
Effects of Community-Wide Vaccination with PCV-7 on Pneumococcal Nasopharyngeal Carriage in The Gambia: A Cluster-Randomized Trial
Background:
Introduction of pneumococcal conjugate vaccines (PCVs) of limited valency is justified in Africa by the high burden of pneumococcal disease. Long-term beneficial effects of PCVs may be countered by serotype replacement. We aimed to determine the impact of PCV-7 vaccination on pneumococcal carriage in rural Gambia.
Methods and Findings:
A cluster-randomized (by village) trial of the impact of PCV-7 on pneumococcal nasopharyngeal carriage was conducted in 21 Gambian villages between December 2003 to June 2008 (5,441 inhabitants in 2006). Analysis was complemented with data obtained before vaccination. Because efficacy of PCV-9 in young Gambian children had been shown, it was considered unethical not to give PCV-7 to young children in all of the study villages. PCV-7 was given to children below 30 mo of age and to those born during the trial in all study villages. Villages were randomized (older children and adults) to receive one dose of PCV-7 (11 vaccinated villages) or meningococcal serogroup C conjugate vaccine (10 control villages). Cross-sectional surveys (CSSs) to collect nasopharyngeal swabs were conducted before vaccination (2,094 samples in the baseline CSS), and 4–6, 12, and 22 mo after vaccination (1,168, 1,210, and 446 samples in CSS-1, -2, and -3, respectively).
A time trend analysis showed a marked fall in the prevalence of vaccine-type pneumococcal carriage in all age groups following vaccination (from 23.7% and 26.8% in the baseline CSS to 7.1% and 8.5% in CSS-1, in vaccinated and control villages, respectively). The prevalence of vaccine-type pneumococcal carriage was lower in vaccinated than in control villages among older children (5 y to <15 y of age) and adults (≥15 y of age) at CSS-2 (odds ratio [OR] = 0.15 [95% CI 0.04–0.57] and OR = 0.32 [95% CI 0.10–0.98], respectively) and at CSS-3 (OR = 0.37 [95% CI 0.15–0.90] for older children, and 0% versus 7.6% for adults in vaccinated and control villages, respectively). Differences in the prevalence of non-vaccine-type pneumococcal carriage between vaccinated and control villages were small.
Conclusions:
Vaccination of Gambian children reduced vaccine-type pneumococcal carriage across all age groups, indicating a “herd effect” in non-vaccinated older children and adults. No significant serotype replacement was detected.
: Please see later in the article for the Editors' Summary
Published in the journal:
. PLoS Med 8(10): e32767. doi:10.1371/journal.pmed.1001107
Category:
Research Article
doi:
https://doi.org/10.1371/journal.pmed.1001107
Summary
Background:
Introduction of pneumococcal conjugate vaccines (PCVs) of limited valency is justified in Africa by the high burden of pneumococcal disease. Long-term beneficial effects of PCVs may be countered by serotype replacement. We aimed to determine the impact of PCV-7 vaccination on pneumococcal carriage in rural Gambia.
Methods and Findings:
A cluster-randomized (by village) trial of the impact of PCV-7 on pneumococcal nasopharyngeal carriage was conducted in 21 Gambian villages between December 2003 to June 2008 (5,441 inhabitants in 2006). Analysis was complemented with data obtained before vaccination. Because efficacy of PCV-9 in young Gambian children had been shown, it was considered unethical not to give PCV-7 to young children in all of the study villages. PCV-7 was given to children below 30 mo of age and to those born during the trial in all study villages. Villages were randomized (older children and adults) to receive one dose of PCV-7 (11 vaccinated villages) or meningococcal serogroup C conjugate vaccine (10 control villages). Cross-sectional surveys (CSSs) to collect nasopharyngeal swabs were conducted before vaccination (2,094 samples in the baseline CSS), and 4–6, 12, and 22 mo after vaccination (1,168, 1,210, and 446 samples in CSS-1, -2, and -3, respectively).
A time trend analysis showed a marked fall in the prevalence of vaccine-type pneumococcal carriage in all age groups following vaccination (from 23.7% and 26.8% in the baseline CSS to 7.1% and 8.5% in CSS-1, in vaccinated and control villages, respectively). The prevalence of vaccine-type pneumococcal carriage was lower in vaccinated than in control villages among older children (5 y to <15 y of age) and adults (≥15 y of age) at CSS-2 (odds ratio [OR] = 0.15 [95% CI 0.04–0.57] and OR = 0.32 [95% CI 0.10–0.98], respectively) and at CSS-3 (OR = 0.37 [95% CI 0.15–0.90] for older children, and 0% versus 7.6% for adults in vaccinated and control villages, respectively). Differences in the prevalence of non-vaccine-type pneumococcal carriage between vaccinated and control villages were small.
Conclusions:
Vaccination of Gambian children reduced vaccine-type pneumococcal carriage across all age groups, indicating a “herd effect” in non-vaccinated older children and adults. No significant serotype replacement was detected.
: Please see later in the article for the Editors' Summary
Introduction
The prevention of pneumococcal disease is a major international public health priority, especially in children in developing countries [1]. On the basis of a trial conducted in California in the United States [2], the first licensed pneumococcal conjugate vaccine (PCV), PCV-7, was introduced in the US in 2000. This vaccine has been highly successful in reducing the incidence of invasive pneumococcal disease (IPD) in both vaccinated children and in the non-vaccinated older population [3],[4]. This herd effect has been attributed to reduced nasopharyngeal carriage of pneumococci of vaccine type (VT) in vaccinated infants, resulting in decreased transmission to contacts [3]–[6]. In the US, small increases in the incidence of both IPD and carriage caused by pneumococci of non-vaccine types (NVTs) have been detected, a phenomenon termed serotype replacement [4],[7]–[12]. In European countries, the prevalence of serotypes included in PCV-7 is generally lower than in the US, and the impact of PCV-7 has been more heterogeneous, with less overall public health benefit as a result of more marked serotype replacement [10]–[14].
