
Laparoscopic management of ovarian torsion at 26 weeks of gestation
Laparoskopická léčba torze vaječníku ve 26. týdnu gestace
Cíl: Uvádíme případ torze vaječníku ve 26. týdnu těhotenství, která byla úspěšně řešena laparoskopicky. Kazuistika: 29letá žena ve 26. týdnu těhotenství se dostavila na pohotovost s bolestí v levém dolním kvadrantu. Ultrazvukové vyšetření odhalilo cystu o rozměrech 64 × 60 mm v levém vaječníku a dopplerovské zobrazení nedokázalo detekovat průtok krve v levém vaječníku. Pacientce byla diagnostikována torze levého vaječníku a následně podstoupila laparoskopickou detorzi levého vaječníku a cystektomii. Pacientka neprodělala žádné pooperační chirurgické ani porodnické komplikace a měla nekomplikovaný vaginální porod ve 39. týdnu těhotenství. Závěr: Při chirurgické léčbě adnexální torze v těhotenství může být laparoskopie bezpečně provedena nejen v I. a II. trimestru, ale také ve III. trimestru, za předpokladu dostatečné chirurgické erudice a dostupného vhodného vybavení.
Klíčová slova:
těhotenství – laparoskopie – torze vaječníku
Authors:
İbrahim Kale
![]() ; Cem Yalçınkaya
; Cem Yalçınkaya
![]() ; Gülten Merve Özalp Çelikçi
; Gülten Merve Özalp Çelikçi
![]()
Authors place of work:
Department of Obstetrics and Gynecology, Umraniye Training and Research Hospital, Istanbul, Turkey
Published in the journal:
Ceska Gynekol 2025; 90(5): 395-397
Category:
Kazuistika
doi:
https://doi.org/10.48095/cccg2025395
Summary
Objective: We report a case of ovarian torsion at 26 weeks of gestation that was successfully managed laparoscopically. Case report: A 29-year-old woman at 26 weeks of pregnancy presented to the emergency department with left lower quadrant pain. Ultrasound examination revealed a 64 × 60 mm cyst in the left ovary, and Doppler imaging could not detect blood flow in the left ovary. The patient was diagnosed with left ovarian torsion and subsequently underwent laparoscopic left ovarian detorsion and cystectomy. The patient experienced no postoperative surgical or obstetric complications and had an uncomplicated vaginal delivery at 39 weeks of gestation. Conclusion: In the surgical management of adnexal torsion during pregnancy, laparoscopy can be safely performed not only in the 1st and 2nd trimesters but also in the 3rd trimester, provided that adequate surgical expertise and appropriate equipment are available.
Keywords:
pregnancy – laparoscopy – ovarian torsion
Backgroud
Adnexal torsion, which encompasses torsion of the ovary, fallopian tube, paratubal cyst, or a combination of these, is a common gynecologic emergency. Adnexal torsions occur more frequently on the right side than on the left. The lower incidence of left-sided torsion is attributed to the protective effect of the descending colon [1]. Isolated ovarian torsion occurs when the ovary rotates around the infundibulopelvic and/or utero-ovarian ligament, typically in the presence of a cyst or mass. This rotation can lead to partial or complete obstruction of blood flow within these ligaments, which contain the vascular supply to the ovary, resulting in clinical symptoms [1].
Ovarian torsion can occur at any age; however, it is most commonly observed in women of reproductive age. The reported incidence of ovarian torsion during pregnancy is 1.6 per 10,000 pregnancies [2]. The most important risk factors are ovarian cysts or masses and previous ovarian torsion [3]. Ovarian torsion typically presents with sudden-onset, severe, unilateral lower abdominal pain. This is often accompanied by nausea and vomiting and may be associated with signs of peritoneal irritation. Transabdominal ultrasonography is the preferred imaging modality for diagnosing adnexal torsion, with a sensitivity of 92% and a specificity of 96%. The torsioned ovary is typically enlarged and may be associated with free fluid in the abdomen. The absence of blood flow in the affected ovary on Doppler ultrasound further supports the diagnosis [1].
This report presents a case of ovarian torsion in a 26-week pregnant woman that was successfully managed with laparoscopic surgery.
