
Usage of shear wave elastography for diagnosis of changes of oculomotor muscles in endocrine orbitopathy
Authors:
M. Zemanová
Authors place of work:
Oční klinika FN a LF MU, Brno přednosta prof. MUDr. Eva Vlková, CSc.
Published in the journal:
Čes. a slov. Oftal., 75, 2019, No. 1, p. 14-24
Category:
Původní práce
doi:
https://doi.org/10.31348/2019/1/2
Summary
Background: Shear wave elastography (SWE) is an imaging modality using advantage of ultrasound to detect differences of elastic properties (mechanical rigidity) of tissues. SWE increasingly develops across medical specialities and is already used in hematology, urology and oncology. In the field of ophthalmology using SWE to evaluate corneal mechanical properties, peripapillary biomechanical qualities in glaucoma patients several papers were published Also SWE ultrasound mechanical specificity safety studies were published.
Aim of this work is to review SWE technique and its potentional using during examination in patients with endocrine orbitopathy (EO). In practical part of this work is evaluated the elasticity of oculomotor rectus muscles in healthy population, in patients with EO in early stage of disease (oculomotor muscles oedema) and in patients with EO in terminal stage of this disease (oculomotor muscles fibrosis) is determinate. Also possibility of using SWE (in comparison with standard ultrasound examination) for measuring thickness of oculomotor muscles is evaluated.
Methods: There were 60 eyes in 30 patients with EO examined and the elasticity of oculomotor muscles was determined. Results were compared with values of elasticity in 40 eyes in healthy population of 20 people. All measurements were performed with ultrasonic system Aixplorer of SuperSonic manufacturer in standardized terms and been undertaken by the same performer. Each value was measured several times to reduce measurement errors.
Results: Oculomotor rectus muscle elasticity values in healthy population measured by using SWE were as follows: musculus rectus superior (MRS) 19.7 ± 3.2 kPa, musculus rectus medialis (MRM) 20.5 ± 3.6 kPa, musculus rectus inferior (MRI) 20.4 ± 3.1 kPa and musculus rectus temporalis (MRT) 20.2 ± 1.7 kPa. As statistical analysis shows, there is no significant difference between muscles (ANOVA test p > 0.05); overall elasticity of oculomotor muscles in healthy population is 20.3 ± 3.0 kPa. Elasticity of muscles in group of EO patients in oedema stage and EO patients in fibrosis stage is 18.4 ± 3.2 kPa and 34.6 ± 7.5 kPa respectively. Both values show statistical significance in the comparison with healthy population (p < 0.05).
Conclusion: This work result shows SWE as an EO diagnostic possibility. Elasticity of oculomotor muscles correlates with stages of the disease. Higher elasticity in oedema stage and higher stiffness in fibrosis stage. By involving and including into diagnostic algorithm, SWE could help with EO patient’s examination, offer chance to confirm more accurately the diagnosis and in some cases might even replace magnetic resonance (MRI), which is more expensive and time consuming method.
Keywords:
ultrasound – endocrine orbitopathy – thyroid associated orbitopathy – elastography – shear-wave – ophthalmology – extraocular muscles
INTRODUCTION
This study deals with an examination of the potential contribution of the diagnostic display method shear wave elastography (SWE) in diagnosing changes to the oculomotor muscles in patients with endocrine orbitopathy (EO). Although SWE is being used with ever increasing frequency in diagnostics across medical disciplines, the published studies on its use in ophthalmology focus especially on an evaluation of the properties of the cornea, or peripapillary structures in patients with glaucoma. This study demonstrates the results of an evaluation of the oculomotor muscles using the SWE method, which has previously not been used elsewhere in the Czech Republic in examination of the orbit.
Endocrine orbitopathy (EO) is a chronic disease of all the orbital structures (extraocular muscles, periorbital fat and conjunctival tissue, orbital septum and lachrymal gland), characterised by inflammation in the parabulbar and retrobulbar space, with secondary affliction of the eye. EO is associated with thyropathies, most often (in up to 90% of patients) with autoimmune Graves-Basedow (G-B) thyrotoxicosis. In the case of EO an increase in the volume of the orbital tissue takes place, with a protrusion of the eyeballs (exophthalmos), deterioration of venous return, with manifestations of congestion in the anterior segment of the eye, change of the elastic properties of the oculomotor muscles and secondary development of diplopia. In serious cases exposure keratopathy may develop, as well as corneal ulcers and compression of the optic nerve (neuropathy) [11]. At present EO is divided according to its severity into mild, medium and severe forms, based on the study by Bartalen et al. from 2008 [2]. The clinical activity of the pathology is evaluated according to the Clinical Activity Score (CAS), which determines the degree of the ongoing inflammatory process [11, 12, 24]. The course of EO is characterised by several phases. EO begins with the initial phase of activity, during which the pathology is manifested, and in which the clinical symptoms of the disease progressively worsen. There follows the plateau phase, with progressive stabilisation, which may persist for a number of years. In this phase we do not observe any further deterioration of the condition, and sometimes even a slight improvement may occur. In the terminal phase there is a spontaneous improvement, and the activity of the disease is completely extinguished. The clinical picture of EO is highly diverse. The symptoms of EO include manifestations on the eyelids (retraction of eyelids, preseptal edemas of the eyelids), conjunctivas (injection and chemosis of the conjunctivas, dry eye syndrome) and orbit (exophthalmos, oculomotor disorders, optic neuropathy, secondary glaucoma). Treatment of EO should be directed toward reducing the volume and pressure in the orbit. The therapeutic options are lifestyle adjustments (not smoking), local lubrication therapy, pharmacological treatment (treatment of thyroid gland disorders by adjustment to correct function, gluco-corticoids, immunosuppressants), surgical treatment (decompression of orbit, plastic surgery of oculomotor muscles and eyelids, strumectomy) and radiotherapy (irradiation of the orbits, radioiodine therapy following total thyroidectomy) [11].
