
Yield of Display Modules of Corneal Tomography for Early Diagnosis of Corneal Ectasia
Authors:
O. Vlasák 1,2; J. Škorpíková 1; Z. Hlinomazová 2; V. Kalandrová 2
Authors place of work:
Biofyzikální ústav Lékařské fakulty MU, Brno, přednosta prof. RNDr. Vojtěch Mornstein, CSc
1; Evropská oční klinika Lexum, lékařská ředitelka doc. MUDr. Zuzana Hlinomazová, Ph. D.
2
Published in the journal:
Čes. a slov. Oftal., 74, 2018, No. 5, p. 175-183
Category:
Původní práce
doi:
https://doi.org/10.31348/2018/5/2
Summary
The thesis deals with comparison of topographic corneal indexes and their importance for the diagnosis of corneal ectatic disease. The corneas with different stages of keratoconus, forme fruste keratoconus, pellucid marginal degeneration, corneal warpage syndrome, and physiological cornea with varying values of regular astigmatism were included in the tested group. The study was conducted in 2015–2018 at the European Eye Clinic Lexum Brno. The study group contained 208 eyes, 111 eyes with keratoconus, 31 eyes with forme fruste keratoconus, 23 eyes with pellucid marginal degeneration, 10 eyes with corneal warpage syndrome and 33 physiological eyes. 19 corneal parameters and indexes were monitored for these ectatic diseases, which were compared with healthy corneas with regular astigmatism. A single-factor ANOVA test, a Student t-test were used for statistical analysis. Pearson's coefficients were used to assess the correlation. In all the observed tomographic parameters a statistically significant difference was found between the physiological and ectatic group of corneas. The parameters with the highest statistical difference were BEThLo, ISV, IHD, D, Rmin. Statistically significant indices were also found between the forme fruste keratoconus and physiological corneas. The best parameters for detecting the subclinical keratoconus were the back elevation at the thinniest point of the cornea (BEThLo), the difference between the thinniest and the central point of cornea (CP-TL), the maximum pachymetic progression index and the Db and D indexes (p < 0.000). The most suitable parameters for the KK progression monitoring in our study were the ISV, KI, IVA, Df, D, Dp, Db, BEThLo and Rmin. All these parameters showed a strong correlation rate (r> 0.6) according to Pearson's correlation coefficient. Statistically significant differences in the KK and PMD groups were found in the index of relative pachymetry, central pachymetry, CKI and Dp.
Key words:
Pentacam, corneal ectasia, keratoconus, pellucid marginal degeneration, corneal warpage syndrome, forme fruste keratoconus
Introduction
With the arrival of more economical and precise laser methods of correcting ocular refractive errors, ever younger patients are undergoing corrective procedures. However, this fact presents a danger in the form of failure to discover or overlooking of corneal diseases which may be manifested only at a later age or after the laser refractive procedure. With the aid of corneal tomography we may project the parameters of the cornea into specific graphic maps and indexes. The aim of the study was to find a correlation between corneal indexes and the given corneal pathology. Which indexes show a change upon keratoconus, pellucid marginal degeneration and corneal warpage syndrome? A better understanding of these quantities may help us in the correct assessment of progression of any applicable disease, and thus also with the commencement of treatment. The observed corneal parameters which we compared in the study are listed and described below:
- ISV – Index of Surface Variance (of Keratometry)
- IVA – Index of Vertical Asymmetry
- KI – Keratoconus Index
- CKI – Centre Keratoconus Index
- IHA – Index of Height Asymmetry
- IHD – Index of Height Decentration
- Rmin – Index of minimum radius of corneal curvature
- Pmax – Index of maximum pachymetric progression
- BEThLo – Back elevation in thinnest location of cornea
- R. Pachy – Relative pachymetry
- Kmax – Maximum keratometry
- CP – Pachymetry in the centre of pupil
- TL – Pachymetry in the thinnest location of cornea
- Df – difference of elevations between 1BFS and 2ERS on
- anterior surface of cornea
- Db – difference of elevations between 1BFS and 2ERS on
- posterior surface of cornea
- Dp – pachymetric progression
- Dt – corneal thickness in the thinnest location
- Da – vertical distance of the thinnest location from corneal apex
- D – final index.
The indexed corneal data (D) is compared with a normative database. A comparison is also conducted of by how many standard deviations (SD) the given corneal data differs from the mean value of the norm. If the deviation is within the range of 1.6 to 2.6 times the SD, the value is displayed as borderline, in yellow. If the value is more than 2.6 times the SD, it is displayed in red.
Index of Surface Variance (ISV)
This is the index providing information about the irregularity of keratometry of the anterior segment of the cornea. It represents the dimensionless standard deviation of individual saggital radii of the cornea from the value of average curvature. We find an increased value in all types of irregularities of the anterior surface of the cornea (corneal scars, CWS, irregular astigmatism etc.). A value higher than 37 is considered abnormal (indicated in yellow) and a value higher than 41 is considered pathological (indicated in red).
