
Harnessing Health IT for Improved Cardiovascular Risk Management
article has not abstract
Published in the journal:
. PLoS Med 7(8): e32767. doi:10.1371/journal.pmed.1000313
Category:
Essay
doi:
https://doi.org/10.1371/journal.pmed.1000313
Summary
article has not abstract
Summary Points
-
Cardiovascular disease (CVD) risk management through drug, dietary, and other interventions can significantly prevent or delay CVD events.
-
Despite evidence for effectiveness, large gaps have been demonstrated between what is known and what is actually done in health care.
-
Information technology (IT) has the potential to support clinicians to close these gaps throughout processes of care delivery.
-
IT can be used to support identification of at-risk individuals, CVD risk assessment and management, care planning, patient self-management, and evaluation of improvements in care and health outcomes.
-
To achieve the potential of IT-based programmes requires a supportive social and political environment, substantial organisational changes, and active patient and clinician engagement.
Cardiovascular disease (CVD) is one of the leading causes of death and disability worldwide, accounting for 16.7 million (29.2%) of total global deaths, 80% of them taking place in low - or middle-income countries [1]. While death is inevitable, premature death and loss of productive years of life from CVD is, for the most part, preventable. Much can be achieved by population-wide interventions that seek to lower cigarette and salt consumption, obesity prevalence, and blood cholesterol levels in the entire population [2]. At a personal health level, there is an abundance of evidence that reducing modifiable CVD risk factors (smoking, lipid fractions, blood pressure, diabetes) through drug, dietary, and other interventions can prevent or delay CVD events. Almost all adults could achieve a 50%–80% relative reduction in CVD risk if they took a combination of a lipid-lowering drug, a blood pressure lowering drug, and aspirin [3]. The higher the pre-treatment CVD risk, the greater the absolute benefit and therefore the greater the cost-effectiveness of treatment [4]. Therefore, many national guidelines now advocate identifying those at high risk of a future CVD event in the short-term and tailoring the intensity of management for individuals according to their baseline CVD risk.
Is CVD Risk Reduction Happening in Practice?
Large gaps have been demonstrated between what is known to be effective and what is actually done in health care [5],[6]. Studies have shown that a formal CVD risk assessment to systematically identify high-risk patients is rarely conducted [7],[8], and audits of care indicate substantial under-use of effective CVD interventions by clinicians [9]–[12].
The reasons why clinicians do not follow patient management guidelines have been explored in some depth [13]–[15] and reflect a complex interplay of organisational, health system, provider, and patient factors. Barriers include lack of time, heavy workload and other competing demands, a lack of teamwork and organisation in the practice, paperwork, bureaucracy, and a lack of support to conduct preventive care [13]–[15]. Guidelines have been criticised for being too complex and focused on single diseases, whereas patients present with multiple problems. Even if clinicians have the ability, time, and resources to act on the evidence, for management to be effective the patient needs to understand and agree with the approach, be motivated to make changes, and be willing and able to adhere to a management plan.
Can Technological Innovation Help to Close the CVD Evidence-Practice Gap?
There is growing interest in the potential of information technology (IT) to reduce human error and variation in patient care. A recent systematic review has investigated the impact of a wide range of health IT [16]. Three major benefits were found for quality of care (particularly in association with preventive care):
-
increased adherence to guideline-based care;
-
enhanced surveillance and monitoring; and
-
decreased medication errors.
