
Efficacy and safety of emergent microsurgery in acute ischaemic stroke patients after intravenous thrombolysis and mechanical thrombectomy failures – a systematic review
Účinnost a bezpečnost urgentní mikrochirurgie u pacientů s akutním ischemickýmiktem po selhání intravenózní trombolýzy a mechanické trombektomie – systematické review
Cíl: Cílem tohoto systematického přehledu bylo ověřit úlohu urgentní mikrochirurgické embolektomie a extrakraniálního-intrakraniálního bypassu jako třetí linie léčby v případech uzávěru velké mozkové cévy po selhání standardní léčby. Soubor a metodika: Provedli jsme rozsáhlou rešerši osmi zdrojů publikované i nepublikované literatury. Dva recenzenti nezávisle na sobě provedli analýzu názvů, abstraktů, plných textů a poté provedli kritické hodnocení a extrakci dat z vybraných studií pomocí standardizovaných nástrojů. Výsledky zahrnutých studií jsme narativně syntetizovali. Výsledky: Vyhledávání identifikovalo osm relevantních článků, zahrnujících 12 pacientů s urgentním uzávěrem velké cévy (terminální krkavice nebo střední mozková tepna) a selháním standardní léčby, kteří podstoupili mikrochirurgický zákrok do 24 hodin od vzniku příznaků. Mikrochirurgická embolektomie byla provedena ve čtyřech případech (33 %), extrakraniální-intrakraniální bypass v pěti případech (42 %), jejich kombinace ve dvou případech (16 %) a manipulační intraoperační rekanalizace v jednom případě (8 %). Skóre na škále National Institutes of Health Stroke Scale se předoperačně pohybovalo v rozmezí 7–25 bodů a pooperačně (1–7 dní po operaci) v rozmezí 1–18 bodů. Funkční nezávislosti (modifikované Rankinovo skóre 0–2) bylo dosaženo u devíti pacientů (75 %) po 3–12 měsících po operaci. Závěr: Urgentní mikrochirurgická embolektomie, extrakraniální-intrakraniální bypass nebo kombinace těchto metod se jeví jako bezpečná a potenciálně účinná třetí linie léčby u pacientů s urgentním uzávěrem velké cévy v přední mozkové cirkulaci.
Klíčová slova:
cévní mozková příhoda – trombolýza – trombektomie – mikrochirurgie
Authors:
M. Grubhoffer 1,2; J. Fiedler 1,3; S. Slezáková 4,5; M. Bombic 1; M. Klugar 4,5
Published in the journal:
Cesk Slov Neurol N 2025; 88(2): 83-88
Category:
Přehledný referát
doi:
https://doi.org/10.48095/cccsnn202583
Summary
Aim: This systematic review aimed to verify the role of emergent microsurgical embolectomy and extracranial-intracranial bypass as third-line treatments in cases of intracranial large-vessel occlusion after failure of standard treatment. Materials and methods: We extensively searched eight sources of published and unpublished literature. Two reviewers independently performed titles, abstracts, and full text analyses, and then performed critical appraisal and data extraction from selected studies using standardised tools. We narratively synthesised the findings of the included studies. Results: The search identified eight relevant articles, including 12 patients with emergent large-vessel occlusion (carotid terminus or middle cerebral artery), and standard treatment failure who underwent microsurgery within 24 h from symptom onset. Microsurgical embolectomy was performed in four cases (33%), extracranial-intracranial bypass in five cases (42%), their combination in two cases (16%), and manipulative intraoperative recanalization in one case (8%). National Institutes of Health Stroke Scale score ranged pre-operatively from 7 to 25 points and postoperatively (1–7 days after surgery) from 1–18 points. Functional independence (modified Rankin Scale score 0–2) was achieved in nine patients (75%) at 3–12 months postoperatively. Conclusion: Emergent microsurgical embolectomy, extracranial-intracranial bypass, or a combination of these methods appear to be a safe and potentially effective third-line treatment for patients with emergent occlusion of large vessels in the anterior cerebral circulation
Keywords:
stroke – thrombolysis – thrombectomy – microsurgery
Introduction
Intravenous thrombolysis (IVT) and mechanical thrombectomy (MT) represent a therapeutic standard in the treatment of emergent large-vessel occlusion (ELVO) in patients with stroke [1]. Two recent studies have extended the therapeutic window for MT in selected patients with preserved perfusion parameters up to 16 or 24 h, respectively [2–4]. This time window continues to widen [5,6]. In endovascular studies, successful recanalization after MT, resulting in a modified Thrombolysis in Cerebral Infarction (mTICI) score of 2b-3, was achieved in 59–88% of cases [7–11]. However, in approximately 10% of cases no recanalization could be achieved at all [12].