Index of Vertical Asymmetry (IVA)
This index expresses in millimetres the difference between average upper and lower corneal curvature (also known as the I-S ratio). It therefore represents a type of index of symmetry of corneal curvature in which the dividing line between the upper and lower comparative parts is horizontal. Precisely as a result of this situation the IVA value in the central and horizontal point of the rotated KK (e.g. junctional type of KK) is not generally very high. An IVA value higher than 0.28 mm (approx. 1.5 D upon average Km = 43.5 D) is considered abnormal, above 0.32 mm (approx. 1.7 D) is considered pathological.
Keratoconus Index – KC Index (KI)
This is a dimensionless index providing information about the ratio between the average value of curvature between the upper and lower half of the cornea. A value above 1.07 is considered abnormal.
Centre Keratoconus Index (CKI)
This is a dimensionless index comparing the average values of saggital curvature in the central and peripheral ring. It serves primarily for the detection of the central form of KK. A value higher than 1.03 is considered abnormal.
Index of Height Asymmetry (IHA)
This index is an analogy of the IVA index, with the difference that we do not compare curvature but the value of elevation, thus the average value of the height elevation map of the upper and lower part of the cornea. The reference line is again horizontal. In the central form of KK we do not find such increased values as in the classic form. It is expressed in micrometres and we consider a value higher than 19 microns to be abnormal, 21 microns pathological. This is a newer index than IVA (S-I), which also showed higher sensitivity in the area of detection of KK.
Index of Height Decentration (IHD)
The value of deviation of elevation in a vertical direction, expressed in micrometres, is calculated from a Fourier analysis. It is calculated in a 3-millimetre ring. An abnormal value is higher than 0.014 microns, pathological is higher than 0.016 microns.
Index of minimum radius of corneal curvature (Rmin):
This index states the lowest measured value of saggital curvature in millimetres. A value lower than 6.71 mm is considered abnormal. The average value is 7.87 ± 0.27 mm (1).
METHOD
The data collection took place from 2015 to 2018 at the European Eye Clinic Lexum in Brno. The examined cohort contains 208 eyes, of which 111 are eyes with keratoconus, 31 eyes with forme fruste keratoconus (FFKC), 23 eyes with pellucid marginal degeneration, 10 eyes with corneal warpage syndrome and 33 eyes are physiological. The measurement was conducted on a Pentacam corneal tomograph (Oculus Optikgerate GmbH, Wetzlar, Germany). The version of diagnostic and display software was 1.20r41 (build: 2474). The measurement was conducted by specially trained personnel. The validity of the measurement was not allowed to decrease beneath 95%, the balance of the images was monitored on a Scheimpflug image overview display. Primarily the following three display interfaces were used for visualisation of the corneal parameters: Hollady Report, Belin/Ambrósio Enhanced Ectasia and Refractive report. The stage of keratoconus was determined with the aid of Amsler-Muckenhirn (2) classification of the Pentacam instrument. This classification does not incorporate the degree of cornea thinning and its ectatic changes on the posterior surface (3). It gives a false negative evaluation of eyes with increased posterior elevation (keratoconus posterior) and conversely gives false positive evaluation of cases of dislocated corneal apex (this includes for example also conditions of fixation malfunction of the patient) (4).
Graph 1 presents a histogram of the age distribution of the examined cohort.

Table 2 summarises the representation of sex and diagnoses.


Table 3 presents the numerical and percentage distribution of the entire cohort according to the Amsler-Muckenhirn classification of keratoconus. The analytical software of the Pentacam instrument determined 72 eyes as physiological, 5 as abnormal, 10 as suspect and divided the remaining 121 eyes into KK stages 1 to 4. Upon a comparison with table 2, in which there are 43 eyes without ectatic changes (Physiological + CWS), we determine a difference of 29 eyes, which were erroneously falsely negative for ectatic pathology (the program did not state either abnormal or suspect values).

The data analysis took place within the program STATISTICA 12 (Statistica, Tulsa, OK, US). According to the frequency of data and the graphic appearance of the histograms, a single factor ANOVA test was used for the statistical analysis of three and more groups. The Pearson correlation coefficients r served us for assessing the relationships between two quantitative variables. A Student two-tailed t-test was chosen for comparison of the statistical significance of two quantitative variables. Statistical significance of the results was evaluated at a 5% level of significance (p < 0.05). Statistically significant values are highlighted in the tables in red.
RESULTS
The first to be analysed was the group of physiological and ectatic eyes (KK+PMD+FFKC). We found a statistically significant difference (p < 0.05) in all the examined attributes. The following table 4 illustrates the compared parameters of the cornea. These parameters are arranged according to statistical significance p.

We also assessed the differences between the group of physiological eyes and eyes with forme fruste keratoconus (FFKC). The results are summarised in table 5. The parameters are again arranged according to statistical significance p.

