categories (continents instead of WHO regions; Table S3), are provided as supplemental information. In addition, information is provided illustrating which countries are included in the different WHO regions (also see Figure S1) [29]. In brief, all malaria endemic countries on the African continent fall under the Africa Regional Office (AFRO), with the exception of Djibouti, Somalia, and Sudan, which fall under the EMRO office.
Discussion
This is the first time, to our knowledge, that contemporary species-specific estimates of the annual number of pregnancies at risk of malaria globally have been made. Our findings suggest that in 2007 approximately 125 million pregnancies occurred in areas with P. falciparum and/or P. vivax transmission, resulting in 83 million live births; representing approximately 60% of all pregnancies globally. Approximately 85 million pregnancies occurred in areas with P. falciparum transmission and 93 million in areas with transmission of P. vivax transmission, of which about 53 million occurred in areas where both species co-exist. The pregnancies at risk estimates for P. falciparum and P. vivax in Africa (32 million [30 million in the WHO-AFRO region]) are consistent with the previous estimates by WHO (25–30 million). By contrast, the numbers at risk outside Africa are much higher (95 million) than previously estimated (25 million). Comparisons between the estimates produced in this study and the previous WHO estimates are made difficult because details of the methodology used by the WHO is not provided and it is not clear if they included all transmission areas or only areas with stable malaria transmission. Inclusion of only those areas with stable P. falciparum transmission in our study resulted in global risk estimates of just less than 55 million pregnancies, 31 million in Africa and 23 million in the other regions, i.e., very similar to the previous WHO estimates. However, the numbers of pregnancies at risk outside Africa increase almost 4-fold if areas with unstable P. falciparum transmission are included (clinical incidence <1 per 10,000 population/year) (30 million) and areas situated in the temperate regions outside the limits of P. falciparum transmission that have P. vivax transmission only (40 million) are also included. It is also not clear if the previous WHO estimates included pregnancies resulting in live births only or included adjustments for induced abortions or spontaneous pregnancy loss. Since only approximately two-thirds of all pregnancies result in live births, estimates that include all pregnancies are about one-third higher than estimates based on live births only.
Although risk estimates are widely quoted figures, it is important to place them in perspective. The estimates provided here merely define the global distribution of pregnancies that occur within the global spatial limits of malaria transmission. These estimates therefore represent “any risk” of exposure to malaria during pregnancy, and do not represent the distribution of actual incidence or health burden on mothers and unborn babies, which is beyond the scope of this paper. More than half (71 million) of the 125 million pregnancies occur in areas with unstable P. falciparum transmission (31 million) or with transmission of P. vivax only (40 million), and the risk of acquiring malaria in these areas is extremely low. Thus, although these 71 million pregnancies represent more than 50% of the global number of pregnancies at risk, they may only contribute a small proportion to the number of infections in pregnancy. For example, if the actual incidence of malaria infection in these very low transmission areas is 1 in 10,000 per person-year (52 wk), and if the average pregnancy resulting in a live birth takes 38 wk from fertilisation to term, then 71 million pregnancies at risk may result in only 5,188 actual malaria infections, whereas in areas with infection rates of 1.36 or higher per person-year, all term pregnancies have been potentially exposed to malaria. Furthermore, the definition of stable transmission for P. falciparum used included all areas with more than one clinical case per 10,000 population per year. This included almost all pregnancies at risk in the AFRO Region (99% of the 30 million pregnancies at risk) and 25 million of the 95 million (26%) pregnancies in the other WHO regions. However, these stable transmission strata cover a very wide range of transmission intensities and the actual risk of infection to the 55 million individuals and the impact on maternal and infant health varies enormously within this range.
At the higher end of the transmission spectrum, the majority of malaria infections in pregnancy remain asymptomatic or pauci-symptomatic, yet are a major cause of severe maternal anaemia and preventable low birth weight, especially in the first and second pregnancies. In areas with stable, but low transmission, and certainly in areas with unstable and exceptionally low transmission, infections can become severe in all gravidae groups because most women of childbearing age in these regions have low levels of pre-pregnancy and pregnancy-specific protective immunity to malaria [30]. The most recent version of the World Malaria Map [28] from the Malaria Atlas Project shows that 89% of the populations in stable P. falciparum areas outside Africa live in areas characterised by low malaria endemicity (defined as P. falciparum parasite rate in children 2–10 y of age of ≤5%). This total includes all of the stable P. falciparum transmission areas in the Americas, and 88% of the populations at risk in the Central and South-East Asia-Pacific region [31]. Our estimates do not take seasonality into account and include all pregnancies occurring throughout the year, whereas those pregnancies that occur outside of the transmission season may be at no risk, or very low risk of exposure.
