
Long-term inpatient disease burden in the Adult Life after Childhood Cancer in Scandinavia (ALiCCS) study: A cohort study of 21,297 childhood cancer survivors
In this population-based cohort study in Denmark, Finland, Iceland, and Sweden, Sofie de Fine Licht and colleagues present the increased long-term burden of disease serious enough to require hospitalization in survivors of childhood cancer.
Published in the journal:
. PLoS Med 14(5): e32767. doi:10.1371/journal.pmed.1002296
Category:
Research Article
doi:
https://doi.org/10.1371/journal.pmed.1002296
Summary
In this population-based cohort study in Denmark, Finland, Iceland, and Sweden, Sofie de Fine Licht and colleagues present the increased long-term burden of disease serious enough to require hospitalization in survivors of childhood cancer.
Introduction
The number of childhood cancer survivors is increasing steadily in many parts of the world because of the extraordinary improvement in survival rates during the past five decades [1]. In the Nordic countries, four of five childhood cancer patients can expect to be long-term survivors [2]. These major improvements in survival come, however, at a price. Because of intense exposure to radiation and highly toxic compounds during treatment, a high proportion of survivors of childhood cancer now face somatic, mental, and cognitive late effects, many of which become clinically apparent even decades after the cancer was cured [3–7]. Only a limited number of studies have investigated the hospitalisation pattern subsequent to treatment for cancer diagnosed during childhood, adolescence, and young adulthood [8–13]. They all revealed an overall increased risk for hospitalisation. However, the record linkage studies with diagnostic inpatient information [9,10,12,13] were limited by study size and unable to give reliable risk estimates for rare types of childhood cancer or combinations of types of childhood cancer and types of subsequent disease. The larger studies were either based on self-reported information on causes for hospitalisation [7] or questionnaire data from patients’ primary health care physicians [10], with a relatively large proportion of survivors lost to follow-up.
In a population-based cohort study with virtually no loss to follow-up and exclusive use of medically verified diagnostic information from individual inpatient records, we studied the full range of somatic morbid conditions requiring hospitalisation in 21,297 5-year survivors of childhood cancer diagnosed between 1943–2008. As this is the largest long-term follow-up study of inpatient care among childhood cancer survivors conducted so far, it allowed stratifications and detailed analyses that were not possible in previous studies and provides novel information on diseases that first become symptomatic in middle age or senescence. Thus, the primary aim of our study was to present a comprehensive yet detailed overview of the long-term frequency and distribution of somatic diseases serious enough to require hospitalisations in survivors of childhood cancer combined and by type of cancer.
Methods
Cancer survivor and comparison cohorts
This retrospective, register-based cohort study is part of the collaborative study Adult Life after Childhood Cancer in Scandinavia (ALiCCS) (www.aliccs.org) [14]. The ALiCCS study was approved by the national bioethics committee, the data protection authority, or the national institute for health and welfare in the respective countries (Denmark: 2010-41-4334; Finland: THL/520/5.05.00/2016; Iceland: VSN 10–041; and Sweden: Ö 10–2010, 2011/19). Consent from study participants was not required as all data were available in national health registers.
The basic childhood cancer cohort in the present analysis is a subcohort of the Nordic ALiCCS material, comprising 33,576 individuals with cancer diagnosed in Denmark, Finland, Iceland, or Sweden in people under the age of 20 years in the periods 1943–2008 in Denmark, 1971–2008 in Finland, 1955–2008 in Iceland, and 1958–2008 in Sweden (Fig 1) [15–18]. Patients from Norway were not included, as complete hospitalisation histories with all diseases included in the present study were not available. From the cancer registries, we obtained each patient’s personal identification number, date of diagnosis, and type of cancer and assigned patients to the 12 main diagnostic groups of the International Classification Scheme for Childhood Cancer, with lymphoma divided further into Hodgkin, non-Hodgkin lymphoma, and other lymphomas [19]. For each childhood cancer patient, we randomly selected five comparison individuals from the national population registers who were alive on the date of the cancer diagnosis of the corresponding patient; of the same sex, age, and country; and without a cancer diagnosis before the age of 20 years. Fewer than five comparison individuals were available for 157 patients, leaving 167,712 participants for study. For both patients and comparison individuals, we obtained information from the population registers on vital status and emigration during follow-up.

