
Which causes less pain? A comparison of misoprostol and dinoprostone in labor induction
Který způsobuje menší bolest? Srovnání misoprostolu a dinoprostonu při indukci porodu
Cíl: Efektivní zvládání porodní bolesti je v prenatální péči zásadní. Identifikace faktorů, které přispívají ke zvýšené bolesti u pacientek podstupujících indukci porodu, je nezbytná pro optimalizaci kontroly bolesti. Tato studie hodnotí úroveň bolesti u pacientek po indukci porodu, kterým je vaginálně podáván misoprostol nebo dinoproston pro zrání děložního čípku, pomocí vizuální analogové stupnice (VAS – visual analog scale). Materiály a metody: Tato prospektivní studie zahrnuje 60 dobrovolnic, kterým byl podáván buď vaginálně dinoproston (50 %), nebo vaginálně misoprostol (50 %) jako látky podporující zrání děložního čípku. Skupina 1 se skládá z pacientek, jimž byl podáván misoprostol, skupina 2 zahrnuje pacientky, kterým byl podáván dinoproston. Skóre VAS bylo zaznamenáváno jak během aktivního porodu, tak i během porodu. Kromě těchto hodnocení bolesti byly zdokumentovány výsledky porodu a charakteristiky pacientek, mezi skupinami byly provedeny srovnávací analýzy. Výsledky: Podle skóre VAS byla intenzita bolesti ve skupině 1 v obou fázích porodu významně nižší ve srovnání se skupinou 2 (během aktivního porodu: 6,67 ± 2,68 vs. 7,77 ± 1,59; p < 0,05; během období korunkování: 8,9 ± 1,32 vs. 9,8 ± 0,55; p < 0,05). Skóre bolesti všech účastnic zaznamenané během korunkování bylo významně vyšší než skóre zaznamenané během aktivního porodu (p < 0,05). Mezi oběma látkami nebyl pozorován žádný statisticky významný rozdíl, pokud jde o podávání oxytocinu ani o interval od podání léku do porodu (p > 0,05). Závěr: Při výběru látky podporující zrání děložního čípku je třeba zohlednit skóre bolesti. Misoprostol může být spojen s nižší úrovní bolesti.
Klíčová slova:
misoprostol – dinoproston – zrání děložního čípku – porodní bolest – vizuální analogová stupnice
Authors:
Sultan Canan 1
![]() ; Sare Cancu Kalkan 2
; Sare Cancu Kalkan 2
![]() ; Selçuk Özden 1,3
; Selçuk Özden 1,3
![]() ; Hilal Uslu Yuvaci 1,3
; Hilal Uslu Yuvaci 1,3
![]() ; Mehmet Sühha Bostanci 1,3
; Mehmet Sühha Bostanci 1,3
![]()
Authors place of work:
Department of Obstetrics and Gynecology, Sakarya Training and Research Hospital, Sakarya, Turkey
1; Labor and Delivery Unit, Sakarya Training and Research Hospital, Sakarya, Turkey
2; Sakarya University Faculty of Medicine, Department of Obstetrics and Gynecology, Sakarya, Turkey
3
Published in the journal:
Ceska Gynekol 2025; 90(6): 442-446
Category:
Původní práce
doi:
https://doi.org/10.48095/cccg2025442
Summary
Objective: Effective labor pain management is essential in prenatal care. Identifying factors that contribute to increased pain in patients undergoing labor induction is essential for optimizing pain control. This study assesses pain levels in labor induction patients receiving vaginal misoprostol or dinoprostone for cervical ripening using a visual analogue scale (VAS). Materials and methods: This prospective study includes 60 volunteer women who received either vaginal dinoprostone (50%) or vaginal misoprostol (50%) as cervical ripening agents. Group 1 consists of patients who received misoprostol, while Group 2 includes those who were administered dinoprostone. VAS scores were recorded during both active labor and crowning. In addition to these pain assessments, birth outcomes and patient characteristics were documented, and comparative analyses were conducted between the groups. Results: According to VAS scores, pain intensity was significantly lower in Group 1 compared to Group 2 at both stages of labor (during active labor: 6.67 ± 2.68 vs. 7.77 ± 1.59, P < 0.05; during crowning: 8.9 ± 1.32 vs. 9.8 ± 0.55, P < 0.05). All participants’ pain scores recorded during crowning were significantly higher than those recorded during active labor (P < 0.05). No statistically significant difference was observed between the two agents in terms of oxytocin administration or the interval from drug administration to delivery (P > 0.05). Conclusions: Pain scores should be considered when selecting a cervical ripening agent. Misoprostol may be associated with lower pain levels.
