
HIV Knowledge and Attitudes in Healthcare in Slovakia
Authors:
D. Valkovičová Staneková 1
![]() ; S. Wimmerová 2
; S. Wimmerová 2
![]() ; M. Hábeková 2
; M. Hábeková 2
![]()
Authors place of work:
St. Elizabeth University of Health & Social work, Bratislava, Slovakia
1; Slovak Medical University, Bratislava, Slovakia
2
Published in the journal:
Epidemiol. Mikrobiol. Imunol. 75, 2026, č. 2, s. 71-78
Category:
Původní práce
doi:
https://doi.org/10.61568/emi/11-6717/20260323/143210
Summary
Objective: HIV related stigma in healthcare remains one of the biggest obstacles to ending HIV/AIDS epidemy. The aim of the study was to investigate knowledge in HIV prevention/control, behaviours, and discrimination towards people living with HIV (PLWH) among health-care providers in Slovakia. Methods: Slovakia adapted the 2023 ECDC/EACS survey – originally implemented in 54 countries - between 15 September and 5 December 2023. Data were collected via an online anonymous questionnaire and analysed by Chi-square for homogeneity and by Fisher-Freeman-Halton Exact Test. Results: Out of 177 respondents 83.1% were females and 16.9% males. The average age was 43.2 years. The majority were physicians (55.9%) followed by other clinicians (23.7%). A substantial proportion of participants were not aware of having treated any people living with HIV (PLWH) within the past 12 months (72.3%). Most respondents had received training in patients’ informed consent, privacy, and confidentiality (63.3%). Significantly fewer had been trained in equity, diversity, and inclusion (10.2%), infection control (19.8%), HIV stigma and discrimination (9.6%), or post-exposure prophylaxis (PEP) (9.6%). Only 9.6% of respondents had correct knowledge about all three topics: undetectable equals untransmittable (U=U), pre-exposure prophylaxis (PrEP) and PEP; 18.1% had correct knowledge about two of them, 36.7% about one, and 35.6% were not familiar with any. Knowledge about U=U, PrEP, and PEP was significantly associated with the number of PLWH respondents who had interacted with at work in the past 12 months, but showed no significant association with years of healthcare experience or participation in relevant trainings. Fear of occupational transmission did not differ between clinical and non-clinical staff. A notable proportion of respondents (25.4%) expressed a preference to avoid providing care to people who inject drugs, followed by sex workers (12.4%), transgender individuals (7.3%), and men who have sex with men (5.7%). Completing training in all topics did not have a significant impact on concerns about the care and treatment of PLWH. Conclusion: The findings provide an important insight into the scope and forms of HIV-related stigma in healthcare facilities in Slovakia, which should be gradually overcome by raising the visibility of PLWH, a deeper understanding of their problems and their acceptance. Therefore, close cooperation between healthcare workers, lay public, media and non-governmental and for shaping targeted organizations is necessary for reducing fear and prejudice against to PLWH measures and policies to reduce stigma and improve care for PLWH.
Keywords:
Slovakia – healthcare – HIV – Stigma – Knowledge – attitudes
INTRODUCTION
HIV related stigma in healthcare remains one of the biggest obstacles to ending AIDS epidemic. Stigma is defined as a discrediting social difference that results in de valuation or a ‘spoiled social identity’. It occurs in social interactions and is reproduced by existing social inequalities and the exercise of power [1]. Stigma is a well documented barrier to good health, driving delayed care‐seeking, avoidance of clinics, and poor medication adherence, all of which diminish the impact of HIV prevention and treatment programs. To intervene effectively, it is important must understand when, where, and why stigma appears inside healthcare. Recognizing this, UNAIDS has set a clear benchmark: by 2030, fewer than 10 percent of people living with HIV (PLWH) should encounter stigma in any health facility [2].