Before linkage of study participants to the respective national hospital registers, we excluded those in whom more than one cancer was diagnosed during childhood, those who had died or emigrated before the start of the national hospital registers (Sweden, stepwise inclusion of counties in 1964–1987 and nationwide since 1987; Finland, 1975; Denmark, 1977; Iceland, 1999), and those who had died or emigrated within 5 years of the date of cancer diagnosis or an equivalent time lag for the population comparisons. These exclusions resulted in cohorts of 21,518 5-year childhood cancer survivors and 152,481 population comparison individuals (Fig 1).
Hospital admissions
The nationwide hospital registries hold information on all nonpsychiatric hospital admissions in the four countries [20,21]. Registration is mandatory, and the treating physician submits diagnostic information electronically. Each admission to a hospital initiates a record, which includes the personal identification number of the patient, the dates of admission and discharge, a primary discharge diagnosis, and supplementary diagnoses coded according to the International Classification of Diseases 7th–10th revisions (ICD-7–ICD-10).
Data on cancer survivors and comparison individuals were linked to the hospital registers, and a full hospital history with discharge diagnoses was established for each person with a previous hospital contact. We excluded cancer survivors and comparison individuals who had ever been hospitalised with a congenital malformation or chromosome abnormality (ICD-8 codes 740–759, ICD-10 codes Q00–Q99), as this could possibly confound the associations between childhood cancer and several of the outcomes, leaving 21,297 5-year survivors of childhood cancer and 152,231 population comparison individuals for the risk analysis (Fig 1).
To quantify the inpatient disease burden among study participants comprehensibly, we grouped the hospital discharge diagnoses into 120 disease categories or diagnoses, which in turn were assembled into 12 main diagnostic groups (S1 Table). The 12 main diagnostic groups were mutually exclusive; all neoplasms were grouped in the two main diagnostic groups of malignant neoplasms and benign neoplasms. Diagnoses coded according to ICD-7, ICD-9, and ICD-10 were adapted to ICD-8 to the extent possible, as shown in the table. We did not include the ICD sections of ill-defined diseases and the group of injuries and violence in the analysis, as these were regarded as too unspecific for solid conclusions. Mental disorders were the focus of a previous study [3], and childbirth and pregnancy complications require special considerations and will be investigated in separate publications.
Statistical analysis
Follow-up for diseases other than cancer was started 5 years after the date of cancer diagnosis for the cancer survivors and the corresponding date for the comparison individuals or at the beginning of the hospital registers (Denmark, 1977; Finland, 1975; Iceland, 1999; Sweden, from 1968–1987 stepwise inclusion of counties and nationwide since 1987), whichever occurred later. Follow-up for a second cancer in survivors and a first cancer in comparisons started at age 20 years at the earliest. Follow-up ended on the date of death, the date of emigration, or the end of the study (Iceland: 31 December 2008; Sweden: 31 December 2009; Denmark: 31 October 2010; Finland: 31 December 2012), whichever occurred first. As hospital registers do not reliably distinguish hospitalisations due to a relapse from those due to a primary cancer, we used the cancer registries for information on second primary cancers among childhood cancer survivors and first primary cancers among comparison individuals in analyses of hospitalisation risk. Thus, hospitalisations with childhood cancer recurrence were not included in the main analyses of hospitalisation risk.