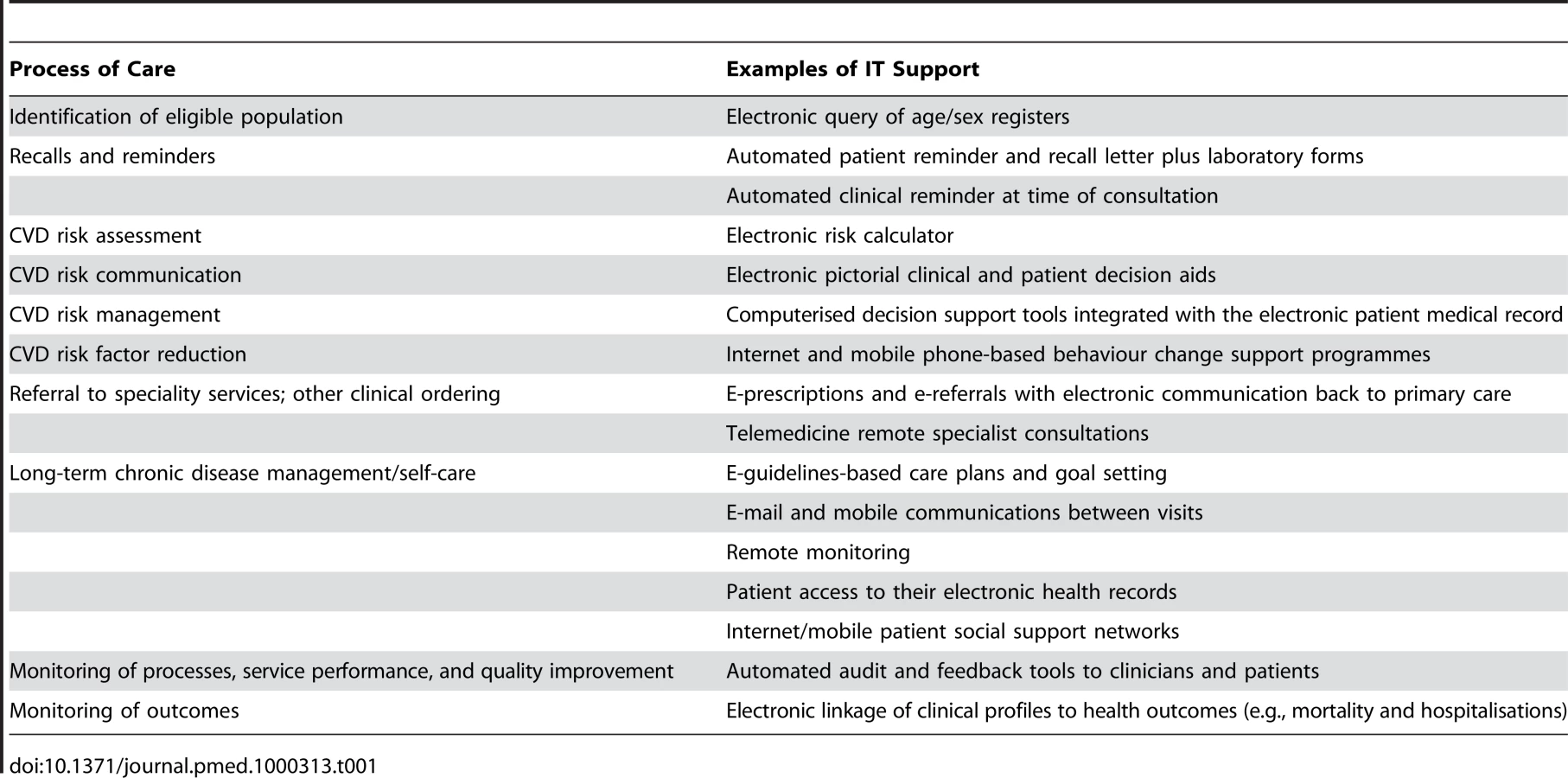
Table 1 shows where health IT could be used to support the process of CVD risk assessment and management in primary care practices. The focus is on tailoring interventions to specific patients based on recorded data and thus providing personalised prevention.
Most of these technologies are predicated on
-
the presence of an electronic medical record (EMR, defined as computer-based clinical data of an individual that are location-specific and kept by a single practice or office, health centre, or ambulatory clinic [17]); and
-
the ability to register patients, query the database to identify patients of interest, and contact them.
Electronic queries to identify those eligible for CVD risk assessment and utilisation of simple rules-based automated reminder and recall systems have been increasingly used internationally since the late 1970s. Electronic calculators for estimates of CVD risk have been available since the early 1990s. However, only recently have more patient - and clinician-friendly CVD risk communication tools been developed (see Box 1 for an example).
Box 1. Example of CVD Risk Communication Tool Currently Being Used in New Zealand
Your Heart Forecast, a tool that graphically depicts absolute, relative, and long-term measures of CVD risk as well as a more accessible metric, your “cardiovascular age” or “heart age”. It also shows the benefit of risk factor reduction (http://www.yourheart.forecast.org.nz/) [35].
Computerised decision support systems (CDSSs) can rapidly and automatically convert the recommendations from evidence-based syntheses into guidance for clinicians, tailored for an individual patient's profile. Systematic reviews have found moderate evidence of CDSS effectiveness with respect to provider processes and performance, but the effects on patient outcomes are understudied and, where research has been conducted, inconsistent [18]–[20].
E-prescribing and e-referrals are becoming widespread in countries with a high degree of practice computerisation and Internet connectivity. The challenge is to add value to this system via more extensive two-way sharing of information. This could include notification of filled prescriptions and alerts in the practice system for un-filled prescriptions; notification of changes to care plans and medications by other providers; and missed appointments at other health services.