Since the beginning of the HIV epidemic, Slovakia has been one of the EU Member States with the lowest incidence in Europe. However, in the last decade, there was observed an upward trend in the incidence of new cases and the number of PLWH is also rapidly increasing. In Slovakia from 1985 to 31. 12. 2024, a total of 1 585 HIV cases were registered, from them 1302 were Slovak citizens (1173 men and 129 women). In 2023, a total of 92 new cases of HIV infection were newly diagnosed in Slovakia (from them 72 among Slovak citizens), which represents an incidence of 1.7 cases per 100,000 inhabitants. Since the beginning of the HIV epidemic in Slovakia in 1985, transmission of the infection has dominated in men who have sex with men (MSM) [3]. The first non-governmental organization (NGO) “HIV/AIDS Slovakia” founded by PLWH for patients was registered in Slovakia only in February 2023.
In Slovakia, HIV testing is provided by public health authorities, general practitioners (GPs), STI clinics, and some NGOs. All reactive HIV results must be confirmed at the National Reference Centre for HIV/AIDS Slovak Medical University in Bratislava (NRC). Once a diagnosis is confirmed, patients are referred to one of five specialized HIV/AIDS centers located in infectious disease clinics. While receiving regular care from HIV specialists, PLWH also maintain contact with GPs and other healthcare professionals for unrelated health issues. HIV care in Slovakia is covered under mandatory health insurance; however, even uninsured individuals are entitled to HIV care and antiretroviral treatment by law. Furthermore, healthcare professionals cannot legally refuse care based on a person’s HIV status. After learning their HIV status, PLWH are required to sign an informed consent form confirming that they understand their diagnosis and agree not to transmit the virus to others. They are also required to inform their sexual partners and healthcare professionals about their HIV status. In case of threat or spread of infection, individuals may be subject to prosecution. Unfortunately, Slovakia’s Criminal Code does not reflect current scientific understanding, particularly the principle of undetectable equals untransmittable (U = U). As a result, HIV continues to be stigmatized in both personal and healthcare contexts.
In Slovakia, as in other countries, understanding HIV-related stigma in healthcare requires insight from all individuals working within the health sector, including both clinical and non-clinical staff. Slovakia currently has no nationwide data on how healthcare workers perceive and treat PLWH, even though late diagnosis is common, and fear of stigma is frequently cited as a reason for postponing healthcare-seeking. To address the lack of data on stigma in healthcare, Slovakia adapted the 2023 ECDC/EACS survey – originally implemented in 54 countries to assess knowledge, attitudes, and practices –specifically to reflect its national context [4].
METHODS
This cross-sectional survey, targeting all professionals working in healthcare in Slovakia; (both clinical and non-clinical), was conducted between 15 September and 5 December 2023. Participation was voluntary and based on a non-probability, self-selected sampling approach. A link to the online version of the Slovak version of the ECDC/EACS questionnaire was distributed to health care workers through the Slovak Medical Society (SLS) and the Slovak Chamber of Other Health Workers (SKIZP). Participation in online survey allowed to assess the level of knowledge in HIV prevention/ control, behaviors, and discrimination towards PLWH among health-care workers (HCWs). Answers from Slovak respondents were collected anonymously and analysed using the Chi-square test for homogenity and by Fisher-Freeman-Halton Exact Test, as well as descriptive statistics, to compare responses based on healthcare-related characteristics.