Only the primary diagnosis, i.e., the main reason for hospitalisation at each inpatient contact, was included in the analyses. If participants had more than one hospital admission for a particular disease category, only the first record was retained. Risk was analysed for each of the 120 disease categories, and the numbers of first hospitalisations for somatic diseases in different categories were added up for the 12 main diagnostic groups. For each person, the final sum yielded the total number of first hospitalisations for diseases requiring hospitalisation in different categories. The observed number of first hospital admissions of survivors of childhood cancer for a given disease category was compared with expected numbers derived from the appropriate sex-, age-, and calendar period-specific hospitalisation rates of the comparison cohort, and the standardised hospitalisation rate ratios (RRs) were estimated. The significance and 95% confidence intervals (95% CIs) were computed using Fieller’s theorem and assuming that the observed number of first hospital contacts follows a Poisson distribution [22]. The absolute excess risk (AER), i.e., the additional risk for hospitalisation above background levels, was derived as the difference between the observed and expected first hospitalisation rates for a particular disease category per 100,000 person-years of follow-up. We did not stratify analyses by ethnicity, because this variable is not available in the Nordic population registers. However, the group of non-white individuals is historically of limited size in the Nordic countries and especially so among children.
Using the same methods as for the RR, we also added up the total number of bed days spent in hospital for cancer survivors and the number expected had they had the sex-, age-, and calendar period-specific bed day rates of the comparison individuals. We thus derived standardised bed day ratios (SBDRs) for cancer survivors. In the analyses of bed days, we included not only the first hospitalisation for a given disease category but all hospitalisations for diseases of the ICD sections of interest. Bed days for cancer recurrences were included in the analyses of SBDR.
Results
Table 1 gives the main characteristics of the 21,297 5-year childhood cancer survivors included in the analysis. The survivors were monitored in the national hospital registers for 336,554 person-years (mean: 16 years; range: 0–42 years). Of the survivors, 27% (5,655/21,297) and 12% (2,546/21,297) were followed beyond the ages of 40 and 50 years, respectively.

Overall, 9,698 (45.5%) childhood cancer survivors were ever admitted to hospital for somatic disease, when 5,399.2 (25.4%) were expected, yielding an RR of 1.80 (1.76–1.84). The 9,698 survivors ever hospitalised experienced 21,325 first admissions to hospital for diseases in one or more of the 120 disease categories listed in S1 Table, when 10,999.0 were expected, yielding an overall RR for a new category-specific admission of 1.94 (Table 2). The underlying RRs were 1.83 (1.78–1.87) in Denmark, 1.87 (1.82–1.92) in Finland, 1.64 (1.35–1.99) in Iceland, and 2.10 (2.05–2.15) in Sweden. Based on the observed and expected hospitalisation rates of 6,336.3 and 3,268.1 per 100,000 person-years, respectively, the AER of survivors for a new category-specific admission to hospital was 3,068 per 100,000 person-years (Table 2). Thus, for each additional year of follow-up, approximately 3 of 100 survivors of childhood cancer were hospitalised for a new excess disease. Although the relative risk was significantly increased at all ages, the degree of increase diminished substantially with increasing age, i.e., from a relative risk of 3.4 in the age group 5–9 years to 1.3 in survivors aged 60 years or older. The absolute risk did not show a similar linear decline: after about 5,700 excess category-specific hospitalisations per 100,000 person-years in the age group 5–9 years, the AERs varied from 2,500 to 3,700 excess hospitalisations per 100,000 person-years for all subsequent age groups.

Fig 2 shows the relative risk for hospitalisation for somatic diseases belonging to each of the 12 main diagnostic groups; the highest risks were seen for diseases of the nervous system and sense organs (RR: 3.6 [3.4–3.7]), followed by diseases of the blood and blood-forming organs (RR: 2.8 [2.5–3.2]), endocrine diseases and nutritional deficiencies (RR: 2.8 [2.7–3.0]), and new primary cancers (RR: 2.6 [2.4–2.8]).