Table 5 shows the statistically significant difference in the values of BEThLo, CP-TL, Db, Pmax, D, Dp, IVA, Da, IHD, KI, Df, IHA and ISV. We see a manifest predominance of pachymetric indexes and parameters informing about the characteristics of the posterior surface of the cornea.
For an assessment of the correlation between the stage of KK and the examined corneal parameters we used a Pearson's correlation coefficient. The statistics include only corneas with KK. The result is presented in table 6.

Table 6 presents parameters with a strong degree of correlation (r > 0.6) with the stage of KK. It concerns the following values: ISV, KI, IHD, Rmin, IVA, Df, D, Db, Dp, BEThLo. Here we see a predominance of topographic indexes of the anterior surface of the cornea.
The last analysis determines differences between the group of eyes with KK and PMD. The results are illustrated in table 7.
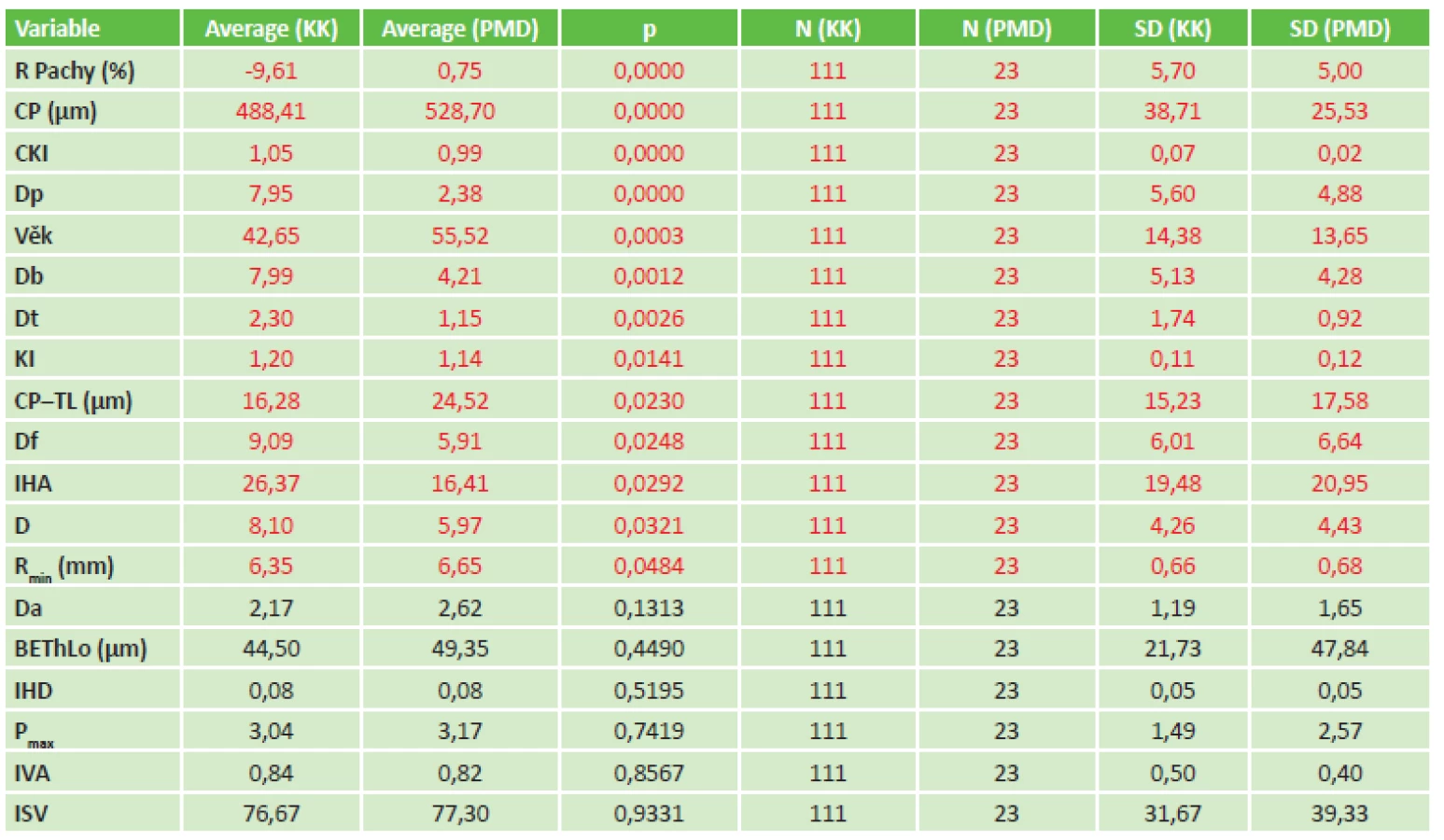
According to table 7, the most appropriate parameters for differential diagnostics include the KK and PMD values of relative and central pachymetry, the index Dp and CKI.