RESULTS
Demographic characteristics
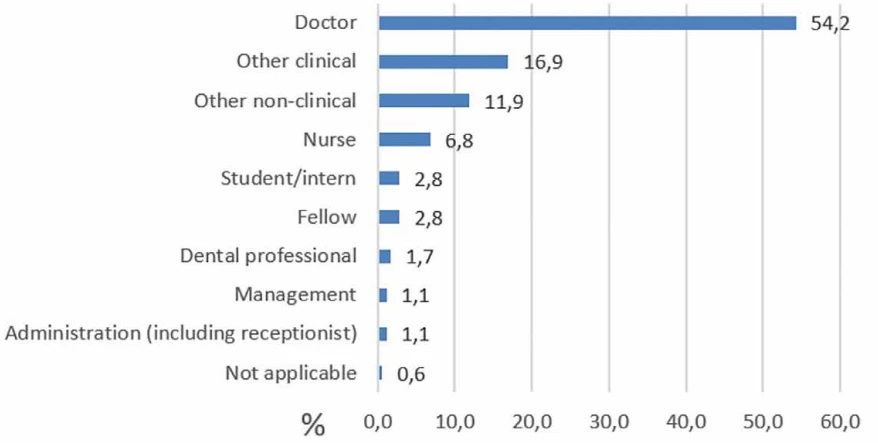
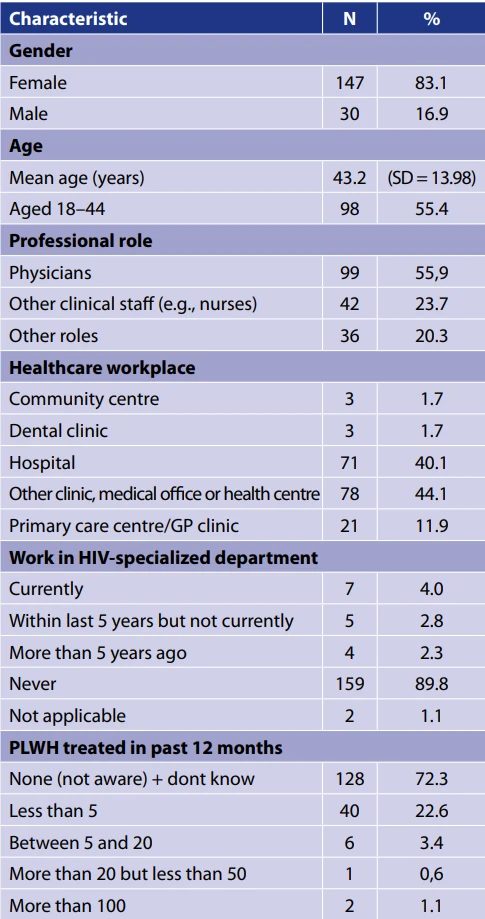
A total of 177 healthcare professionals participated in the survey. The primary characteristics of the surveyed cohort (N = 177) are summarized in Table 1. Most of respondents were females (83.1%), less men (16.9%). Average age of participants (43.2) did not differ between genders. They performed a variety of healthcare roles (Figure 1), although the majority were physicians (55.9%) other clinicians, e.g. nurses (23.7%) (Table 1, Figure 1). Most respondents were working in other clinics, medical offices or health centres (40.1%) and hospitals ( 40.1%), while less were primarily working in HIV specialized department (2.8%) and infection disease departments (1.7%). Most were not aware of having treated any PLWH within the past 12 months (72.3%) or the number of patients treated was less than five (22.6%). Only 1.1% had treated more than 100 PLWH during the past year (Table 1).
HIV training and knowledge
Participants reported whether they had received training in key areas related to HIV and stigma prevention. The majority received training in informed consent, privacy, and confidentiality (63.3%), while fewer had training in infection control (19.8%), equity, diversity, and inclusion (10.2%), HIV stigma and discrimination (9.6%), and post-exposure prophylaxis (PEP) (9.6%). Clinical staff received training in all areas slightly less frequently than others, with a significant difference found only in equity, diversity, and inclusion (p = 0.033). Gender differences were minimal, except that men were significantly less likely than women to have received training on informed consent, privacy, and confidentiality (p = 0.038). Receiving training in all these areas did not significantly affect respondents’ concerns regarding the care and treatment of PLWH.