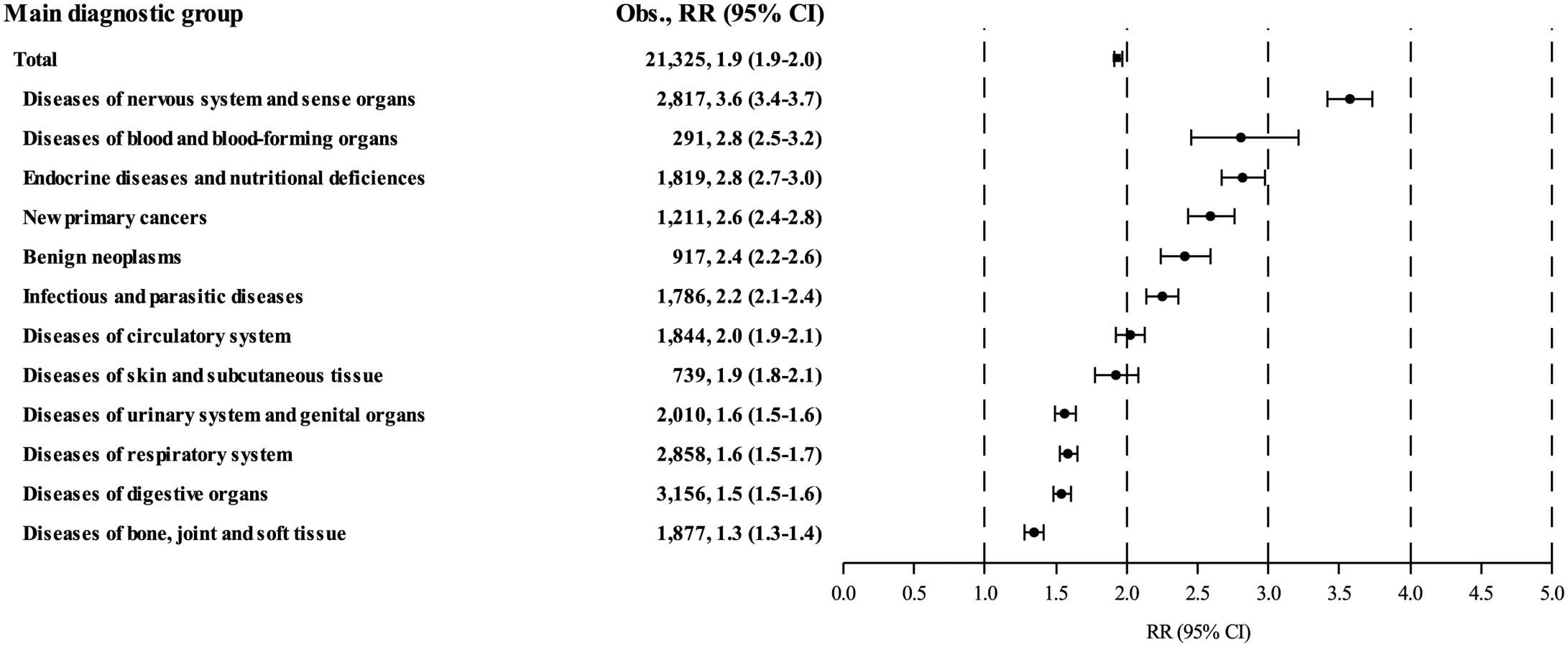
Table 3 shows that the pattern of excess hospitalisations among survivors is dominated by diseases of the nervous system and sense organs (AER: 603 per 100,000 person-years), followed by diseases of the endocrine system and nutritional deficiencies (AER: 349 per 100,000 person-years), diseases of the digestive organs (AER: 330 per 100,000 person-years), and diseases of the respiratory system (AER: 314 per 100,000 person-years). Together, these four main diagnostic groups constituted 50.6% (1,596/3,154) of all new excess hospitalisations, mainly for epilepsy (AER: 199 per 100,000 person-years), diseases of nerves and peripheral ganglia (AER: 157 per 100,000 person-years), pneumonia (AER: 144 per 100,000 person-years), and pituitary hypofunction (AER: 101 per 100,000 person-years). Table 3 shows the estimated relative and absolute risks of cancer survivors for each of the main diagnostic groups and a selected number of disease categories. The full table including all 120 disease categories is presented in S2 Table. Particularly high relative risks were seen for pituitary hypofunction (RR: 72.0; n = 341), testicular dysfunction (RR: 22..9; n = 19), tumours of the central nervous system (CNS) (RR: 11.8; n = 257), and herpes zoster (RR: 11.2; n = 58).