Changes of the oculomotor muscles and orbital structures in EO are diagnosed as standard using display methods such as ultrasonography, magnetic resonance imaging (MRI) or computer tomography (CT). The display methods verify the degree of affliction of the extraocular muscles, determine the phase of the pathology and last but not least assist us in observing the effect of therapy [12, 24].
The theme of the study is to evaluate the elasticity of the oculomotor muscles (which changes during the course of EO) using the modality of SWE.
Shear-wave elastography (SWE): SWE is an ultrasonic concept which displays the elastic properties of tissues, increases the specificity of ultrasound examination and thereby improves diagnostic certainty. The method is based on automatic generation of transitional transverse waves (shear waves). SWE is capable of very precisely localising and displaying the elasticity of small lesions with millimetre resolution. It provides quantitative information (values in kPa) on elasticity of human tissues scanned in real time. It rests upon the fact that a change of the mechanical properties of tissue (above all change of rigidity) is often a reflection of pathological processes. The clinical benefits of SWE include very high reproducibility, thanks to the acquisition of SWE maps, high reliability of measurement of size and elasticity of lesions, and high sensitivity and specificity in comparison with conventional ultrasonographic examinations. A disadvantage of SWE is in particular the greater technological demand factor and higher cost in comparison with standard ultrasonic examinations [3, 10, 29]. The output of SWE is an ultrasonic B-mode image covered with a colour-coded map, in which a colour is attributed to each point of tissue, coding its elastic properties. Colour coding of the image is on a scale of red to blue, in which more rigid tissues are displayed in warm shades (red, yellow) and soft tissues in cold colours (blue, purple) [16, 29].
The inspiration for the work was a study by Greek authors from 2010 [6], comparing elastographic horizontal images of the oculomotor muscles and their different elasticity in primary position and in extreme gaze directions. At the time of the commencement of this research, it concerned the only published work dealing with the elasticity of the oculomotor muscles. The fact that the elasticity of the oculomotor muscles changes during the course of EO helped put this study into practice.
AIMS OF STUDY
To determine the average value of elasticity of the oculomotor rectus muscles in the healthy population.
To evaluate the elasticity of the oculomotor rectus muscles in the initial phase of EO in the stage of inflammatory infiltration and edema of the muscles.
To evaluate the elasticity of the oculomotor rectus muscles in the terminal phase of EO with fibrosis of the muscles.
To compare the modalities of SWE and standard ultrasonic (US) examination upon measurement of the width of the oculomotor rectus muscles.
COHORT AND METHOD
A total of 50 patients (100 orbits) were included in the evaluated cohort, examined on the elastographic ultrasonic system Aixplorer from the SuperSonic company (fig. 1) [16] at the Internal Gastroenterology Clinic (IGEC) at Brno University Hospital, under standard conditions and always by the same user. The measurements were conducted repeatedly, for the purpose of reducing errors of measurement. The method of transpalpebral examination (via closed eyelids) was used on all patients in a longitudinal image (fig. 2), in which the probe is placed perpendicular to the corneal limbus, the control signal of the probe in the direction toward the cornea [14]. Using this examination method, the individual oculomotor rectus muscle is displayed longitudinally from the equator to the muscle cone (front-to-back incision of eye socket), the probe is always placed contralaterally to the examined muscle. All four oculomotor rectus muscles in both eyes were examined in all patients. The examination was performed using a linear convex probe SuperMicroConvex 12-3 (fig. 3) [16]. Elasticity of the oculomotor muscles was measured outside of the area of the tendon, where there is physiologically higher echogenicity, in order to avoid distorted interpretation of the results. The individual oculomotor muscles were always measured in the primary position of the eyeball. Each individual muscle was measured perpendicular to the axis of the muscle. With regard to the fact that the muscles are not solid tissue and have a heterogeneous internal structure, elasticity was measured in the region of interest (ROI), the diameter of which corresponded to the thickness of the measured muscle. Upon evaluation of the width of the individual muscles, their shorter diameter was always measured.



The usability of an elastographic instrument for measuring the thickness of the afflicted oculomotor muscles was tested on the cohort of patients. The results were compared with the measurement of the same muscles with the aid of a standard US examination using the Compact Touch instrument from the Quantel medical company with a 10MHz probe at the Department of Ophthalmology at the University Hospital in Brno. In addition, a comprehensive ophthalmological examination was performed on all the tested subjects, incorporating determination of central visual acuity, measurement of intraocular pressure, standard biomicroscopic examination of the anterior and posterior segment on a slit lamp, examination of motility of the eyeballs and exophthalmometry with the aid of a Hertel exophthalmometer.
