
Léčba relabovaného/ refrakterního difuzního velkobuněčného B lymfomu v perspektivě dat z reálného světa
Treatment of relapsed/refractory diffuse large B-cell lymphoma and the real-world data perspective
Management of relapsed/refractory diffuse large B-cell lymphoma (R/R DLBCL) has undergone significant transformation in recent years. Second line therapy has shifted from conventional salvage regimens toward immunotherapy-based approaches. CAR T-cell therapy is now the preferred option for patients with early relapse or primary refractory disease, while salvage chemoimmunotherapy followed by autologous stem cell transplantation consolidation remains reserved for younger, fit individuals with late relapses. Bispecific antibodies (BiAbs) combined with chemotherapy (i.e., glofitamab plus GemOx) offer effective alternatives for transplant-ineligible patients. Additional novel options include Pola-BR and tafasitamab-lenalidomide, particularly for elderly or frail individuals. In third line and later settings, treatment is increasingly individualized. CAR T-cell therapy remains the preferred modality if not previously administered; otherwise, BiAbs (glofitamab, epcoritamab, odronextamab), antibody-drug conjugates (loncastuximab tesirine, brentuximab vedotin), and lenalidomide-based regimens are considered. Real-world data from the NiHiL registry support the clinical utility of these novel agents and demonstrate improved survival outcomes following their integration into routine clinical practice.
Keywords:
relapse – Diffuse large B-cell lymphoma – therapy – real-world data – refractory
Autoři:
P. Vodička; M. Trněný
Působiště autorů:
First Department of Medicine, First Faculty of Medicine, Charles University and General Hospital, Prague
Vyšlo v časopise:
Transfuze Hematol. dnes,31, 2025, No. 4, p. 305-309.
Kategorie:
Původní práce
doi:
https://doi.org/10.48095/cctahd202528
Souhrn
Management relabovaného/refrakterního difuzního velkobuněčného B-lymfomu (R/R DLBCL) prošel v posledních letech významnou proměnou. Léčba druhé linie se posunula od konvenčních záchranných režimů směrem k přístupům založeným na imunoterapii. Terapie pomocí CAR T-lymfocytů je nyní preferovanou možností u pacientů s časným relapsem nebo primárně refrakterním onemocněním, zatímco záchranná chemoimunoterapie následovaná konsolidací autologní transplantací kmenových buněk zůstává vyhrazena pro mladší, celkově fit jedince s pozdními relapsy. Bispecifické protilátky (BiAbs) v kombinaci s chemoterapií (např. glofitamab plus GemOx) představují účinné alternativy pro pacienty nevhodné k transplantaci. K dalším novým možnostem patří Pola-BR a kombinace tafasitamab-lenalidomid, zejména u starších nebo křehkých pacientů. Ve třetí linii a později je léčba stále více individualizovaná. Terapie CAR T-lymfocyty zůstává preferovanou modalitou, pokud dosud nebyla použita; v opačném případě se zvažují bispecifické protilátky (glofitamab, epcoritamab, odronextamab), protilátko-lékové konjugáty (loncastuximab tesirin, brentuximab vedotin) a režimy založené na lenalidomidu. Reálná data z registru NiHiL podporují klinickou užitečnost těchto nových léků a ukazují na zlepšení přežití po jejich zařazení do běžné klinické praxe.
Klíčová slova:
léčba – relaps – difuzní velkobuněčný B lymfom – data z reálné praxe – refrakterní
INTRODUCTION
Diffuse large B-cell lymphoma (DLBCL) is the most common type of non-Hodgkin lymphoma (NHL), accounting for 30–40% of B-cell NHLs (B-NHLs), with approximately 700 new cases diagnosed annually in the Czech Republic [1]. The incidence of DLBCL rises with age, with the median age at diagnosis in the seventh decade of life. DLBCL is curable, with 60–70% cure rate using the first-line R-CHOP regimen and, more recently, Pola-R-CHP for patients with high-intermediate - or high-risk disease according to the International Prognostic Index (IPI) [2]. However, 30–40% of patients either fail to respond to initial therapy or experience disease progression or relapse, referred to as relapsed/refractory (R/R) DLBCL.
