
CHANGE OF SURGICALLY INDUCED CORNEAL ASTIGMATISM AND POSITION OF ARTIFICIAL INTRAOCULAR LENS OVER TIME
Authors:
I. Popov; J. Juhas; K. Kopálová; V. Krásnik
Authors place of work:
Klinika oftalmológie LF UK a UN Bratislava
Published in the journal:
Čes. a slov. Oftal., 79, 2023, No. 2, p. 88-93
Category:
Původní práce
doi:
https://doi.org/10.31348/2023/14
Summary
Aims: To analyze changes in surgically induced corneal astigmatism and articial intraocular lens (IOL) stability over time following cataract surgery. To compare the interchangeability of measurements between an automatic keratorefractometer (AKRM) and a biometer.
Material and methods: In this prospective observational study, the above-mentioned parameters were collected from 25 eyes (25 subjects) on the first day, first week, first and third month after uncomplicated cataract surgery. We used IOL-induced astigmatism (difference between refractometry and keratometry) as an indirect indicator of IOL stability change. We used the Blant-Altman method to analyze consistency between devices.
Results: At the above time points, surgically induced astigmatism (SIA) decreased as follows: 0.65 D; 0.62 D; 0.60 D and 0.41 D (in the first day, week, month and third month respectively). Astigmatism induced by changes of the position of the IOL varied as follows: 0.88 D; 0.59 D; 0.44 D and 0.49 D. Changes in both parameters were statistically significant (p<0.05). Neither the measurements of the astigmatism value nor the astigmatism angle showed a statistically significant difference between the devices (p>0.05).
Conclusion: Both surgically induced astigmatism and astigmatism induced by IOL decreased over time, in which both changes were statistically significant. The decrease in SIA was most pronounced between the first and third month after surgery. For IOL-induced astigmatism, the greatest decrease was within the first month after surgery. The differences in measurement between the biometer and AKRM were statistically insignificant, but the clinical interchangeability between the given methods is questionable, especially with regard to measurement of the astigmatism angle.
Keywords:
surgically induced astigmatism – intraocular lens position – astigmatism change over time
INTRODUCTION
The cornea forms approximately two thirds [1] of the entire refractive power of the eye, and in the Caucasian population it measures an average of 11.96 cm horizontally (“white to white”), while in the vertical dimension it is smaller. Its average dioptric power is 44.3 D and average astigmatism is 0.91 D [2].
However, these parameters may be influenced by intervention with the integrity of the cornea, for example by incision during cataract surgery, which may cause changes to corneal curvature. The quantification of these changes is expressed under the title of surgically induced astigmatism (SIA). This is defined as the difference between postoperative and preoperative astigmatism, and can be measured either with the aid of manifest refraction or analysis of corneal curvature [1]. Cataract surgery is the most frequently performed operation in ophthalmology [3]. Surgically induced astigmatism caused by corneal incisions is a very important factor influencing the postoperative result and patient satisfaction. It is assumed that temporal incisions cause lesser SIA than superior incisions, and that the degree of SIA may also be influenced by the length, shape and width of the incision [4]. It is necessary to reckon with the degree of SIA in the calculation of the artificial intraocular lens (IOL) in biometry. Healing of the cornea is a dynamic process [5]. This is also linked to change of SIA over time. It is important to know the stabilisation of postoperative astigmatism, whether this is for the purpose of correct timing of the final postoperative correction, or in the case of further planning of treatment and diagnosis of the ocular pathology. Besides the cornea, postoperative astigmatism is also influenced by astigmatism induced by an artificial intraocular lens (IOL-induced astigmatism). Monofocal non-toric lenses may also induce astigmatism due to their tilt or decentration. Tilt is manifested most pronouncedly upon instability of the IOL in the capsule, which may occur in the early postoperative period, until the IOL becomes stabilised by adhesion of the capsule. For this reason, in our study we decided to observe the change of SIA and IOL-induced astigmatism over time, following standard cataract surgery with the implantation of a monofocal IOL. In the postoperative period an automatic keratorefractometer (AKRM) is often used at postoperative follow-up examinations for measuring refraction and corneal astigmatism. Occasionally situations also occur (for example opacity of the optic media) in which it is not possible to measure corneal astigmatism with a biometer, and it is thus necessary to supplement data from an AKRM. As a result, we decided also to compare the precision of agreement of keratometry between a biometer and an automatic keratorefractometer.