The total cohort of 100 orbits included 60 orbits of 30 patients with clinical symptoms of EO and demonstrated thyropathy, who had been referred from endocrinology to the IGEC at Brno University Hospital in the period from September 2014 to September 2017. This group comprised 8 men and 22 women aged from 27 to 75 years (median age 58.5 years). All these patients had Graves-Basedow disease (thyrotoxicosis), and all had undergone total thyroidectomy at various time intervals since examination. In patients with EO, the average values of elasticity of the oculomotor muscles were defined in the individual phases of the pathology - in the acute phase of edema and inflammatory infiltration of the muscles, and in the chronic phase with a proportion of fibrotic changes of the muscles. There was an initial total of 20 patients (40 eyes) in the acute phase of EO, in 9 of whom progression to the phase of inactivity was evident during the course of the observation period, and therefore 9 patients were measured in both active and inactive stages of the pathology. The group of acute phase of EO included patients with clinically expressed activity of the pathology (CAS>3), with positive symptoms on the eyelid and protrusion of the eyeball. The patients were administered general immunosuppressants, or were shortly before indication of a bolus of Solu-Medrol i.v. A total of 10 patients (20 orbits) were in the chronic phase of inactivity. Activity of the pathology was completely extinguished in these patients (CAS≤1), the patients had deviation of the eyeball with persistent diplopia and were indicated for strabismus surgery. All four oculomotor rectus muscles were measured in all the tested subjects, and only afterwards were the extended muscles evaluated. Extension was considered to mean extension of the shorter diameter beyond physiological values (MRS up to 6.8 mm, MRM up to 4.7 mm, MRI up to 3.6 mm, MRT up to 3.8 mm) according to the normative values for the healthy population, taking into account age, sex and physical constitution [4].
Both cohorts of patients with EO were compared with a healthy population numbering 40 orbits of 20 persons (5 men, 15 women) aged from 25 to 77 years (median age 40.5). The oculomotor muscles in the healthy population are characteristic in their ellipsoid shape in transverse cross-section, and as a result in their measurement we differentiate evaluation of the shorter and longer diameter. The shorter diameter was always evaluated in the cohort of tested healthy subjects.
A dispersion analysis (ANOVA test) was used for the statistical evaluation and analysis, which mutually compared the individual oculomotor rectus muscles in a healthy control group. A double-selection one-way Student T-TEST was also used, in which two different groups were always compared (healthy population in comparison with a group with active phase of EO; healthy population in comparison with terminal phase of EO). A further analytical method used was a Spearman correlation analysis, which evaluated the thickness of the oculomotor muscles in patients with EO measured by a classic US instrument and elastograph.
The frequency of affliction of the individual oculomotor rectus muscles was not the focus of this study, however upon processing of the results the following frequency was determined in patients with EO. The musculus rectus superior (MRS), musculus rectus medialis (MRM) and musculus rectus inferior (MRI) were afflicted in 55% of cases, the musculus rectus temporalis (MRT) was afflicted in 33.3%. If only one oculomotor muscle was afflicted in isolation (in 8 orbits), a vertical muscle was most frequently afflicted (in 50% of cases this concerned the MRS, in 25% MRI, affliction of the MRM and MRT was identified in 12.5% - one case each time). Upon affliction of two oculomotor muscles, the most frequently afflicted was the MRS, followed by the MRM. Affliction of two oculomotor muscles was identified in 13 orbits, the most frequent affliction was evident in the case of MRM, MRS and MRS), a total of 17 orbits involved affliction of three oculomotor muscles. All the oculomotor muscles were afflicted in a total of 9 orbits. Upon isolated affliction of only one oculomotor muscle in patients with EO, the most frequently afflicted was a vertical muscle. If only one muscle was extended, this most often concerned the MRS (48.8%), followed by MRI (31.7%) or MRM (19.5%), while MRL was not afflicted in isolation in a single case. Upon affliction of two oculomotor muscles, the MRS was extended in 64.3%, MRI and MRM in 60.7% and MRL in 14.3%. Upon affliction of three oculomotor muscles, the most frequently extended was the MRM (93.1%), followed by the MRI (86.2%), MRS (69%) and MRL (51.7%). In the cohort we demonstrated affliction of the muscles in the right eye in 6 patients, in 7 patients with EO the muscles in the left eye were afflicted, and in 17 patients this concerned bilateral affliction of the oculomotor muscles.
RESULTS
In the cohort of patients, the SWE image of a healthy population was defined (numbering 40 orbits, 20 tested subjects), with a finding of average elasticity values of the oculomotor muscles in kPa. This group was compared with a group of patients with EO (total number of 60 orbits, 30 tested subjects).
