
Atypical placental site nodule detected via hysteroscopy – first case report from Brazil
Atypický uzlík v placentární oblasti detekovaný hysteroskopií – první kazuistika z Brazílie
Atypický uzlík v placentárním místě (APSN – atypical placental site nodule) je vzácná forma gestační trofoblastické choroby (GTD – gestational trophoblastic disease), která vzniká proliferací intermediárních trofoblastů s nejistým klinickým chováním. Je považován za potenciální prekurzor vzácných forem gestační trofoblastické neoplazie (GTN – gestational trophoblastic neoplasia), jako je trofoblastický tumor v placentárním místě (PSTT – placental site trophoblastic tumor) a epiteloidní trofoblastický tumor (ETT – epithelioid trophoblastic tumor). Tato kazuistika popisuje první brazilský případ APSN diagnostikovaný hysteroskopií u 43leté ženy po potratu. Histopatologická analýza odhalila ohraničený, hyalinizovaný agregát intermediárních trofoblastů s jadernou atypií, pozitivním imunobarvením na PLAP a p63 a indexem Ki-67 > 5 %. Pacientka odmítla hysterektomii a zvolila konzervativní léčbu s pečlivým sledováním. Po 12 měsících sledování nebyla pozorována žádná progrese. Tento případ zdůrazňuje diagnostické výzvy APSN vzhledem k jeho nenápadnému projevu a překrývání s benigními uzlíky v místě placenty nebo dokonce s PSTT/ETT. Hysteroskopie se ukázala jako cenná jak pro diagnózu, tak pro léčbu zachování fertility. Přestože hysterektomie v mnoha případech zůstává definitivní léčbou, stále častěji se zvažují individualizované přístupy vyvažující onkologickou bezpečnost a reprodukční cíle. Dlouhodobá klinická bdělost je nezbytná, protože APSN může předcházet agresivním formám GTN. Naléhavě jsou zapotřebí multicentrické studie a registry, které by stanovily směrnice založené na důkazech pro diagnostiku, léčbu a sledování této vzácné léze a zlepšily by výsledky pacientů s těmito neobvyklými formami GTD.
Klíčová slova:
atypický uzlík v placentární oblasti – gestační trofoblastické onemocnění – gestační trofoblastická neoplazie – trofoblastický tumor v placentární oblasti – epiteloidní trofoblastický tumor
Authors:
Antônio Braga 1-3
![]() ; Gabriela Paiva 1,2
; Gabriela Paiva 1,2
![]() ; Lilian Padron 1
; Lilian Padron 1
![]() ; Aretha Nobre 1
; Aretha Nobre 1
![]() ; Juliana Soares Pereira 3
; Juliana Soares Pereira 3
![]() ; Gustavo Yano Callado 4
; Gustavo Yano Callado 4
![]() ; Joffre Amim Junior 1
; Joffre Amim Junior 1
![]() ; Sue Yazaki Sun 5
; Sue Yazaki Sun 5
![]() ; Edward Araujo Júnior 4-6
; Edward Araujo Júnior 4-6
![]() ; Jorge Rezende-Filho 1
; Jorge Rezende-Filho 1
![]() ; Neil Horowitz 7
; Neil Horowitz 7
![]() ; Ross Berkowitz 7
; Ross Berkowitz 7
![]()
Authors place of work:
Department of Gynecology and Obstetrics, School of Medicine, Maternity School. Federal University of Rio de Janeiro (UFRJ), Rio de Janeiro, Brazil
1; Department of Maternal and Child Health, Postgraduate Program in Medical Sciences. School of Medicine, Fluminense Federal University (UFF), Niterói, Brazil
2; Postgraduate Program in Applied Health Sciences. University of Vassouras, Vassouras, Brazil
3; Discipline of Woman Health, Albert Einstein Israelite College of Health Sciences (FICSAE), Albert Einstein Israelite Hospital, São Paulo, Brazil
4; Department of Obstetrics, Paulista School of Medicine, Federal University of São Paulo (EPM-UNIFESP), Sao Paulo, Brazil
5; Discipline of Woman Health, Municipal University of São Caetano do Sul (USCS), São Caetano do Sul, Brazil
6; New England Trophoblastic Dis ease Center, Division of Gynecologic Oncology, Department of Obstetrics, Gynecology and Reproductive, Biology, Brigham and Women’s Hospital, Harvard Medical School, Boston, USA
7
Published in the journal:
Ceska Gynekol 2025; 90(6): 479-485
Category:
Kazuistika
doi:
https://doi.org/10.48095/cccg2025479
Summary