Expanding spectrum of novel therapeutic strategies is now available in the management of R/R DLBCL, particularly T-cell-engaging therapies (CAR T-cell therapy, bispecific antibodies [BiAbs], immunomodulatory agents, checkpoint inhibitors), antibody-drug conjugates (ADC), and other targeted agents [3]. Based on the results of registration trials, these strategies have the potential to improve the historically poor prognosis of R/R DLBCL patients. However, validating these approaches in routine clinical practice requires robust real-world data.
This article reviews current treatment modalities for R/R DLBCL and demonstrates the importance of real-world evidence (RWE) analyses from registry datasets.
SECOND LINE TREATMENT
The standard second-line treatment for R/R DLBCL consisted of salvage chemoimmunotherapy using platinum-containing regimens – cisplatin-based (R-ESHAP, R-DHAP) or carboplatin-based (R-ICE) – combined with the monoclonal antibody rituximab until 2022. During salvage induction therapy, patients typically undergo peripheral blood stem cell collection after prior stimulation with granulocyte colony-stimulating factor (G-CSF). Those who achieve adequate disease control (complete remission [CR] or partial remission [PR]) proceed to high-dose chemotherapy, most commonly the BEAM conditioning regimen, followed by autologous stem cell transplantation (ASCT) using previously harvested, cryopreserved hematopoietic stem cells. Eligibility for this approach is generally limited to fit younger patients (≤65–75 years) without significant comorbidities, representing approximately half of all R/R DLBCL cases. Even among patients initially considered as candidates for ASCT, some patients to achieve a sufficient response to salvage therapy and therefore cannot proceed to ASCT. Furthermore, subsequent relapse remains a concern even after successful ASCT.
CAR T-cell therapy has been approved in the second line setting since 2022, with broader adoption in the Czech Republic since 2023 [4,5]. This immunotherapy is now approved for patients with high-risk DLBCL who fail to achieve complete metabolic remission after first-line treatment, including those with PR, stable disease, primary progression, or relapse within 12 months of completing initial therapy.
Other immunotherapy strategies – including immunomodulatory agents, checkpoint inhibitors, and BiAbs – are also being investigated or incorporated into practice. One promising approach in this context is the combination of the anti-CD20 × anti-CD3 BiAb glofitamab with gemcitabine and oxaliplatin (GemOx). This regimen combines the direct cytotoxic effect of GemOx with the potent T-cell–mediated immune activation induced by glofitamab. In the randomized registration trial, glofitamab + GemOx demonstrated an overall survival (OS) benefit (primary endpoint) in comparison with R-GemOx in heavily pretreated and transplant-ineligible patients, with a manageable safety profile. Although this study raised some important questions, this combination has been approved in EU countries by EMA and offers an option for patients, who are not candidates for CAR T-cell therapy [6].
For similar patient population, other treatment options include conventional chemoimmunotherapy (platinum-, gemcitabine-, or bendamustine-based regimens, including Pola-BR), immunotherapy combinations such as tafasitamab plus lenalidomide or rituximab plus lenalidomide, participation in clinical trials, or best supportive/palliative care.
THIRD-LINE TREATMENT AND BEYOND
For patients who fail the second line therapy, treatment options were historically limited to mostly palliative, consisting of gemcitabine - or bendamustine-based chemotherapy regimens with modest efficacy. In recent years, however, the therapeutic paradigm has undergone a transformation, with the emergence of novel targeted and immune-based therapies offering a realistic possibility of meaningful and durable remissions. Management at this stage is highly individualized and determined by multiple variables, including age, ECOG performance status (PS), comorbidity profile, and prior lines of therapy.
Whenever feasible, enrolment in a prospective clinical trial remains the preferred option, as it offers access to novel investigational agents. For patients who have not received CAR T-cell therapy in earlier lines, are ≤75 years of age (or even older with excellent fitness), and present with adequate ECOG PS, CAR T-cell should be considered the treatment of choice. Currently approved products in this setting – axicabtagene ciloleucel (axi-cel), lisocabtagene maraleucel (liso-cel), and tisagenlecleucel (tisa-cel) – have demonstrated efficacy, with long-term remission in a subset of patients with chemo refractory disease which could be considered as potentially curable [7–9].