-
Evaluation of elasticity values of oculomotor muscles in healthy population
The determined values of elasticity of the oculomotor muscles are presented in table 1. In the healthy population, the musculus rectus superior (MRS) has a median elasticity value of 19.7 ± 3.2 kPa, the musculus rectus medialis (MRM) has a value of 20.5 ± 3.6 kPa, the musculus rectus inferior (MRI) has a value of 20.4 ± 3.1 kPa and the musculus rectus temporalis (MRT) has elasticity of 20.2 ± 1.7 kPa. A dispersion analysis demonstrated that the elasticity values for the individual oculomotor muscles do not differ statistically significantly (ANOVA test p > 0.05). It is therefore possible to take the median elasticity of the entire cohort numbering 160, with values of 20.3 ± 3.0 kPa, as the determined elasticity value of the oculomotor rectus muscles in the healthy population. More detailed statistics of the measured elasticity values of the oculomotor muscles in the control group are illustrated in the histogram of frequencies (graph 1). An example of measurement of elasticity of the MRS in a healthy individual is presented in fig. 4.



-
Evaluation of elasticity of oculomotor muscles in initial phase of EO in stage of inflammatory infiltration and muscle edema
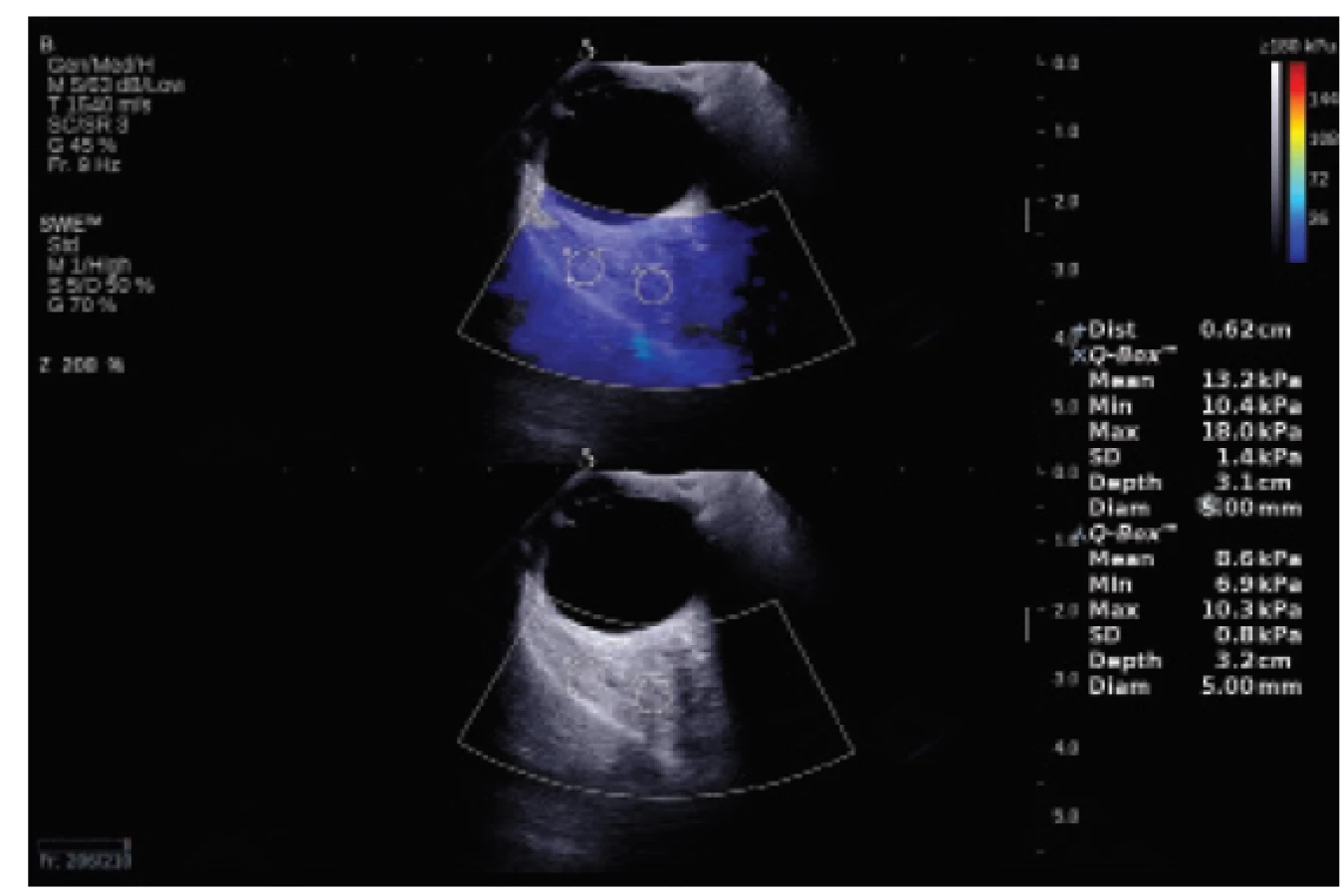
In patients with EO in the stage of inflammatory infiltration and muscle edema, elasticity was evaluated in a cohort of 83 oculomotor muscles. The result is an elasticity value of 18.4 ± 3.2 kPa. The deviation from the control group is statistically significant (double-selection one-way T-TEST p < 0.05), and it is possible to state that the oculomotor muscles in patients with EO in the stage of inflammatory infiltration and edema have higher elasticity (lower rigidity). A histogram of frequencies of the examined cohort is presented in graph 2. A statistical comparison of the elasticity values with the healthy population is presented in table 2 and graph 3. An example of measurement of the elasticity of an edematous MRS is presented in fig. 5.