MATERIAL AND METHOD
In our prospective study we observed the development of astigmatism in the form of SIA and IOL-induced astigmatism over time in patients who were planned for standard cataract surgery with the implantation of an IOL into the capsule. Before the operation, biometry was performed on each patient with the aid of the optical biometer Lenstar LS900 (Haag-Streit AG, Koeniz, Switzerland). The cohort included only patients without irregular astigmatism, who had not undergone any previous eye operations and were without any known or newly discovered corneal pathology such as keratoconus, corneal scars, dry eye syndrome and others. We selected values of beneath 2.0 D of astifmatism and less than 47.0 D as the steepest value of keratometry (Steep K) as the safe limit in order to exclude ectatic corneal diseases. Patients with symptoms of pterygium were also excluded from observation. The patients were all operated on by the same surgeon, using a uniform technique. The main 2-degree corneal incision with a width of 2.75 mm was located at no. 12 on the clock face. Two paracenteses with a width of 1 mm were located at numbers 10 and 2. The artificial intraocular lens was placed in the capsule following uncomplicated cataract surgery with the aid of phacoemulsification and bimanual irrigation and aspiration. A single-piece MD Tech I-stream hybrid IOL with a quadrilateral shape, made of hybrid (hydrophobic and hydrophilic) acrylic material, was implanted. At the end of the operation, the paracenteses were sealed by hydration. It was not necessary to hydrate the main incision in any of the patients. On the next postoperative day, the patients were also examined in mydriasis using a slit lamp. Decentration of the IOL was evaluated visually. We did not observe pronounced decentration of the IOL in any of the patients, and all of them had the edge of the optical part of the IOL covered circularly with capsulorhexis. If the cornea was without visible signs of edema, the patients were included in the further analyses. If both eyes were operated on, and provided that it met the inclusion criteria, only the right eye of the patient was included in the analysis. All patients were examined on the first day, the first week, the first month and the third month after surgery. In order to ensure the most precise possible analysis, the change of astigmatism was observed with the aid of the same Lenstar LS900 optical biometer also in the postoperative period. During the follow-up examinations, the patients also underwent an examination with an AKRM (Nidek AKR-1a). We calculated surgically induced astigmatism with the aid of a vector analysis according to the formula mentioned in the article by Sánchez-Taberner [6]. For quantification of the influence of IOL-induced astigmatism, we used the absolute values of the difference between refractometry and keratometry from the AKRM. We displayed the results as the average observed quantities, with minimum and maximum values. The data in the values of SIA and IOL-induced astigmatism manifested deviations from normal distribution, and as a result we used a Friedman non-parametric test for comparison of the averages from repeated measurements. For the post-hoc analysis we used the Bonferroni correction. For evaluation of the concordance of the results of keratometry between the biometer and the AKRM from the third month after surgery, we used the Blant-Altman method [7]. We stipulated the level of alpha significance at 0.05. We converted astigmatisms from keratometry to values that were compatible with the imaging of astigmatism in biometry, and in the calculation we displayed the values within a range from 270° to 90°, in which we indicated the given values from -90° to +90° (Fig. 1). In order to exclude methodical errors, we manually checked and adequately corrected differences greater than 90°. For example, at an angle of 80° and 100°, following conversion we arrived at 80° and -80°, which makes a difference of 160°, whereas the actual difference is only 20°. In our study we adhered to the principles of the Helsinki declaration.

RESULTS
The data was analyzed from 25 out of 30 patients. Five patients did not complete the observation due to contracting COVID-19 or for other health reasons. The analysed cohort contained 6 men and 19 women. The descriptive statistics of the cohort and the development of SIA over time are illustrated in Table 1.