Among patients relapsing after CAR T-cell therapy or those ineligible for this approach several options could be considered. BiAbs targeting CD20 and CD3 antigens – such as glofitamab, epcoritamab or odronextamab – represent one option for patients with ECOG PS 0–1, with relatively high chances of achieving response, including complete remission [10–12]. Another alternative is the use of ADC like loncastuximab tesirine or polatuzumab vedotin (the latter in combination with bendamustine and rituximab [Pola-BR]) [13]. Chemoimmunotherapy remains an option for relatively fit patients.
For patients with limited physiological reserves or advanced age, less intensive targeted therapeutic strategies are preferred. These include lenalidomide-based regimens (rituximab + lenalidomide, tafasitamab + lenalidomide) [14].
In the setting of severe frailty, poor ECOG PS, or rapid clinical deterioration, management is generally limited to palliative chemo - or radiotherapy, with the primary objective of symptom control and preservation of quality of life.
THE NIHIL REGISTRY
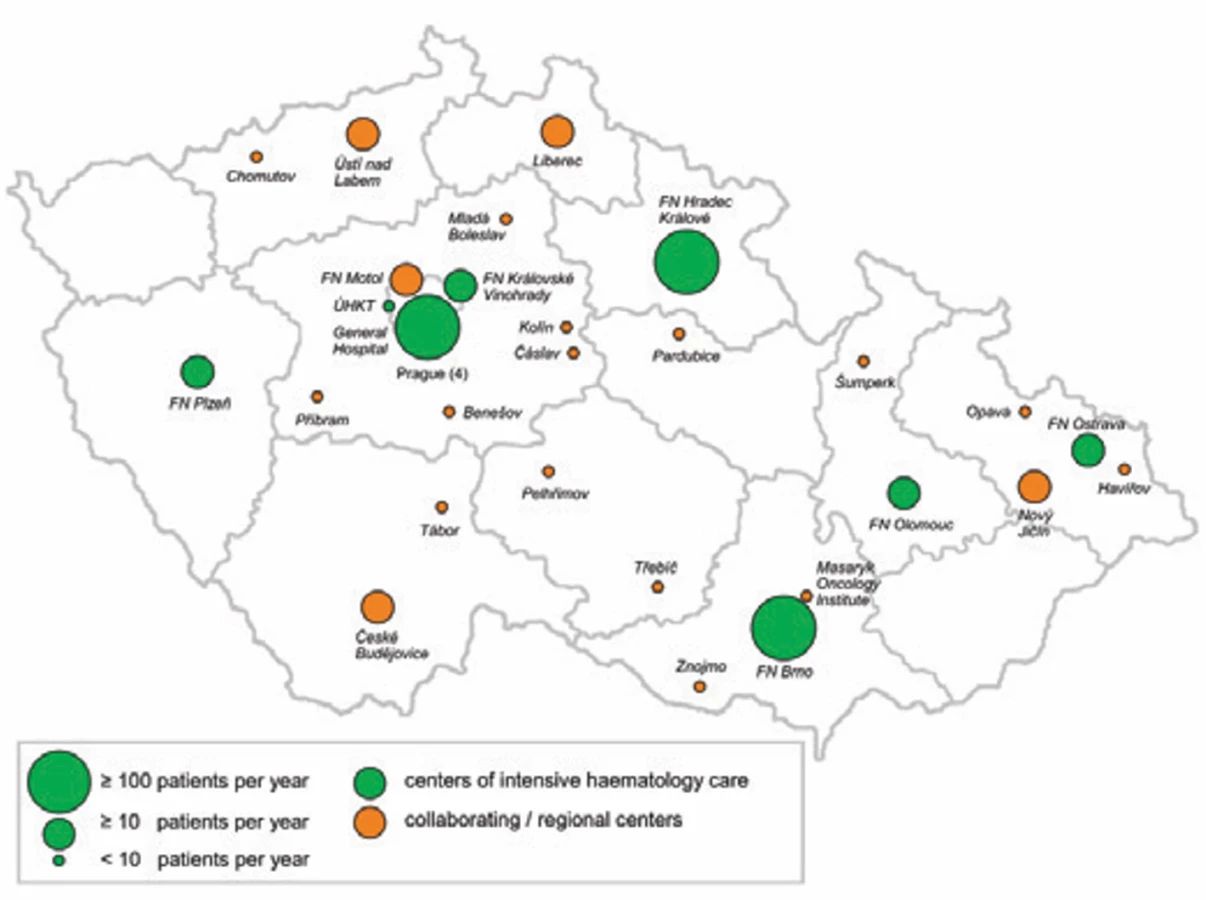
The Czech national non-Hodgkin lymphoma (NHL) registry “NiHiL” (registered in ClinicalTrials.gov under NCT03199 066) was established in 1999 by the Czech Lymphoma Study Group (CLSG) to monitor epidemiological data, treatment modalities, and outcomes of NHL patients in real-world clinical practice. The registry has collected data on 25,454 unique NHL cases from its beginning through mid-2025. Approximately 70% of all NHL patients in the Czech Republic treated at one of the eight university hospital-based intensive centres of intensive haematology care or collaborating regional hospitals have been included in the registry in recent years (Fig. 1). The agreement between the CLSG and each participating hospital, which covered all key aspects of data collection and usage in compliance with GDPR regulations, was signed. The project was approved by the relevant ethics committee.
Patients are enrolled at the time of lymphoma diagnosis after signing informed consent, and their data are recorded in anonymized form. Data are submitted electronically via a secure online system. The following forms are available for each patient: registration form, diagnostic form, treatment form, follow-up form, and other malignancies form. The diagnostic form includes final diagnosis according to the current World Health Organization (WHO) classification system (including a copy of the histopathological report), date of diagnosis, clinical stage, presence of B symptoms, nodal and extranodal