Atypical placental site nodule (APSN) is a rare form of gestational trophoblastic disease (GTD) originating from the proliferation of intermediate trophoblasts, with uncertain clinical behavior. It is considered a potential precursor to rare forms of gestational trophoblastic neoplasia (GTN), such as placental site trophoblastic tumor (PSTT) and epithelioid trophoblastic tumor (ETT). This report describes the first Brazilian case of APSN diagnosed via hysteroscopy in a 43-year-old woman following miscarriage. Histopathological analysis revealed a circumscribed, hyalinized aggregate of intermediate trophoblasts with nuclear atypia, positive immunostaining for PLAP and p63, and a Ki-67 index > 5%. The patient declined hysterectomy, opting for conservative management with close monitoring. After 12 months of follow-up, no progression was observed. This case emphasizes the diagnostic challenges of APSN, given its subtle presentation and overlap with benign placental site nodules or even PSTT/ETT. Hysteroscopy proved valuable for both diagnosis and fertility-preserving management. Although hysterectomy remains the definitive treatment in many cases, individualized approaches balancing oncologic safety and reproductive goals are increasingly considered. Long-term clinical vigilance is essential, as APSN may precede aggressive GTN forms. Multicenter studies and registries are urgently needed to establish evidence-based guidelines for the diagnosis, treatment, and follow-up of this rare lesion, improving patient outcomes in these uncommon forms of GTD.
Keywords:
gestational trophoblastic disease – gestational trophoblastic neoplasia – atypical placental site nodule – placental site trophoblastic tumor – epithelioid trophoblastic tumor
Introduction
Gestational trophoblastic disease (GTD) encompasses a heterogeneous group of lesions derived from villous and intermediate trophoblasts (IT), with varying potential for invasion, malignancy, metastasis, and prognosis [1]. The most common forms of GTD originate from the villous trophoblast and include the hydatidiform mole, which carries a 5–20% risk of progression to gestational trophoblastic neoplasia (GTN) [2,3], as well as the invasive mole and choriocarcinoma, both of which are highly responsive to chemotherapy [4]. In contrast, the IT gives rise to placental site nodules (PSNs) – both typical and atypical (APSNs) [5,6] – as well as placental site trophoblastic tumor (PSTT) and epithelioid trophoblastic tumor (ETT) [7]. The latter two are chemoresistant and associated with poorer prognoses [8].
While typical PSNs appear to lack potential for progression to GTN, a subset of lesions has been described with intermediate features between a typical PSN and ETT [5]. These lesions are characterized by larger size (> 5 mm), a higher Ki-67 index (ranging from 8% to 15%), and increased cellularity compared to typical PSNs, and were subsequently designated as APSNs [9]. Despite these atypical features, such lesions were initially considered benign in terms of clinical outcome, similar to PSNs. However, in 2015, Kaur et al. [9] reported a series of 21 APSN cases in which 14% (3/21) progressed to GTN (PSTT and/or ETT) during a 16-month follow-up based on hormonal surveillance. Following this publication, APSN was incorporated into the 2020 World Health Organization classification of tumors of the female genital tract as a precursor lesion to GTN [10].
The biological behavior of APSN remains uncertain, and clinical management is not yet well defined, ranging from expectant monitoring to prophylactic hysterectomy. The aim of this report is to present the first Brazilian case of APSN detected via hysteroscopy, discussing the diagnostic criteria for this entity, its potential progression to PSTT/ETT, and appropriate therapeutic approaches.