Own observation
A 29-year-old woman at 26 weeks of gestation, calculated from her last menstrual period, presented to the emergency department with left lower quadrant pain. This was her second pregnancy, and she had a history of laparoscopic left salpingectomy for an ectopic pregnancy. The patient reported a 6-hour history of worsening left abdominal pain and was subsequently evaluated with ultrasound. The ultrasound revealed a single fetus in vertex presentation with positive fetal cardiac activity. Fetal measurements were consistent with the 26th week of gestation, and the estimated fetal weight was 867 grams. The amniotic fluid volume was normal, the placenta was on the posterior uterine wall, and the umbilical artery Doppler findings were consistent with the gestational age. A 64 × 60 mm cyst without septation was identified on the left ovary. Doppler ultrasound failed to assess blood flow in the left ovary. Transvaginal ultrasound showed a closed cervix with a length of 34 mm. The patient’s non-stress test test was reactive, and no uterine contractions were observed.
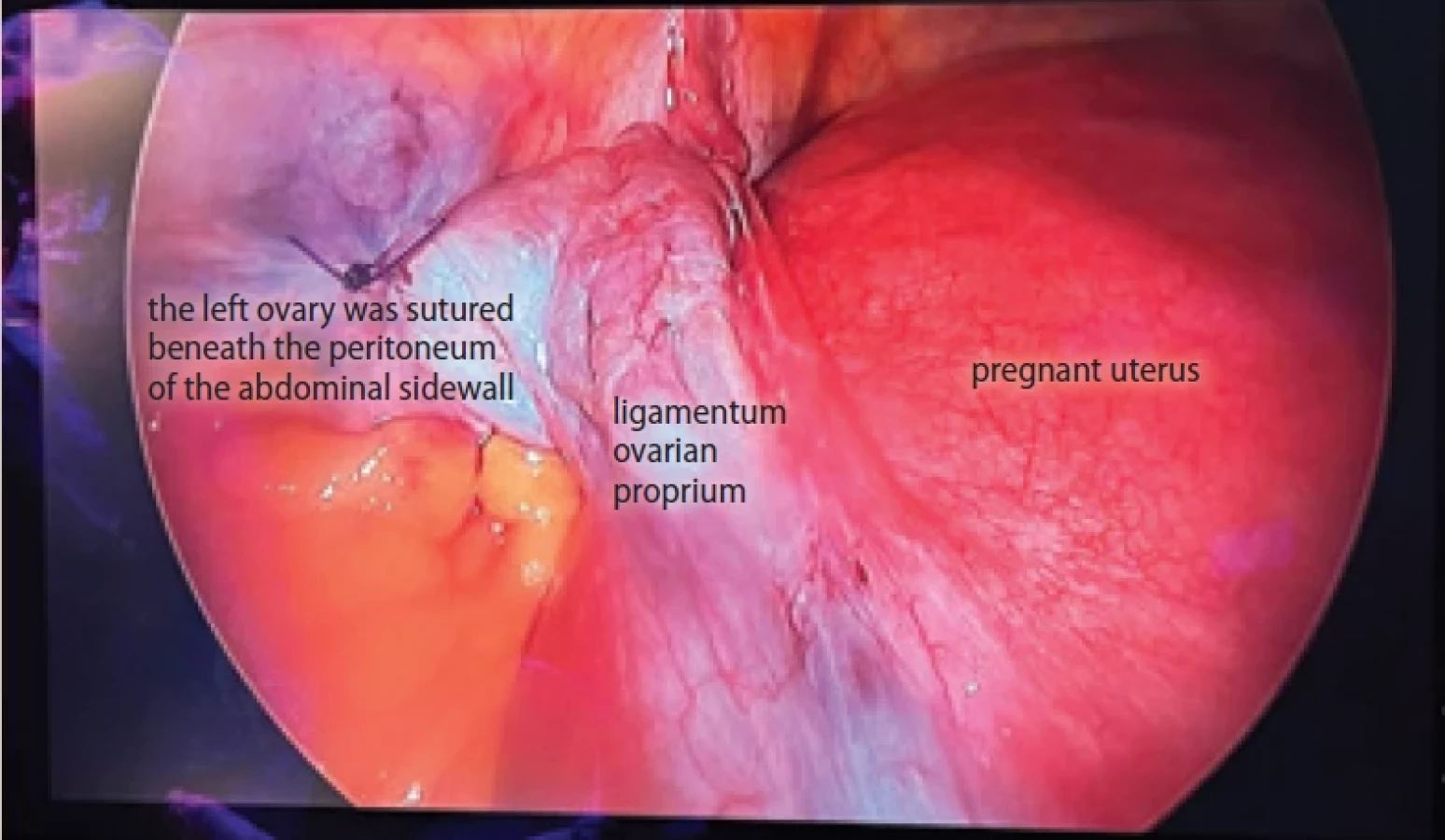
Based on the clinical presentation and ultrasound findings, the patient was diagnosed with left ovarian torsion, and laparoscopic surgery was planned. Before surgery, the location of the uterine fundus was confirmed using ultrasound guidance, and the Palmer point was marked on the abdominal skin. A Veress needle was inserted at the Palmer point to establish pneumoperitoneum at a pressure of 15 mmHg. Following this, a 10 - mm trocar was inserted at the Palmer point, followed by the introduction of a laparoscopic camera. Panoramic inspection revealed a normal right fallopian tube and ovary. On the left ovary, a cyst measuring approximately 6 cm in diameter was identified, accompanied by two complete torsions of the adnexa secondary to the cyst (Fig. 1). Considering the uterus, adnexal structures, and intestines, four 5 - mm trocars were placed: one on the right side of the rectus muscle, two on the left side, and one at the umbilicus. The left ovary was detorsioned, and the cyst was excised. The remaining ovarian tissue was repaired using sutures. The left infundibulopelvic and ovarian ligaments were observed to be significantly elongated and freely mobile. Therefore, to prevent re-torsion, the repaired left ovary was sutured to the abdominal sidewall after dissecting the peritoneum (Fig. 2). No surgical or obstetric complications occurred postoperatively. The patient had an uneventful vaginal delivery at 39 weeks of gestation. Histopathological examination of the cyst excised from the left ovary was consistent with a serous cystadenoma.

Discussion
Ovarian torsion occurs most frequently during the 1st and early 2nd trimesters of pregnancy, likely due to the presence of an enlarged corpus luteum cyst. It is less common in the 3rd trimester, as the gravid uterus exerts a compressive effect that restricts the mobility of the ovarian pedicles [4].