Persisting occlusion after a failed MT is associated with an unfavourable outcome, requiring further attempts at vessel recanalization [13]. Microsurgery offers alternative ways of ELVO recanalization in the anterior cerebral circulation using two main approaches – microsurgical embolectomy (ME) and extracranial-intracranial bypass (EC-IC) – or their respective combination. The aim of this systematic analysis of the available literature was to assess the safety and efficacy of emergent ME and EC-IC bypass (i.e., up to 24 h from symptom onset) in acute cerebral revascularization after IVT. Furthermore, we verified the role of microsurgery as a third-tier option in failed IVT and MT cases.
Materials and methods
We registered the systematic review protocol in the PROSPERO registry under the number CRD42017078511 and published the systematic review protocol [14]. Whereas to prepare this systematic review, we used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and the Joanna Briggs Institute (JBI) Reviewer‘s Manual [15,16].
Nuances from the published protocol
Compared with the original protocol, we decided to include ME and EC-IC bypasses or their combination, as reflected in our search strategy. We also partially adjusted the list of search sources because some sources no longer existed or did not contain information relevant to our topic. Moreover, we broadened the search strategies based on the results of the initial search.
Interventions
We considered studies that included adult patients with acute ischaemic stroke and ELVO after the use of standard intravenous recombinant tissue plasminogen activator (rt-PA) treatment (a dose of 0.9 mg/kg or 0.6 mg/kg of rt-PA in a 4.5 h treatment window) followed by failure of MT.
All studies involving ME, EC-IC bypass, or their combination performed within 24 h of symptom onset were included in this analysis. Time intervals of up to 8, 16, and 24 h from symptom onset until intervention were used for further group stratification.
Outcomes
All studies using standardised evaluation criteria were included in the analysis: National Institutes of Health Stroke Scale (NIHSS) score at 24 h after intervention, five and seven days after stroke, or at discharge in case of earlier onset; modified Rankin scale (mRS) score at 90 days and one year after stroke; and mTICI score.
Secondary endpoints were occurrence of symptomatic intracerebral haemorrhage including subarachnoid haematomas, defined as parenchymal haemorrhage of the second type and clinical deterioration of NIHSS score ≥ 4, mortality at 90 days and one year after stroke, and surgical complications.
Studies included in the review
All studies evaluating IVT therapy (standard intravenous rt-PA dose of 0.9 mg/kg in Europe and 0.6 mg/kg in Asia administered within 4.5 h after symptom onset) in adults with acute ischaemic stroke and intracranial ELVO in the anterior circulation with subsequent MT failure were included in this review.
Search strategy
A three-step search strategy was used for this systematic review. First, we conducted an initial limited search of the MEDLINE (Ovid) database. Additional text words and index terms were identified from relevant retrieved records. A second search was performed using newly detected keywords and index terms and was translated for each included database. Third, the reference lists of all of the studies that met the inclusion criteria searched for additional studies. There were no language or publication year search limitations; however, only studies with English abstracts were included in the review.
We searched MEDLINE (Ovid), Embase (Ovid), CINAHL (EBSCOhost), Web of Science Core Collection, Scopus, ProQuest Health and Medical Collection, and EBM Reviews (Ovid) databases. We also searched MedNar, a source of unpublished studies and grey literature. The identified records were uploaded to EndNote X9 and deduplicated using the method published by Bramer et al. [17].
Searches across all of the mentioned sources were first conducted in April 2020 and then repeated with no changes in the search strategies in January 2023. An update of the existing search and correct representation of the retrieved results in the PRISMA 2020 flow diagram was performed according to the method described by Bramer and Bain [18].
EC-IC – extrakraniální-intrakraniální; EVT – endovaskulární léčba; IVT – intravenózní trombolýza; ME – mikrochirurgická embolektomie;
n – počet; PRISMA – Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Study records
All database search outcomes considered for inclusion in the study were assessed by two independent evaluators (MG and JF) in two steps. First, article titles and abstracts were evaluated. Second, all relevant texts were analysed.
Critical appraisal
Papers selected for retrieval were assessed by two independent evaluators (MG and JF) for methodological quality prior to inclusion in the review using standardised critical appraisal instruments from JBI; for example, the Checklist for Case Reports [16]. Conflicting cases were examined by a third evaluator (MK). JF did not assess his own published works.