DISCUSSION
Several studies exist which confirm the essential role of corneal tomography in the diagnosis of ectasia (5-9). The studies determine which of the tomographic indexes are most alarming for the case of detection of ectatic cornea. Orucoglua et al. (10) present a large cohort of eyes (513 physiological and 612 keratoconic), but unfortunately do not analyse in further detail the group of eyes with keratoconus. The study confirms that in all the topometric indexes, a statistically significant difference was found between a healthy and ectatic cornea, and our study also corresponds with this finding. Huseynli et al. (11) assessed differences in tomographic parameters between normal, FFKC and KKC corneas in 249 eyes. The results in their keratoconic group were very similar, only the values of the IVA and IHD indexes were higher in the ectatic group in our study (IVA: 0.73 as against 0.52; IHD 0.07 as against 0.04). The results of the statistical analyses were in congruity, all the assessed parameters were statistically significantly different between both examined groups. In a study by R. Shetty et al. (12), the authors stated that the strongest topographic parameters for the detection of KK included the indexes ISV, IHA, IHD, KI, ARTmax and D. On the contrary, Hashemi et al. (13) evaluated KI, IVA, the value of lowest pachymetry and Kmax among the best parameters for the detection of KK. Studies from 2015 by Muftuoglu et al. (5) and Lopes et al. (14) primarily accentuate the contribution of the BAD-D index for the detection of KK. Our study confirms the results of these studies, although we evaluated BEThLo as the best parameter for the detection of KK. The final D index ranked among the five indexes with the highest value of statistical significance of the difference between physiological and ectatic corneas.
Although the diagnosis of advanced keratoconus can be performed easily on the basis of the presence of abnormal corneal tomographic indexes, the differentiation of forme fruste keratoconus from a normal cornea is generally difficult (15). Forme fruste (subclinical, suspect) keratoconus is the term used to denote the as yet unaffected eye in unilateral form of keratoconus. It concerns a cornea with clinically non-manifested keratoconus, in which keratoconus could erupt in the case of performance of laser surgery. The identification of forme fruste keratoconus is not common, since it is most frequently found in unilateral form of keratoconus. A study by Galletti et al. (16) informs us that for the detection of subclinical form of KK there are statistically significantly different values of pachymetric progression, elevation of the posterior surface, BEThLo, Df, Db, Dp and D. Our study demonstrated analogous results, we did not evaluate the standard value of elevation of the posterior surface of the cornea.
A number of studies indicate the insufficient sensitivity of topographic indexes of the anterior surface of the cornea, and recommend focusing on the parameters of its posterior surface, where keratoconic changes are expected to occur earlier (17-19). Our study confirms a greater contribution of parameters of the posterior surface as against the anterior in the role of detecting the subclinical form of KK, and corresponds with the results of the study by Uçakhana et al. (20). Only the value of minimal curvature of the anterior surface of the cornea did not demonstrate a statistically significant difference in our study (Rmin: p = 0.076). The parameters describing the posterior surface of the cornea (BEThLo, Db, D), together with the pachymetric ones (CP-TL, Pmax) formed a set of five indexes with the highest statistical difference (p < 0.0000) between FFKC and the physiological group of corneas. The best attribute for detection of FFKC in our study transpired to be the index of elevation of the posterior surface of the cornea in the location of lowest pachymetry, which is a component of the Belin – Ambrosio display. This fact is confirmed also by a study by Fukuda et al. (21). It is therefore possible to state that our study rather confirmed previous changes on the posterior surface of the cornea in the case of FFKC as opposed to changes on the anterior surface.
Assessment of the progression of ectatic pathology is one of the indication criteria for the commencement of treatment with the aid of collagen cross-linking (CXL). Since this is an irreversible procedure bringing irreversible changes on the cornea, correct assessment of the progression of ectasia is essential. According to the Global Consensus on Keratoconus and Ectatic Diseases (2015), no consistent or clear definition of the progress of ectasia exists (22). They defined the progression of KK by means of a change of at least two of the following parameters: increase of curvature of anterior surface of cornea, increase of curvature of posterior surface of cornea and thinning of cornea. Nevertheless, the panellists also concurred that there was a lack of specific quantitative data for defining the progression of KK (22). Chatzis et al. (23) in their study evaluated that demonstration of progression in children and adolescents should not be the decisive criterion for commencement of treatment. Other studies incline toward the view that it is necessary to demonstrate progression of keratoconus, but address the time intervals at which it is necessary to assess the progression of the disease, and which parameters are most important for assessment. V. Romano et al. (24) N.J.: 1995 state that a two-monthly follow-up for assessment of progression of KK is sufficient. Progression is confirmed upon increase of Kmax by at least 1.0 D and reduction of pachymetry in the thinnest location by 20 microns. Gore et al. (25) in their research combined the studies (26-28) of several teams of authors, and specified more precisely the level and type of recommended parameters for confirmation of progression of KK:
- Kmax > 1 D increase
- Kmax - Kmin > 1 D increase
- Kaverage > 0.75 D increase
- pachymetry > 2% reduction of central pachymetry
- keratometry at corneal apex > 1 D increase
- spherical equivalent > 0.5 D
Epstein et al. (29) recommended the value of maximum keratometry (Kmax) as the best single-factor indicator of the progression of KK. It is evident that Kmax is one of the most widely used indexes for the detection and evaluation of progression of ectasia. Nevertheless, in more recent studies it has been shown that the value of Kmax determined from a small part of the anterior surface of the cornea need not correspond to the degree of ectasia. It ignores the effect of the posterior surface of the cornea, and progression of KK may take place without a change of Kmax or even with a reduction thereof (30-32).