The American Association of Gastrointestinal and Endoscopic Surgeons published recommendations regarding the diagnosis, treatment, and use of laparoscopy for surgical conditions during pregnancy. According to these guidelines, laparoscopy is considered safe in all trimesters of pregnancy, with minimal morbidity for both the fetus and the mother. It is recommended that adnexal torsion be diagnosed and managed, and that detorsion be performed if the condition is identified before tissue necrosis occurs [5]. The Surgical Working Group for Minimally Invasive Surgery reported that laparoscopic surgery during pregnancy is safe for both the mother and the fetus. Additionally, they provided key recommendations for performing laparoscopic procedures in pregnant women with non-gynecological conditions [6].
Bassi et al. compared 1,336 cases of ovarian torsion during pregnancy with an equal number of cases in non-pregnant individuals. The findings indicated that laparotomy was significantly more frequently preferred for the surgical management of ovarian torsion in pregnant women, whereas laparoscopy was utilized at a considerably lower rate. Additionally, the rate of conversion from laparoscopic surgery to laparotomy was reported to be significantly lower in pregnant women compared to non-pregnant women [2]. In another study published in 2020, 33 pregnant women diagnosed with ovarian torsion were compared with 72 non-pregnant women regarding the surgical management of ovarian torsion. Among pregnant women with ovarian torsion, 45.4% were in the 1st trimester, 27.3% in the 2nd trimester, and 27.3% in the 3rd trimester. The preference for laparoscopic surgery was 15.2% in the pregnant group, compared to 54.2% in the non-pregnant group. Laparoscopic surgery was performed in 26.7% of cases during the 1st trimester and 11.1% during the 2nd trimester, while laparotomy was preferred in all cases during the 3rd trimester [4]. In a 2024 study, 155 pregnant women who underwent surgery for adnexal torsion at different gestational weeks were compared in terms of surgical outcomes. Among them, 102 underwent laparoscopic surgery, while 53 underwent laparotomy. All patients who underwent laparoscopy were in the 1st or 2nd trimester. Laparotomy was preferred in all cases of adnexal torsion in the 3rd trimester. Miscarriage rates, preterm birth rates, and gestational age at delivery were similar between the two groups [7].
As evident from the studies above, while the laparoscopic approach is commonly used to treat adnexal torsion in the 1st and 2nd trimesters, laparoscopic procedures in the 3rd trimester are rare and primarily reported as case studies [8,9]. Despite the well-documented advantages of laparoscopic surgery in managing adnexal masses, concerns persist regarding its use in pregnant women during the third trimester. These concerns primarily stem from the risk of uterine and fetal injury due to trocar placement and the potential adverse effects of pneumoperitoneum.