Keywords:
labor pain – misoprostol – dinoprostone – cervical ripening – visual analogue scale
Introduction
In current obstetrics worldwide, a practical, safe, and comfortable method of labor induction is an essential part of active prenatal care. Although there are various debates about the timing of labor, once the decision to induce labor is made, we have a limited number of tools at our disposal to manage an unfit cervix. These tools can be divided into mechanical and pharmacological methods. A definitive method has not yet been determined as a cervical ripening agent because no agent is superior to the other [1].
Prostaglandins are frequently used as pharmacological agents for cervical ripening. Misoprostol is a synthetic analog of prostaglandin E1 [2]. Although it was produced to treat stomach ulcers, it is now widely used in labor induction due to its effect as a cervical ripening agent [3]. Dinoprostone is a prostaglandin E2 analog frequently used in labor induction [4]. Many studies investigate the superiority of these two commonly used agents, but the superiority of one over the other has not been proven [2,5,6].
Regular uterine contractions during labor physiologically cause labor pain [7]. In addition, stretching of the vaginal wall during the delivery is one of the causes of labor pain [8]. While birth pain may be due to physiological reasons, psychological causes such as fear of childbirth have also been identified [9]. Cervical ripening agents are known to increase labor pain [10]. Since the cause of labor pain is not fully known, identifying the factors that affect the increase in pain will help in prevention.
Although no universally standardized scale for assessing labor pain has been established, spesific tools are widely recognized for their reliability and effectiveness. Among these, the visual analog scale (VAS) is commonly used in clinical practice and research to quantify and characterize pain intensity and quality [11]. Given its widespread clinical use, ease of application, and validated reliability in assessing acute pain, the VAS was employed in this study to evaluate the subjective intensity of labor pain quantitatively. This unidimensional tool allowed for a standardized and objective comparison of pain perception across different stages of labor.
Labor induction should be safe, effective, and also comfortable. Therefore, in this study, we aimed to investigate the pain effect of using vaginal misoprostol and dinoprostone vaginal inserts on labor pain in elective induction in low - -risk patients.
Materials and methodology
This study was designed as a prospective case-control study. After receiving approval from the Non-Interventional Ethics Committee of Sakarya University Faculty of Medicine, the study followed the Declaration of Helsinki (Approval No: 258126-196, Date: 23.06.2023). All study participants were informed about the study process, and informed consent forms were obtained.
Patient selection
The study was planned with patients who were admitted to Sakarya Training and Research Hospital Labor Ward between June 2023 and September 2023, with a decision to induce labor due to late-term pregnancy. Criteria for inclusion in the study were volunteering, having used a cervical ripening agent during labor follow-up, having no additional risk factors, being over 18 years of age, and being fluent in Turkish.
a) not wanting to participate in this study;
b) withdrawing at any time during the process after wishing to participate in the study;
c) labor follow-up resulting in a cesarean section;
d) operative vaginal birth;
e) performing an episiotomy;
f) shoulder dystocia during labor;
g) use of labor assisting maneuvers for any reason;
h) use of any labor analgesia;
i) high-risk pregnancy (e. g., preeclampsia, diabetes mellitus, fetal growth restriction, oligohydramnios, polyhydramnios, etc.);
j) preterm birth;
k) the decision to give birth for any reason other than late-term pregnancy;
l) not knowing Turkish were the reasons for exclusion from the study.
High-risk pregnancies were excluded from the study because they may affect pain through unknown mechanisms and cause deviation in the outcome. Only low-risk pregnancies were included in the study. Among the indications for labor induction, only late-term pregnancy (between 41 0/7 and 41 6/7 weeks [12]) was included in the study.