Kanellopoulose et al. (33) stated that for gradation of the stages of KK, the most sensitive indexes are ISV, IVA and IHD. The value of dioptric error and keratometry is not statistically significant for determining the stage of KK. As a classification schema they used the Amsler-Krumeich scale (34). Our study correlates with these results. The highest statistical significance was demonstrated by the indexes ISV, KI, IHD and Rmin. The IVA index was in 5th place of correlation (Rmin: r = 0.845; IVA: r = 0.795). Duncan et al. (35) noted the necessity of compiling information about the posterior surface of the cornea for assessing the progression of KK. They evaluated the more recent ABCD classification scale as more precise in comparison with methods comparing only the anterior surface of the cornea. Despite the fact that our analytical software on the Pentacam instrument did not yet contain the classification ABCD schema at the time of analysis, it was already possible to evaluate the parameters on which this classification is based and the indexes assessing also the posterior surface of the cornea (this concerns primarily the following indexes: BEThLo – back elevation in thinnest location of cornea, R Pachy – relative pachymetry, Db – difference of elevations between BFS and ERS on posterior surface of cornea). According to our study, the best parameters for gradation were the indexes ISV, KI, IHD, Rmin, IVA, Df, D, Db, Dp and BEThLo. We see that the indexes providing information about the posterior surface of the cornea (Db, D and BEThLo) are also in strong correlation with the stage of KK. Unfortunately we cannot unequivocally recommend any of the classification schemas for assessment of the stages of keratoconus, since we did not evaluate the latest ABCD classification schema, which was introduced after we gathered the research data. However, we can explicitly recommend that the used classification schema should contain both pachymetric indexes and topographic indexes from the anterior and posterior surface of the cornea. This is for the reason that in the initial stages of ectatic pathology, there is a predominance of progression of pathological values from the posterior surface, and later a predominance of progression of values from the anterior surface of the cornea.
In our study we also dealt with differentiation of KK and PMD. In practice we rather encounter a search for subclinical form of keratoconus and the issue of timely detection of PMD may be overlooked. Some ophthalmologists are of the opinion that in the case of PMD this represents only another peripheral form of keratoconus (36, 37). The differentiation of these two pathologies is important for determining the prognosis of the disease and the correct approach to treatment. Management of the treatment of PMD has its specifics in comparison with the treatment of KK, determined by the fact that although it is manifested primarily in the third to the fifth decade of life, it concerns a progressing disease (38). By contrast, manifestation and the greatest progression of KK occurs around the time of puberty, and diagnosed keratoconus in the fourth decade of life or later is generally rather in a pacific state. Cases of diagnosis of PMD at a young age are also known in the professional literature. Sridhar and Mahesh, in a group of 58 patients, presented an 8-year-old patient with PMD (39). Sinjab and Youssef in a cohort of 15 eyes presented a 16-year-old patient, and mentioned the term PLK (pellucide like keratoconus), which they indicated as an equivalent of FFKC in keratoconus (38). In our cohort the average age in PMD was 55.5 ± 13.6 years with a minimum of 33 years and maximum 74 years, in KK 42.7 ± 14.4 years with minimum 16 and maximum 80 years, in which these averages were statistically significantly different (p < 0.05). However, with reference to the above-mentioned study it is not possible to confirm that age is a valid criterion for differential diagnostics of KK and PMD. A risk of incorrect diagnosis of KK as against PMD is found in the case of correction of irregular curvature with the aid of intrastromal corneal ring segments (ICRs). This especially concerns the use of a ring in the inferior region of the cornea, where the greatest thinning takes place in PMD. For this reason the use of CXL may appear to be a better option for treatment of PMD (40).
In the case of PMD, flattening occurs in the vertical meridian, with induction of against-the-rule-astigmatism. Colour saggital display of the fragility of the cornea shows a characteristic appearance of two kissing penguins, or the claws of a bird of prey. As stated by Maguire et al., this appearance may be misleading, since we may encounter it also in the case of KK (36). There are few studies which compare the topographic parameters between these two pathologies. Lebow states a difference in the values of higher order aberrations, in which coma predominates in KK and trefoil in PMD (41). Koc et al. (42) compared inferior type of KK and PMD with physiological corneas. In the PMD group, all D indexes were higher than in the control group (p < 0.01), but at the same time were lower than in the group of inferior type of KK (with the exception of the Dt index p = 0.96). Our study corresponds with these results, although the Dt index also showed a statistically significantly lower value in PMD in comparison with KK (p = 0.003). However, we did not have only inferior types included in the KK group.