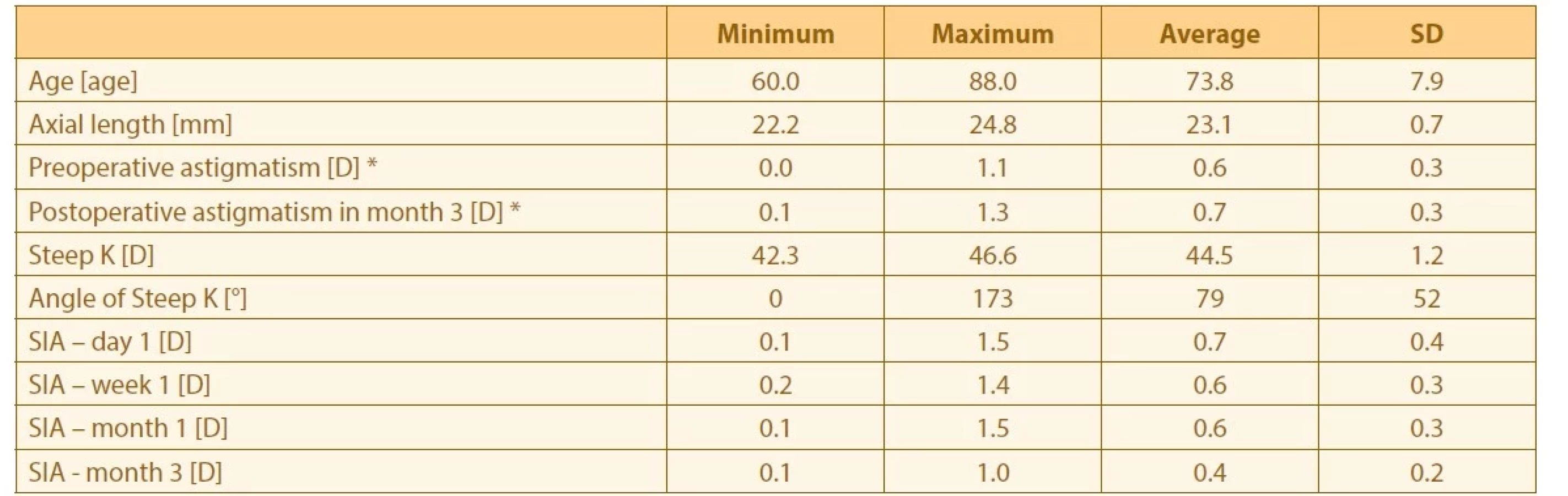
SIA – Surgically Induced Astigmatism
SD – Standard Deviation
* Corneal Astigmatism measured with the Lenstar LS900
SIA in individual time periods compared among themselves. The differences between the individual points in time were statistically significant (p < 0.05). A final decrease by 0.23 D was observed, which in some cases may be clinically significant. Surgically induced astigmatism decreased over time, in which the most pronounced decrease occurred between the first and the third month. Change of SIA over time is illustrated in Graph 1.

We also conducted a post-hoc analysis using a Wilcoxon text with Bonferroni correction. A statistically significant difference in SIA was recorded in the post-hoc analysis between the first day and the third month (p < 0.05), and also between the first and third months (p < 0.05). Values of significance are presented following the application of the Bonferroni correction. The other differences were statistically insignificant.
The development of the value of postoperative refractometry stated in the spherical equivalent is illustrated in Table 2.

SE – Spherical Equivalent
Refractometry initially recorded a slight myopic shift up to the first postoperative week, whereas the opposite trend appears between the first and third postoperative months. These changes are associated with change of SIA and also with change in the position of the IOL, in which it is not possible to differentiate the effect of the two phenomena solely on the basis of these values. The development of the change of refractometry was not statistically significant (Friedman test, p > 0.05).
We presented the influence of IOL on the overall value of astigmatism as the difference between overall and corneal astigmatism. The development of this value is illustrated in Table 3. The difference in the development of astigmatism was statistically significant (Friedman test, p < 0.05), specifically between the first day and the first month (p = 0.018, post-hoc analysis with Bonferroni correction).

We analyzed the interchangeability of the keratometry values from the biometer and the AKRM with the aid of the Blant-Altman method. We analysed the values of the height of astigmatism and its angle separately. The average differences in the measurements and limits of agreement between them are illustrated in Table 4.

SD – Standard Deviation
The values of the height of astigmatism showed a statistically insignificant difference between the measurements (p = 0.80). The average difference between the values of astigmatism between the instruments was very small (0.0 ± 0.3 D). Lenstar overestimated the value of the angle by 9 ± 22°. The interchangeability of the measurements is illustrated in Graph 2, where we can see that two values are located outside of the 95% interval of agreement. In the case of the angle of astigmatism, the difference between the measurements was also statistically insignificant (p = 0.06). The correlation of the measurements is presented in Graph 3. We considered the range of the limit of agreement between the measurements of angle of astigmatism (86°) to be very broad, and for this reason we analyzed whether greater imprecisions of measurements occur in the case of higher astigmatisms. We did not find any significant correlation between the degree of the astigmatism and the difference in the measurements of its angle (p = 0.43; Pearson correlation coefficient r = 0.16).