-
Evaluation of elasticity of oculomotor muscles in terminal phase with fibrous muscles
In the group of patients with EO, elasticity was evaluated in the chronic stage, with limited motility and deviation of the eyeball in a cohort of 116 oculomotor muscles. The determined elasticity value is 34.6 ± 7.5 kPa, which concerns a value significantly higher (higher rigidity, lower elasticity) than in the control group, which was also confirmed by the analysis (double-selection one-way T-TEST p < 0.05). A histogram of frequencies of the examined cohort is presented in graph 4. A statistical comparison of the elasticity values with the healthy population is presented in table 3 and graph 5. An example of measurement of the elasticity of an edematous MRS is presented in fig. 6.




-
Comparison of elastographic US instrument and standard US examination upon measurement of width of oculomotor muscles
In the control (healthy) group of the population, in a comparison of an examination by elastographic ultrasonic instrument and by a standard US examination, the measured values of thickness of oculomotor muscles were entirely identical. Examination on an elastographic ultrasonic instrument demonstrated better resolution of the individual interfaces of the oculomotor rectus muscles in comparison with a standard US examination.
A total of 119 afflicted oculomotor muscles were measured (muscles in active and inactive phase of EO). The analysis (pair T-TEST) of the cohort in patients with EO demonstrated that the results from both modalities are statistically significantly different (p < 0.05). The results of measurement of thickness of oculomotor muscles from both modalities are compared in table 4. From table 4 it is evident that the values of thickness of oculomotor muscles measured by the SWE method are higher, although statistically insignificant. According to expectations, the deviations between US and SWE measurement were the largest in the case of the rectus musculus inferior, the difference in the measured thickness of muscles in some cases reached as much as 30%. As illustrated in graph 6, the conducted analysis (Spearman correlation) of values of thickness of the oculomotor muscles in patients with EO measured by a classic US instrument and elastograph shows a strong correlation.


DISCUSSION
Standards of elasticity values of human tissues such as the breast gland, liver, prostate or thyroid gland are progressively being established across medical disciplines [16]. The imaging of the superficial musculoskeletal system and the rectal region are being studied, and in other fields of medicine such as cardiology, the use of SWE is starting to be emphatically promoted. The main studies from 2011 and 2012, which provided the basic data on elasticity of human tissues and became groundbreaking works are studies from hepatology [8], urology [1] and oncology of the mammary glands [15]. In endocrinology SWE helps determine a precise diagnosis in locating nodes in the thyroid gland [23].
In ophthalmology today, international studies are taking place, in which the preliminary results show that in future SWE could in certain cases replace financially costly imaging diagnostic methods, which are furthermore burdensome for the patient.
A team of French scientists [26] published a study documenting changes of the mechanical properties of the cornea following the stabilisation procedure corneal cross-linking (CXL). The authors Touboul et al. [27] in their study tested SWE in in-vivo conditions, evaluating the effect in a CXL experiment on 6 rabbits. The conclusions of this study also evaluate SWE as an effective tool for evaluating photopolymerisation of collagen structures of the cornea during CXL.
In a study by the authors Nguyen et al. [18], SWE was used for a quantitative evaluation of corneal rigidity in pigs and two-dimensional mapping of the surface of the cornea after the performance of CXL. The same author [17] also published a study on the possibilities of use of SWE in an evaluation of corneal anisotropy.
The authors Dikici et al. in their study [7] demonstrate the possibility of using SWE to evaluate the biomechanical properties of the peripapillary region in the diagnosis of glaucoma. The study demonstrated that the average rigidity values in each measured region (perineural region of sclera, optic nerve) are significantly higher in patients with glaucoma in comparison with a healthy control group. In the case of glaucoma they demonstrated greater rigidity of the measured structures of the eyeball and declared SWE to be a promising method.
A study was also published by the authors Zha et al. [30], dealing with the question of the safety of elastography. A measurement was conducted on 126 live rats divided into 7 groups. The authors used high acoustic pressure (mechanical index 1.6), observed the SWE image of the eyeball, vitreous body and periocular soft tissues. In the conclusion of the study they state the safety of the technique and the possibility of its use on humans.
The literature [6] also contains available data from Greek authors comparing ultrasound images of the horizontal oculomotor muscles (m. rectus temporalis, m. rectus medialis) in five people and their different elasticity in primary position and in adduction or abduction. In primary position the rigidity (MRM 25.8 ± 12.1 kPa and MRT 25.7 ± 14.3 kPa) of the horizontal oculomotor muscles is higher than in adduction (MRM 21.1 ± 13.4 kPa and MRT 23.1 ± 17.8 kPa) and abduction (MRM 22.3 ± 14.0 kPa and MRT 22.9 ± 16.7 kPa). The same author [5] evaluates the elasticity of the ciliary body and intraocular lens in 10 rabbit eyes. The experiment in vivo observes changes of the intraocular lens, ciliary body and overall ocular rigidity following the instillation of atropine and pilocarpine. The result of the experiment is that SWE is able to detect changes of rigidity in the anterior ocular segment in rabbit eyes, and may therefore potentially be beneficial for humans, where changes of rigidity of the ocular tissues (complex of ciliary body, suspensory ligament, lens) play an important role in the diagnosis of pseudoexfoliation syndrome, cataract or presbyopia.