Fig 3A shows that the slight increase in overall AER seen in childhood cancer survivors over 40 years of age (Table 1) is due to marked increases in the AERs for diseases of the circulatory system, new primary cancers, and respiratory diseases with age. Moreover, the figure shows that the prevailing diagnostic groups during early life were diseases of the nervous system and sense organs and infectious and parasitic diseases. Except for a small peak among adolescent survivors for hospitalisation for diseases of the endocrine system, the AERs of the seven remaining main diagnostic groups did not show any appreciable variation by attained age (Fig 3B).

Survivors of all types of childhood cancers were at significantly increased risk for admission to hospital for subsequent disease (Fig 4). Survivors of neuroblastoma were at highest risk (RR: 2.6), followed by survivors of hepatic tumours (RR: 2.5), CNS tumours (RR: 2.4), Hodgkin lymphoma (RR: 2.4), and other lymphomas (RR: 2.3). Panels A—M in S1 Fig show the variations in the excess hospitalisation patterns among survivors of the 11 main groups of childhood cancer and of the two subgroups of lymphoma. For example, slightly more than half of all excess hospitalisations of survivors of CNS tumours were for subsequent diseases of the nervous system and sense organs and endocrine disorders and nutritional deficiencies, while infectious and parasitic diseases and diseases of the circulatory system were the primary reasons for hospitalisation of survivors of leukaemia and Hodgkin lymphoma, respectively.

The 9,698 cancer survivors who were ever hospitalised spent a total of 422,218 days in hospital whereas 85,071.7 were expected, yielding an overall SBDR of 4.96 (Table 4). The highest SBDRs were seen for survivors of hepatic tumours (SBDR: 9.9), followed by survivors of leukaemia (SBDR: 8.9), neuroblastoma (SBDR: 8.4), and CNS tumours (SBDR: 6.9). Fig 5 shows that most of the days spent by cancer survivors in hospital were for cancer recurrences and new primary cancers (SBDR: 24.2), followed by diseases of the nervous system and sense organs (SBDR: 5.8), diseases of blood and blood-forming organs (SBDR: 4.2), and benign neoplasms (SBDR: 3.4). The high overall SBDR for diseases of the nervous system and sense organs was due mainly to a particularly high SBDR of 15.9 (15.5–16.2) for epilepsy. Panels A—M in S2 Fig show the SBDR distributions for survivors of each of the 11 main groups of childhood cancer and the two subgroups of lymphoma, and S3 Fig shows the SBDR distribution for cancer recurrences and new primary cancers by main group of childhood cancer.


Discussion
This population-based study of 21,297 5-year survivors of childhood cancer in the Nordic countries gives an extensive overview of the pattern of later somatic conditions that are serious enough to require inpatient care. The study shows that survivors are hospitalised because of a new somatic disease twice as often as population comparisons and that they spend five times as many days in hospital. Although cancer and its treatment may affect practically all organ systems adversely, the pattern of diseases requiring hospitalisation of survivors varied widely by type of childhood cancer and by survivors’ attained age. Despite the variations, however, the important findings are that the majority of childhood cancer survivors are at substantial risk for late effects requiring inpatient care and that the risk remains increased throughout life.
Our results concur with the mounting evidence of an excess risk for serious long-term morbidity in survivors of childhood cancer. Thus, in a clinical assessment, Geenen et al. identified chronic late effects in 74.5% of survivors treated in a single institution in The Netherlands [23]. Using self-reported outcomes, Oeffinger et al. showed that 62.3% of survivors included in the North American Childhood Cancer Survivor Study (CCSS) experienced at least one adverse, chronic late effect, equivalent to a 3.3-fold higher risk than their siblings [24]. This result is fairly consistent with the hospitalisation rate ratio for somatic disease of close to 2 seen in our study, taking into account differences in the sources of information and the maximum age at the end of follow-up (48 years in CCSS, lifelong in the Nordic study). In a later analysis of the CCSS material, Kurt et al. reported a survivor hospitalisation rate that was 1.6 times higher (95% CI 1.6–1.7) than that derived from a United States National Hospital Discharge Survey covering the period 1992–2005 [8].