Introduction of PCVs into the routine immunization programs of sub-Saharan African countries is justified by the high pneumococcal disease burden [1],[15]–[19] and the evidence of efficacy of PCVs provided by clinical trials [20],[21]. However, the ecology and epidemiology of pneumococcal carriage and IPD in this region is different from that seen in the US or Europe. First, rates of pneumococcal carriage in sub-Saharan Africa are among the highest described [22]–[25] and result in high rates of transmission [26]. Second, there is a wide variety of serotypes associated with both carriage and invasive disease, and prevalence of individual serotypes differs from those seen in developed countries [15],[22]–[28]. Third, vaccination in African countries is usually a three-dose regimen given during infancy, without a booster, as opposed to the booster-containing schedules widely used in industrialized countries.
The factors that drive serotype replacement, which vary in degree from community to community [29], are not fully understood. It is likely that vaccination facilitates serotype replacement by inducing a humoral and/or cellular immune response that makes it more difficult for VT pneumococci to colonize the nasopharynx, opening the way for colonization by NVT pneumococci and, perhaps, by other bacteria. In countries where PCV has been introduced into routine immunization programs, immune pressure against VT pneumococci will increase gradually as more vaccinated individuals enter the population. Determining the consequence of this will require long-term longitudinal studies. As an alternative, we have undertaken a village-randomized trial in which the pneumococcal population of some villages has been exposed to maximum immune pressure by immunizing the whole population with PCV-7.
Methods
Study Population
Villages in the Sibanor area, Western Region, The Gambia, were selected for the study as they are representative of rural areas in The Gambia and are distant from the area where a PCV-9 vaccine trial had been undertaken a few years earlier [20]. Twenty-one of the 55 villages in the Sibanor area were selected based on the criteria that they had a population ranging from 80 to 660 inhabitants and were separated from each other by a distance of at least 3 km. The overall population of the selected villages was 5,441 in June 2006. During the last trimester of 2006, 1,532 refugees from southern Senegal lived temporarily in these villages. The prevalence of HIV infection among pregnant women attending Sibanor Hospital, adjacent to the study area, between 2000 and 2001 was 3% [30] and is stable. The climate of The Gambia is tropical with one short rainy season from June to October. Other characteristics of the study population are described elsewhere [23].
Study Preparation
Before the trial started, village meetings were held to discuss the nature and objectives of the study with village elders and other members of the study villages [23]. When village consent had been obtained, the village was mapped and a full census taken and updated annually. All residents of the 21 selected villages were eligible for inclusion in the study, including those born during the study period. Study participants gave individual informed consent; parental consent was obtained for children up to 16 y of age.
The study was approved by the joint Medical Research Council (MRC)/Gambia Government Ethics Committee and by the ethics committee of the London School of Hygiene and Tropical Medicine. The conduct of the trial was guided by a Data Safety and Monitoring Board.
Trial Design
The protocol of the trial and CONSORT checklist are available in Text S1 and Text S2, respectively.
A cluster-randomized (by village) controlled trial of PCV-7 was conducted. PCV-7 was the study vaccine, and a meningococcal serogroup C conjugate was the control vaccine. Blinding included vaccine recipients and laboratory personnel. Study nurses were aware of the nature of the vaccines given but played no other part in the conduct of the trial.
Time trends within the vaccinated and control villages were investigated using a before and after approach, measuring pneumococcal carriage in PCV-7 vaccinated and control villages before and after vaccination.
Pre-vaccination cross-sectional survey
Between 8 December 2003 and 19 May 2004, 2 y before vaccination started, a baseline cross-sectional survey (CSS) was undertaken in 21 villages in the Sibanor area. A nasopharyngeal swab (NPS) was collected from a random selection of the village's population and cultured for pneumococci. Details of how this baseline study was conducted and its findings have been reported previously [23]. The overall prevalence of pneumococcal carriage among children and adults was approximately 70%. A random selection of the NPSs collected in this baseline CSS has been used to provide a population with a similar age distribution to the populations investigated in the post-vaccination CSSs described below. Sampling and culturing methods for the baseline and post-vaccination CSSs did not differ.
Randomization
The number of residents in the study villages varied substantially. Therefore, village randomization was performed at the MRC laboratories at Fajara using several steps. First, a random integer was chosen to select 11 or 10 intervention villages versus 10 or 11 control villages. Population sizes in January 2006 for the 21 villages were stored in a Stata program file (do file) for the village allocation scheme. One thousand allocation-size-balanced schemes (difference between the two groups of less than 10%) were created, and one was randomly chosen.
Vaccination
Because the non-licensed PCV-9 vaccine (including serotypes 1 and 5 in addition to the PCV-7 serotypes) had already been shown to be effective in young children in a randomized controlled trial conducted in The Gambia, it was considered unethical not to give PCV-7 to young children in all of the study villages. Therefore, all children in the trial aged between 2 and 30 mo at the start of the study, the age group covered by the PCV-9 trial [20], received PCV-7, as did any child born during the period of the study. Infants aged between 2 and 11 mo received three doses of the vaccine given at monthly intervals, and children aged between 12 and 30 mo received two doses with a 1-mo gap between injections. Infants born during the study received three doses of the vaccine given monthly at the ages of approximately 2, 3, and 4 mo.
Village randomization was applied to individuals who were above the age of 30 mo when vaccination started. On the basis of their randomization group, individuals above the age of 30 mo received either one dose of PCV-7 (Prevenar, Pfizer) (11 vaccinated villages) or one dose of a meningococcal serogroup C conjugate vaccine (Meningitec, Pfizer) (10 control villages). The meningococcal vaccine was given to ensure blinding and is not expected to have had any effect on pneumococcal carriage.