Data collection
Data were extracted by two independent evaluators (MG and JF) using a standardised extraction system, the CARE Checklist [19].
Missing data
In case of missing data, authors of the evaluated studies were contacted via electronic communication. Only the authors of four articles replied and provided adequate information. Three potentially relevant studies whose authors did not respond to the call were excluded due to insufficient data.
Data synthesis
Based on the descriptive nature of the extracted data, we performed a synthesis without meta-analysis of the findings from the included studies, accompanied by descriptive statistics.
Results
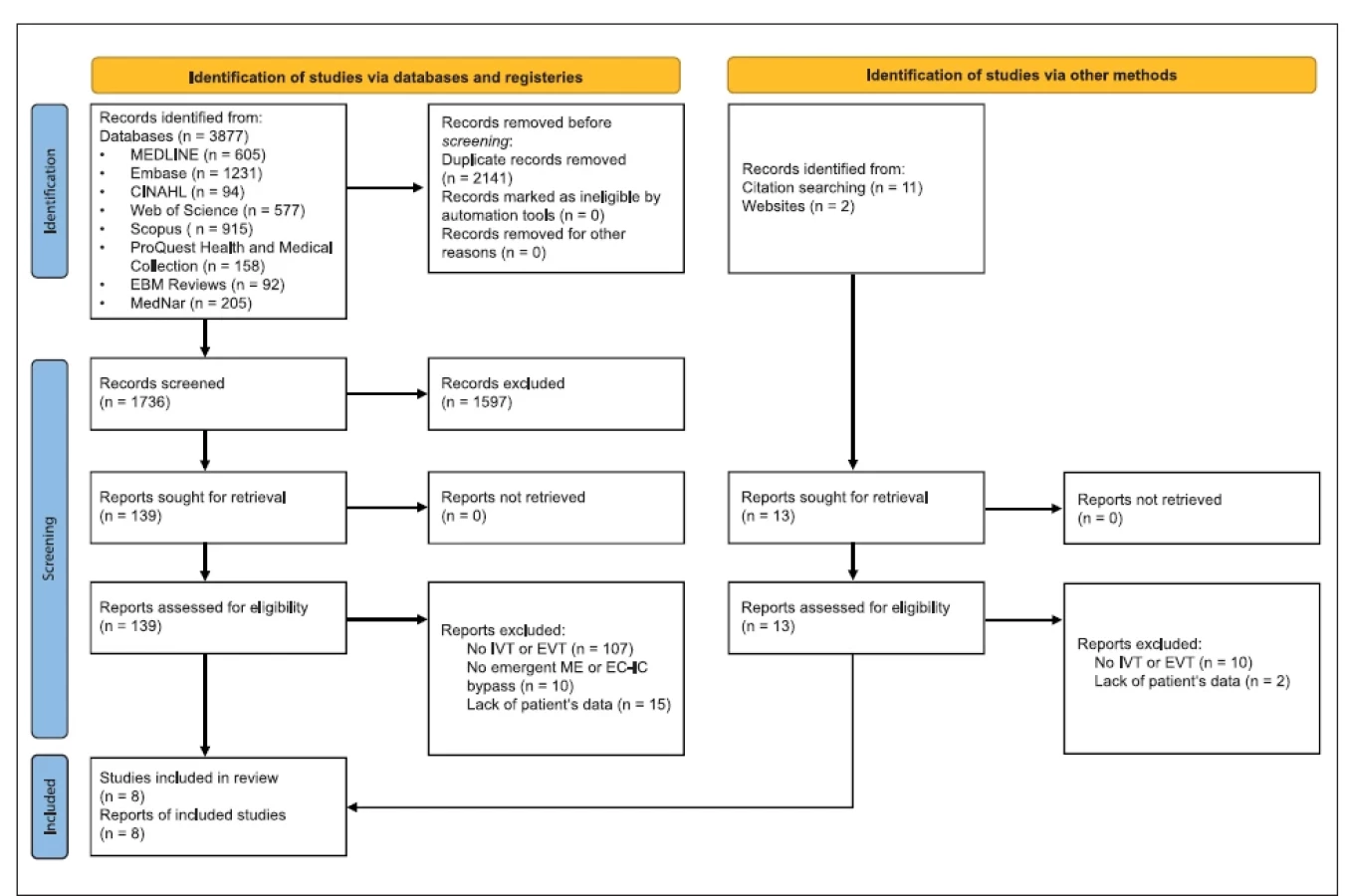
The search performed in January 2023 retrieved 3,877 records, of which 2,141 were duplicates. The titles and abstracts of 1,736 records were analysed independently by primary and secondary evaluators according to the inclusion criteria. Full texts were obtained from 139 potentially relevant reports. Another 13 potentially relevant reports were found by studying the references to the former. A total of 144 irrelevant reports were excluded from the next phase of the study. The remaining eight studies were included in this systematic review. A detailed description of the retrieval and selection of the studies is provided in the PRISMA 2020 flow diagram (Fig. 1) [20].