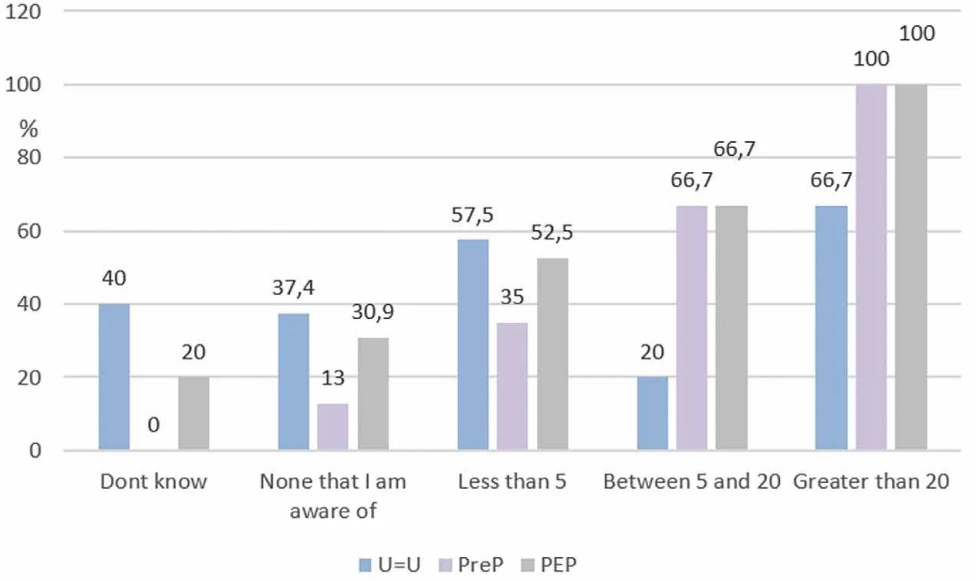
Knowledge was assessed using agreement with three key statements: 42.9% correctly agreed with U = U, 37.9% with the effectiveness of PEP, 20.9% with the preventive use of PrEP (pre-exposure prophylaxis). Only 9.6% of respondents correctly answered all three questions; 18.1% answered two correctly, 36.7% one correctly, and 35.6% answered none correctly. Knowledge levels did not significantly differ by gender, workplace setting, years of healthcare experience, or current professional role. However, men demonstrated significantly higher knowledge about PrEP than women (p < 0.001). Participation in infection control/PEP training did not significantly improve PEP knowledge or
reduce concern about occupational HIV exposure. Notably, respondents who had interacted with more PLWH in the past 12 months had significantly higher knowledge about U = U, PrEP, and PEP (p < 0.176 for U=U, PrEP,
p < 0.001, PEP < 0.001) (Figure 2).
Attitudes and behaviors toward PLWH
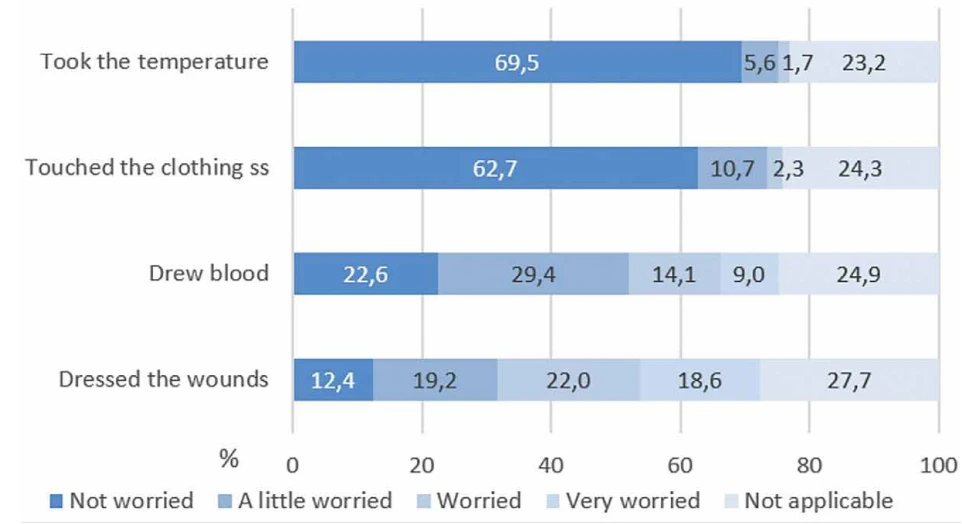
More than half of respondents (59.0%) expressed concern when dressing the wounds of PLWH, with 18.6% reporting being “very worried.” Similarly, 52.6% expressed concern when drawing blood, including 9.0% who were “very worried.” Levels of concern did not significantly differ between clinical and non-clinical staff, and neither previous training nor knowledge about HIV was associated with reduced fear of occupational exposure (Figure 3).