PCV-7 vaccination started in 17 July 2006, and by 2 mo the first round of vaccination had been completed (first dose given to 50%–75% of eligible individuals in vaccinated and control villages). Meningococcal vaccine was unavailable for several weeks, and hence meningococcal vaccination was delayed beyond the intended date of administration. Individuals who moved into the study villages during the study period were vaccinated and managed following the standardized procedures of the trial, including 1,532 Senegalese refugees who moved into 13 of the study villages (869 in control and 633 in vaccinated villages) during the last trimester of 2006. Following a census update, these individuals were vaccinated and managed following the study protocol. No serious adverse events that could be attributed to PCV-7 were observed in children or adults.
Post-vaccination surveys
Approximately 4–6, 12, and 22 mo after vaccination, a NPS sample was collected from 1,200 randomly selected individuals during CSSs (post-vaccination CSS-1 [15 November 2006–13 March 2007], CSS-2 [17 July–12 September 2007], and CSS-3 [8 July–1 September 2008], respectively). It was originally planned that CSS-3 would be conducted 24 mo after vaccination. However, a mass campaign by the Gambian National Trachoma Elimination Programme involving administration of one dose of azithromycin to all individuals older than 6 mo of age except pregnant women started at the time of the last study CSS in most study villages, meaning that the results of this survey could not ultimately be used. Instead, samples from a concurrent longitudinal survey in the same villages taken 0 to 3 mo before the intended start of the final CSS (12 April–25 June 2008) were used to estimate the effects of vaccination 2 y after the start of the trial. A maximum of one sample per individual was included from this dataset, giving a total of 446 samples that we called CSS-3. All these 446 samples were collected before the azithromycin campaign started.
Sample Handling
NPSs were collected during all CSSs using a calcium alginate swab, from the posterior wall of the nasopharynx, and immediately inoculated into vials containing skim-milk-tryptone-glucose-glycerol transport medium, which were placed in a cold box before transfer to the MRC Fajara laboratories (a distance of 90 km) within 8 h of collection, in accordance with the World Health Organization protocol for evaluation of pneumococcal carriage [31]. Inoculated vials were stored at −70°C until they were tested in batches by subculture onto gentamicin blood agar for selective isolation of Streptococcus pneumoniae.
Laboratory Methods
10 µl of thawed, inoculated skim-milk-tryptone-glucose-glycerol medium was plated onto gentamicin blood agar and incubated for 18–24 h at 35°C in 5% CO2. Pneumococcal identification was based on colony morphology and conventional methods of characterization (optochin susceptibility and bile solubility assays) [23]. Serotyping was performed at MRC Fajara laboratories, with capsular and factor typing sera (Statens Serum Institut), using a modified latex agglutination assay [32]. Equivocal results were confirmed by the Quellung reaction. Laboratory methods were consistent for all CSSs.
Data Management and Statistical Analysis
Age groups were defined as follows: (i) young children: individuals 2 to 5 y of age; (ii) older children: individuals 5 to 15 y of age; and (iii) adults: individuals aged 15 y and above. Pneumococcal serotypes were grouped as follows: (i) VT: serotypes included in PCV-7 (4, 6B, 9V, 14, 18C, 19F, and 23F) plus 6A, which shows cross-protective immunity with serotype 6B; and (ii) NVT: any other pneumococcal serotype including non-typable pneumococcus. Individuals can carry more than one serotype, and all serotypes were included in the analysis. The primary outcomes of the study for each of the age groups were (i) the prevalence of carriage of VT pneumococci and (ii) the prevalence of carriage of NVT pneumococci.
The sample size was calculated so as to be able to detect a 50% reduction in the prevalence of carriage of VT for each of the three study age groups among individuals resident in PCV-7 vaccinated villages compared to individuals from control villages, with 90% power at a 5% significance level (from 30% to 15%). These calculations resulted in an overall sample size of 1,200 individuals per CSS. The study power for comparing study arms in CSS-3 was compromised by the unanticipated trachoma elimination campaign. In an ad hoc analysis, we also included comparison of individual serotypes between vaccinated and control villages for each CSS covering all study age groups. Because all children under the age of 30 mo at enrollment or born during the study received PCV-7 (in both vaccinated and control villages), the effect of vaccination on carriage could not be measured among young children by comparing vaccinated versus control villages. However, the study protocol allowed the evaluation of the indirect effect of vaccinating children on the rest of the population of the control villages. Analysis of carriage used “person” as the unit of analysis, whereas analysis of serotypes used “isolate” as the unit of analysis.
Comparisons of median ages, village populations, and other quantitative measures of household characteristics in vaccinated and control villages were made using Wilcoxon rank-sum tests. Comparisons of sex, ethnic group distribution, and other categorical variables were made using Chi-square tests. For each of the CSSs, comparisons were made of carriage of VT and NVT pneumococci in control versus vaccinated villages using mixed effects logistic regression with village included as a random effect to allow for the cluster randomized design. Mixed effects logistic regression was used to compare carriage in different CSSs within each study arm, treating CSS as a categorical variable and adjusting for age as a continuous variable. For individual serotypes, similar analyses were carried out using fixed effects logistic regression and a clustered sandwich variance estimator to allow for the clustered design. The analyses were carried out using Stata 11 (StataCorp). p-Values less than 0.05 were taken to indicate statistical significance.