Case report
This case report was approved by the Research Ethics Committee of the Maternity School of the Federal University of Rio de Janeiro (CAAE: 90140425.3.0000.5275), and written informed consent was obtained from the patient authorizing its publication.
A 43-year-old Black woman, gravida 1 para 0, with no previous obstetric complications, experienced a spontaneous late miscarriage at 18 weeks of gestation. She had been admitted with abnormal vaginal bleeding and uterine contractions. Prenatal ultrasounds and routine exams had been normal, and she reported no symptoms during pregnancy. Manual removal of the retained placenta followed by uterine curettage was performed under anesthesia without complications.
Histopathological examination of the placenta showed no fetal vasculopathy and no features suggestive of proliferative trophoblastic activity. Prior to pregnancy, the patient had been using combined oral contraceptive pill continuously due to polycystic ovary syndrome and had no personal or family history of other relevant medical conditions.
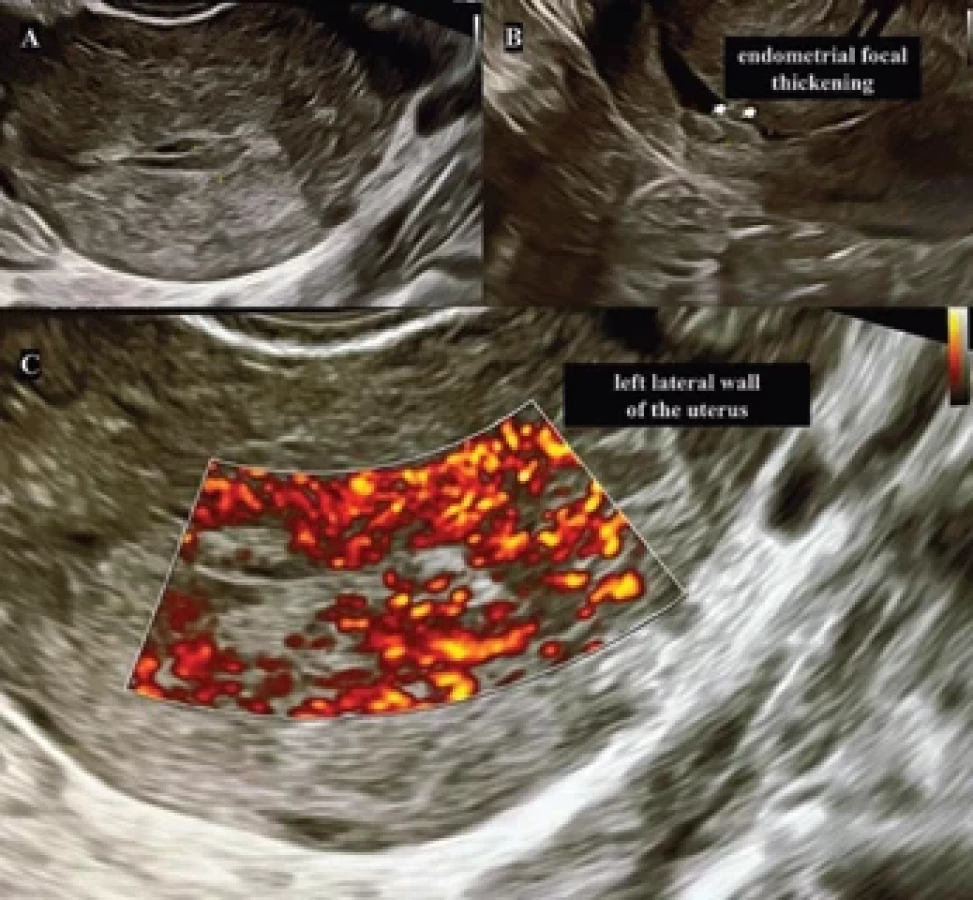
As she expressed a desire to conceive again, a transvaginal ultrasound was performed one month later. It revealed a discrete focal thickening of the endometrium with increased vascularity on color Doppler mapping (Fig. 1). Pelvic magnetic resonance imaging (MRI) was requested but showed no abnormalities (Fig. 2). Subsequently, hysteroscopy confirmed a focal endometrial thickening in the left cornual region of the uterus, measuring approximately 0.7 cm (Fig. 3).