In our study we found a statistically significant difference between the group of KK and PMD in the following parameters: R Pachy, CP, CKI, age, CP-TL, IHA, Rmin, KI and all D indexes (Dp, Db, Dt, Df, D). Among the most statistically different parameters were R Pachy, CP, CKI and Dp. R Pachy informs us about the percentage deviation of pachymetry from the normalised referential body in the shape of a toric ellipsoid. In PMD a more positive percentage value appears in the centre of the cornea as opposed to the inferior periphery, where the greatest thinning occurs and thereby induction of the highest negative values of relative pachymetry. By contrast, in KK the greatest thinning occurs close to the centre of the cornea, thus the central values of relative pachymetry appear as negative. The highest negative values of relative pachymetry are found in the central, apical form of KK. The index of central pachymetry (CP) and centre keratoconus index (CKI) are similar. The CKI index provides information about the ratio of saggital curvature between the central and peripheral ring of keratometry. With regard to localisation of the place of highest curvature and thinning in the inferior periphery in PMD, both of these indexes will be less pathological than in KK. In our cohort of eyes with PMD, in certain cases they even reached normal values. For differential diagnostics between PMD and KK we therefore recommend a view of display of relative pachymetry, the value of CKI and CP.
CONCLUSION
The study confirmed the important role of corneal tomography on the principle of Scheimpflug display for the detection and evaluation of corneal ectasias. We statistically confirmed the significance of topographic and tomographic indexes for the differentiation of ectatic corneas from physiological. We determined that virtually all the parameters we selected (with the exception of age) are statistically significantly different between these groups. We evaluated the indexes ISV, IVA, KI, CKI, IHA, IHD, CP, TL, Df, Db, Dp, Dt, Da, D and also Rmin, BEThLo, R Pachy, Pmax and age. We found a correspondence with newer studies, which refute the view that one universal corneal parameter should be prioritised for the detection of ectasia. We rather recommend taking into account several corneal parameters, above all the values BEThLo, ISV, IHD, D and Rmin, which in our study showed themselves to be most promising in the area of detecting ectatic cornea.
In the area of detecting forme frust keratoconus, a slight shift away from the assessment of the parameters used from the anterior surface of the cornea is evident in international studies. Our study concurs with these opinions. We determined that the values of the pachymetric indexes and the indexes providing information about the characteristics of the posterior surface of the cornea are a suitable indicator of incipient corneal ectasia. This fact correlates with the view that ectatic changes of the cornea begin primarily on its posterior surface. Our study classified the indexes BEThLo, Db, D, CP-TL and Pmax among the parameters with the highest statistical significance. This group of five did not include any of the indexes providing information purely about the characteristics of the anterior surface of the cornea.
We found significance of these parameters also for the gradation of stages of keratoconus, which is important for an assessment of the progression of ectasia and initiation of applicable treatment. The parameters with a strong correlation (r > 0.6) with progression of keratoconus included ISV, KI, IHD, Rmin, IVA, Df, D, Db, Dp and BEThLo. Unfortunately we are unable to unequivocally recommend any of the classification schemas for assessment of the stages of keratoconus, since we did not evaluate the latest ABCD classification schema, which was introduced after our gathering of the research data.
Although some ophthalmologists are of the opinion that in the case of PMD this concerns only another peripheral form of keratoconus, we do not concur with this view. Between the group of KK and PMD we found statistically significant differences. Paradoxically, the parameters with the highest statistical difference did not include the age of patients but R Pachy, CP, CKI and Dp. In particular, the values and map display of relative pachymetry were demonstrated to be reliable in the differential diagnostics of these two corneal pathologies.
The authors of the study declare that no conflict of interest exists in the compilation, theme and subsequent publication of this professional communication, and that it is not supported by any pharmaceuticals company.
Received: 13. 6. 2018
Accepted: 30. 10. 2018
Available on-line: 27. 3. 2019
Mgr. Ondřej Vlasák, Ph.D.

Biofyzikální ústav Lékařské fakulty MU,
Brno
Zdroje
1. Moving keratoconus classification into the modern era | Ophthalmology Magazine [online]. [vid. 2018-07-11]. Dostupné z: https://www.eyeworld.org/article-moving-keratoconus-classification-into-the-modern-era
2. Crosslinking (x-linking, CXL) - Okulista.pl [online]. [vid. 2018-07-11]. Dostupné z: http://www.okulista.pl/oferta-crosslinking-x-linking-cxl--136.html
3. Belin, M., Khachikian, SS., Ambrosio, R.: Elevation based corneal tomography. 2012 [vid. 2018-07-17]. ISBN 978-9962-678-53-3. Dostupné z: http://lib.myilibrary.com/Open.aspx?id=615100
4. Sinjab, MM.: Corneal topography in clinical practice (Pentacam system): basics and clinical interpretation. New Delhi: Jaypee Bros. Medical Pub., 2012. ISBN 978-93-5025-575-9.