In total, 7.9% of participants reported avoiding physical contact with PLWH, 26.0% used double gloves, and 47.5% wore gloves during all patient interactions. An additional 26.0% reported using special infection-control measures specifically with PLWH. Dentists were significantly more likely to use all these precautions compared to other professionals (p < 0.001). Participants with greater knowledge of PrEP and PEP were less concerned about physical contact (p < 0.001) and less likely to use double gloves (p = 0.017 and p = 0.01, respectively).
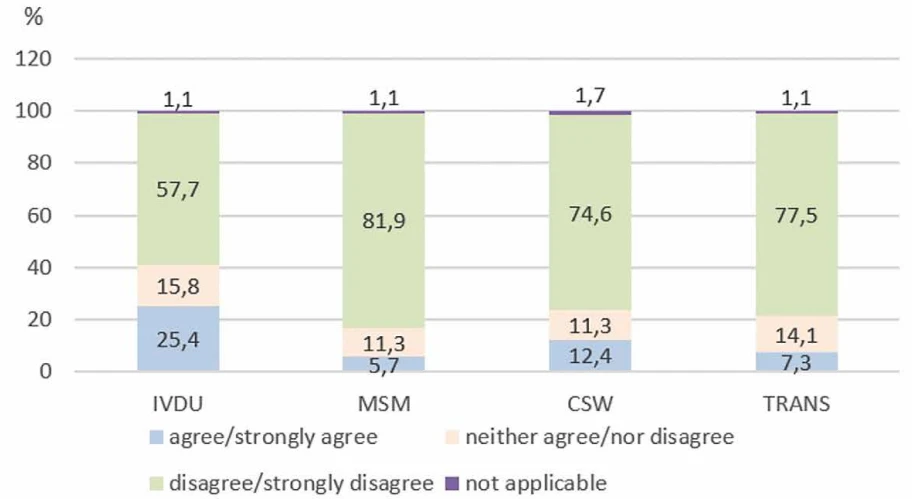
A total of 25.4% of respondents reported a preference to avoid providing care to people who inject drugs (PWID), followed by lower proportions for sex workers (SW) (12.4%), transgenders (TG) (7.3%), and MSM (5.7%). This preference was most pronounced in dental clinics, where 66.7% of respondents reported unwillingness to care for PWID (Figure 4). No significant differences were observed based on gender. However, respondents with training in equity, diversity, and inclusion were significantly more willing to provide care to MSM and PWID (p < 0.001), but less willing to care for SW and TG (p = 0.002). Infection control training was associated with a lower willingness to provide care for
TG (p = 0.011).
Over the past 12 months, 29.9% of respondents observed discriminatory remarks toward PLWH in healthcare settings, with fewer reporting unwillingness to care (16.4%), lower quality of care (12.4%), or disclosure of HIV status without consent (8.5%). Additionally, 26.6% believed HIV is acquired through irresponsible behaviour, 20.9% associated it with excessive sexual partners, and 6.2% believed that PLWH do not care if they transmit HIV. Among the more positive findings of the study, 53.7% of respondents affirmed that PLWH have the right to a fulfilling sexual life, while 56.5% supported the right of women living with HIV to have children. Importantly, only 3.4% of participants perceived HIV infection as a punishment for immoral behavior, and a mere 0.6% expressed the view that PLWH should feel ashamed.
DISCUSSION
Slovakia has one of the lowest HIV incidence rates in the EU but a growing prevalence. As a result, many HCWs in Slovakia rarely encounter PLWH in clinical practice. In our study, although most participants were doctors (55.9%) or other clinical staff (23.7%), 72.3% were not aware of having treated any PLWH in the past 12 months, and those who did mostly treated fewer than five patients (22.6%).
Like the ECDC/EACS survey [4], the most received training among participants was on informed consent, privacy, and confidentiality (65% vs. 63.3%). In contrast, other key topics – such as infection control including PEP (19% vs. 38%), equity and inclusion (14% vs. 35%), and HIV stigma (8.5% vs. 27%) were much less represented in Slovakia [4]. Clinicians had received less training, suggesting that these topics receive insufficient attention in medical education.