Histological analysis of an endometrial biopsy obtained during hysteroscopy revealed a circumscribed, hyalinized aggregate of intermediate trophoblasts with central hyalinization and cohesive nests and cords exhibiting cytologic and mild nuclear atypia. Immunohistochemical staining was positive for placental alkaline phosphatase (PLAP) and p63, with a Ki-67 proliferation index > 5%, as shown in Fig. 4. The diagnosis of APSN was confirmed by two independent pathologists.
The patient was referred to the Rio de Janeiro GTD reference center, where her serum human chorionic gonadotropin (hCG) levels were within normal limits. A chest X-ray showed no evidence of metastatic disease, and pelvic MRI revealed a centered, homogeneous endometrium measuring 1 mm in thickness, with no expansile lesions identified in the uterine cavity.
The patient was counseled regarding the uncertain natural history of APSN, including its potential progression to PSTT or ETT. Hysterectomy was proposed as definitive treatment; however, the she declined surgical intervention due to her nulliparity and desire to preserve fertility.
Monthly serum hCG levels remained within the normal range over 12 months of follow-up. Control hysteroscopies performed at 6 and 12 months post-diag - nosis revealed a homogeneously distributed endometrium with a smooth surface, reddish coloration, normal vascularization, and the presence of glands with a dotted pattern, consistent with a proliferative endometrium. Histological confirmation through biopsy corroborated these findings.
As the patient continues to express a desire to conceive, she is currently under follow-up at the preconception care service of our institution.



Discussion
This is the first reported case of an APSN identified by hysteroscopy in Brazil, emerging from a GTD reference center that has managed over 10,000 patients across the full GTD spectrum [11]. In the entire case series from the largest Brazilian referral center, this is the 10th identified APSN, corresponding to a prevalence of less than 1 in 1,000 GTD cases. The rarity of this diagnosis is underscored not only by the scarcity of reports in international literature but also by its low incidence even in high-volume, specialized centers. This emphasizes the uniqueness of the present case and the relevance of its publication for both the scientific and clinical communities.
Diagnosing APSN remains a considerable challenge due to its subtle clinical presentation and histopathological overlap with other entities within the trophoblastic spectrum. In routine pathology practice, APSNs may be misinterpreted as benign PSNs or underestimated as regressive gestational remnants. However, emerging evidence suggests that APSNs may serve as precursor lesions to malignant entities such as PSTT and ETT, both derived from intermediate trophoblasts [8]. This highlights the critical need for heightened awareness among pathologists, particularly those working in reproductive pathology and gynecologic oncology [12–14].
In this context, the use of strict diagnostic criteria and immunohistochemical panels is essential. While PSNs typically exhibit minimal proliferative activity (Ki-67 index < 5%), APSNs show increased mitotic activity, nuclear atypia, and a higher Ki-67 index, often ranging from 10% to 20%. Immunostaining for hPL, CD146 (Mel-CAM), and p63 plays a crucial role in distinguishing APSN from PSTT, ETT, and benign remnants [9,12–14]. Nevertheless, despite the availability of these tools, diagnostic variability and interpretive uncertainty remain common, complicating clinical management [15,16].
One of the most significant clinical implications of APSN is its potential for malignant progression [9,14,17]. Although data are limited, available reports suggest that APSNs may precede the development of PSTT and/or ETT, both of which are rare, aggressive GTN forms with variable prognosis and limited response to chemotherapy. Notably, prognosis worsens when the interval between the antecedent pregnancy and GTN diagnosis exceeds four years [7,8]. Therefore, clinical vigilance and long-term monitoring are pivotal following an APSN diagnosis.
Hormonal surveillance, particularly serial serum hCG measurements, remains an essential component of follow-up. While APSNs may not always result in elevated hCG levels, rising titers can indicate progression to GTN [9,15,17]. Unfortunately, many APSN cases present with normal hCG levels. In addition, imaging modalities such as transvaginal ultrasound and chest X-ray may be useful for evaluating local recurrence or progression, especially in patients desiring uterine preservation [18].