DISCUSSION
In our study we observed a number of quantities in connection with the anatomical restructuring of surgical wounds and other ocular structures following uncomplicated cataract surgery. The main focus was on observing changes in corneal curvature following surgical incisions over time in the form of SIA. It ensues from the results that in terms of refraction, we cannot consider the process of healing to be complete even one month after surgery. In his study, Qin He observed a statistically insignificant decrease of SIA between the first and sixth months after surgery by 0.1 D [8]. In our study we observed a significant decrease of SIA, and the size of the decrease in our study was also larger between the first and third month (0.2 D). In Qin’s study a 2.2 mm incision was used, which may have caused an overall lower SIA and a smaller decrease thereof. On the basis of Qin He’s study it is possible to assume that the decrease of SIA between the third and sixth month is negligible, and we would not expect any further significant decrease also in our own cohort. A study conducted by Theodoulidou observed a decrease of SIA between the first and the sixth month from 0.3 to 0.12 D [9]. A similar time frame of observation was chosen in the study conducted by Rainer [10], which however observed a temporal and superotemporal incision with a width of 3 mm. In the case of a temporal incision, they observed a decrease of SIA by 0.3 D between the first week and the third month, which is more than in our observation (we recorded a decrease by 0.21 D). However, in the case of a superotemporal incision they in fact recorded an increase by 0.1 D within the given period of time. In our study we observed the greatest decrease between the first and third months. Up to the first month the development of astigmatism was virtually unchanged. A similar phenomenon was observed by Liang in the case of a 2.2 mm and also a 3.0 mm incision, in which a more pronounced decrease of SIA also occurred up to the third month, specifically by 0.08 D in the 2.2 mm incision and by 0.2 D in the 3.0 mm incision [11].
Alteration of the position of the IOL may cause various aberrations such as defocus, astigmatism, coma and other higher-order aberrations. Tilt of up to 2–3° and decentration up to 0.2–0.3 mm are clinically insignificant in the case of virtually all types of IOL [12]. Monofocal spherical IOLs have a lesser influence on these aberrations upon alteration of the position of the IOL in comparison with aspherical, toric or multifocal IOLs [13]. Tilt and decentration of the IOL occur upon a background of various different factors. These include for example the natural tilt of the patient’s own original lens [14], asymmetrical fixation of the IOL in the capsule (part in the capsule, part in the sulcus) and crack in the capsule [12]. While a long axial length, thick lens and large or decentred capsulorhexis mainly cause decentration, previous pars plana vitrectomy, short axial length, incomplete coverage of the optics of the IOL capsule and capsular fibrosis mainly cause tilt [15-17]. For example, in the case of an aspherical monofocal IOL, horizontal tilt causes astigmatism against the rule. At a 5° tilt it causes 0.14 D and at 10° this is 0.56 D in the case of a 28 D IOL [18]. In our study we attempted to eliminate factors associated with capsulorhexis by selecting patients in whom we had excluded decentred capsulorhexis and capsulorhexis without complete coverage of the optics. Although we calculated the influence of the lens only on the basis of the difference between overall refraction and keratometry, it was not possible to differentiate the influence of tilt from decentration, and in addition we only assessed the influence on astigmatism, in which higher-order aberrations were not analyzed. From the results (Table 3) it is evident that the greatest decrease of IOL-induced astigmatism occurs between the first day and the first week, and the subsequent decrease up to the third month is more gradual. This more pronounced decrease is significant between the first day and the first month (p = 0.018). This is probably connected with the formation of adhesions of the IOL with the capsule in the early postoperative period, which is in accordance with the theory that complete capsular adhesion takes effect in the case of acrylic IOLs already on the 11th postoperative day [19]. In highly myopic eyes this time is extended [20], although this type of eye was not present in our cohort.