Conclusion
This case report describes the successful laparoscopic management of ovarian torsion in the early 3rd trimester. With adequate surgical expertise and appropriate equipment, we believe that adnexal torsion can be effectively treated using laparoscopic surgery even in the 3rd trimester.
Zdroje
1. Adnexal torsion in adolescents: ACOG committee opinion No, 783. Obstet Gynecol 2019; 134 (2): e56–e63. doi: 10.1097/AOG.0000000000003373.
2. Bassi A, Czuzoj-Shulman N, Abenhaim HA. Effect of pregnancy on the management and outcomes of ovarian torsion: a population-based matched cohort study. J Minim Invasive Gynecol 2018; 25 (7): 1260–1265. doi: 10.1016/j.jmig.2018.03.022.
3. Asfour V, Varma R, Menon P. Clinical risk factors for ovarian torsion. J Obstet Gynaecol 2015; 35 (7): 721–725. doi: 10.3109/01443615.2015.1004524.
4. Wu WF, Wang ZH, Xiu YL et al. Characteristics and surgical invervention of ovarian torsion in pregnant compared with nonpregnant women. Medicine (Baltimore) 2020; 99 (24): e20627. doi: 10.1097/MD.0000000000020627.
5. Pearl J, Price R, Richardson W et al. Guidelines for diagnosis, treatment, and use of laparoscopy for surgical problems during pregnancy. Surg Endosc 2011; 25 (11): 3479–3492. doi: 10.1007/s00464-011-1927-3.
6. Förster S, Reimer T, Rimbach S et al. CAMIC recommendations for surgical laparoscopy in non-obstetric indications during pregnancy. Zentralbl Chir 2016; 141 (5): 538–544. doi: 10.1055/s-0035-1545904.
7. Zhang Z, Zhang Y, Fu H et al. Laparotomy versus laparoscopy for the treatment of adnexal torsion during pregnancy. BMC Pregnancy Childbirth 2024; 24 (1): 714. doi: 10.1186/s12884-024-06898-x.
8. Bernigaud O, Fraison E, Thiberville G et al. Ovarian torsion in a twin pregnancy at 32 weeks and 6 days: a case-report. J Gynecol Obstet Hum Reprod 2021; 50 (6): 102117. doi: 10.1016/j.jogoh.2021.102117.
9. Lapides A, Ma W, McKinney C et al. Laparoscopically-treated ovarian torsion in a 32-week pregnancy: a case report. Case Rep Womens Health 2023; 37: e00496. doi: 10.1016/j.crwh.2023.e00496.
ORCID of authors
İ. Kale 0000-0001-7802-7199
C. Yalçınkaya 0000-0001-7533-0838
G. M. Ö. Çelikçi 0000-0002-3504-8632
Submitted/Doručeno: 15. 3. 2025
Accepted/Přijato: 10. 4. 2025
İbrahim Kale, MD
Department of Obstetrics and Gynecology
Umraniye Training and Research Hospital
Elmalıkent, Adem Yavuz Cd.
34764 Ümraniye/İstanbul
Turkey
dribakale@hotmail.com
Štítky
Dětská gynekologie Gynekologie a porodnictví Reprodukční medicínaČlánek vyšel v časopise
Česká gynekologie

2025 Číslo 5
- Inosin pranobex v léčbě HPV infekcí děložního čípku
- Aktuální doporučení EAU pro léčbu nekomplikovaných cystitid
- Vědecké poznatky rozptylující obavy spojené s používáním nitroděložní antikoncepce i u mladých žen
- Používání intrauterinních tělísek uvolňujících měď a riziko tubární infertility u nuligravidních žen
- Účinnost dlouhodobě působící reverzibilní antikoncepce
Nejčtenější v tomto čísle
- Vaginal fisting and risk of anogenital injury
- Placental insufficiency and late-onset growth restriction in fetuses appropriate for gestational age
- Results of the Endometriosis Health Profile-30 questionnaire in women aged 18– 30 years in the Czech Republic
- Prevalence and hormonal profiling of secondary amenorrheic patients presenting to a fertility clinic – an observational study
Zvyšte si kvalifikaci online z pohodlí domova
Mazová zátka a její řešení
nový kurzVšechny kurzy