Application of cervical ripening agent
In Group 1, 25 mcg of misoprostol (Cytotec®; Pfizer) was administered vaginally. The application was repeated every 6 hours until the Bishop score reached 9. In Group 2, 10 mg of dinoprostone (Propess®; Ferring Pharmaceuticals) was administered, and the application continued until the Bishop score reached 6, at which point it was stopped [13].
Assessment of labor pain intensity
Pain assessment in this study was conducted using a validated self-report tool: the VAS, which quantitatively measures the subjective intensity of pain. Participants were asked to indicate their perceived pain level on a 10-centimeter horizontal line, ranging from “no pai” (0) on one end to “worst imaginable pain” (10) on the other [14]. VAS scores were recorded at two distinct stages of labor: during the active phase and at the time of crowning. This approach allowed for a standardized and reliable evaluation of pain intensity across different time points in the labor process.
Scorings were performed on each patient in the first and second stages of labor. The initial scoring was done in the first stage, when active uterine contractions disrupted the patient’s comfort, and the cervical dilation was 5 or 6 cm. The second scoring was performed during the crowning. All scoring was done by a single investigator, blind to the cervical ripening agents used throughout the study.
Data acquisition
After all scoring was completed and recorded, data on patients’ demographic characteristics, gestational age at birth, the type of cervical ripening agent used, the timing of its application, and the time of birth were obtained from the hospital’s computerized record system and archive files. These data were then documented for analysis.

Study outcomes
This study’s primary outcomes were the VAS score during active labor and the VAS score during crowning. The secondary outcomes assessed in this study included the time interval from drug administration to delivery, the total duration of oxytocin administration, and the difference in VAS pain scores between the active phase of labor and the crowning stage. This comparison was conducted to evaluate pain intensity progression throughout labor and capture potential variations in pain perception at distinct stages.
Statistical analysis
Descriptive analyses were conducted to obtain information regarding the general characteristics of the study population. The normality of the data was assessed using the Shapiro-Wilk test and by analyzing kurtosis and skewness values. Differences in characteristic features among patient groups were evaluated using the independent two-sample T-test for normally distributed parameters and the Mann-Whitney U-test for non-normally distributed parameters. Categorical variables were analyzed using Pearson’s chi-square test.
Continuous variables for parametric analyses were expressed as mean ± ± standard deviation, whereas categorical variables were presented as percentages and frequencies. For nonparametric continuous variables, median values and interquartile ranges (Q3–Q1) were provided in brackets. Additionally, a paired-sample T-test was conducted to examine changes in pain scores during active labor and crowning.
A P-value of < 0.05 was considered statistically significant. Statistical analyses were performed using IBM SPSS Statistics, Version 23.0 (Armonk, NY: IBM Corp.).
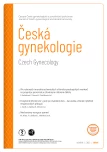
![VAS in the patient groups [14]. Tab. 2. VAS ve skupinách pacientů [14].](https://pl-master.mdcdn.cz/media/cache/media_object_image_large/media/image/87f8068b6ef9741ac69a76ab24c67520.png)
Results
Sixty volunteers who received cervical ripening agents were included in this study. Thirty of them received vaginal misoprostol, and 30 received vaginal dinoprostone.
Among the analyzed variables, age, body mass index (BMI), cervical effacement during active labor, fetal head station during active labor, VAS score during active labor, and VAS score during crowning exhibited a normal distribution. In contrast, the other variables did not follow a normal distribution.
The analysis revealed no statistically significant differences between the two groups concerning their characteristic features, as demonstrated in Tab. 1.
The comparison of VAS revealed higher scores in Group 2 than in Group 1 at both stages (Tab. 2).
In addition to these findings, a paired-sample T-test indicated a significant increase in VAS from active labor to crowning. VAS score was higher during crowning than during active labor (M = –2.133, SD = 1.567, t (59) = –10.543, P < 0.001, 95% CI (–2.538, –1.728)).
Discussion
In recent years, the frequency of labor induction has been rising in developed and developing countries, particularly in many middle - and high-income nations [15]. Although the indications for labor induction vary, no cervical ripening method has been proven to be superior to others in improving labor progression or birth outcomes [16]. Consequently, the choice of method is mainly based on the physician’s preference and experience. This study contributes to the developing scientific evidence supporting the selection of cervical ripening agents with consideration for patient comfort.