We critically appraised retrieved studies by the JBI Critical Appraisal Checklist for Case Reports (Tab. 1) [16]. Studies were generally reported well and in a trustworthy way. The best and worst scores were seven and five, respectively. Almost all studies clearly reported the patients’ demographic characteristics, patient history, and timeline.
Types of microsurgery
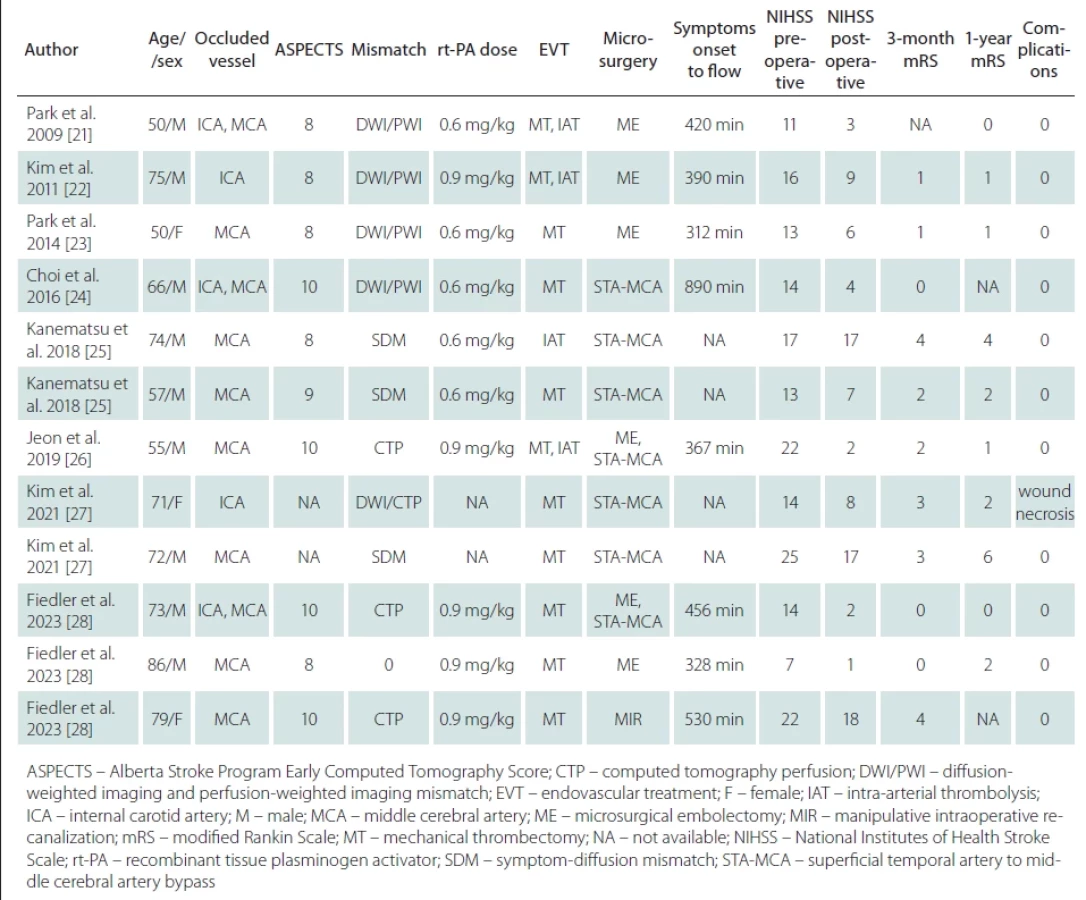
Eight relevant studies, including 12 patients aged 50–86 years were selected (Tab. 2) [21–28]. Of these, nine were male (75%). The case reports were predominantly from Asian centres, and only one study was from a European institution. ME was performed in four cases (33%), superficial temporal artery to middle cerebral artery (STA-MCA) bypass in five cases (42%), and manipulative intraoperative recanalization (MIR) in one case (8%). In two cases (16%), STA-MCA bypass was added to the ME as a flow augmentation procedure. The IVT dose was not specified in two cases. In five cases (42%) a dose of 0.6 mg/kg and in other five cases (42%) 0.9 mg/kg were used. Endovascular treatment failure was documented in all of the cases. Mismatch evaluation was based on MRI perfusion-diffusion in four cases (33%), CT perfusion-diffusion in one case (8%), CT perfusion in three cases (25%), and symptom-diffusion in three cases (25%). In one patient, no perfusion assessment was documented before surgery.