Another study [21] describes changes of the vitreous body, the retina-choroid-sclera complex and value of retrobulbar pressure in 20 myopic eyes. On the basis of this study, it is assumed that in clinical practice SWE may in future be of assistance in the diagnosis of EO, ocular tumours and in the evaluation of the vitreous space following application of intravitreal injections. The same authors [22] in a prospective study compare a group of patients with proliferative diabetic retinopathy (PDR) after panretinal photocoagulation with a control group of patients with nonproliferative diabetic retinopathy (NPDR). The average values of the retina-choroid-sclera complex are statistically significantly higher (p = 0.002) than in the control group of patients with NPRD. The SWE method reliably evaluates the effect of panretinal photocoagulation, after which a change occurs to the elasticity of the wall of the eyeball (rigidity of the retina-choroid-sclera complex increases).
The authors Unal et al. [28] in a prospective study evaluate the elastographic image of the disc of the optic nerve in 40 eyes of 40 patients (20 eyes with primary open-angle glaucoma, 20 eyes from a healthy control group). The elasticity values in the patients with glaucoma differ statistically significantly (in glaucoma the tissues are more rigid). This finding may help in understanding biomechanical changes in the field of glaucoma and facilitate a quicker diagnosis of early stages of the pathology.
Another study by the authors Sit et al. from 2017 [25] deals with the definition of the corneal Young's modulus in 20 eyes of 10 healthy persons (696 ± 113 kPa) and correlates this value with the value of intraocular pressure (12.8 ± 2.7 mmHg), age, central corneal thickness and axial length of the eye. The result is the observation that Young's modulus of elasticity is associated with the value of intraocular pressure. Whether the elasticity of ocular tissues is altered, above all the sclera in glaucoma, remains a question for further essential studies.
French authors [9] used SWE in a study to measure a cadaverous Achilles tendon, and conclude that SWE may provide information about the biomechanical properties of the Achilles tendon by a non-invasive method.
Karhanová [13] in her study states the frequency of affliction of the individual oculomotor muscles in comparison with the normative values, taking into account the different norms for men and women as follows: the musculus rectus medialis (MRM) was extended in 55.2%, musculus rectus temporalis (MRT) in 33.8%, musculus rectus inferior (MRI) in 57.1% and musculus rectus superior (MRS) in 59.1%. In my cohort of patients with EO, the frequency of affliction of the individual muscles was practically identical to the results of Karhanová's study from 2014.
During EO, the US image of the oculomotor muscles alters in the sense of a change of their width, internal structure and reflectivity, which in the first phase of the disease can be well distinguished in comparison with the retrobulbar space. In patients with EO, inflammatory infiltration and edema of the muscles leads to an extension of their venter musculi, and therefore to an increase of their shorter diameter. In further phases of EO, the difference becomes obscured due to the influence of an accumulation of glycosaminoglycans, a reproduction of fat and increasing echogeneity of the orbital fat and muscles, making the individual tissue interfaces difficult to measure and define. US examination is suitable for displaying the eyeball and the anterior 2/3 of the orbital space, but does not enable visualisation in the region of the orbital apex. US examination also fails in the evaluation of extremely thickened oculomotor muscles and often is incapable of fully measuring the posterior limit of the extended oculomotor muscle. Subjectively it is possible to state that thanks to the use of a linear probe, measurement on an elastograph provides better spatial resolution, better reproducibility and specificity of measurement in cases where conventional US examination fails as a result of significant edematous and fibrotic changes in the muscles, and often leads to an imprecise definition of the limit of the muscle in the retrobulbar region. Standard US examination therefore occasionally underestimates the thickness of muscles, and most often fails in the measurement of the thickness of the musculus rectus inferior (MRI), which is frequently difficult to detect as a consequence of the anatomical configuration of the orbit (larger supraorbital ridge).
Within the cohort it is evident that the values of width of the oculomotor muscles differ depending on sex, age and physical constitution. The norms for the physiological values of width of the oculomotor muscles differ according to the used imaging method, as illustrated in table 5, as well as ethnic and socio-economic differences. As published by Özgen et al. [20], in the male population the average values of width of the oculomotor muscles are significantly higher (p < 0.001) than in women.

Thanks to the fact that the elasticity values of various tissues of the eyeball fluctuate within a certain, often substantial range (see aforementioned published studies), it shall further be necessary to conduct several further studies in order to reach a precise definition of the physiological elasticity values of ocular and orbital structures using the SWE method. After a sufficient amount of performed experiments and scientific studies, it shall be possible to determine precisely the range of elasticity values in various pathologies, and above all to gain a better understanding of the biomechanical properties of the individual ocular structures, which are altered in certain pathologies.
The study demonstrated statistically significant differences of elasticity values in patients with EO in the phase of fibrotic changes of the oculomotor muscles.
The only limitation of this study is the relatively small cohort of patients.