CDSSs can also form the basis of shared goal setting and the development of care plans for risk reduction. Instant electronic access and registration into self-management programmes removes barriers, such as having to attend another session, uses the “teachable moment” (i.e., being informed one is at high risk of an acute cardiac event) to enhance motivation, and can involve the primary care provider to motivate and tailor appropriately to the individual's risk profile. Internet-based programmes to support self-management and healthy behaviour change are proliferating. While there is limited evidence for effectiveness of IT-based self-management programmes, smoking cessation is one area that has been rigorously trialled. A recent meta-analysis of 22 randomised controlled trials found “… sufficient clinical evidence to support the use of Web - and computer-based smoking cessation programs for adult smokers” (RR 1.44, 90% confidence interval 1.27–1.64) [21]. Social networking Web sites are also being used formally and informally for such support. Patientslikeme.com is just one example of harnessing social networking to provide peer support for patients with the same conditions [22]. However, the social networking phenomenon does not easily lend itself to rigorous research of effectiveness.
Electronic patient portals or patient access to electronic health records can further empower patients to manage their disease and become active participants in their own health outcomes. However, there is limited research published on the effectiveness of these tools with respect to health outcomes, particularly for CVD.
Telehealth interventions include any telecommunications between a provider and patient between clinic visits, such as via phone, Internet, videoconference communication, and text messaging. A systematic review of telehealth interventions for the secondary prevention of coronary disease found significant differences in smoking, lipid levels, and systolic blood pressure in patients taking part in such interventions [23]. Mobile phones are likely to play an important role here in the future, allowing behaviour change support to be proactively sent directly to people wherever they are in formats from simple SMS/text messages to multimedia video messages. Such programmes can be tailored and personalised, and yet are eminently scalable to large diverse populations (see Box 2 for an example). Two recent systematic reviews of health care delivered via mobile phone found 26 studies in smoking cessation, diabetes care, physical activity, stress management, hypertension, and other conditions [24],[25]. These reviews reported significant behaviour change, with clinical and process improvements in the majority of studies.
Box 2. Example of a Mobile Phone Programme Being Used in New Zealand and the United Kingdom
Txt2quit is a free national text messaging smoking cessation programme in New Zealand that people can join by phone or online (http://www.quit.org.nz/txt2quit). It was implemented following a large randomised controlled trial which showed a doubling of short-term quit rates [36]. A similar study of this intervention, called txt2stop, is now being conducted in the UK.
Telemedicine has also taken the form of live remote specialist consultation (for patients in geographically isolated areas), or the transmission of diagnostic images/video/data for review by specialists. This also includes remote monitoring at home by devices that transmit data (e.g., ECG, blood pressure, weight, blood glucose) to a health care provider for interpretation and alterations to care. Home-based telemonitoring using Internet and mobile phone technology has been demonstrated to reduce hospital admissions for those with congestive heart failure and, if admitted, to reduce the length of stay [26],[27].
Finally, IT support is vital for monitoring processes and outcomes for clinical audit and research with pay-for-performance programmes such as the United Kingdom quality and outcomes framework based on the necessity of an “IT spine”. Health IT records are increasingly being used for CVD research, for example, to generate large risk prediction cohorts [28],[29].
What Is Needed to Implement a Systematic Technology-Based Approach for CVD?
The benefits of implementing a systematic health IT approach could include improvements in the quality of care, reduced duplication, improving access to services in areas of growing demand and limited resources, and improved monitoring and evaluation. However, while some health IT systems implementations succeed, the majority are likely to fail [30]. The greater the personal and organisational change required by a system, the greater the risk of failure. Adverse effects of health IT implementation can include increased time for direct and indirect patient care [31], the loss of privacy and confidentiality, and possible changes to the doctor–patient relationship [32]. The time commitment involved with learning and implementing new systems may be substantial. The set-up costs of computerisation and implementation of health IT can be large and require ongoing investment. Furthermore, IT is a rapidly evolving science. By the time a large-scale project is completed, technology has often moved on [33].
Key elements that facilitate the development of a systematic technology-based approach are the availability of high quality national or international CVD guidelines, and local health IT specialists with the ability to develop reliable systems and the willingness and resources to maintain, sustain, and continue to innovate in response to consumer, clinician, and local health service needs. At a national level, policies that support prevention of CVD and long-term condition management need to be aligned with national IT policies that support the development of unified informatics standards for collecting health data, coding, messaging, and network infrastructure. While privacy and confidentiality concerns remain, there is a need for mature privacy statutes and ensuring consumers are aware of the potential uses of their health data.