In the ME group and MIR, pterional craniotomy was used in 3/7 cases (43%), minimally invasive and rapid surgical embolectomy in 3/7 cases (43%), and lateral supraorbital craniotomy in 1/7 case (14%). The onset-to--flow time ranged from 312–420 min in the ME group and 367–456 min in the ME and EC-IC bypass combination group. In the bypass group, temporal data were not documented in four patients (80%).
Outcomes
National Institutes of Health Stroke Scale at 24 h after intervention, five and seven days after stroke, or at discharge in case of an earlier onset: Preoperatively NIHSS ranged from 7–25 points and postoperatively (1–7 days after surgery) from 1–18 points.
Modified Rankin scale at 90 days and at one year after stroke: Functional independence (mRS score 0–2) was achieved in nine patients (75%) at 3–12 months after the surgery evaluation interval. Severe neurological deficits (mRS score 4–5) persisted in two patients (17%). One patient died of lung cancer more than three months after the stroke.
mTICI: Complete mTICI 3 recanalization was achieved in all seven cases of ME and MIR.
Secondary endpoints: No haemorrhagic complications were recorded after IVT or surgery. The only complication associated with surgery was wound necrosis, which occurred in one patient (8%).
Discussion
Mechanical thrombectomy improves functional outcomes and reduces mortality of patients with ELVO at three months in comparison with pharmacological therapy alone [29]. Recent studies DEFUSE 3 and DAWN have shown that patients with penumbra-core and clinical-core mismatch benefit from reperfusion therapy even 16 and 24 h after onset, respectively [2,3]. Even the presence of collaterals on CTA plays an important role in predicting the potential benefit of endovascular treatment 6 h after symptom onset [30].
Despite advances in the latest endovascular devices, recanalization has not always been successful. Leischner et al. described three types of MT failure [12]. First, the occluded segment could not be approached due to an unsuccessful femoral artery puncture at the groin, stenosis, or elongation of the extracranial arteries. Second, the occlusion is reached but cannot be passed through using endovascular tools. Third, the passage through the occlusion site is successful; however, the retrieval of the embolus per se fails [12]. MT failure could be associated with the size and aetiology of the embolus, intracranial atherosclerosis, or endothelial damage caused during the neurointervention [13]. Availability of the endovascular treatment is an important factor as well. Some institutions do not offer neurointerventional treatment 24 h a day, seven days a week [31]. Persisting large-vessel occlusion is a strong predictor of neurological deterioration. This trend was also reported in a recently published two-centre study, EMIAS [28]. However, in a small number of patients, emergent microsurgery can provide good clinical outcome (mRS score 0–2) in 58% of patients with standard recanalization therapy failure, in contrast to control groups, where this outcome was achieved in only 10–12% of patients [28].
Microsurgical revascularization with ME or EC-IC bypass is an alternative reperfusion method. However, since the beginning of the 1970s its development has not been straightforward. The initial enthusiasm faded away after the publication of the results of the Extracranial–Intracranial Bypass Study Group in 1985 [32]. Neither the Carotid Occlusion Surgery Study (COSS) in 2011 nor the Carotid and Middle Cerebral Artery Occlusion Surgery Study (CMOSS) in 2023 changed this; furthermore, it did not show EC-IC bypass superiority in comparison with pharmacological management [33,34]. However, these trials did not study acute revascularization. In contrast, several smaller studies showed evidence of the benefit of early EC-IC bypass in the prevention of progressive neurological deficits in acute ischaemic stroke [35–38]. Recently, a quantitative radiological analysis by Jo et al. showed that perfusion status after emergent EC-IC bypass was correlated with good outcomes in patients with ELVO [39].