involvement, laboratory results, and prognostic scores. This form is used at both initial diagnosis and relapses. The treatment form contains the treatment plan and detailed information on therapy, including chemotherapy regimens, number of cycles, monoclonal antibody therapy, radiotherapy, stem cell transplantation, CAR T-cell therapy, and others. Response assessment is adapted to the current response criteria for lymphomas [15]. The follow-up form is updated at least once a year and includes follow-up status, response to the most recent therapy, date of relapse, and/or death. Data quality is ensured through audits, typically conducted twice a year.
The registry platform has repeatedly been used for data analyses in academic studies, named patient programs, highly innovative treatment regimens (e. g., ibrutinib for mantle cell lymphoma [16], brentuximab vedotin for anaplastic large-cell lymphoma, [17] Pola-BR for R/R DLBCL [18]), as well as for the approval and clinical implementation process of these therapies in routine practice in the Czech Republic. Based on its large patient population, comprehensive dataset, and long-term follow-up, the NiHiL registry is one of the most extensive of its kind in Europe.
However, maintaining the registry for more than 25 years requires addressing several challenges. One is the need to adapt to evolving histopathological classifications – for example, the 5th edition of the WHO classification introduced substantial changes, particularly in defining molecular subtypes of aggressive B-NHL and in grading of follicular lymphoma. Such updates must be implemented in a way that preserves compatibility with earlier classifications, often requiring retrospective review of previously entered data. Another challenge is tracking treatment modalities, especially in light of the rapid development of novel therapies for NHL. To accurately capture data on patients receiving these treatments, the registry must be updated continuously and in near real time.
As diagnostic and therapeutic modalities continue to expand, the volume of collected data will grow accordingly. The registry’s functionality still relies heavily on local data centres at participating institutions. New technologies such as artificial intelligence (e. g., for extracting data from hospital information systems and converting them into structured registry entries) could substantially streamline and accelerate this process in the future. The projects using the NiHiL registry had repeatedly been supported by grants from the Ministry of Health of the Czech Republic.