Our risk estimates for P. vivax are likely to be less accurate than those for P. falciparum because of greater uncertainties about the basic biology of transmission and clinical epidemiology. For example, the climatic constraints on P. vivax transmission are less well defined, the accuracy of clinical reporting of P. vivax in areas with coincidental P. falciparum is poor, and the untreated hypnozoite stage of P. vivax, which can remain dormant in infected liver cells for months or years, provides an additional challenge to the interpretation of prevalence and incidence data [15]. We used a refined P. vivax risk map that resulted in a 19% increase over previous population at risk estimates (adjusted for population growth) [18],[19], principally resulting from the removal of the population density masks and thereby the inclusion of many large cities. In most of these cities, pregnancies will be at low or very low risk of autochthonous infections. Imported malaria associated with travel to rural areas may be a greater risk factor in these cities. We did not consider infections with P. ovale or P. malariae, as their distribution is not well described and the adverse effects on maternal health and the newborn infant are unknown.
In the current analysis we used the map of the global spatial limits of P. falciparum malaria, which stratifies the malaria endemic world by stable and unstable transmission published in 2008 [15].This map uses a simple divide between very low risk and higher transmission intensities and a crude proxy to account for the corresponding levels of acquired immunity in women of childbearing age. As a next step, we will examine the burden of malaria in pregnancy in terms of health impact on the pregnant women (e.g., febrile episodes, impact on maternal anaemia and maternal mortality), the newborn baby (e.g., impact on the frequency of preterm births and low birth-weight) and the infant (e.g., susceptibility to malaria). For this project, we will use the more refined P. falciparum transmission intensity model of risk within the defined stable limits which was developed recently by the Malaria Atlas Project [31], allowing disease impact calculations across multiple transmission strata to be made. It is also important to take the different pregnancy outcomes into account in these further burden estimates. Of the 125 million pregnancies, one in five are estimated to be terminated voluntarily during the period of risk for miscarriage, and only about two-thirds (82.6 millions) are expected to result in live births. Although malaria in pregnancy is associated with miscarriages and stillbirths [30], the majority of the health and economic burden is likely through the impact on pregnancies that result in live births by increasing the risk of preterm births and low birth-weight [30] and by modifying the susceptibility to malaria in the infant [32]–[34].
Most of the existing research and policy guidance for malaria control in pregnancy has focussed on P. falciparum in the stable transmission regions of sub-Saharan Africa. The results of this study are consistent with the previous WHO-RBM risk estimates for areas with stable P. falciparum malaria in Africa, but our work offers advancement on the existing risk estimates for malaria endemic countries outside Africa. In these regions, the burden of malaria in pregnancy is less well defined, both in terms of the number of pregnancies and its actual impact on health. Policy guidelines for malaria control in pregnancy are also less well developed for these regions.
These estimates of the number of pregnancies at risk of malaria provide a first step towards a spatial map of the burden of malaria in pregnancy and a more informed platform with which to estimate the associated disease and economic impact and its geographical distribution. Such global estimates provide guidance in terms of priority setting for resource allocation for both research and policy for the control of malaria in pregnancy. This project provides a dynamic framework that allows risk estimates to be updated when new risk maps of P. falciparum and P. vivax become available as the world attempts to move towards malaria elimination and eradication.
Supporting Information
{kind=link}
Zdroje
1. RBM Pregnant women and Infants Geneva WHO Available:http://malaria.who.int/pregnantwomenandinfants.html Accessed 5 January 2010
2. World Health Organization 2004 A strategic framework for malaria prevention and control during pregnancy in the African region Brazzaville World Health Organization: Regional Office for Africa AFR/MAL/04/01 AFR/MAL/04/01
3. SnowRW
CraigM
DeichmannU
MarshK
1999 Estimating mortality, morbidity and disability due to malaria among Africa's non-pregnant population. Bull World Health Organ 77 624 640
4. United Nations Children's Fund 1998 The state of the world's children New York Oxford University Press
5. World Health Organization 2003 Geneva WHO Available: http://www.who.int/features/2003/04b/en/ Accessed 5 January 2010
6. BairdJK
2007 Neglect of Plasmodium vivax malaria. Trends Parasitol 23 533 539
7. HaySI
GuerraCA
TatemAJ
NoorAM
SnowRW
2004 The global distribution and population at risk of malaria: past, present, and future. Lancet Infect Dis 4 327 336
8. SinghN
ShuklaMM