The STA, which serves as a bypass donor, augments the flow distal to the MCA. Direct elimination of the occlusion and potential restoration of the flow in local branching perforators are advantages of ME. In recent Japanese studies where ME was used as the first - or second-tier therapeutic modality, recanalization success rate in ELVO reached 91–100%. Functional independence (mRS score 0–2) was seen in 28.6–30% of patients, whereas 0–14.3% died [31,40,41]. Ota et al. directly compared MT and ME with no statistically significant differences. They also demonstrated a perfect microsurgical technique with a recanalization time of only 32.5 min [42]. The surgeon should be prepared for both variants of the operation. Combinations of microsurgical techniques are also discussed in this review. Surgery within 24 h of IVT remains controversial. However, no haemorrhagic complications were observed during the postoperative period in this review. Nevertheless, preoperative coagulation screening with eventual coagulation factor substitution is appropriate.
This study has few limitations. Firstly, most case reports or small cohorts included a small number of patients. Furthermore, the recording of temporal periods in acute stroke treatment was inconsistent and not in accordance with valid recommendations. However, this study has a notable strength, as it is a robustly performed systematic review with an extensive and rigorous search strategy.
Conclusion
In patients with ELVO in the anterior cerebral circulation after IVT and MT failure, ME, EC-IC bypass, or their combination appears to be a safe and potentially efficacious third-tier treatment. Further prospective comparative studies with optimal information sizes are needed to acknowledge their efficacy and safety in defining the indication criteria and potential implementation in official stroke treatment guidelines.
Funding
The study was supported by the České Budějovice Hospital, Czech Republic, project nr. 2023 01.
Conflict of interest
The authors declare they have no potential conflicts of interest concerning drugs, products, or services used in the study.
Zdroje
1. Powers WJ, Rabinstein AA, Ackerson T et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2019; 50 (12): e344–e418. doi: 10.1161/STR.0000000000000211.
2. Albers GW, Marks MP, Kemp S et al. Thrombectomy for stroke at 6 to 16 hours with selection by perfusion imaging. N Engl J Med 2018; 378 (8): 708–718. doi: 10.1056/NEJMoa1713973.
3. Nogueira RG, Jadhav AP, Haussen DC et al. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N Engl J Med 2018; 378 (1): 11–21. doi: 10.1056/NEJMoa1706442.
4. Šaňák D, Mikulík R, Tomek A et al. Doporučení pro mechanickou trombektomii akutního mozkového infarktu – verze 2019. Cesk Slov Neurol N 2019; 82/115 (6): 700–705. doi: 10.14735/amcsnn2019700.
5. Sarraj A, Hassan AE, Abraham MG et al. Trial of endovascular thrombectomy for large ischemic strokes. N Engl J Med 2023; 388 (14): 1259–1271. doi: 10.1056/ NEJMoa2214403.
6. Huo X, Ma G, Tong X et al. Trial of endovascular therapy for acute ischemic stroke with large infarct. N Engl J Med 2023; 388 (14): 1272–1283. doi: 10.1056/NEJMoa2213379.
7. Berkhemer OA, Fransen PS, Beumer D et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med 2015; 372 (1): 11–20. doi: 10.1056/NEJMoa1411587.
8. Jovin TG, Chamorro A, Cobo E et al. Thrombectomy within 8 hours after symptom onset in ischemic stroke. N Engl J Med 2015; 372 (24): 2296–2306. doi: 10.1056/ NEJMoa1503780.
9. Goyal M, Demchuk AM, Menon BK et al. Randomized assessment of rapid endovascular treatment of ischemic stroke. N Engl J Med 2015; 372 (11): 1019–1030. doi: 10.1056/NEJMoa1414905.
10. Campbell BC, Mitchell PJ, Kleinig TJ et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med 2015; 372 (11): 1009–1018. doi: 10.1056/NEJMoa1414792.
11. Saver JL, Goyal M, Bonafe A et al. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N Engl J Med 2015; 372 (24): 2285–2295. doi: 10.1056/NEJMoa1415061.
12. Leischner H, Flottmann F, Hanning U et al. Reasons for failed endovascular recanalization attempts in stroke patients. J Neurointerv Surg 2019; 11 (5): 439–442. doi: 10.1136/neurintsurg-2018-014060.
13. Maingard J, Phan K, Lamanna A et al. Rescue intracranial stenting after failed mechanical thrombectomy for acute ischemic stroke: a systematic review and meta--analysis. World Neurosurg 2019; 132: e235–e245. doi: 10.1016/j.wneu.2019.08.192.