Results
Trial Profile
Twenty-one villages were randomized to one or the other of the two study groups (Figure 1). Characteristics of the two groups of villages (vaccinated and control) are shown in Table 1. Demographic and epidemiological characteristics of the villages were similar, except for the distribution of ethnic groups (p<0.001); the Mandinka ethnic group was overrepresented in the vaccinated villages. Characteristics of the individuals included in each of the study CSSs are shown in Table S1. The percentages of the population that had been vaccinated by the time of each post-vaccination CSS are shown in Figure 1 and Table S2. Vaccine coverage with PCV-7 in the vaccinated villages ranged from 85% to 92%. In the control communities, PCV-7 coverage in the post-vaccination surveys increased from 33% (CSS-1) to 62% (CSS-3) in young children, who represented 5% and 9% of the overall population in this study arm, respectively. Additional information regarding time since PCV-7 vaccination in the study villages during each of the post-vaccination CSSs is shown in Table S3. Although PCV-7 vaccination was conducted simultaneously in vaccinated and control villages, NPS collection in CSS-1 was performed slightly later in control than in vaccinated villages. In CSS-1, half of the individuals were sampled within 177 d (approximately 6 mo) after PCV-7 vaccination started in control villages and within 125 d (approximately 4 mo) after PCV-7 vaccination started in vaccinated villages. Coverage with meningococcal vaccine in older children and adults in control villages in CSS-1 was low (Figure 1 and Table S2) and improved over the CSSs, but this delay should not have any effect on the study objectives.
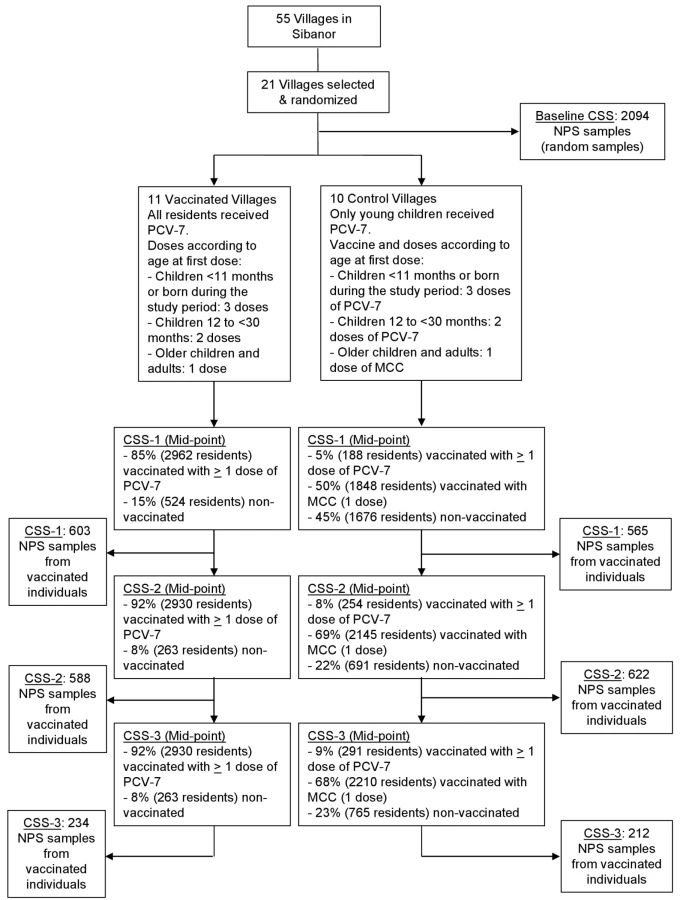

Overall, 2,094 NPS samples were included in the pre-vaccination CSS and 1,168, 1,210, and 446 NPS samples in post-vaccination CSS-1, CSS-2, and CSS-3, respectively. Table 2 provides a summary of the number of samples collected per study CSS and the median age and sex of sampled individuals in each CSS. For CSS-3, children in the “young children” group were older than in the previous CSS (median 4 versus 3 y, respectively, p<0.001), and adults from the control communities were younger than those in the vaccinated communities (median 26 versus 39 y, respectively, p<0.001).

Prevalence of Pneumococcal Carriage
Pre-vaccination survey
The overall prevalence of pneumococcal carriage in the pre-vaccination CSS was high (71.1%) and decreased with age. The proportion of VT among pneumococcal carriers also decreased with age. The prevalence of pneumococcal carriage by age group and by future vaccine arm are shown in Table 3. The overall prevalence was similar in both study arms, but a slightly lower prevalence of VT carriage was observed among villages where universal vaccination was later introduced (not statistically significant for any of the comparisons).

Comparisons of vaccinated and control villages in each of the post-vaccination surveys
The overall prevalence of pneumococcal carriage was similar in all post-vaccination CSSs between vaccinated and control villages (Table 3; Figure 2).

The prevalence of carriage of VT pneumococci was lower in vaccinated than in control villages in all post-vaccination CSSs for all age groups, reaching statistical significance in CSS-2 and CSS-3 (except for younger children) (Table 3; Figure 2).
The prevalence of carriage of NVT pneumococci was similar in vaccinated and in control villages in all post-vaccination surveys, except for a higher prevalence of NVT pneumococci among adults in vaccinated communities during CSS-1 (odds ratio [OR] = 1.50 [95% CI 1.03–2.18], p = 0.035) (Table 3; Figure 2).
Time Trends within Trial Arms
The overall prevalence of pneumococcal carriage fell markedly after vaccination and reached minimum levels in post-vaccination CSS-2 in both study arms (Table 4; Figure 2) and in all age groups, except adults in control villages, whose prevalence was lower in CSS-1.

The decrease in the prevalence of VT carriage seen in both vaccinated and control villages was statistically significant for all age groups and any post-vaccination CSS when compared to the pre-vaccination survey, with one exception in the control group (see Table 4; Figure 2).