Without clinical and health service buy-in, no IT solution will be successful. The solutions need to be effective, user-friendly, and integrated with all other systems, and ultimately must be efficient in terms of person-time. Berg describes this as a “… process of mutual transformation …” involving organisational change and allowing for change in the IT strategy arising out of the process of implementation [34].
In summary, CVD management requires partnerships between providers and patients, between staff within an institution, between service providers in the primary care setting, and between primary, secondary, and tertiary care services. For IT to achieve the potential to close the gap between evidence and practice and translate into positive patient outcomes there needs to be teamwork and a change in the way clinicians and services work together. This is particularly important for long-term health conditions such as CVD, where there is often unbounded need in the face of limited resources.
Zdroje
1. World Health Organisation 2003 The world health report 2003 - shaping the future Geneva World Health Organisation
2. MurrayCJL
LauerJA
HutubessyRCW
NiessenL
TomijimaN
2003 Effectiveness and costs of interventions to lower systolic blood pressure and cholesterol: a global and regional analysis on reduction of cardiovascular-disease risk. Lancet 361 717 725
3. WaldNJ
LawMR
2003 A strategy to reduce cardiovascular disease by more than 80%. BMJ 326 1419
4. JacksonR
LawesCMM
BennettDA
MilneRJ
RodgersA
2005 Treatment with drugs to lower blood pressure and blood cholesterol based on an individual's absolute cardiovascular risk. Lancet 365 434 441
5. McGlynnEA
AschSM
AdamsJ
KeeseyJ
HicksJ
2003 The quality of health care delivered to adults in the United States. New Eng J Med 348 2635 2645
6. WoolfSH
JohnsonRE
2005 The break-even point: when medical advances are less important than improving the fidelity with which they are delivered. Ann Fam Med 3 545 552
7. MontgomeryAA
FaheyT
PetersTJ
MacIntoshC
SharpDJ
2000 Evaluation of computer based clinical decision support system and risk chart for management of hypertension in primary care: randomised controlled trial. BMJ 320 686 690
8. WellsS
FurnessS
RafterN
HornE
WhittakerR
2008 Integrated electronic decision support increases cardiovascular disease risk assessment four fold in routine primary care practice. Eur J Cardiovasc Prev Rehabil 15 173 178
9. KallioV
HamalainenH
HakkilaJ
LuurilaO
1979 Reduction in sudden deaths by a multifactorial intervention programme after acute myocardial infarction. Lancet 2 1091 1094
10. KotsevaK
WoodD
De BackerG
De BacquerD
PyoralaK
2009 EUROASPIRE III: a survey on the lifestyle, risk factors and use of cardioprotective drug therapies in coronary patients from 22 European countries. Eur J Cardiovasc Prev Rehabil 16 121 137
11. KotsevaK
WoodD
De BackerG
De BacquerD
PyoralaK
2009 Cardiovascular prevention guidelines in daily practice: a comparison of EUROASPIRE I, II, and III surveys in eight European countries. Lancet 373 929 940
12. WebsterRJ
HeeleyEL
PeirisDP
BayramC
CassA
2009 Gaps in cardiovascular disease risk management in Australian general practice. Med J Aust 191 324 329
13. BazianL
2005 Do evidence-based guidelines improve the quality of care? Evidence-Based Healthcare and Public Health 9 270 275
14. CabanaMD
RandCS
PoweNR
WuAW
WilsonMH
1999 Why don't physicians follow clinical practice guidelines? A framework for improvement. JAMA 282 1458 1465
15. GrolR
GrimshawJ
2003 From best evidence to best practice: effective implementation of change in patients' care. Lancet 362 1225 1230
16. ChaudhryB
WangJ
WuS
MaglioneM
MojicaW
2006 Systematic review: impact of health information technology on quality, efficiency, and costs of medical care. Ann Intern Med 144 742 752
17. ProttiD
2007 Comparison of information technology in general practice in 10 countries. Healthcare Q 10 107 116
18. GargAX
AdhikariNKJ
McDonaldH
Rosas-ArellanoMP
DevereauxPJ
2005 Effects of computerized clinical decision support systems on practitioner performance and patient outcomes: a systematic review. JAMA 293 1223 1238
19. ShojaniaKG
JenningsA
MayhewA