14. Klugar M, Fiedler J, Licenik R et al. Efficacy and safety of emergent microsurgical embolectomy in patients with acute ischemic stroke after the failure of intravenous thrombolysis and mechanical thrombectomy – a systematic review protocol. Cesk Slov Neurol N 2020; 83/116 (4): 416 – 420. doi: 10.14735/amcsnn2020416.
15. Moher D, Shamseer L, Clarke M et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev 2015; 4 (1): 1. doi: 10.1186/2046-4053-4-1.
16. Moola S, Munn Z, Sears K et al. Conducting systematic reviews of association (etiology): The Joanna Briggs Institute‘s approach. Int J Evid Based Healthc 2015; 13 (3): 163–169. doi: 10.1097/XEB.0000000000000064.
17. Bramer WM, Giustini D, de Jonge GB et al. De-duplication of database search results for systematic reviews in EndNote. J Med Libr Assoc 2016; 104 (3): 240–243. doi: 10.3163/1536-5050.104.3.014.
18. Bramer W, Bain P. Updating search strategies for systematic reviews using EndNote. J Med Libr Assoc 2017; 105 (3): 285–289. doi: 10.5195/jmla.2017.183.
19. Riley DS, Barber MS, Kienle GS et al. CARE guidelines for case reports: explanation and elaboration document. J Clin Epidemiol 2017; 89 : 218–235. doi: 10.1016/j.jclinepi.2017.04.026.
20. Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021; 372: n71. doi: 10.1136/bmj.n71.
21. Park J, Hwang YH, Kim Y. Extended superciliary approach for middle cerebral artery embolectomy after unsuccessful endovascular recanalization therapy: technical note. Neurosurgery 2009; 65 (6): e1191–e1194. doi: 10.1227/01.NEU.0000351783.00831.BB.
22. Kim DW, Jang SJ, Kang SD. Emergency microsurgical embolectomy for the treatment of acute intracranial artery occlusion: report of two cases. J Clin Neurol 2011; 7 (3): 159–163. doi: 10.3988/jcn.2011.7.3.159.
23. Park J, Hwang YH, Huh S et al. Minimally invasive and rapid surgical embolectomy (MIRSE) as rescue treatment following failed endovascular recanalization for acute ischemic stroke. Acta Neurochir (Wien) 2014; 156 (11): 2041–2049. doi: 10.1007/s00701-014-2179-5.
24. Choi JH, Park HS. Emergent double-barrel bypass shortly after intravenous administration of recombinant tissue plasminogen activator for acute ischemic stroke. J Cerebrovasc Endovasc Neurosurg 2016; 18 (3): 258–263. doi: 10.7461/jcen.2016.18.3.258.
25. Kanematsu R, Kimura T, Ichikawa Y et al. Safety of urgent STA-MCA anastomosis after intravenous rt-PA treatment: a report of five cases and literature review. Acta Neurochir (Wien) 2018; 160 (9): 1721–1727. doi: 10.1007/s00701-018-3576-y.
26. Jeon HJ, Lee JY, Cho BM et al. Four-year experience using an advanced interdisciplinary hybrid operating room: potentials in treatment of cerebrovascular disease. J Korean Neurosurg Soc 2019; 62 (1): 35–45. doi: 10.3340/jkns.2018.0203.
27. Kim JH, Yoon W, Kim CK et al. Efficacy and safety of timely urgent superficial temporal artery-to-middle cerebral artery bypass surgery in patients with acute ischemic stroke: a single-institutional prospective study and a pooled analysis. Cerebrovasc Dis 2021; 50 (1): 34–45. doi: 10.1159/000512106.
28. Fiedler J, Roubec M, Grubhoffer M et al. Emergent microsurgical intervention for acute stroke after mechanical thrombectomy failure: a prospective study. J Neurointerv Surg 2023; 15 (5): 439–445. doi: 10.1136/neurintsurg-2022-018643.
29. Katsanos AH, Malhotra K, Goyal N et al. Mortality risk in acute ischemic stroke patients with large vessel occlusion treated with mechanical thrombectomy. J Am Heart Assoc 2019; 8 (21): e014425. doi: 10.1161/JAHA.119.014425.
30. Pirson FAVA, Hinsenveld WH, Goldhoorn RB, et al. MR CLEAN-LATE, a multicenter randomized clinical trial of endovascular treatment of acute ischemic stroke in The Netherlands for late arrivals: study protocol for a randomized controlled trial. Trials 2021; 22 (1): 160. doi: 10.1186/s13063-021-05092-0.