Knowledge levels on key prevention concepts – U=U, PEP, and PrEP – were also lower in Slovakia (42.9%, 37.9%, and 20.9%) than both the European average (61%, 56%, and 41%) [5] and Eastern Europe overall (49%, 45%, and 31%) [4]. HIV care providers should generally inform their patients about U=U as part of routine HIV care. Communicating the benefits and risks of treatment is fundamental to patient decision-making, and this benefit of HIV treatment should be no exception [6]. While the ECDC/EACS survey [4] identified predictors of higher knowledge (being male, younger, a medical doctor, or experienced in HIV care), in our study, knowledge did not significantly vary by gender, role, facility type, or years of experience. Just men exhibited significantly greater knowledge regarding PrEP compared to women. However, knowledge improved significantly with the number of PLWH treated in the past year. This suggests that the low knowledge levels in Slovakia are likely linked to limited exposure to HIV care and a lack of related training.
Over half of the respondents expressed concern when providing certain types of care to PLWH, such as dressing wounds or drawing blood. Similarily, in the study in Oman routine tasks, such as dressing wounds, drawing blood and touching clothes, were a cause of concern for 24–52% of HCWs [7]. In our study there was no significant difference between clinical and non-clinical staff, however, dentists reported using precautionary measures more often – though only three dentists participated, so this finding should be interpreted cautiously. Similarly, another study in the HIV community in Slovakia revealed that 31.6% of PLWH who experienced stigmatization were primarily rejected by dentists and other medical professionals [8]. Czech study, 41% of the respondents had been refused dental care at some point in the past because of their HIV-positive status [9]. A Dutch study found similar trends: HCWs with limited experience reported fear of occupational HIV infection and often took unnecessary precautions [10]. In our study, participation in training did not reduce concerns, but better knowledge of PrEP and PEP was linked to lower fear of physical contact and less frequent use of double gloves. This highlights the role of education in reducing stigma and improving infection control practices.
Among key populations, PWID were the group HCWs most often preferred not to treat. Some trainings had a significant effect – positive or negative – on attitudes toward volnurable groups, including MSM, SW, TG and PWID. However, due to small sample sizes, it was not possible to determine specific reasons for these preferences, and these results require further research. These findings indicate persistent stigma and societal bias in Slovakia toward marginalised groups such as LGBT (lesbian, gay, bisexual, and transgender) individuals [11]. Biases in care preferences risk undermining equitable healthcare. Key populations that have higher HIV prevalence, such as MSM, PWID, TG and SW, experience additional stigma and discrimination based on their behaviour and identities. This contributes to the concentrated HIV epidemics seen in these populations in many CEE countries [12]. In our study no significant differences were observed based on gender in preferences and attitudes toward providing care for key populations. In Dutch study younger age, male gender, and surgical specialties were linked to higher stigma; training on stigma was associated with lower stigma [13]. As suggested in the literature, addressing stigma requires more than medical knowledge – it demands education that explicitly addresses discrimination and bias.
Additionally, stigma and low awareness also affect HIV testing uptake. As noted by Schweitzer et al. 2023 [12], stigma and intersectional discrimination in Central and Eastern Europe reduce engagement with testing and care services. The authors emphasize the need for evidence-based strategies to tackle stigma, which could improve not only the lives of PLWH, but also reduce HIV transmission and address growing epidemics in the region.
HIV-related stigma in healthcare is a well-documented barrier to care. In our study, 12.4–29.9% of respondents had observed stigmatising behaviour in their workplaces in the past year. This aligns with findings from a Czech study, where total of 27% of the respondents admitted having been denied or suspended health care, 44% reported inappropriate comments from healthcare workers, and 32% of the respondents avoided visiting the healthcare facility [8]. In a multi-country study, 17% of PLWH reported discrimination from HCWs, especially dentists, general practitioners, and gynecologists [14]. A review of literature from 2012–2023 confirmed that stigma negatively affects antiretroviral therapy (ART) adherence, retention in care, and virologic suppression, especially among young people [15].