REAL-WORLD EVIDENCE
While randomized clinical trials remain the gold standard for establishing efficacy and safety of novel therapeutic modalities in R/R DLBCL, their eligibility criteria often exclude a substantial proportion of patients encountered in routine practice [19]. Consequently, RWE is essential to capture the outcomes, tolerability, and treatment patterns in unselected, heterogeneous patient populations in a daily practice.
One example of regimen-specific RWE is the national registry-based analysis of Pola-BR regimen in transplant-ineligible patients with R/R DLBCL. In a cohort of 21 individuals from the NiHiL registry, median OS reached 8.7 months and median progression-free survival (PFS) 3.8 months, with an ORR of 33%. The toxicity profile was consistent with the pivotal GO29365 trial (Pola-BR arm: N = 40, N = 106 in the extension cohort), most commonly including grade 3–4 neutropenia (29%), thrombocytopenia (38%), anaemia (19%), infections (24%), and peripheral neuropathy (5%) [20]. Notably, 19% of patients received Pola-BR as a bridging therapy during CAR T-cell manufacturing, highlighting its utility beyond palliative intent. Although survival outcomes were less favourable than in the trial setting – likely reflecting higher baseline frailty and disease burden – the regimen demonstrated a manageable safety profile and clinically meaningful activity in this population [21].
A further illustration of the growing RWE dataset comes from the compassionate use program of glofitamab in the Czech Republic [22]. Altogether 26 patients with heavily pretreated R/R DLBCL (median of 3 prior lines; range 3–5) were analysed, including 38% with prior CAR T-cell therapy. The median age was 73 years (compared to 66 years in the pivotal trial), CRS occurred in 42% of patients (versus 63%), all grade 1–2, with no neurotoxicity observed [23]. Among 23 evaluable patients, the ORR was 52%, with 30% achieving CR (compared to 52% ORR and 37% CR in the pivotal trial). However, post-CAR T-cell failure responses were limited, with only 2/8 patients achieving PR. Median PFS was 3 months and median OS 11 months. Lack of treatment response was the dominant adverse prognostic factor for both PFS (P < 0.01) and OS (P = 0.01). Outcomes were better in patients with only three prior lines compared to those with ≥ 4 lines of therapy, supporting an earlier integration of glofitamab in the treatment strategies.
Beyond individual regimens, population-level registry data can reveal how the introduction of innovative modalities transforms therapeutic outcomes over time. In a recent NiHiL registry analysis of 312 patients receiving third-line therapy, outcomes were compared across two eras defined by CAR T-cell availability: Era 1 (2018–2020, prior to the broad adoption of CAR T-cell) and Era 2 (2021–2023). The incorporation of CAR T cells, BiAbs, and ADC was associated with significant improvements in survival: 2-year OS increased from 29% to 43% (P = 0.01) and 2-year event-free survival from 13% to 24% (P = 0.01). Response rates also increased significantly, with ORR improving from 30% to 46% (P = 0.01) and CR rates from 18% to 30% (P = 0.02). Treatment patterns shifted accordingly, with CAR T-cell use rising from 6% to 32% and novel agent use from 13% to 22% (P < 0.01). These findings demonstrate that the rapid adoption of novel agents into routine practice can yield population-level survival benefits within just a few years.
Taken together, these RWE analyses underscore two key messages: first, that real-world outcomes, while sometimes more modest than those reported in trials, confirm the clinical utility and manageable safety profiles of novel agents such as Pola-BR and glofitamab; and second, that the incorporation of these and other innovative modalities into R/R DLBCL management is already yielding measurable survival benefits at the population level. Continued prospective registry analyses will be essential to refine patient selection, optimize sequencing strategies, and maximize the impact of these therapies in daily practice.
CONCLUSION
DLBCL has evolved from a uniformly fatal malignancy in the first half of the 20th century to a disease that is curable in a substantial proportion of patients First‑line therapy evolved from CHOP to R‑CHOP and, more recently, Pola‑R‑CHP (IPI 3–5), while ASCT became an established consolidation strategy in R/R disease.
Therapeutic innovation has been particularly pronounced in R/R DLBCL. Immunotherapeutic approaches, notably CAR T-cell therapy, BiAbs, and ADC, have emerged as key treatment modalities and are now being shifted into earlier treatment lines. Optimal sequencing and integration of these therapies within existing treatment algorithms remain the subject of ongoing clinical investigation.