For NVT pneumococci, changes in the pattern of carriage differed according to study age group (Table 4; Figure 2). Among the youngest children, there was an increase in prevalence of NVT pneumococci between baseline and CSS-1 that returned to baseline levels in CSS-2 and CSS-3. Among older children, there was a decrease in carriage of NVT pneumococci in CSS-2 in both study arms, but carriage increased in CSS-3 to its former level. Among adults, there was a significant decrease in carriage of NVT between baseline and post-vaccination CSS-1 in both study arms, and the final prevalence in CSS-3 was still lower than baseline (OR = 0.46 [95% CI 0.26–0.82], p = 0.008, and OR = 0.53 [95% CI 0.31–0.92], p = 0.024, for control and vaccinated villages, respectively).
In the time trend analysis, the overall decrease between the pre-vaccination CSS and CSS-1 was bigger for VT than for NVT in both vaccinated (OR = 0.24 [95% CI 0.17–0.33] for VT and OR = 0.58 [95% CI 0.47–0.72] for NVT) and control villages (OR = 0.23 [95% CI 0.16–0.33] for VT and OR = 0.72 [95% CI 0.59–0.89] for NVT) (Table 4).
Individual Serotypes
The most prevalent serotypes in the pre-vaccination CSS among VT pneumococci were serotypes 23F (n = 86), 6A (n = 84), and 6B (n = 80), and among NVT pneumococci, serotypes 3 (n = 182), 11 (n = 81), and 7C (n = 52). During the post-vaccination CSSs, serotype 3 remained the most prevalent among NVT isolates, followed by serotype 11, except for CSS-3, when serotypes 11 and 19A were the most common. The most prevalent VT serotypes in the post-vaccination surveys were serotypes 19F and 6A. Table 5 shows the prevalence of VT serotypes and the most prevalent NVT serotypes for each CSS in vaccinated and control villages. The prevalence of carriage of serotype 5 pneumococci increased in vaccinated villages from 0% to 4.7%. Seven of the 11 serotype 5 isolates detected in CSS-3, were obtained from older children (64%), and seven came from the same village.

Details of the time trends for individual serotypes within vaccinated and control villages are shown in Table S4. Most of the VT serotypes significantly decreased compared to the baseline CSS in vaccinated and control villages. Decrease of serotype 6A was less prominent in control villages. Of the most prevalent NVT serotypes, serotype 3 and 7C decreased in vaccinated communities, and serotypes 5, 19A, and 23B significantly increased in vaccinated communities in CSS-3.
Discussion
To anticipate the potential long-term effects of the introduction of pneumococcal conjugate vaccination in sub-Saharan Africa, we have conducted a novel randomized, controlled trial in which a population of pneumococci was exposed to maximum immune pressure by vaccinating all residents of 11 Gambian villages with PCV-7. We measured the prevalence of pneumococcal carriage in these villages before and on three occasions after vaccination, and compared these findings with those obtained in control villages where only young children had been vaccinated with PCV-7. Time trends were investigated by comparing pneumococcal carriage within both groups of villages before and after vaccination.
By the time this study was ready to start, the results of the Gambian PCV-9 trial had become available [20], showing a high level of protection against IPD in children under the age of 30 mo, so it was considered unethical to proceed with a trial in which all children in this age group did not receive PCV, as had been originally intended. This design modification weakened the ability of the study to show the direct effect of vaccination on the community through differences between vaccinated and control villages, but serendipitously allowed demonstration of a potential herd effect resulting from immunization of children in control communities. Changes in the prevalence of carriage between the before and after vaccination surveys need to be interpreted with caution because of the potential influence of temporal trends unrelated to vaccination. However, methods used for sampling and isolation of pneumococci were consistent over the study period, including pre - and post-vaccination surveys. Furthermore, the investigators are not aware of any changes in the study villages that could have affected risk factors for carriage during the conduct of the study, apart from the administration of azithromycin at the time of the last CSS, an event which has been addressed in the analysis.
A time trend analysis showed a marked drop in the prevalence of carriage of VT pneumococci among all age groups in vaccinated and control villages following vaccination. The decline in the prevalence of VT carriage in older children and adults in the control villages strongly suggests a herd effect resulting from vaccination of infants and toddlers in those villages. This effect was apparent as early as 6 mo after vaccination and persisted for at least the next 2 y. This finding is in line with results from a pre-vaccination observational study conducted in the same villages that suggested that transmission occurred mainly from young children to older members of the family [26]. Although the study villages were separated by at least 3 km, some mingling between communities may have contributed to the herd effect observed in the control villages, as some older children resident in these villages attended school in neighboring villages. Because of the high level of transmission of pneumococcal infection in Africa [26], there have been concerns that induction of herd immunity through vaccination of infants might be more difficult to achieve in this continent than elsewhere. We have shown here, to our knowledge for the first time in Africa, a herd effect on carriage of VT pneumococci, which might be translated into herd protection against IPD in adults, following routine immunization of infants and young children, as has been observed in the US [4]. Our findings are relevant for other countries in Africa contemplating the introduction of PCVs where the pattern of pneumococcal infection is similar to that in The Gambia. Whether a similar effect will be observed in countries with a high prevalence of HIV (HIV-infected adults are more susceptible to being carriers of pediatric pneumococcal serotypes) remains unknown.
The prevalence of carriage of VT pneumococci was slightly lower, but statistically significantly so, in individuals from vaccinated than from control villages in most post-vaccination comparisons. Thus, vaccination of older children and adults with PCV-7 had some additional effect in decreasing rates of carriage of VT pneumococci, but this effect was not marked.