In a few newer studies of the risk for late morbidity among survivors of cancer diagnosed during childhood, adolescence, and young adulthood (age range: 0–24 years), diagnostic information from hospital discharge registers was used as the outcome measure [9,10,12,13]. These studies, conducted in Utah, US; British Columbia, Canada; Scotland; and The Netherlands, included 1,499, 1,374, 5,229, and 1,382 survivors, respectively. They show a similar picture of substantial excess hospitalisation for a wide range of diseases, with increased cumulative numbers of days at hospital, as compared with population comparisons. Because of the substantially larger sample included in the present study and a follow-up period extending into middle age and beyond, we are able to provide a more detailed description of subsequent disease for a broader age range while maintaining relatively narrow 95% confidence limits. One notable difference between the four studies mentioned above and ours is that they included hospitalisations for psychiatric diseases, cancer recurrence, congenital abnormalities, injuries, suicide, and externally caused morbidities in the analysis, and the studies in British Columbia, Utah, and The Netherlands also included hospitalisations for pregnancy complications and delivery [9,12,13]. This probably explains the moderately higher overall risks for hospitalisation reported in those studies.
We used hospital-based diagnoses made by physicians as markers of disease outcome. Although this approach increased the validity of the diagnostic information, less severe late effects might have been missed because they were treated sufficiently as hospital outpatients or in the primary health care system. This implies that we almost certainly underestimate the absolute overall somatic disease burden experienced by childhood cancer survivors. As this limitation also applies to the comparison cohort, however, the validity of the relative risk estimates is acceptable, although restricted to conditions that require a hospital contact. Moreover, we cannot exclude the possibility that our results were affected by better medical surveillance of the survivors than the population comparisons, which could explain part of the longer hospital stays in the survivors. Not covered by the present study of the somatic disease burden but important to stress is the fact that many childhood cancer survivors face additional and sometimes significant challenges due to cognitive and other psychological adverse effects from cancer and its treatment [3,7].
The information on treatment currently included in the Nordic cancer registries is generally too crude or absent for meaningful analyses of type and dose of chemotherapy and radiation and specific disease outcomes. Although our study does not attribute causality, this comprehensive overview provides important clinical information on the lifelong inpatient disease burden experienced by childhood cancer survivors overall and of a number of patient characteristics, including type of childhood cancer, type of late effect, sex, and attained age. Associations, including dose-response effects, between specific treatment regimens and the risk of selected late effects are being addressed in clinical case-cohort studies within the ALiCCS cohort [14].
As our study is population based and includes a randomly selected comparison group and data from high-quality health registers, we consider our results valid for children treated for cancer in other countries with similar health care systems.
In conclusion, we found that survivors of childhood cancer have a highly increased long-term disease burden, with a broad range of late effects that require inpatient treatment and substantially longer stays in hospital as compared with the background population of similar age and sex. This will inevitably constitute a growing health care challenge for our society, affecting medical costs, and may profoundly influence the quality of life and life expectancy of childhood cancer survivors. Our findings underscore the need for continued follow-up of survivors, with particular focus on survivors of neuroblastoma, hepatic tumours, CNS tumours, Hodgkin lymphoma, and leukaemia. In particular, primary health care physicians should be aware of the risk for second primary cancers in patients who are childhood cancer survivors, as the relative risks for cancers are high and tumours may appear earlier in life than usual.