RamsayCR
EcclesMP
2009 The effects of on-screen, point of care computer reminders on processes and outcomes of care. Cochrane Database Syst Rev (3) CD001096
20. SintchenkoV
MagrabiF
TipperS
2007 Are we measuring the right end-points? Variables that affect the impact of computerised decision support on patient outcomes: a systematic review. Med Inform Internet Med 32 225 240
21. MyungS-K
McDonnellDD
KazinetsG
SeoHG
MoskowitzJM
2009 Effects of Web - and computer-based smoking cessation programs: meta-analysis of randomized controlled trials. Arch Intern Med 169 929 937
22. FrostJH
MassagliMP
2008 Social uses of personal health information within PatientsLikeMe, an online patient community: what can happen when patients have access to one another's data. J Med Internet Res 10 e15
23. NeubeckL
RedfernJ
FernandezR
BriffaT
BaumanA
2009 Telehealth interventions for the secondary prevention of coronary heart disease: a systematic review. Eur J Cardiovasc Prev Rehabil 16 281 289
24. KrishnaS
BorenSA
BalasEA
2009 Healthcare via cell phones: a systematic review. Telemed J E Health 15 231 240
25. WhittakerR
BorlandR
BullenC
LinRB
McRobbieH
2009 Mobile phone-based interventions for smoking cessation. Cochrane Database Syst Rev (4) CD006611
26. GiordanoA
ScalviniS
ZanelliE
CorraU
LongobardiGL
2009 Multicenter randomised trial on home-based telemanagement to prevent hospital readmission of patients with chronic heart failure. Int J Cardiol 131 192 199
27. ScherrD
KastnerP
KollmannA
HallasA
AuerJ
2009 Effect of home-based telemonitoring using mobile phone technology on the outcome of heart failure patients after an episode of acute decompensation: randomized controlled trial. J Med Internet Res 11 e34
28. Hippisley-CoxJ
CouplandC
VinogradovaY
RobsonJ
MayM
2007 Derivation and validation of QRISK, a new cardiovascular disease risk score for the United Kingdom: prospective open cohort study. BMJ 335 136
29. WellsS
2008 Getting Evidence to and from general practice consultations for cardiovascular risk management using computerised decision support [PhD thesis] Auckland University of Auckland
30. HeeksR
2006 Health information systems: failure, success and improvisation. Int J Med Inform 75 125 137
31. EslamiS
Abu-HannaA
de KeizerNF
2007 Evaluation of outpatient computerized physician medication order entry systems: A systematic review. J Am Med Inform Assoc 14 400 406
32. MitchellE
SullivanF
2005 A descriptive feast but an evaluative famine: systematic review of published articles on primary care computing during 1980–97. BMJ 322 279 282
33. MeigsJB
CagleiroE
DubeyA
Murphy-SheehyP
GildesgameC
2003 A controlled trial of web-based diabetes disease management: the MGH Diabetes Primary Care Improvement Project. Diabetes Care 26 750 757
34. BergM
2001 Implementing information systems in health care organizations: myths and challenges. Int J Med Inform 64 143 156
35. WellsS
KerrA
EadieS
WiltshireC
JacksonR
2010 ‘Your Heart Forecast’: a new approach for describing and communicating cardiovascular risk? Heart 96 708 13
36. RodgersA
CorbettT
BramleyD
RiddellT
WillsM
2005 Do u smoke after txt? Results of a randomised trial of smoking cessation using mobile phone text messaging. Tob Control 14 255 261
Štítky
Interní lékařstvíČlánek vyšel v časopise
PLOS Medicine
2010 Číslo 8
- Diosmin a hesperidin: Co ukazuje farmakokinetika?
- Neuropatie výrazně zpomaluje proces hojení u povrchových ran
- Diagnostika osteoporózy v kontextu současných doporučení
- Rána vizitkou (nejen) chirurga
- Patogeneze vzniku keloidní jizvy
Nejčtenější v tomto čísle
- Using Touchscreen Electronic Medical Record Systems to Support and Monitor National Scale-Up of Antiretroviral Therapy in Malawi
- Physical Activity Attenuates the Genetic Predisposition to Obesity in 20,000 Men and Women from EPIC-Norfolk Prospective Population Study
- Challenges in Developing Evidence-Based Recommendations Using the GRADE Approach: The Case of Mental, Neurological, and Substance Use Disorders
- Reducing Malaria Transmission in Africa: A Model-Based Evaluation of Intervention Strategies
Zvyšte si kvalifikaci online z pohodlí domova
Mazová zátka a její řešení
nový kurzVšechny kurzy