Upon a comparison of the agreement in measurements of the degree of astigmatism with the aid of AKM and biometry, we observed statistically insignificant differences (p = 0.8). The differences between the instruments upon measurement of the angle of astigmatism were also statistically insignificant, if only suggested (p = 0.06). In their study, Hashemi et al. observed a relatively good agreement in the measurement of degree of astigmatism by AKM with Lenstar, which is in accordance with our own observations. However, the agreement between the instruments improved in their study upon the application of correction from the regression formula from their analysis [21]. On the other hand, our results are not in accordance with Altınel’s study or with Hashemi’s second study, though this was conducted on children [22,23]. Despite our observation of a statistically insignificant difference between the instruments upon measurement of the degree of astigmatism, a question remains as to whether the range of agreement (1.0 D) is clinically acceptable. Acceptability may only be assessed individually. Agreement in the angle of astigmatism was not compared in any of the above-mentioned studies, even though in Hashemi’s study on children an astigmatism vector analysis was conducted, which contains information about the power and angle of astigmatism. In this case, it is difficult to differentiate between the two quantities in the analysis. In our study we compared a broad interval of limits of agreement from a clinical perspective upon a comparison of measurement of the angle of astigmatism (86°). Here it is also questionable as to whether such a broad interval of agreement is clinically acceptable, since it now approaches 90°, which completely alters astigmatism. The size of the differences in the measurements of the angle did not correlate with the height of astigmatism (p=0.43; r = 0.16).
Our study illustrated the development of corneal astigmatism upon the healing of incisions following cataract surgery over time. It also indirectly observed stabilization of the IOL within the lens capsule. An advantage is the homogeneous cohort of patients operated on by a single surgeon with one type of IOL and the same technique. A potential drawback of the study may be that upon evaluation of the development of astigmatism we did not measure the length of the incision, which may influence healing and SIA. In addition, upon changes of position of the IOL, higher-order aberrations and the actual change of position of the IOL were not measured.
This study has not been submitted to any other journal or published elsewhere. The authors of the study declare that no conflict of interests exists in the compilation, theme and subsequent publication of this professional communication, and that it is not supported by any pharmaceuticals company.
Received: November 8, 2022
Accepted: January 23, 2023
Available on-line: March 30, 2023
MUDr. Mgr. Ivajlo Popov Ph.D, MPH, FEBO
Klinika oftalmológie LF UK a UN Bratislava
Ružinovská 6
82101 Bratislava
E-mail: ivajlo.popov@gmail.com
Zdroje
1. Azar D. Refractive Surgery. Elsevier, 2019.
2. Popov I, Waczulikova I, Stefanickova J, et al. Analysis of biometric parameters of 2340 eyes measured with optical biometer Lenstar LS900 in a Caucasian population. Eur J Ophthalmol. 2021; 1120672121998920.
3. Acosta R, Hoffmeister L, Román R, Comas M, Castilla M, Castells X. Systematic review of population-based studies of the prevalence of cataracts. Arch Soc Espanola Oftalmol. 2006;81 : 509-516.
4. Marek R, Klus A, Pawlik R. Comparison of surgically induced astigmatism of temporal versus superior clear corneal incisions. Klin Oczna. 2006;108 : 392-396.
5. Kamil S, Mohan RR. Corneal stromal wound healing: Major regulators and therapeutic targets. Ocul Surf. 2021;19 : 290-306.
6. Sánchez-Tabernero S. SIA-formula: an easy way to calculate surgically induced astigmatism. Eye. 2018;32 : 659-660.
7. Bland JM, Altman DG. Measuring agreement in method comparison studies. Stat Methods Med Res. 1999;8 : 135-160.
8. He Q, Huang J, He X, Yu W, Yap M, Han W. Eect of corneal incision features on anterior and posterior corneal astigmatism and higher-order aberrations after cataract surgery. Acta Ophthalmol (Copenh). 2021;99:e1027-e1040.
9. Theodoulidou S, Asproudis I, Kalogeropoulos C, Athanasiadis A, Aspiotis M. The role of sideport incision in astigmatism change after cataract surgery. Clin Ophthalmol Auckl NZ. 2015;9 : 1421-1428.
10. Rainer G, Menapace R, Vass C, Annen D, Findl O, Schmetterer K. Corneal shape changes after temporal and superolateral 3.0 mm clear corneal incisions. J Cataract Refract Surg. 1999;25 : 1121-1126.
11. Liang JL, Xing XL, Yang XT, Jiang YF, Zhang H. [Clinical comparison analysis in surgically induced astigmatism of the total, anterior and posterior cornea after 2.2-mm versus 3.0-mm clear corneal incision cataract surgery]. Zhonghua Yan Ke Za Zhi Chin J Ophthalmol. 2019;55 : 495-501.