CONCLUSION
This study demonstrates the results of an evaluation of oculomotor muscles using the method of shear-wave elastography, which to date has not yet been used anywhere else in the Czech Republic in examination of the orbit. The study considers the possibilities of using SWE for diagnosing changes of oculomotor muscles in patients with endocrine orbitopathy. Determination of the prevalence of EO in practice is influenced above all by the sensitivity of the method. It is precisely SWE, thanks to its high degree of reproducibility and indisputable advantages (better display of retrobulbar space, better precision of measurement, independence of examiner) in comparison with standard US examinations (less financially costly, dependence on experience of examiner, impossibility of displaying posterior parts of orbit, impossibility of unequivocally excluding other orbital pathologies), that represents a more sensitive modality.
The study demonstrated that the elasticity of individual oculomotor muscles depends on the stage of the pathology. It defines different elasticity values in patients in EO in the phase of inflammatory infiltration and edema of the muscles, and different values in the stage of fibrous changes.
The study further demonstrated that with the aid of SWE we are able to precisely define the individual oculomotor muscles and better determine their dimensions in comparison with standard US examination, which occasionally fails in the measurement of short diameters in the case of pronounced thickening of the oculomotor muscles within the framework of EO. In contrast with conventional US examination, SWE, thanks to its high resolution capacity, specificity and possibility of changing the scope of the examined area of interest, represents a more sensitive method and enables us to better evaluate the retrobulbar space.
The results of the study indicate the possibility of using SWE in the diagnosis of EO, in which elasticity of the oculomotor muscles correlates with the degree of affliction, both in the phase of edema and inflammatory infiltration, and in the state of fibrosis. Inclusion of the method within diagnostic procedures would ease and increase the precision of examination of patients with EO. The method could become an alternative to magnetic resonance imaging, which is more time consuming and also more expensive.
The author of the study declares that no conflict of interest exists in the compilation, theme and subsequent publication of this professional communication, and that it is not supported by any pharmaceuticals company.
Received by the Editorial Department on: 23 July 2018
Accepted for printing on: 4.2.2019
MUDr. Markéta Zemanová, Ph.D.
Department of Ophthalmology, University Hospital and Faculty of Medicine, Masaryk University Brno
Jihlavská 20
625 00 Brno
e-mail: Zemanova.Marketa@fnbrno.cz
Zdroje
1. Barr, RG., Memo, R., Schaub, CR.: Shear wave ultrasound elastography of the prostate: initial results. Ultrasound Q, 28(1); 2012 : 13-20.
2. Bartalena, L., Baldeschi, L., Dickinson, AJ. et al.: Consensus statement of the European group on Graves‘ orbitopathy (EUGOGO) on management of Graves‘ orbitopathy. Thyroid, 18(3); 2008 : 333-46.
3. Bercoff, J., Tanter, M., Fink, M.: Supersonic shear imaging: A new technique for soft tissues elasticity mapping. IEEE Trans. Ultrason. Ferroelectr., Freq. Control, 51(4); 2004 : 396-409.
4. Byrne, SF., Gendron, EK., Glaser, JS. et al.: Diameter of normal extraocular recti muscles with echography. Am J Ophthalmol., 112(6); 1991 : 706-13.
5. Detokaris, ET., Drakonaki, EE., Ginis, H. et al.: Evaluation of iridociliary and lenticular elasticity using shear-wave elastography in rabbit eyes. Acta Medica (Hradec Králové), 57(1); 2014 : 9-14.
6. Detorakis, ET., Drakonaki, EE., Tsilimbaris, MK. et. al.: Real-time ultrasound elastographic imaging of ocular and periocular tissues: a feasibility study. Ophthalmic Surg Lasers Imaging, 41(1); 2010 : 135-41.
7. Dikici, AS., Mihmanli, I., Kilic, F. et al.: In Vivo Evaluation of the Biomechanical Properties of Optic Nerve and Peripapillary Structures by Ultrasonic Shear Wave Elastography in Glaucoma. Iran J Radiol, 13(2); 2016: e36849.
8. Ferraioli, G., Tinelli, C., Dal Bello, B. et al.: Accuracy of real-time shear wave elastography in the assessment of liver fibrosis in chronic hepatitis C: A pilot study. Hepatology, 56(6); 2012 : 2125–33.
9. Haen, TX., Roux, A., Soubeyrand, M. et. al.: Shear waves elastography for assesment of human Achilles tendon`s biomechanical properties: an experimental study. J Mech Behav Biomed Mater, 69; 2017 : 178-84.
10. Hrazdira, I.: Úvod do ultrasonografie v otázkách a odpovědích: pro studenty lékařské fakulty. Brno, Klinika zobrazovacích metod LF MU, Fakutlní nemocnice u Sv.Anny v Brně. 2008. dostupné na www: www.med.muni.cz/dokumenty/pdf/uvod_do_ultrasonografie1.pdf.
11. Hrdá, P., Novák, Z., Šterzl, I.: Endokrinní orbitopatie: Edice farmakoterapie pro praxi. Svazek 41. Praha, Maxdorf; 2009. ISBN 978-80-7345-194-3.
12. Karhanová, M.: Diagnostika endokrinní orbitopatie v praxi. In: Rozsíval, P. (Ed), Trendy soudobé oftalmologie: svazek 8. Praha, Galén, 2012, s. 15-32.