Our study also found that stigmatising beliefs persist. Over 25% of respondents believed HIV is a result of irresponsible behaviour, and over 50% agreed that people with detectable viral loads should avoid sexual activity. Such views can influence the quality of care and advice provided. On the positive side, over half agreed that PLWH have the right to fulfilling sexual lives and that women with HIV should be allowed to have children. These views likely reflect awareness of effective prevention of vertical transmission, as according to information from the NRC, no HIV-positive child has been born in Slovakia to date.
Overall, although the sample of respondents we monitored represents only a small part of the number of people working in healthcare in Slovakia in 2023, our findings indicate the urgent need to improve HIV-related education in Slovakia, not only in clinical knowledge but also in addressing stigma and discrimination. Training programmes should be expanded to include all health professions and focus on equitable, compassionate care for all, especially key populations. Efforts should be made through inter-sectoral collaboration to ensure that all existing UNAIDS recommendations to combat stigma against people living with HIV in the country are adopted and implemented [16]. Ending HIV-related stigma and discrimination requires a multi-faceted approach involving individual actions, community engagement, and policy changes. It involves challenging negative attitudes, promoting education, and ensuring access to rights and services for PLWH [17].
CONCLUSION
Although the study sample does not represent the entire healthcare sector, the findings suggest that improving education about HIV alone is not sufficient to reduce prejudice and stigma in healthcare settings in Slovakia. Stigma-reduction training should be more included in ongoing education for HCWs. An anonymous hotline or website could help patients and staff report discrimination safely. Involvement of patient organizations in education is important for raising the visibility of PLWH, a deeper understanding of their problems and their acceptance. Therefore, close cooperation between HCWs, lay public, media and NGOs is necessary for reducing fear and prejudice against to PLWH and other vulnerable groups in Slovakia and for shaping targeted measures and policies to reduce stigma and improve care for PLWH.
Acknowledgements
The authors would like to thank the members of the ECDC/EACS Steering Group for the opportunity to involve Slovakia in the ECDC/ EACS Stigma Survey, especially Teymur Nori, Ana Mendez-Lopez and Esteban Martinez, who oversaw the development of this survey and provided guidance throughout the development of this project. Thanks also go to the Slovak Medical Association (SLS) and the Slovak Chamber of Other Healthcare Professionals (SKIZP) for distributing the online questionnaire to individual professional societies, as well as to all respondents for their willingness and time to complete the questionnaire.
Zdroje
1. Goffman, E. Stigma. Notes on the management of spoiled identity. PENGUIN BOOKS. Copyrighted Material. PENGUIN CLASSICS. UK. Available on www:<https://cdn.penguin.co.uk/dam-assets/
books/9780241548011/9780241548011-sample.pdf.
2. UNAIDS: The AIDS epidemic can be ended by 2030 with your help. UNAIDS, 2016. Available on www:<https://www.unaids.org/sites/default/files/media_asset/UNAIDS_with your-help_en.pdf.
3. UVZ: Výročná správa o činnosti úradov verejného zdravotníctva SR podľa jednotlivých odborov verejného zdravotníctva za rok 2023, UVZ, 2024. Available on www: <https://www.uvzsr.sk/
documents/d/uvz/vs-ruvz-za-rok-2024-pdf.
4. ECDC: HIV stigma in the healthcare setting Monitoring implementation of the Dublin Declaration on partnership to fight HIV/AIDS in Europe and Central Asia, ECDC, 2024. Available on www: < https://www.ecdc.europa.eu/en/publications-data/hiv-stigma-healthcare-setting-monitoring-implementation-dublin-declaration.
5. Mendez-Lopez A, Burns F, Sullivan A, Deogan Ch. et al. Knowledge about biomedical HIV prevention among healthcare workers: A cross-sectional study in Europe and Central Asia. HIV Med , 2025. DOI: 10.1111/hiv.70048.
6. Calabrese SK, Mayer KH. Providers should discuss U=U with all patients living with HIV. Lancet HIV, 2019 Apr;6(4):e211-e213. DOI: 10.1016/S2352-3018(19)30030-X. Epub 2019 Feb 13.
7. Shah S, Elgalib A, Al-Wahaibi A, Al-Fori M et al. Knowledge, Attitudes and Practices Related to HIV Stigma and Discrimination Among Healthcare Workers in Oman. Sultan Qaboos Univ Med J, 2020;20(1):e29–e36. DOI: 10.18295/squmj.2020.20.01.005.