Labor is inherently associated with significant pain, and a substantial proportion of women require analgesic support during the process. To address this need, pharmacological and non-pharmacological pain management strategies have been developed and are continually refined [17]. Selecting a method that minimizes pain from the onset of labor may also reduce the need for additional analgesia. The findings of this study underscore the importance of considering maternal pain perception when selecting a cervical ripening agent. Specifically, misoprostol was associated with significantly lower pain scores compared to dinoprostone during both the active phase of labor and the crowning stage, suggesting a potential advantage of misoprostol in maternal comfort. However, further studies are warranted to validate these results and to explore the underlying mechanisms contributing to the difference in pain perception between these two agents.
Previous studies and meta-analyses have evaluated misoprostol and dinoprostone’s primary maternal and neonatal outcomes [16,18]. These outcomes primarily focused on maternal factors such as vaginal delivery rates, cesarean section rates, the need for additional oxytocin, and uterine tachysystole [19–22]. Evidence indicates no clear superiority between these two cervical ripening agents regarding key maternal outcomes [16]. However, our study is the first to investigate their effects on labor pain. We found that, in this regard, misoprostol offers a more significant advantage over dinoprostone.
Although the difficulty of labor pain is experienced seriously by patients, some patients refuse labor analgesia for various reasons [23]. However, it has been found that this painful process increases postpartum depression [24]. Therefore, it would be a mistake to think of labor pain as a short-term, transient condition and to ignore it due to the patient’s refusal. In order to make this process less painful from the beginning, misoprostol can be chosen as a cervical ripening agent.
A recent study compared the effects of oral misoprostol, vaginal misoprostol, and vaginal dinoprostone on labor duration and found no significant difference in the time from drug administration to delivery [20]. Consistent with the existing literature, our study also showed no significant difference between the vaginal misoprostol and vaginal dinoprostone groups in terms of the time interval between administration and delivery.
This study determined that oxytocin administration was similar in both groups, with no statistically significant difference. These findings align with the existing literature [21].
Evidence has demonstrated that pain perception and intensity increase as labor progresses [25]. Similarly, our findings indicate that pain was more intense during crowning in both medication groups. Consistent with the literature, these results suggest that labor analgesia should not be overlooked during the crowning phase.
The limitation of our study is the small sample size. However, this can be explained by our hospital’s approach to labor pain management. As a standard practice, we provide comprehensive education on pain-relief options both during the antenatal period and from admission to the delivery room until birth. We actively encourage patients to consider pharmacological and non-pharmacological pain relief methods. As a result, the number of patients who do not receive any form of labor analgesia is relatively low.
Conclusion
Labor pain is a crucial factor that should be considered when selecting the appropriate cervical ripening agent for labor induction. Both misoprostol and dinoprostone are commonly used prostaglandins for this purpose, each with distinct pharmacological properties and effects on uterine activity. While both agents are effective in promoting cervical ripening and facilitating labor progression, emerging evidence suggests that misoprostol may be associated with less labor pain compared to dinoprostone. This potential difference in pain perception could have significant implications for maternal comfort, pain management strategies, and overall birth experience.
Despite these observations, the current body of literature remains limited, and further large-scale, well-designed studies are needed to validate these findings. Future research should compare the severity and duration of labor pain associated with different induction agents while considering other relevant factors such as labor duration, neonatal outcomes, and maternal satisfaction. Understanding the impact of labor pain on patient outcomes could lead to more individualized approaches to labor induction, ultimately improving maternal and perinatal care.
Zdroje
1. Blanc-Petitjean P, Carbonne B, Deneux-Tharaux C et al. Comparison of effectiveness and safety of cervical ripening methods for induction of labour: a population-based study using coarsened exact matching. Paediatr Perinat Epidemiol 2019; 33 (5): 313–322. doi: 10.1111/ppe.12569.
2. Datta MR, Ghosh MD, AyazAhmed Kharodiya Z. Comparison of the efficacy and safety of sublingual versus oral misoprostol for the induction of labor: a randomized open-label study. Cureus 2023; 15 (11): e49422. doi: 10.7759/cureus.49422.