Management of APSN remains a subject of debate. Some authors advocate definitive surgical treatment, typically via hysterectomy, especially in cases with atypical features, incomplete resection, or in women who have completed childbearing. This approach ensures diagnostic certainty and eliminates the potential risk of subsequent GTN [9,17]. However, in younger women desiring future fertility, a conservative approach may be considered. This includes complete local excision (preferably via hysteroscopy or, alternatively, curettage), combined with close clinical, hormonal, and radiological follow-up [18,19].
Imaging methods such as transvaginal ultrasound and pelvic MRI may yield normal results in APSN cases, as demonstrated by Lockett et al. [20]. In that cohort, conventional imaging frequently failed to detect abnormalities associated with APSNs. Among all imaging modalities evaluated, hysteroscopy had the highest diagnostic yield, though 44% of cases still showed a normal-appearing endometrial cavity. The remaining cases showed 11% with endometrial polyps, 22% with focal endometrial lesions, 11% with retained nonviable placental tissue, and 11% with endometrial thickening. These findings support the role of hysteroscopy in both diagnostic and therapeutic management.
Hysteroscopy enables direct visualization of the endometrial cavity and precise localization of focal lesions, which is especially useful when APSNs are small, asymptomatic, or incidentally discovered [20,21]. Hysteroscopic resection allows for complete lesion excision while preserving the uterus, making it a favorable option for women of reproductive age. Moreover, hysteroscopy facilitates targeted sampling for histopathological and immunohistochemical analysis – crucial for distinguishing APSNs from PSNs and malignant counterparts such as PSTT and ETT. In selected cases, hysteroscopy may serve as both a diagnostic and fertility-preserving therapeutic tool, provided that careful long-term follow-up is maintained.
Two of the most comprehensive APSN studies come from Charing Cross Hospital (London) [9] and Brigham and Women’s Hospital (Boston) [17]. Both centers consider hysterectomy the definitive treatment. However, at the Boston center, there is a broader inclination toward conservative management in patients with reproductive desires. These differing approaches reflect the current uncertainty surrounding APSN and underscore the importance of individualized care, multidisciplinary decision-making, and referral to specialized GTD centers, where diagnostic expertise and fertility-preserving strategies can be integrated. Prospective data are urgently needed to establish evidence-based management guidelines.
In the present case, the patient’s reproductive age and desire for fertility preservation were central to the clinical decision-making process. Conservative management was deemed acceptable, contingent on close monitoring. A limitation of this report is the relatively short follow-up period after remission, which may affect the timely detection of late recurrence. Nevertheless, the case contributes to the growing body of literature supporting the feasibility of fertility-preserving strategies in selected patients, although definitive recommendations remain premature.
Ultimately, this case highlights the many uncertainties that persist regarding APSN – from diagnostic criteria and classification to optimal treatment and surveillance strategies. Further research is needed to better define its natural history and malignant potential. Multicenter registries and collaborative research initiatives are essential to advance knowledge in this area.
Conclusion
In conclusion, APSN is a rare and diagnostically challenging lesion with significant clinical implications. Although generally considered a benign or borderline entity, its potential association with malignant GTN warrants thorough evaluation and sustained follow-up. Raising awareness among clinicians and pathologists is crucial for timely diagnosis and appropriate management. In reproductive-aged women, treatment must balance oncologic safety with fertility preservation. As more cases are reported, a clearer clinical pathway is expected to emerge.
Zdroje
1. Lok C, van Trommel N, Braicu EI et al. Practical Guidelines for the Treatment of Gestational Trophoblastic Disease: Collaboration of the European Organisation for the Treatment of Trophoblastic Disease (EOTTD) – European Society of Gynaecologic Oncology (ESGO) – Gynecologic Cancer InterGroup (GCIG) – International Society for the Study of Trophoblastic Diseases (ISSTD). J Clin Oncol 2025; 43 (18): 2119–2128. doi: 10.1200/JCO-24-02326.