SharmaVP
1999 Epidemiology of malaria in pregnancy in central India. Bull World Health Organ 77 567 572
9. NostenF
McGreadyR
SimpsonJA
ThwaiKL
BalkanS
1999 Effects of Plasmodium vivax malaria in pregnancy. Lancet 354 546 549
10. PoespoprodjoJR
FobiaW
KenangalemE
LampahDA
WarikarN
2008 Adverse pregnancy outcomes in an area where multidrug-resistant plasmodium vivax and Plasmodium falciparum infections are endemic. Clin Infect Dis 46 1374 1381
11. BalkDL
DeichmannU
YetmanG
PozziF
HaySI
2006 Determining global population distribution: methods, applications and data. Adv Parasitol 62 119 156
12. HaySI
SnowRW
2006 The Malaria Atlas Project: developing global maps of malaria risk. PLoS Med 3 e473 doi:10.1371/journal.pmed.0030473
13. SnowRW
GuerraCA
NoorAM
MyintHY
HaySI
2005 The global distribution of clinical episodes of Plasmodium falciparum malaria. Nature 434 214 217
14. HaySI
SmithDL
SnowRW
2008 Measuring malaria endemicity from intense to interrupted transmission. Lancet Infect Dis 8 369 378
15. GuerraCA
GikandiPW
TatemAJ
NoorAM
SmithDL
2008 The limits and intensity of Plasmodium falciparum transmission: implications for malaria control and elimination worldwide. PLoS Med 5 e38 doi:10.1371/journal.pmed.0050038
16. GuerraCA
SnowRW
HaySI
2006 Mapping the global extent of malaria in 2005. Trends Parasitol 22 353 358
17. GuerraCA
SnowRW
HaySI
2006 Defining the global spatial limits of malaria transmission in 2005. Adv Parasitol 62 157 179
18. GuerraCA
2007 Mapping the contemporary global distribution limits of malaria using empirical data and expert opinion Oxford University of Oxford 258
19. TatemAJ
GuerraCA
KabariaCW
NoorAM
HaySI
2008 Human population, urban settlement patterns and their impact on Plasmodium falciparum malaria endemicity. Malar J 7 218
20. Center for International Earth Science Information Network (CIESIN)/Columbia University; International Food Policy Research Institute (IFPRI)/the World Bank/and Centro Internacional de Agricultura Tropical (CIAT) 2007 Global Rural Urban Mapping Project (GRUMP) alpha: Gridded Population of the World; version 2 with urban reallocation (GPW-UR) Palisades (New York) CIESIN; Columbia University Available: http://sedac.ciesin.columbia.edu/gpw. Accessed 5 January 2010
21. United Nations Population Division; Department of Economic and Social Affairs 2007 World population prospects; the 2006 revision; ST/ESA/SER.A/261/ES New York United Nations
22. HaySI
NoorAM
NelsonA
TatemAJ
2005 The accuracy of human population maps for public health application. Trop Med Int Health 10 1073 1086
23. UNPD 2006 World population prospects: population database. Available: http://esa.un.org/unpp/. Accessed 5 January 2010
24. SedghG
HenshawS
SinghS
AhmanE
ShahIH
2007 Induced abortion: estimated rates and trends worldwide. Lancet 370 1338 1345
25. StantonC
LawnJE
RahmanH
Wilczynska-KetendeK
HillK
2006 Stillbirth rates: delivering estimates in 190 countries. Lancet 367 1487 1494
26. LeridonH
1977 Human fertility: the basic components (Table 4.20) Chicago University of Chicago Press
27. HammersloughCR
1992 Estimating the probability of spontaneous abortion in the presence of induced abortion and vice versa. Public Health Rep 107 269 277
28. HenshawSK
BinkinNJ
BlaineE
SmithJC
1985 A portrait of American women who obtain abortions. Fam Plann Perspect 17 90 96
29. World Health Organization 2009 WHO regional offices Geneva World Health Organisation Available: http://www.who.int/about/regions/en/ Accessed 5 January 2010
30. DesaiM
ter KuileFO
NostenF
McGreadyR
AsamoaK
2007 Epidemiology and burden of malaria in pregnancy. Lancet Infect Dis 7 93 104
31. HaySI
GuerraCA
GethingPW
PatilAP
TatemAJ
2009 A world malaria map: Plasmodium falciparum endemicity in 2007. PLoS Med 6 e1000048 doi:10.1371/journal.pmed.1000048
32. MutabingwaTK
BollaMC
LiJL
DomingoGJ
LiX
2005 Maternal malaria and gravidity interact to modify infant susceptibility to malaria. PLoS Med 2 e407 doi:10.1371/journal.pmed.0020407
33. Le HesranJY
CotM
PersonneP
FievetN
DuboisB
1997 Maternal placental infection with Plasmodium falciparum and malaria morbidity during the first 2 years of life. Am J Epidemiol 146 826 831
34. SchwarzNG
AdegnikaAA
BreitlingLP
GaborJ
AgnandjiST
2008 Placental malaria increases malaria risk in the first 30 months of life. Clin Infect Dis 47 1017 1025
Štítky
Interní lékařstvíČlánek vyšel v časopise
PLOS Medicine
2010 Číslo 1
- Ivabradin zlepšuje kvalitu života starších pacientů se srdečním selháním
- Fixní kombinace kandesartan/amlodipin v terapii arteriální hypertenze
- Inovace v hojení ran: krytí Zetuvit Plus Silicone Border pro optimální management exsudátu z ran
- Rána vizitkou (nejen) chirurga
- Patogeneze vzniku keloidní jizvy
Nejčtenější v tomto čísle
- The Evolution of the Epidemic of Charcoal-Burning Suicide in Taiwan: A Spatial and Temporal Analysis
- Male Circumcision at Different Ages in Rwanda: A Cost-Effectiveness Study
- Geographic Distribution of Causing Invasive Infections in Europe: A Molecular-Epidemiological Analysis
- “Working the System”—British American Tobacco's Influence on the European Union Treaty and Its Implications for Policy: An Analysis of Internal Tobacco Industry Documents
Zvyšte si kvalifikaci online z pohodlí domova
Mazová zátka a její řešení
nový kurzVšechny kurzy