The prevalence of carriage of NVT pneumococci among adults was lower in the post-vaccination surveys than in the pre-vaccination survey in both control and vaccinated communities. This decrease was not observed in other age groups in either vaccinated or control villages, so this may have been a chance finding. There was a significant gap between the time that the pre-vaccination study was done and the first post-vaccination survey, and it is possible that there may have been some change in the pattern of carriage in the study villages during this time. However, surveys undertaken in The Gambia over a period of many years, including several conducted in the study area, have consistently shown very high levels of carriage, and it is unlikely that the overall level of carriage would have changed during this period, although there could have been some changes in serotype distribution [7],[23],[24],[26],[28],[33]. “Up and down” trends in the prevalence of different serotypes have been documented previously in the area over time [26]. Another possible explanation includes a nonspecific effect on health produced by the intervention, but such an effect should have been observed in all age groups. Still, the observed decrease of NVT pneumococci prevalence from the pre-vaccination CSS to post-vaccination CSS-1 was significantly lower than the decrease of VT pneumococci prevalence observed for these two CSSs in both vaccinated and control communities.
The absence of a significant increase in the prevalence of carriage of NVT pneumococci in any age group, and the limited differences between control and vaccinated villages, are surprising, as many previous studies [8],[9],[12], including some conducted in The Gambia [7],[34], have shown a marked increase in the prevalence of carriage of NVT pneumococci after vaccination. These previous carriage studies conducted in The Gambia focused on infants and younger children [7],[34], an age group not sampled in our study. Lack of an increase in NVT pneumococci prevalence has previously been documented in a carriage study of household contacts among Native Americans whose children participated in a PCV-7 vaccine trial [35]. The investigators observed no increase in carriage of NVT pneumococci among older children and adults within households of children vaccinated with PCV-7, although a reduction in carriage of VT pneumococci was found in the adult age group. An increase in carriage of NVT pneumococci was found only in non-vaccinated household members <5 y of age from households with PCV-7 vaccinees. Encouragingly, vaccination of older children and adults in our study did not add selection pressure towards an overall increase in carriage of NVT pneumococci.
We have also observed in our study a decrease of the overall pneumococcal carriage in the post-vaccination CSSs compared to the pre-vaccination CSS. Because there is little serotype replacement, PCV introduction might also have had an effect on the overall prevalence of pneumococcal carriage at least up to 2 y after vaccination. Pneumococcal prevalence reached its lowest levels in the post-vaccination CSS-2. As mentioned above, secular trends or the health effect of the intervention could partly explain such results.
An increase in carriage of serotype 5 pneumococci seen in vaccinated villages in CSS-3 was due largely to an outbreak in one village and may have been a chance finding unrelated to vaccination, an event similar to one observed in the study community before any intervention was performed [26]. However, the possibility of an association with PCV vaccination is of concern as this serotype, along with serotype 1, is a major cause of IPD in The Gambia [36] and elsewhere in Africa [15],[22],[27]. Both serotype 5 and serotype 1 pneumococci also have the potential to cause epidemics [37]–[39]. An increase in the prevalence of carriage of NVT serotypes such as 19A and 23B was observed during CSS-3 in the vaccinated villages (shown in both the arm comparison and the time trend analysis), probably driven by young children. An increase in carriage of serotype 19A after PCV vaccination has been documented previously in The Gambia [7] and elsewhere [8],[9],[11],[12]. An increase has also been widely documented for IPD caused by this serotype [4],[10],[11], demonstrating lack of cross-protection of PCV-7 for serotype 19A. Serotype 6A was still present in all post-vaccination surveys but with lower prevalence in each of the post-vaccination CSSs compared to the pre-vaccination survey in both vaccinated and control communities, suggesting the expected vaccine protective effect in carriage, and potentially on IPD, a finding that justifies inclusion of this serotype in the VT group. However, the 6A decrease was statistically significant only among vaccinated communities. Serotype 3 was the most prevalent NVT serotype detected both before and after vaccination in this study, and serotype 19A was shown to be the most common at some point after vaccination. Both of these serotypes and serotype 6A are contained in the PCV-13, which has been shown to be immunogenic in infants, with potential protective effect against serotype-specific IPD [40]–[42]. PCV-13 has recently replaced PCV-7 in routine childhood immunization programs in The Gambia and would be expected to provide coverage of these serotypes.
This study faced an additional challenge. The last post-vaccination survey was disrupted by the administration of azithromycin to individuals in several study villages as part of a national trachoma elimination program that had not been envisaged when the carriage study was planned. To avoid any direct or indirect effect resulting from this treatment, CSS-3 analyses include only a third of the target number of samples, all collected before treatment started in the area, and therefore, this survey lacked statistical power for comparison of vaccinated versus control villages.
Despite the challenges and limitations of this study, the main findings are robust and very encouraging. Vaccination of young Gambian children reduced carriage of VT pneumococci in vaccinated children but also in vaccinated and non-vaccinated older children and adults, revealing to our knowledge for the first time in Africa a potential herd effect from vaccination of young children. The immunological pressure induced by vaccinating whole communities did not lead to a community-wide increase in carriage of NVT pneumococci during a 2-y period after vaccination. Further long-term follow-up carriage studies in this community are planned.