2. Braga A, Paiva G, Barcellos M et al. Diagnosis and management of molar pregnancies. Hematol Oncol Clin North Am 2024; 38 (6): 1149–1159. doi: 10.1016/j.hoc.2024.07.001.
3. Joneborg U. Epidemiology of gestational trophoblastic disease. Hematol Oncol Clin North Am 2024; 38 (6): 1173–1190. doi: 10.1016/j.hoc.2024.07.003.
4. Wang X, Wu J, Xie W. Evolution of treatment strategies for gestational trophoblastic neoplasia: chemotherapy, immunotherapy, and molecular targeted therapy. Curr Treat Options Oncol 2024; 25 (8): 1055–1062. doi: 10.1007/s11864-024-0123-y.
5. Cho EJ, Chun SM, Park H et al. Whole transcriptome analysis of gestational trophoblastic neoplasms reveals altered PI3K signaling pathway in epithelioid trophoblastic tumor. Gynecol Oncol 2020; 157 (1): 151–160. doi: 10.1016/j.ygyno.2019.09.022.
6. Shih IM, Kurman RJ. The pathology of intermediate trophoblastic tumors and tumor-like lesions. Int J Gynecol Pathol 2001; 20 (1): 31–47. doi: 10.1097/00004347-200101000 - 00004.
7. Wang V, Elias KM, Berkowitz RS et al. Placental site trophoblastic tumors and epithelioid trophoblastic tumors. Hematol Oncol Clin North Am 2024; 38 (6): 1277–1286. doi: 10.1016/j.hoc.2024.08.016.
8. Horowitz NS, Goldstein DP, Berkowitz RS. Placental site trophoblastic tumors and epithelioid trophoblastic tumors: biology, natural history, and treatment modalities. Gynecol Oncol 2017; 144 (1): 208–214. doi: 10.1016/j.ygyno.2016.10.024.
9. Kaur B, Short D, Fisher RA et al. Atypical placental site nodule (APSN) and association with malignant gestational trophoblastic disease; a clinicopathologic study of 21 cases. Int J Gynecol Pathol 2015; 34 (2): 152–158. doi: 10.1097/PGP.0000000000000128.
10. Lokuhetty D, White VA, Watanabe R. Female genital Tumours. 5th ed. Lyon: Internal Agency for Research on Cancer (IARC) 2020.
11. Freitas F, Braga A, Viggiano M et al. Gestational trophoblastic neoplasia lethality among Brazilian women: a retrospective national cohort study. Gynecol Oncol 2020; 158 (2): 452–459. doi: 10.1016/j.ygyno.2020.04.704.
12. Kaur B. Pathology of gestational trophoblastic disease (GTD). Hematol Oncol Clin North Am 2024; 38 (6): 1191–1217. doi: 10.1016/j.hoc.2024.08.017.
13. Perez CE, Chapel DB, Skala SL. Application of current pathologic criteria for atypical placental site nodule suggests that refined criteria are needed. Int J Gynecol Pathol 2023; 42 (5): 482–490. doi: 10.1097/PGP.0000000000000934.
14. He Y, Yang W, Zhang Y. Atypical placental site nodules: five cases and literature review. Zhong Nan Da Xue Xue Bao Yi Xue Ban 2025; 50 (1): 99–104. doi: 10.11817/j.issn.172-7347. 2025.240134.
15. Jo U, Kim GH, Kim KR. Reconsideration of the diagnostic criteria for an atypical placental site nodule comparing typical placental site nodule of the uterus: a report of two cases. Int J Gynecol Pathol 2024; 43 (1): 61–66. doi: 10.1097/PGP.000000000000958.
16. Jeremie G, Allias F, Trecourt A et al. Molecular analyses of chorionic-type intermediate trophoblastic lesions: atypical placental site nodules are closer to placental site nodules than epithelioid trophoblastic tumors. Mod Pathol 2023; 36 (1): 100046. doi: 10.1016/j.modpat.2022.100046.