Until recently, DLBCL therapy has been predominantly “molecularly agnostic”, applicable across all subtypes. Recent studies have begun to explore targeted therapies for biologically defined subgroups characterized by recurrent genetic alterations, but broader implementation of such precision approaches is currently constrained by the cost and turnaround time of molecular profiling. Nevertheless, the adoption of personalized treatment strategies is promising for improving outcomes, particularly for patients with high-risk R/R DLBCL.
Zdroje
1. Krejči D, Pehalová LA, Talábová A, et al. Současné epidemiologické trendy novotvarů v České Republice. ÚZIS Novotvary. 2018 (227): 345.
2. Tilly H, Morschhauser F, Sehn LH, et al. Polatuzumab vedotin in previously untreated diffuse large B-cell lymphoma. N Engl J Med. 2022; 386 (4): 351–363.
3. Thieblemont C, Gomes Da Silva M, Leppä S, et al. Large B-cell lymphoma (LBCL): EHA Clinical Practice Guidelines for diagnosis, treatment, and follow-up. Hemasphere. 2025; 9 (9): e70207.
4. Locke FL, Miklos DB, Jacobson CA, et al. Axicabtagene ciloleucel as second-line therapy for large B-cell lymphoma. N Engl J Med. 2022; 386 (7): 640–654.
5. Kamdar M, Solomon SR, Arnason J, et al. Lisocabtagene maraleucel versus standard of care with salvage chemotherapy followed by autologous stem cell transplantation as second-line treatment in patients with relapsed or refractory large B-cell lymphoma (TRANSFORM): results from an interim analysis of an open-label, randomised, phase 3 trial. Lancet. 2022; 399 (10343): 2294–2308.
6. Abramson JS, Ku M, Hertzberg M, et al. Glofitamab plus gemcitabine and oxaliplatin (GemOx) versus rituximab-GemOx for relapsed or refractory diffuse large B-cell lymphoma (STARGLO): a global phase 3, randomised, open-label trial. Lancet. 2024; 404 (10466): 1940–1954.
7. Abramson JS, Palomba ML, Gordon LI, et al. Lisocabtagene maraleucel for patients with relapsed or refractory large B-cell lymphomas (TRANSCEND NHL 001): a multicentre seamless design study. Lancet. 2020; 396 (10254): 839–852.
8. Schuster SJ, Bishop MR, Tam CS, et al. Tisagenlecleucel in adult relapsed or refractory diffuse large B-cell lymphoma. N Engl J Med. 2019; 380 (1): 45–56.
9. Locke FL, Ghobadi A, Jacobson CA, et al. Long-term safety and activity of axicabtagene ciloleucel in refractory large B-cell lymphoma (ZUMA-1): a single-arm, multicentre, phase 1-2 trial. Lancet Oncol. 2019; 20 (1): 31–42.
10. Hutchings M, Morschhauser F, Iacoboni G, et al. Glofitamab, a novel, bivalent CD20-targeting T-cell-engaging bispecific antibody, induces durable complete remissions in relapsed or refractory B-cell lymphoma: a phase I trial. J Clin Oncol. 2021; 39 (18): 1959–1970.
11. Thieblemont C, Phillips T, Ghesquieres H, et al. Epcoritamab, a novel, subcutaneous CD3xCD20 bispecific T-cell-engaging antibody, in relapsed or refractory large B-cell lymphoma: dose expansion in a phase I/II trial. J Clin Oncol. 2023; 41 (12): 2238–2247.
12. Ayyappan S, Kim WS, Kim TM, et al. Final analysis of the phase 2 ELM-2 study: odronextamab in patients with relapsed/refractory (R/R) diffuse large B-cell lymphoma (DLBCL). Blood. 2023; 142 (Suppl 1): 436–436.
13. Sehn LH, Herrera AF, Flowers CR, et al. Polatuzumab vedotin in relapsed or refractory diffuse large B-cell lymphoma. J Clin Oncol. 2020; 38 (2): 155–165.