3. Zordo SD. The biomedicalisation of illegal abortion: the double life of misoprostol in Brazil. Hist Cienc Saude Manguinhos 2016; 23 (1): 19–36. doi: 10.1590/S0104-59702016000100003.
4. Socha MW, Flis W, Pietrus M et al. Results of induction of labor with prostaglandins E1 and E2 (the RIPE Study): a real-world data analysis of obstetrical effectiveness and clinical outcomes of pharmacological induction of labor with vaginal inserts. Pharmaceuticals (Basel) 2023; 16 (7): 982. doi: 10.3390/ph16070982.
5. Bakker R, Pierce S, Myers D. The role of prostaglandins E1 and E2, dinoprostone, and misoprostol in cervical ripening and the induction of labor: a mechanistic approach. Arch Gynecol Obstet 2017; 296 (2): 167–179. doi: 10.1007/s00404-017-4418-5.
6. Gornisiewicz T, Kusmierska-Urban K, Huras H et al. Comparison of Misoprostol versus Dinoprostone for delivery induction among pregnant women without concomitant disease. Ginekol Pol 2020; 91 (12): 726–732. doi: 10.5603/ GP.2020.0119.
7. Hulsbosch LP, Nyklicek I, Potharst ES et al. Development of the Labor Pain Relief Attitude Questionnaire for pregnant women (LPRAQ-p). BMC Pregnancy Childbirth 2020; 20 (1): 718. doi: 10.1186/s12884-020-03415-8.
8. Gido R, Yadeta TA, Tura AK. Utilization of obstetric analgesia for labor pain management and associated factors among obstetric care providers in public hospitals of addis ababa, Ethiopia: a cross-sectional study. Obstet Gynecol Int 2021; 2021 : 9973001. doi: 10.1155/2021/9973001.
9. Huang Y, Zhong Y, Chen Q et al. A comparison of childbirth self-efficacy, fear of childbirth, and labor pain intensity between primiparas and multiparas during the latent phase of labor: a cross-sectional study. BMC Pregnancy Childbirth 2024; 24 (1): 400. doi: 10.1186/s12884-024-06571-3.
10. Saad AF, Pedroza C, Gavara R et al. Dilapan-S vs standard methods for cervical ripening in term pregnancies: an individual patient data meta-analysis. Am J Obstet Gynecol MFM 2024; 7 (1): 101583. doi: 10.1016/j.ajogmf.2024.101583.
11. Winkelman C, Norman D, Maloni JA et al. Pain measurement during labor: comparing the visual analog scale with dermatome assessment. Appl Nurs Res 2008; 21 (2): 104–109. doi: 10.1016/j.apnr.2006.05.002.
12. Practice bulletin no. 146: Management of late-term and postterm pregnancies. Obstet Gynecol 2014; 124 (2 Pt 1): 390–396. doi: 10.1097/01.AOG.0000452744.06088.48.
13. ACOG Practice Bulletin No. 107: Induction of labor. Obstet Gynecol 2009; 114 (2 Pt 1): 386–397. doi: 10.1097/AOG.0b013e3181b48ef5.
14. Delgado DA, Lambert BS, Boutris N et al. Validation of digital visual analog scale pain scoring with a traditional paper-based visual analog scale in adults. J Am Acad Orthop Surg Glob Res Rev 2018; 2 (3): e088. doi: 10.5435/JAAOS Global-D-17-00088.
15. Hedegaard M, Lidegaard O, Skovlund CW et al. Perinatal outcomes following an earlier post-term labour induction policy: a historical cohort study. BJOG 2015; 122 (10): 1377–1385. doi: 10.1111/1471-0528.13299.
16. Lakho N, Hyder M, Ashraf T et al. Efficacy and safety of misoprostol compared with dinoprostone for labor induction at term: an updated systematic review and meta-analysis of randomized controlled trials. Front Med (Lausanne) 2024; 11 : 1459793. doi: 10.3389/fmed.2024.1459793.