Supporting Information
Zdroje
1. O'BrienKLWolfsonLJWattJPHenkleEDeloria-KnollM 2009 Burden of disease caused by Streptococcus pneumoniae in children younger than 5 years: global estimates. Lancet 374 893 902 doi:10.1016/S0140-6736(09)61204-6
2. BlackSBShinefieldHRLingSHansenJFiremanB 2002 Effectiveness of heptavalent pneumococcal conjugate vaccine in children younger than five years of age for prevention of pneumonia. Pediatr Infect Dis J 21 810 815 doi:10.1097/01.inf.0000027926.99356.4c
3. LexauCALynfieldRDanilaRPilishviliTFacklamR 2005 Changing epidemiology of invasive pneumococcal disease among older adults in the era of pediatric pneumococcal conjugate vaccine. JAMA 294 2043 2051 doi:10.1001/jama.294.16.2043
4. WhitneyCGFarleyMMHadlerJHarrisonLHBennettNM 2003 Decline in invasive pneumococcal disease after the introduction of protein-polysaccharide conjugate vaccine. N Engl J Med 348 1737 1746 doi:10.1056/NEJMoa022823
5. PilishviliTLexauCFarleyMMHadlerJHarrisonLH 2010 Sustained reductions in invasive pneumococcal disease in the era of conjugate vaccine. J Infect Dis 201 32 41 doi:10.1086/648593
6. WhitneyCGPilishviliTFarleyMMSchaffnerWCraigAS 2006 Effectiveness of seven-valent pneumococcal conjugate vaccine against invasive pneumococcal disease: a matched case-control study. Lancet 368 1495 1502 doi:10.1016/S0140-6736(06)69637-2
7. CheungYBZamanSMNsekpongEDVan BenedenCAAdegbolaRA 2009 Nasopharyngeal carriage of Streptococcus pneumoniae in Gambian children who participated in a 9-valent pneumococcal conjugate vaccine trial and in their younger siblings. Pediatr Infect Dis J 28 990 995 doi:10.1097/INF.0b013e3181a78185
8. DaganRGivon-LaviNZamirOSikuler-CohenMGuyL 2002 Reduction of nasopharyngeal carriage of Streptococcus pneumoniae after administration of a 9-valent pneumococcal conjugate vaccine to toddlers attending day care centers. J Infect Dis 185 927 936 doi:10.1086/339525
9. HanageWPFinkelsteinJAHuangSSPeltonSIStevensonAE 2010 Evidence that pneumococcal serotype replacement in Massachusetts following conjugate vaccination is now complete. Epidemics 2 80 84 doi:10.1016/j.epidem.2010.03.005
10. HanquetGKisslingEFenollAGeorgeRLepoutreA 2010 Pneumococcal serotypes in children in 4 European countries. Emerg Infect Dis 16 1428 1439
11. HsiehYCLinPYChiuCHHuangYCChangKY 2009 National survey of invasive pneumococcal diseases in Taiwan under partial PCV7 vaccination in 2007: emergence of serotype 19A with high invasive potential. Vaccine 27 5513 5518 doi:10.1016/j.vaccine.2009.06.091
12. van GilsEJVeenhovenRHHakERodenburgGDKeijzersWC 2010 Pneumococcal conjugate vaccination and nasopharyngeal acquisition of pneumococcal serotype 19A strains. JAMA 304 1099 1106 doi:10.1001/jama.2010.1290
13. FlascheSVan HoekAJSheasbyEWaightPAndrewsN 2011 Effect of pneumococcal conjugate vaccination on serotype-specific carriage and invasive disease in England: a cross-sectional study. PLoS Med 8 e1001017 doi:10.1371/journal.pmed.1001017
14. RodenburgGDde GreeffSCJansenAGde MelkerHESchoulsLM 2010 Effects of pneumococcal conjugate vaccine 2 years after its introduction, the Netherlands. Emerg Infect Dis 16 816 823
15. BerkleyJALoweBSMwangiIWilliamsTBauniE 2005 Bacteremia among children admitted to a rural hospital in Kenya. N Engl J Med 352 39 47 doi:10.1056/NEJMoa040275
16. RocaASigauqueBQuintoLMandomandoIVallesX 2006 Invasive pneumococcal disease in children<5 years of age in rural Mozambique. Trop Med Int Health 11 1422 1431 doi:10.1111/j.1365-3156.2006.01697.x
17. RocaASigauqueBQuintoLMoraisLBerengueraA 2010 Estimating the vaccine-preventable burden of hospitalized pneumonia among young Mozambican children. Vaccine 28 4851 4857 doi:10.1016/j.vaccine.2010.03.060
18. ScottJA 2007 The preventable burden of pneumococcal disease in the developing world. Vaccine 25 2398 2405 doi:10.1016/j.vaccine.2006.09.008
19. UsenSAdegbolaRMulhollandKJaffarSHiltonS 1998 Epidemiology of invasive pneumococcal disease in the Western Region, The Gambia. Pediatr Infect Dis J 17 23 28
20. CuttsFTZamanSMEnwereGJaffarSLevineOS 2005 Efficacy of nine-valent pneumococcal conjugate vaccine against pneumonia and invasive pneumococcal disease in The Gambia: randomised, double-blind, placebo-controlled trial. Lancet 365 1139 1146 doi:10.1016/S0140-6736(05)71876-6
21. KlugmanKPMadhiSAHuebnerREKohbergerRMbelleN 2003 A trial of a 9-valent pneumococcal conjugate vaccine in children with and those without HIV infection. N Engl J Med 349 1341 1348 doi:10.1056/NEJMoa035060
22. VallesXFlanneryBRocaAMandomandoISigauqueB 2006 Serotype distribution and antibiotic susceptibility of invasive and nasopharyngeal isolates of Streptococcus pneumoniae among children in rural Mozambique. Trop Med Int Health 11 358 366 doi:10.1111/j.1365-3156.2006.01565.x
23. HillPCAkisanyaASankarehKCheungYBSaakaM 2006 Nasopharyngeal carriage of Streptococcus pneumoniae in Gambian villagers. Clin Infect Dis 43 673 679 doi:10.1086/506941
24. HillPCCheungYBAkisanyaASankarehKLahaiG 2008 Nasopharyngeal carriage of Streptococcus pneumoniae in Gambian infants: a longitudinal study. Clin Infect Dis 46 807 814 doi:10.1086/528688