8. Sojak L, Simekova K, Piesecka L, Wiesinger M et al. Attitudes and Perspectives of People Living with Human Immunodeficiency Virus: Findings From the Positive Perspectives Survey in Slovakia. International Journal of Public Health, 2021, 66. DOI: 10.3389/ijph.2021.642869.
9. Kubátová A, Fialová A, Stupka J, Malý M et al. Stigmatization and discrimination of people living with hiv in the Czech Republic: a pilot Study. Cent Eur J Public Health, 2023; 31(3):210–216. DOI:
10.21101/cejph.a7782.
10. Sarah J. Healthcare workers’ perceptions and practices in the care of people living with HIV in the Netherlands. BMC Health Services Research, 2014, 231. DOI: 10.1155/2020/1098109.
11. Kohútová S. Growing Intolerance Towards LGBTQ+ Minorities in Slovakia. Euro Prospects, 2024. Available on www:<https://europrospects.eu/slovakias-growing-intolerance-towards-lgbtq-minorities/
12. Schweitzer AM, Dišković A, Krongauz V, Newman J et al. Addressing HIV stigma in healthcare, community, and legislative settings in Central and Eastern Europe. AIDS Research and Therapy, 2023, 20(1):87. PMID: 38082352; PMCID: PMC10714556. DOI: 10.1186/s12981-023-00585-1.
13. Jordans M. Factors associated with HIV stigma among healthcare workers in Dutch hospitals: A cross-sectional study. Journal of Infectious Diseases, 2024, 230(4), 567–574. DOI: 10.1177/2325958224128258.
14. Nöstlinger, C, Castro DR, Platteau T, Dias S et al. HIV-related discrimination by health professionals across 14 European countries: A multicountry study. AIDS Care, 2023, 35(2): 204–212. DOI:
10.1089/apc.2013.0247.
15. Perger, T., Davtyan, M., Foster, C. et al. Impact of HIV-Related Stigma on Antiretroviral Therapy Adherence, Engagement and Retention in HIV Care, and Transition to Adult HIV Care in Pediatric and Young Adult Populations Living With HIV: A Literature Review. AIDS Behav, 2025, 2 : 497–516. DOI: 10.1007/s10461-024-04534-5.
16. UNAIDS: Evidence for eliminating HIV-related stigma and discrimination [Internet]. Geneva: UNAIDS; 2020 [cited 2023 Jan 16]. Available on www: <https://www.unaids.org/sites/default/files/media_asset/eliminating-discrimination guidance_en.pdf.
17. UNAIDS. Practical guide to ending HIV-related stigma and discrimination — Best practices and innovative approaches to reduce stigma and discrimination at the country level. UNAIDS,2023. Available on: <https://www.unaids.org/en/resources/documents/2023/GlobalPartnershipStigmaDiscrimination_PracticalGuide.
Štítky
Hygiena a epidemiologie Infekční lékařství MikrobiologieČlánek vyšel v časopise
Epidemiologie, mikrobiologie, imunologie

- Perorální antivirotika jako vysoce efektivní nástroj prevence hospitalizací kvůli COVID-19 − otázky a odpovědi pro praxi
- Parazitičtí červi v terapii Crohnovy choroby a dalších zánětlivých autoimunitních onemocnění
- Vakcíny proti klíšťové encefalitidě
- Kdy je nejlepší očkovat
Nejčtenější v tomto čísle
- Serious tick-borne infections – considering the strengths and weaknesses of currently used laboratory diagnostic methods
- Rare transmission of hepatitis A virus through blood transfusion products
- Factors influencing the presence of Klebsiella pneumoniae and Klebsiella oxytoca species complexes in the developing gut microbiota
- The impact of the COVID-19 pandemic on the incidence of invasive pneumococcal disease in the Czech Republic and whole genome sequencing analysis of Streptococcus pneumoniae serotypes 3 and 19A from 2018–2024
Zvyšte si kvalifikaci online z pohodlí domova
Mazová zátka a její řešení
nový kurzVšechny kurzy