17. Jones L, Othman M, Dowswell T et al. Pain management for women in labour: an overview of systematic reviews. Cochrane Database Syst Rev 2012; 2012 (3): CD009234. doi: 10.1002/14651858.CD009234.pub2.
18. Wang L, Zheng J, Wang W et al. Efficacy and safety of misoprostol compared with the dinoprostone for labor induction at term: a meta-analysis. J Matern Fetal Neonatal Med 2016; 29 (8): 1297–1307. doi: 10.3109/14767058. 2015.1046828.
19. Gregson S, Waterstone M, Norman I et al. A randomised controlled trial comparing low dose vaginal misoprostol and dinoprostone vaginal gel for inducing labour at term. BJOG 2005; 112 (4): 438–444. doi: 10.1111/j.1471-0528. 2004.00496.x.
20. Young DC, Delaney T, Armson BA et al. Oral misoprostol, low dose vaginal misoprostol, and vaginal dinoprostone for labor induction: randomized controlled trial. PLoS One 2020; 15 (1): e0227245. doi: 10.1371/journal.pone. 0227245.
21. De Bonrostro Torralba C, Tejero Cabrejas EL, Envid Lázaro BM et al. Low-dose vaginal misoprostol vs vaginal dinoprostone insert for induction of labor beyond 41st week: a randomized trial. Acta Obstet Gynecol Scand 2019; 98 (7): 913–919. doi: 10.1111/aogs.13556.
22. Saeed GA, Fakhar S, Nisar N et al. Misoprostol for term labor induction: a randomized controlled trial. Taiwan J Obstet Gynecol 2011; 50 (1): 15–19. doi: 10.1016/j.tjog.2009.08.001.
23. Weinstein ER, Aaronson J, Abramovitz et al. Patients’ perspectives on pain relief during childbirth and labor epidurals: a pilot qualitative study among women who chose to deliver without neuraxial labor analgesia. Int J Obstet Anesth 2024; 61 : 104294. doi: 10.1016/j.ijoa. 2024.104294.
24. Tan CW, Tan NY, Sultana R et al. Investigating the association factors of acute postpartum pain: a cohort study. BMC Anesthesiol 2023; 23 (1): 252. doi: 10.1186/s12871-023-02214-w.
25. Lowe NK. The nature of labor pain. Am J Obstet Gynecol 2002; 186 (5 Suppl Nature): S16–S24. doi: 10.1067/mob.2002.121427.
ORCID of authors
S. Canan 0000-0002-4995-8194
S. C. Kalkan 0000-0003-1222-5760
S. Özden 0000-0002-3346-7227
H. Uslu Yuvaci 0000-0001-8067-3165
M. S. Bostanci 0000-0002-4776-6244
Submitted/Doručeno: 27. 8. 2025
Accepted/Přijato: 16. 9. 2025
Sultan Canan, MD
Department of Obstetrics and Gynecology
Sakarya Training and Research Hospital
Şirinevler, Adnan Menderes Street
Sağlık Street No. 195
54100 Adapazarı, Sakarya
Turkey
ssultancanan@gmail.com
Štítky
Dětská gynekologie Gynekologie a porodnictví Reprodukční medicínaČlánek vyšel v časopise
Česká gynekologie
2025 Číslo 6
- Těhotenství a porod u ženy s VWD − kazuistika
- Vědecké poznatky rozptylující obavy spojené s používáním nitroděložní antikoncepce i u mladých žen
- Používání intrauterinních tělísek uvolňujících měď a riziko tubární infertility u nuligravidních žen
- Účinnost dlouhodobě působící reverzibilní antikoncepce
- Antikoncepční pilulka přestává být nejpřitažlivější metodou antikoncepce
Nejčtenější v tomto čísle
- HLA-C and KIR interactions as a possible cause of reproductive failures
- The influence of selected immunohistochemical and clinical-pathological markers on the prognosis of patients with malignant uterine tumors
- Negative pressure wound therapy in gynecologic oncology – current knowledge and clinical applications
- Which causes less pain? A comparison of misoprostol and dinoprostone in labor induction
Zvyšte si kvalifikaci online z pohodlí domova
Mazová zátka a její řešení
nový kurzVšechny kurzy