14. Salles G, Duell J, Gonzalez Barca E, et al. Tafasitamab plus lenalidomide in relapsed or refractory diffuse large B-cell lymphoma (L-MIND): a multicentre, prospective, single-arm, phase 2 study. Lancet Oncol. 2020; 21 (7): 978–988.
15. Cheson BD, Fisher RI, Barrington SF, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: The Lugano Classification. J Clin Oncol. 2014; 32 (27): 3059–3067.
16. Obr A, Benesova K, Janikova A, et al. Ibrutinib in mantle cell lymphoma: a real-world retrospective multi-center analysis of 77 patients treated in the Czech Republic. Ann Hematol. 2023; 102 (1): 107–115.
17. Klanova M, Sykorova A, Janikova A, et al. Brenduximab vedotin in combination with chemotherapy in patients with newly diagnosed CD30-positive peripheral T-cell lymphomas: real-world data. Hematol Oncol. 2023; 41 (S2): 763–764.
18. Vodicka P, Benesova K, Janikova A, et al. Polatuzumab vedotin plus bendamustine and rituximab in patients with relapsed/refractory diffuse large B-cell lymphoma in the real world. Eur J Haematol. 2022; 109 (2): 162–165.
19. Vodicka P, Janikova A, Belada D, et al. Do the control cohorts of phase III randomized trials reflect the real-world results of DLBCL patients? Blood. 2023; 142 (Suppl 1): 4485–4485.
20. Sehn LH, Hertzberg M, Opat S, et al. Polatuzumab vedotin plus bendamustine and rituximab in relapsed/refractory DLBCL: survival update and new extension cohort data. Blood Adv. 2022; 6 (2): 533–543.
21. Vodicka P, Benesova K, Janikova A, et al. Polatuzumab vedotin plus bendamustine and rituximab in patients with relapsed/refractory diffuse large B-cell lymphoma in the real world. Eur J Haematol. 2022; 109 (2): 162–165.
22. Belada D, Mociková H, Obr A, et al. Safety and efficacy of glofitamab in relapsed/refractory diffuse large B-cell lymphoma – data from real-world study. Hematol Oncol. 2025; 43 (S3): e647_70096.
23. Dickinson MJ, Carlo-Stella C, Morschhauser F, et al. Glofitamab for relapsed or refractory diffuse large B-cell lymphoma. N Engl J Med. 2022; 387 (24): 2220–2231.
AUTHOR CONTRIBUTION
PV – preparation of the first draft and final version of the manuscript
MT – critical revision of the manuscript
CONFLICT OF INTEREST STATEMENT
The authors declare no conflict of interest in connection with the topic, preparation and publication of this study. Preparation of the manuscript was not initiated or supported by any pharmaceutical company.
Declaration on the use of AI
Use of Artificial Intelligence in preparation of the manuscript – used for grammar correction.
Štítky
Hematologie a transfuzní lékařství Interní lékařství OnkologieČlánek vyšel v časopise
Transfuze a hematologie dnes

2025 Číslo 4
- Srovnání vlivu omeprazolu a pantoprazolu na antiagregační účinek klopidogrelu
- Současné postavení a přínos sartanů v klinické praxi
- Prognostický význam hladiny natriuretických peptidů při léčbě empagliflozinem
- Hypertrofická obstrukční kardiomyopatie ve světle moderní farmakoterapie – kazuistika
- Management hypertenze v těhotenství
Nejčtenější v tomto čísle
- Doporučení pro diagnostiku a léčbu nežádoucích účinků po terapii CD19 CAR-T lymfocyty u dospělých pacientů s lymfomy a akutní lymfoblastickou leukémií – konsenzus expertů certifikovaných center v ČR a SR pro rok 2025
- Léčba lymfomů CAR-T lymfocyty
- Generační změna terapie klasického Hodgkinova lymfomu
- Folikulární lymfom – proměna léčebného paradigmatu směrem k chemo-free přístupům
Zvyšte si kvalifikaci online z pohodlí domova
Mazová zátka a její řešení
nový kurzVšechny kurzy