5. Muftuogulu, O., Ayar, O., Hurmeric, V. et al.: Comparison of multimetric D index with keratometric, pachymetric, and posterior elevation parameters in diagnosing subclinical keratoconus in fellow eyes of asymmetric keratoconus patients. J Cataract Refract Surg. 2015, 41(3), 557–565.
6. Toprak, I., Yaylali, V., Yilidirim, C.: A combination of topographic and pachymetric parameters in keratoconus diagnosis. Cont Lens Anterior Eye, 38(5); 2015 : 357–362.
7. Kamiya, K., Ishii, R., Shimizu, K. et al.: Evaluation of corneal elevation, pachymetry and keratometry in keratoconic eyes with respect to the stage of Amsler-Krumeich classification. Br J Ophthalmol, 98(4); 2014 : 459–463.
8. Bühren, J.: [Corneal topography and keratoconus diagnostics with Scheimpflug photography]. Der Ophthalmologe: Zeitschrift Der Deutschen Ophthalmologischen Gesellschaft, 111(10); 2014 : 920–926.
9. Galletti, JD., Vázquez, PRR., Minguez, N. et al.: Corneal asymmetry analysis by pentacam scheimpflug tomography for keratoconus diagnosis. J Cataract Refract Surg (Thorofare, N.J.: 1995), 31(2); 2015 : 116–123.
10. Orucoglu, F., Toker, E.: Comparative analysis of anterior segment parameters in normal and keratoconus eyes generated by scheimpflug tomography. J Ophthalmol, 2015; 2015 : 925414.
11. Huseynli, S., Abdulaliyeva, F.: Evaluation of Scheimpflug Tomography Parameters in Subclinical Keratoconus, Clinical Keratoconus and Normal Caucasian Eyes. Turk J Ophthalmol, 48(3); 2018 : 99–108.
12. Shetty, R., Rao, RH., Khamar, P. et al.: Keratoconus Screening Indices and Their Diagnostic Ability to Distinguish Normal From Ectatic Corneas. Am J Ophthalmol, 181; 2017 : 140–148.
13. Hashemi, H., Khabazkhoob, M., Pakazad, R. et al.: Pentacam Accuracy in Discriminating Keratoconus From Normal Corneas: A Diagnostic Evaluation Study. Eye Contact Lens. 2018.
14. Lopes, BT., Ramos, IC., Dawson, DG. et al.: Detection of ectatic corneal diseases based on pentacam. Zeitschrift Fur Medizinische Physik, 26(2); 2016 : 136–142.
15. Ambrósio, R., Caiado, ALC., Guerra, FP. et al.: Novel pachymetric parameters based on corneal tomography for diagnosing keratoconus. J Cataract Refract Surg (Thorofare, N.J.: 1995), 27(10); 2011 : 753–758.
16. Galletti, JD., Delrivo, M., Bonthoux, FF: et al.: Anterior Corneal Surface Descriptors, Posterior Elevation and Pachymetric Progression in Normal and Subclinical Keratoconus as Assessed by Pentacam. Invest Ophthalmol Vis Sci, 53(14); 2012 : 1104–1104.
17. Saad, A., Gantinel, D.: Topographic and tomographic properties of forme fruste keratoconus corneas. Invest Ophthalmol Vis Sci, 51(11); 2010 : 5546–5555.
18. De Sanctis, U., Loiacono, C., Richiardi, L. et al.: Sensitivity and specificity of posterior corneal elevation measured by Pentacam in discriminating keratoconus/subclinical keratoconus. Ophthalmology, 115(9); 2008 : 1534–1539.
19. De Sanctis, U., Aragno, V., Dalmasso, P. et al.: Diagnosis of subclinical keratoconus using posterior elevation measured with 2 different methods. Cornea, 32(7); 2013 : 911–915.
20. Ucakhan, Ö., Centikor, V., Özkan, M. et al.: Evaluation of Scheimpflug imaging parameters in subclinical keratoconus, keratoconus, and normal eyes. J Cataract Refract Surg, 37(6); 2011 : 1116–1124.
21. Fukunda, S., Beheregaray, S., Hoshi, S. et al.: Comparison of three-dimensional optical coherence tomography and combining a rotating Scheimpflug camera with a Placido topography system for forme fruste keratoconus diagnosis. Br J Ophthalmol, 97(12); 2013 : 1554–1559.
22. Gomes, J., Tan, D., Rapuano, Ch. et al.: Global consensus on keratoconus and ectatic diseases. Cornea, 34(4); 2015 : 359–369.
23. Chatzis, N., Hafezi, F.: Progression of keratoconus and efficacy of pediatric [corrected] corneal collagen cross-linking in children and adolescents. J Ophthalmol (Thorofare, N.J.: 1995), 28(11); 2012 : 753–758.
24. Romano, V., Vinciguerra, R., Arbabi, E. et al.: Progression of Keratoconus in Patients While Awaiting Corneal Cross-linking: A Prospective Clinical Study. J Cataract Refract Surg (Thorofare, N.J.: 1995), 34(3); 2018 : 177–180.