Supporting Information
Zdroje
1. de Nully BP, Olsen JH, Hertz H, Carstensen B, Bautz A. Trends in survival after childhood cancer in Denmark, 1943–87: a population-based study. Acta Paediatr. 1995;84(3):316–24. 7780256
2. Gatta G, Botta L, Rossi S, Aareleid T, Bielska-Lasota M, Clavel J, et al. Childhood cancer survival in Europe 1999–2007: results of EUROCARE-5—a population-based study. Lancet Oncol. 2014;15(1):35–47. doi: 10.1016/S1470-2045(13)70548-5 24314616
3. Lund LW, Winther JF, Dalton SO, Cederkvist L, Jeppesen P, Deltour I, et al. Hospital contact for mental disorders in survivors of childhood cancer and their siblings in Denmark: a population-based cohort study. Lancet Oncol. 2013;14(10):971–80. doi: 10.1016/S1470-2045(13)70351-6 23954078
4. de Fine Licht S, Winther JF, Gudmundsdottir T, Holmqvist AS, Bonnesen TG, Asdahl PH, et al. Hospital contacts for endocrine disorders in Adult Life after Childhood Cancer in Scandinavia (ALiCCS): a population-based cohort study. Lancet. 2014;383(9933):1981–9. doi: 10.1016/S0140-6736(13)62564-7 24556022
5. Armstrong GT, Kawashima T, Leisenring W, Stratton K, Stovall M, Hudson MM, et al. Aging and risk of severe, disabling, life-threatening, and fatal events in the childhood cancer survivor study. J Clin Oncol. 2014;32(12):1218–27. doi: 10.1200/JCO.2013.51.1055 24638000
6. Oeffinger KC, Hudson MM. Long-term complications following childhood and adolescent cancer: foundations for providing risk-based health care for survivors. CA Cancer J Clin. 2004;54(4):208–36. 15253918
7. Jacola LM, Edelstein K, Liu W, Pui CH, Hayashi R, Kadan-Lottick NS, et al. Cognitive, behaviour, and academic functioning in adolescent and young adult survivors of childhood acute lymphoblastic leukaemia: a report from the Childhood Cancer Survivor Study. Lancet Psychiatry. 2016;3(10):965–72. doi: 10.1016/S2215-0366(16)30283-8 27639661
8. Kurt BA, Nolan VG, Ness KK, Neglia JP, Tersak JM, Hudson MM, et al. Hospitalization rates among survivors of childhood cancer in the childhood cancer survivor study cohort. Pediatr Blood Cancer. 2012;59(1):126–32. doi: 10.1002/pbc.24017 22180128
9. Sieswerda E, Font-Gonzalez A, Reitsma JB, Dijkgraaf MG, Heinen RC, Jaspers MW, et al. High Hospitalization Rates in Survivors of Childhood Cancer: A Longitudinal Follow-Up Study Using Medical Record Linkage. PLoS ONE. 2016;11(7):e0159518. doi: 10.1371/journal.pone.0159518 27433937
10. Brewster DH, Clark D, Hopkins L, Bauer J, Wild SH, Edgar AB, et al. Subsequent hospitalisation experience of 5-year survivors of childhood, adolescent, and young adult cancer in Scotland: a population based, retrospective cohort study. Br J Cancer. 2014;110(5):1342–50. doi: 10.1038/bjc.2013.788 24366296
11. Rebholz CE, Reulen RC, Toogood AA, Frobisher C, Lancashire ER, Winter DL, et al. Health care use of long-term survivors of childhood cancer: the British Childhood Cancer Survivor Study. J Clin Oncol. 2011;29(31):4181–8. doi: 10.1200/JCO.2011.36.5619 21947833
12. Lorenzi MF, Xie L, Rogers PC, Pritchard S, Goddard K, McBride ML. Hospital-related morbidity among childhood cancer survivors in British Columbia, Canada: report of the childhood, adolescent, young adult cancer survivors (CAYACS) program. Int J Cancer. 2011;128(7):1624–31. doi: 10.1002/ijc.25751 21280033