31. Inoue T, Tamura A, Tsutsumi K et al. Surgical embolectomy for large vessel occlusion of anterior circulation. Br J Neurosurg 2013; 27 (6): 783–790. doi: 10.3109/02688697.2013.793286.
32. EC/IC Bypass Study Group. Failure of extracranial-intracranial arterial bypass to reduce the risk of ischemic stroke. Results of an international randomized trial. N Engl J Med 1985; 313 (19): 1191–1200. doi: 10.1056/NEJM198511073131904.
33. Powers WJ, Clarke WR, Grubb RL Jr et al. Extracranial-intracranial bypass surgery for stroke prevention in hemodynamic cerebral ischemia: the Carotid Occlusion Surgery Study randomized trial. JAMA 2011; 306 (18): 1983–1992. doi: 10.1001/jama.2011.1610.
34. Ma Y, Wang T, Wang H et al. Extracranial-intracranial bypass and risk of stroke and death in patients with symptomatic artery occlusion: The CMOSS randomized clinical trial. JAMA 2023; 330 (8): 704–714. doi: 10.1001/jama.2023.13390.
35. Horiuchi T, Nitta J, Ishizaka S et al. Emergency EC-IC bypass for symptomatic atherosclerotic ischemic stroke. Neurosurg Rev 2013; 36 (4): 559–565. doi: 10.1007/s10143-013-0487-5.
36. Burkhardt JK, Winklhofer S, Fierstra J et al. Emergency extracranial-intracranial bypass to revascularize salvageable brain tissue in acute ischemic stroke patients. World Neurosurg 2018; 109: e476–e485. doi: 10.1016/j.wneu.2017.10.005.
37. Steinberg JA, Rennert RC, Ravina K et al. Rescue cerebral revascularization in patients with progressive steno-occlusive ischemia of the anterior intracranial circulation. World Neurosurg 2020; 133: e609–e618. doi: 10.1016/j.wneu.2019.09.102.
38. Sabouri M, Aminmansour B, Sourani A et al. The role of early superficial temporal to middle cerebral artery bypass revascularization surgery in middle cerebral artery-territory strokes: a systematic review study. Stroke Vasc Interv Neurol 2022; 00: e000281. doi: 10.1161/SVIN.121.000281.
39. Jo H, Seo D, Kim YD et al. Quantitative radiological analysis and clinical outcomes of urgent EC-IC bypass for hemodynamic compromised patients with acute ischemic stroke. Sci Rep 2022; 12 (1): 8816. doi: 10.1038/s41598-022-12728-x.
40. Hino A, Oka H, Hashimoto Y et al. Direct microsurgical embolectomy for acute occlusion of the internal carotid artery and middle cerebral artery. World Neurosurg 2016; 88 : 243–251. doi: 10.1016/j.wneu.2015.12.069.
41. Horiuchi T, Nitta J, Miyaoka Y et al. Open embolectomy of large vessel occlusion in the endovascular era: results of a 12-year single-center experience. World Neurosurg 2017; 102 : 65–71. doi: 10.1016/j.wneu.2017. 02.108.
42. Ota N, Benet A, Kusdiansah M et al. Microsurgical thrombectomy: where the ancient art meets the new era. Neurosurg Rev 2024; 47 (1): 49. doi: 10.1007/s10143-024-02281-8.
Štítky
Dětská neurologie Neurochirurgie NeurologieČlánek vyšel v časopise
Česká a slovenská neurologie a neurochirurgie

- Přibývající důkazy o přínosu léčebného konopí u pacientů s chronickou bolestí
- Nízká hladina vitamínu D v prenatálním období může zvýšit riziko roztroušené sklerózy
- Pacientům s roztroušenou sklerózou pomáhá intermitentní pohybová aktivita
- Zahájení léčby intramuskulárním interferonem beta-1a během první epizody demyelinizace u RS
- Časné klinické prediktory a progrese ireverzibilní invalidity u RS
Nejčtenější v tomto čísle
- Recommended standard of discharge report for stroke patients
- Paraneoplastic neurologic syndromes and autoimmune encephalitis – 10-year monocentric observational study
- Efficacy and safety of emergent microsurgery in acute ischaemic stroke patients after intravenous thrombolysis and mechanical thrombectomy failures – a systematic review
- An artistic portrayal of frontotemporal dementia – “děd Vševěd”: a character from the stage play “Dlouhý, Široký a Krátkozraký” by the theatrical company Divadlo Járy Cimrmana
Zvyšte si kvalifikaci online z pohodlí domova
Mazová zátka a její řešení
nový kurzVšechny kurzy