25. Gore, D., Shortt, A., Allan, B.: New clinical pathways for keratoconus. Eye (London, England), 27(3); 2013 : 329–339.
26. O’Brat, D., Chan, E., Samaras, K. et al.: A randomised, prospective study to investigate the efficacy of riboflavin/ultraviolet A (370 nm) corneal collagen cross-linkage to halt the progression of keratoconus. Br J Ophthalmol, 95(11); 2011 : 1519–1524.
27. Wittig-Silva, Ch., Whiting, M., Lamoureux, E. et al.: A randomized controlled trial of corneal collagen cross-linking in progressive keratoconus: preliminary results. J Cataract Refract Surg (Thorofare, N.J.: 1995), 24(7); 2008: S720-725.
28. Hersh, P., Greenstein, S., Fry, K.: Corneal collagen crosslinking for keratoconus and corneal ectasia: One-year results. J Cataract Refract Surg, 37(1); 2011 : 149–160.
29. Epstein, R., Chiu, Y., Epstein, G.: Pentacam HR criteria for curvature change in keratoconus and postoperative LASIK ectasia. J Refract Surg (Thorofare, N.J.: 1995), 28(12); 2012 : 890–894.
30. Tomidokoro, A., Oshika, S., Amano, S. et al.: Changes in anterior and posterior corneal curvatures in keratoconus. Ophthalmology, 107(7); 2000 : 1328–1332..
31. De Sanctis, U., Loiacono, C., Richiardi, L. et al.: Sensitivity and specificity of posterior corneal elevation measured by Pentacam in discriminating keratoconus/subclinical keratoconus. Ophthalmology, 115(9); 2008 : 1534–1539.
32. Mahmoud, A., Nunez, M., Blanco, C. et al.: Expanding the cone location and magnitude index to include corneal thickness and posterior surface information for the detection of keratoconus. Am J Ophthalmol, 156(6); 2013 : 1102–1111.
33. Kanellopoulos, A., Asimellis, G.: Revisiting keratoconus diagnosis and progression classification based on evaluation of corneal asymmetry indices, derived from Scheimpflug imaging in keratoconic and suspect cases. Clin Ophthalmol (Auckland, N.Z.), 7; 2013 : 1539–1548.
34. Amsler-Krumeich Classification for Grading Keratoconus – OphthaClass [online]. [vid. 2018-07-11]. Dostupné z: http://ophthaclassification.altervista.org/krumeichclass/
35. Duncan, J., Belin, M., Borgstorm, M.: Assessing progression of keratoconus: novel tomographic determinants. Eye and Vision, 3; 2016. [vid. 2018-07-16].
36. Maguire, L., Klyce, D., McDonald, M. et al.: Corneal topography of pellucid marginal degeneration. Ophthalmology, 94(5); 1987 : 519–524.
37. Sridhar, M., Mahesh, S., Bansal, K. et al.: Superior pellucid marginal corneal degeneration. Eye (London, England), 18(4); 2004 : 393–399.
38. Sinjab, M., Youssef, L.: Pellucid-like keratoconus. F1000Research, 1; 2012 : 48.
39. Sridhar, M., Mahesh, S., Bansal, A. et al.: Pellucid marginal corneal degeneration. Ophthalmology, 111(6); 2004 : 1102–1107.
40. Hassan, Z., Nemeth, G., Modis, L. et al.: Collagen cross-linking in the treatment of pellucid marginal degeneration. Indian J Ophthalmol, 62(3); 2014 : 367.
41. Do I See Keratoconus or PMD? [vid. 2018-07-17]. Dostupné z: https://www.reviewofoptometry.com/article/do-i-see-keratoconus-or-pmd
42. Crab claw pattern on corneal topography: pellucid marginal degeneration or inferior keratoconus? Eye. 22. září 2017 [vid. 2018-07-17]. Dostupné z: https://www.nature.com/articles/eye2017198
Štítky
OftalmologieČlánek vyšel v časopise
Česká a slovenská oftalmologie

2018 Číslo 5
- Selektivní laserová trabekuloplastika nesnižuje nitroční tlak více než argonová laserová trabekuloplastika
- Progresi glaukomu je třeba hodnotit strukturálními i funkčními parametry
- Ztráta centrálního vidění po filtrujících operacích glaukomu
- Od PGF-2 alfa-isopropyl esteru k latanoprostu: přehled vývoje Xalatanu
- Compliance u pacientů s glaukomem
Nejčtenější v tomto čísle
- Ocular Manifestations of Granulomatosis with Polyangiitis
- Merkel Cell Carcinoma of the Eyelids (Clinical-Histological Study)
- Pachychoroid Disease of the Macula – Case Report
- Pilot Results of Implantation of the New Hydrophobic Intraocular Lens Zeiss LUCIA 611P in the Czech Republic
Zvyšte si kvalifikaci online z pohodlí domova
Mazová zátka a její řešení
nový kurzVšechny kurzy