12. Ale JB. Intraocular lens tilt and decentration: a concern for contemporary IOL designs. Nepal J Ophthalmol Biannu Peer-Rev Acad J Nepal Ophthalmic Soc NEPJOPH. 2011;3 : 68-77.
13. Ashena Z, Maqsood S, Ahmed SN, Nanavaty MA. Effect of Intraocular Lens Tilt and Decentration on Visual Acuity, Dysphotopsia and Wavefront Aberrations. Vision. 2020;4 : 41.
14. Kimura S, Morizane Y, Shiode Y, et al. Assessment of tilt and decentration of crystalline lens and intraocular lens relative to the corneal topographic axis using anterior segment optical coherence tomography. PloS One. 2017;12:e0184066.
15. Chen X, Gu X, Wang W, et al. Characteristics and factors associated with intraocular lens tilt and decentration after cataract surgery. J Cataract Refract Surg. 2020;46 : 1126-1131.
16. Uzel MM, Ozates S, Koc M, Taslipinar Uzel AG, Yılmazbas P. Decentration and Tilt of Intraocular Lens after Posterior Capsulotomy. Semin Ophthalmol. 2018;33 : 766-771.
17. Ding X, Wang Q, Xiang L, Chang P, Huang S, Zhao Y-E. Three-Dimensional Assessments of Intraocular Lens Stability With High-Speed Swept-Source Optical Coherence Tomography. J Refract Surg Thorofare NJ. 1995 2020;36 : 388-394.
18. Weikert MP, Golla A, Wang L. Astigmatism induced by intraocular lens tilt evaluated via ray tracing. J Cataract Refract Surg 2018;44 : 745-749.
19. Hayashi H, Hayashi K, Nakao F, Hayashi F. Elapsed time for capsular apposition to intraocular lens after cataract surgery. Ophthalmology. 2002;109 : 1427-1431.
20. Zhao Y, Li J, Lu W, et al. Capsular adhesion to intraocular lens in highly myopic eyes evaluated in vivo using ultralong-scan-depth optical coherence tomography. Am J Ophthalmol. 2013;155 : 484 - 491.e1.
21. Hashemi H, Asgari S, Miraftab M, Emamian MH, Shariati M, Fotouhi A. Agreement study of keratometric values measured by Biograph/ LENSTAR, auto-kerato-refractometer and Pentacam: decision for IOL calculation. Clin Exp Optom. 2014; 97 : 450-455.
22. Altınel MG, Uslu H. Agreement of keratometric readings measured using rotating Scheimpflug imaging, auto-refractokeratometer, and biograph in eyes with keratoconus. Int Ophthalmol. 2021;41 : 1659-1669.
23. Hashemi H, Heydarian S, Khabazkhoob M, Yekta A, Emamian MH, Fotouhi A. Keratometry in children: Comparison between auto-refractokeratometer, rotating scheimpflug imaging, and biograph. J Optom. 2019;12 : 99-110.
Štítky
OftalmologieČlánek vyšel v časopise
Česká a slovenská oftalmologie

2023 Číslo 2
- Selektivní laserová trabekuloplastika nesnižuje nitroční tlak více než argonová laserová trabekuloplastika
- Progresi glaukomu je třeba hodnotit strukturálními i funkčními parametry
- Ztráta centrálního vidění po filtrujících operacích glaukomu
- Od PGF-2 alfa-isopropyl esteru k latanoprostu: přehled vývoje Xalatanu
- Compliance u pacientů s glaukomem
Nejčtenější v tomto čísle
- FORMS OF OCULAR LARVAL TOXOCARIASIS IN CHILDHOOD. A REVIEW
- CHANGE OF SURGICALLY INDUCED CORNEAL ASTIGMATISM AND POSITION OF ARTIFICIAL INTRAOCULAR LENS OVER TIME
- VISUAL OUTCOMES, CONTRAST SENSITIVITY, AND SATISFACTION WITH MULTIFOCAL INTRAOCULAR LENS BLENDED TECHNIQUE: LATE MID-TERM RESULTS
- CENTRAL CORNEAL THICKNESS AND INTRAOCULAR PRESSURE CHANGES POST- PHACOEMULSIFICATION SURGERY IN GLAUCOMA PATIENTS WITH CATARACT
Zvyšte si kvalifikaci online z pohodlí domova
Mazová zátka a její řešení
nový kurzVšechny kurzy