13. Kirchhoff AC, Fluchel MN, Wright J, Ying J, Sweeney C, Bodson J, et al. Risk of hospitalization for survivors of childhood and adolescent cancer. Cancer Epidemiol Biomarkers Prev. 2014;23(7):1280–9. doi: 10.1158/1055-9965.EPI-13-1090 24925676
14. Asdahl PH, Winther JF, Bonnesen TG, De Fine Licht S, Gudmundsdottir T, Anderson H, et al. The Adult Life After Childhood Cancer in Scandinavia (ALiCCS) Study: Design and Characteristics. Pediatr Blood Cancer. 2015;62(12):2204–10. doi: 10.1002/pbc.25661 26193842
15. Tulinius H, Storm HH, Pukkala E, Andersen A, Ericsson J. Cancer in the Nordic countries, 1981–86. A joint publication of the five Nordic Cancer Registries. APMIS Suppl. 1992;31 : 1–194. 1301768
16. Gjerstorff ML. The Danish Cancer Registry. Scand J Public Health. 2011;39(7 Suppl):42–5. doi: 10.1177/1403494810393562 21775350
17. Sigurdardottir LG, Jonasson JG, Stefansdottir S, Jonsdottir A, Olafsdottir GH, Olafsdottir EJ, et al. Data quality at the Icelandic Cancer Registry: Comparability, validity, timeliness and completeness. Acta Oncol. 2012;51(7):880–9. doi: 10.3109/0284186X.2012.698751 22974093
18. Barlow L, Westergren K, Holmberg L, Talback M. The completeness of the Swedish Cancer Register: a sample survey for year 1998. Acta Oncol. 2009;48(1):27–33. doi: 10.1080/02841860802247664 18767000
19. Birch JM, Marsden HB. A classification scheme for childhood cancer. Int J Cancer. 1987;40(5):620–4. 3679589
20. Ludvigsson JF, Andersson E, Ekbom A, Feychting M, Kim JL, Reuterwall C, et al. External review and validation of the Swedish national inpatient register. BMC Public Health. 2011;11 : 450. doi: 10.1186/1471-2458-11-450 21658213
21. Lynge E, Sandegaard JL, Rebolj M. The Danish National Patient Register. Scand J Public Health. 2011;39(7 Suppl):30–3. doi: 10.1177/1403494811401482 21775347
22. Fieller EC. Some problems in interval estimation. Journal of the Royal Statistical Society. 1954;16(2):175–85.
23. Geenen MM, Cardous-Ubbink MC, Kremer LC, van den BC, van der Pal HJ, Heinen RC, et al. Medical assessment of adverse health outcomes in long-term survivors of childhood cancer. JAMA. 2007;297(24):2705–15. doi: 10.1001/jama.297.24.2705 17595271
24. Oeffinger KC, Mertens AC, Sklar CA, Kawashima T, Hudson MM, Meadows AT, et al. Chronic health conditions in adult survivors of childhood cancer. N Engl J Med. 2006;355(15):1572–82. doi: 10.1056/NEJMsa060185 17035650
Štítky
Interní lékařstvíČlánek vyšel v časopise
PLOS Medicine
2017 Číslo 5
- Ivabradin zlepšuje kvalitu života starších pacientů se srdečním selháním
- Fixní kombinace kandesartan/amlodipin v terapii arteriální hypertenze
- Inovace v hojení ran: krytí Zetuvit Plus Silicone Border pro optimální management exsudátu z ran
- Rána vizitkou (nejen) chirurga
- Patogeneze vzniku keloidní jizvy
Nejčtenější v tomto čísle
- Mortality and kidnapping estimates for the Yazidi population in the area of Mount Sinjar, Iraq, in August 2014: A retrospective household survey
- Vitamin D levels and susceptibility to asthma, elevated immunoglobulin E levels, and atopic dermatitis: A Mendelian randomization study
- Maternal age and severe maternal morbidity: A population-based retrospective cohort study
- Estimation of the cost-effectiveness of HIV prevention portfolios for people who inject drugs in the United States: A model-based analysis
Zvyšte si kvalifikaci online z pohodlí domova
Mazová zátka a její řešení
nový kurzVšechny kurzy