13. Karhanová, M., Kovář, R., Fryšák, Z. et al.: Postižení okohybných svalů u pacientů s endokrinní orbitopatií. Cesk Slov Oftalmol, 70(2); 2014 : 66-71.
14. Khatib, Z.: Ultrasound methods for evaluating orbital diseases. [online]. [cit. 2018-06-02]. Dostupné na www: www.slideshare.net/vaibhavkhanna1048/usg-69421051.
15. Kim, H., Youk, JH., Gweon, HM. et al.: Diagnostic performance of qualitative shear-wave elastography according to different color map opacities for breast masses. Eur J Radiol, 82(8); 2013 : 326-31.
16. Medata: Supersonic Imagine The Theragnostic CompanyTM. Teoretické základy a principy ShearWaveTM Elastografie [online]. Brno: Medata spol. s.r.o. [cit. 2018-06-02]. Dostupné na www: http://www.medata.cz/_docs/cz_supersonicimagine-swe_teorie.pdf.
17. Nguyen, TM., Aubry, JF., Fink, M. et. al.: In vivo evidence of porcine cornea anisotropy using supersonic shear wave imaging. Invest Ophthalmol Vis Sci, 55(11); 2014 : 7545-52.
18. Nguyen, TM., Aubry, JF., Touboul, D. et al.: Monitoring of cornea elastic properties changes during UV-A/Riboflavin-induced corneal collagen cross-linking using Supersonic Shear Wave Imaging: A Pilot Study. Invest Ophthalmol Vis Sci, 53(9); 2012 : 5948-54.
19. Özgen, A., Ariyurek, M.: Normative measurements of orbital structures using CT. Am J Roentgenol, 170(4); 1998 : 1093-6.
20. Özgen, A., Aydingöz, U.: Normative measurements of orbital structures using MRI. J Comput Assist Tomogr, 24(3); 2000 : 493-6.
21. Pekel, G., Ağladıoğlu, K., Acer, S. et. al: Evaluation of ocular elasticity in high myopia. Optom Vis Sci, 92(5); 2015 : 573-8.
22. Pekel, G., Ağladıoğlu, K., Acer, S. et. al.: Evaluation of ocular and periocular elasticity after panretinal photocoagulation: an ultrasonic elastography study. Curr Eye Res, 40(3); 2015 : 332-7.
23. Sebag, F., Vaillant-Lombard, J., Berbis, J. et al.: Shear Wave Elastography: A New Ultrasound Imaging Mode for the Differential Diagnosis of Benign and Malignant Thyroid Nodules. J Clin Endocrinol Metab, 95(12); 2013 : 5281-8.
24. Schovánek, J., Cibičková, L., Karhanová, M. et. al.: Endokrinní orbitopatie a nová doporučení. Interní Med, 19(5); 2017 : 246-50.
25. Sit, AJ., Lin, SC., Kazemi, A. et. al.: In vivo noninvasive measurement of Young’s modulus of elasticity in human eyes: A feasibility study. J Glaucoma, 26(11); 2017 : 967-73.
26. Tanter, M., Touboul, D., Gennisson, J. L. et al.: High-resolution quantitative imaging of cornea elasticity using supersonic shear imaging. IEEE Trans Med Imaging, 28(12); 2009 : 1881-1893.
27. Touboul, D., Gennisson, JL., Nguyen, TM. et al.: Supersonic shear wave elastography for the in vivo evaluation of transepithelial corneal collagen cross-linking. Invest Ophthalmol Vis Sci, 55(3); 2014 : 1976-84.
28. Unal, O., Cay, N., Yulek, F. et. al.: Real-Time Ultrasound Elastographic Features of Primary Open Angle Glaucoma. Ultrasound Q, 32(4); 2016 : 333-7.
29. Zemanová, M.: Nová diagnostická zobrazovací metoda-shear waves elastografie. Čes. a slov. Oftal, 72(4); 2016 : 103-10.
30. Zha, L., Chen, KQ., Zheng, XZ. et. al.: The safety and feasibility of diagnostic acoustic radiation force impulse elastography used for eyes. A preliminary in vivo study. Med Ultrason, 19(2); 2017 : 185-9.
Štítky
OftalmologieČlánek vyšel v časopise
Česká a slovenská oftalmologie

2019 Číslo 1
- Selektivní laserová trabekuloplastika nesnižuje nitroční tlak více než argonová laserová trabekuloplastika
- Progresi glaukomu je třeba hodnotit strukturálními i funkčními parametry
- Ztráta centrálního vidění po filtrujících operacích glaukomu
- Od PGF-2 alfa-isopropyl esteru k latanoprostu: přehled vývoje Xalatanu
- Compliance u pacientů s glaukomem
Nejčtenější v tomto čísle
- Late postoperative capsular bag distension syndrome
- Primary orbital teratoma – case study
- Treatment of idiopathic choroidal neovascular membrane with ranibizumab - our experience
- RADIATION MACULOPATHY AFTER ONE-DAY SESSION STEREOTACTIC RADIOSURGERY IN PATIENTS WITH CILIARY BODY AND CHOROIDAL MELANOMA
Zvyšte si kvalifikaci online z pohodlí domova
Mazová zátka a její řešení
nový kurzVšechny kurzy