25. AbdullahiONyiroJLewaPSlackMScottJA 2008 The descriptive epidemiology of Streptococcus pneumoniae and Haemophilus influenzae nasopharyngeal carriage in children and adults in Kilifi district, Kenya. Pediatr Infect Dis J 27 59 64 doi:10.1097/INF.0b013e31814da70c
26. HillPCTownendJAntonioMAkisanyaBEbrukeC 2010 Transmission of Streptococcus pneumoniae in rural Gambian villages: a longitudinal study. Clin Infect Dis 50 1468 1476 doi:10.1086/652443
27. CampbellJDKotloffKLSowSOTapiaMKeitaMM 2004 Invasive pneumococcal infections among hospitalized children in Bamako, Mali. Pediatr Infect Dis J 23 642 649
28. DarboeMKFulfordAJSeckaOPrenticeAM 2010 The dynamics of nasopharyngeal streptococcus pneumoniae carriage among rural Gambian mother-infant pairs. BMC Infect Dis 10 195 doi:10.1186/1471-2334-10-195
29. SingletonRJHennessyTWBulkowLRHammittLLZulzT 2007 Invasive pneumococcal disease caused by nonvaccine serotypes among Alaska native children with high levels of 7-valent pneumococcal conjugate vaccine coverage. JAMA 297 1784 1792 doi:10.1001/jama.297.16.1784
30. Schim van der LoeffMFSarge-NjieRCeesaySAwasanaAAJayeP 2003 Regional differences in HIV trends in The Gambia: results from sentinel surveillance among pregnant women. AIDS 17 1841 1846 doi:10.1097/01.aids.0000076303.76477.49
31. O'BrienKLNohynekH 2003 Report from a WHO Working Group: standard method for detecting upper respiratory carriage of Streptococcus pneumoniae. Pediatr Infect Dis J 22 e1 e11 doi:10.1097/01.inf.0000049347.42983.77
32. BrueggemannABGriffithsDTMeatsEPetoTCrookDW 2003 Clonal relationships between invasive and carriage Streptococcus pneumoniae and serotype - and clone-specific differences in invasive disease potential. J Infect Dis 187 1424 1432 doi:10.1086/374624
33. Lloyd-EvansNO'DempseyTJBaldehISeckaODembaE 1996 Nasopharyngeal carriage of pneumococci in Gambian children and in their families. Pediatr Infect Dis J 15 866 871
34. ObaroSKAdegbolaRABanyaWAGreenwoodBM 1996 Carriage of pneumococci after pneumococcal vaccination. Lancet 348 271 272
35. MillarEVWattJPBronsdonMADallasJReidR 2008 Indirect effect of 7-valent pneumococcal conjugate vaccine on pneumococcal colonization among unvaccinated household members. Clin Infect Dis 47 989 996 doi:10.1086/591966
36. AdegbolaRAHillPCSeckaOIkumapayiUNLahaiG 2006 Serotype and antimicrobial susceptibility patterns of isolates of Streptococcus pneumoniae causing invasive disease in The Gambia 1996–2003. Trop Med Int Health 11 1128 1135 doi:10.1111/j.1365-3156.2006.01652.x
37. GessnerBDMuellerJEYaroS 2010 African meningitis belt pneumococcal disease epidemiology indicates a need for an effective serotype 1 containing vaccine, including for older children and adults. BMC Infect Dis 10 22 doi:10.1186/1471-2334-10-22
38. HausdorffWP 2007 The roles of pneumococcal serotypes 1 and 5 in paediatric invasive disease. Vaccine 25 2406 2412 doi:10.1016/j.vaccine.2006.09.009
39. LeimkugelJAdamsFAGagneuxSPflugerVFlierlC 2005 An outbreak of serotype 1 Streptococcus pneumoniae meningitis in northern Ghana with features that are characteristic of Neisseria meningitidis meningitis epidemics. J Infect Dis 192 192 199 doi:10.1086/431151
40. DugganST 2010 Pneumococcal polysaccharide conjugate vaccine (13-valent, adsorbed) [prevenar 13(R)]. Drugs 70 1973 1986 doi:10.2165/11205110-000000000-00000
41. EspositoSTanseySThompsonARazmpourALiangJ 2010 Safety and immunogenicity of a 13-valent pneumococcal conjugate vaccine compared to those of a 7-valent pneumococcal conjugate vaccine given as a three-dose series with routine vaccines in healthy infants and toddlers. Clin Vaccine Immunol 17 1017 1026 doi:10.1128/CVI.00062-10
42. YehSHGurtmanAHurleyDCBlockSLSchwartzRH 2010 Immunogenicity and safety of 13-valent pneumococcal conjugate vaccine in infants and toddlers. Pediatrics 126 e493 e505 doi:10.1542/peds.2009-3027
Štítky
Interní lékařstvíČlánek vyšel v časopise
PLOS Medicine
2011 Číslo 10
- Ivabradin zlepšuje kvalitu života starších pacientů se srdečním selháním
- Fixní kombinace kandesartan/amlodipin v terapii arteriální hypertenze
- Inovace v hojení ran: krytí Zetuvit Plus Silicone Border pro optimální management exsudátu z ran
- Rána vizitkou (nejen) chirurga
- Patogeneze vzniku keloidní jizvy
Nejčtenější v tomto čísle
- STrengthening the Reporting of OBservational studies in Epidemiology – Molecular Epidemiology (STROBE-ME): An Extension of the STROBE Statement
- Universal Definition of Loss to Follow-Up in HIV Treatment Programs: A Statistical Analysis of 111 Facilities in Africa, Asia, and Latin America
- The Effect of Chromosome 9p21 Variants on Cardiovascular Disease May Be Modified by Dietary Intake: Evidence from a Case/Control and a Prospective Study
- Measuring the Performance of Vaccination Programs Using Cross-Sectional Surveys: A Likelihood Framework and Retrospective Analysis
Zvyšte si kvalifikaci online z pohodlí domova
Mazová zátka a její řešení
nový kurzVšechny kurzy