17. Young AN, Lin LH, Abel MK et al. Atypical placental site nodules: clinicopathologic features, management and patient outcomes in an institutional series. Gynecol Oncol 2024; 190 : 215–221. doi: 10.1016/j.ygyno.2024.08.018.
18. Ngan HY, Seckl MJ, Berkowitz RS et al. Diag - nosis and management of gestational trophoblastic disease: 2025 update. Int J Gynaecol Obstet 2025; 171 (Suppl 1): 78–86. doi: 10.1002/ ijgo.70275.
19. Cirstoiu MM, Sajin M, Baros A et al. The role of the ultrasound examination in atypical placental site trophoblastic tumour differential diagnosis and management. A case report. Med Ultrason 2022; 24 (3): 369–371. doi: 10.11152/mu-3149.
20. Lockett G, Thomson AR, Cooper N et al. Ultrasound imaging and hysteroscopy findings in patients referred with atypical placental site nodule to a tertiary gestational trophoblastic centre. Ultrasound Obstet Gynecol 2024; 64 (Suppl 1): 11.
21. Li X, Li Y, Shi X et al. Atypical placental site nodules within the diverticulum of the uterine incision, a rare gestational trophoblastic disease misdiagnosed as intrauterine residue: a case report. Reprod Sci 2024; 31 (2): 555–559. doi: 10.1007/s43032-023-01361-2.
Authors’ contributions
Conceptualization: AB, GP;
Methodology: AB, AN, JSP;
Validation: JAK, JRF, EAJ;
Formal analysis: GYC;
Investigation: LP, AN, JAJ, JRF;
Resources: EAJ;
Data curation: GP, LP, AN, JSP;
Writing – original draft preparation: AB, JAM, NH, RB;
Writing – review and editing: EAJ, SYS;
Visualization: AB, GP, LP, AN, JSP, JAJ, EAJ, GYC, SYC, JRF, NH, RB;
Supervision: JRF, RB;
Project administration: AB.
All authors have read and agreed to the published version of the manuscript.
ORCID of authors
A. Braga 0000-0002-2942-6182
G. Paiva 0000-0003-3856-2116
L. Padrón 0000-0002-7537-6454
A. Nobre 0000-0002-7177-9838
J. S. Pereira 0000-0003-0458-4501
G. Y. Callado 0000-0001-6694-6569
J. Amim Junior 0009-0001-6973-2408
S. Y. Sun 0000-0001-6573-7386
E. Araujo Júnior 0000-0002-6145-2532
J. Rezende-Filho 0000-0002-2193-3374
N. Horowitz 0000-0002-4854-0642
R. Berkowitz 0000-0002-7569-898X
Submitted/Doručeno: 25. 7. 2025
Accepted/Přijato: 5. 8. 2025
Antônio Braga, MD
Maternity School
Federal University
Rua das Laranjeiras, No. 180
Laranjeiras
22240-003 Rio de Janeiro
Brazil
bragamed@yahoo.com.br
Štítky
Dětská gynekologie Gynekologie a porodnictví Reprodukční medicínaČlánek vyšel v časopise
Česká gynekologie
2025 Číslo 6
- Diosmin a hesperidin: Co ukazuje farmakokinetika?
- Diagnostika von Willebrandovy choroby krok za krokem
- Těhotenství a porod u ženy s VWD − kazuistika
- Vědecké poznatky rozptylující obavy spojené s používáním nitroděložní antikoncepce i u mladých žen
- Používání intrauterinních tělísek uvolňujících měď a riziko tubární infertility u nuligravidních žen
Nejčtenější v tomto čísle
- HLA-C a KIR interakce jako možná příčina reprodukčních neúspěchů
- Vliv vybraných imunohistochemických a klinicko-patologických markerů na prognózu pacientek se zhoubným nádorem dělohy
- Podtlaková terapie hojení ran v onkogynekologii – současné poznatky a klinické využití
- Který způsobuje menší bolest? Srovnání misoprostolu a dinoprostonu při indukci porodu
Zvyšte si kvalifikaci online z pohodlí domova
Mazová zátka a její řešení
nový kurzVšechny kurzy