
Neurotrauma and its mortality
Authors:
D. Doll 1,2
![]() ; A. Hora 3
; A. Hora 3
![]() ; F. Burget 2-4
; F. Burget 2-4
![]() ; Z. Krška 5
; Z. Krška 5
![]()
Authors place of work:
Department of Surgery, St. Marienhospital Vechta, Academic Teaching Hospital of the MHH Hannover, Vechta, Germany
1; Baragwanath Hospital, Johannesburg, Republic of South Africa
2; 1st Surgical Department of 1st Faculty of Medicine, Charles University and General University Hospital in Prague, Czech Republic
3; Department of Disaster Medicine, University of Ostrava, Czech Republic
4; 1st Department of Surgery – Department of Abdominal, Thoracic Surgery and Traumatology, 1st Faculty of Medicine, Charles University and General University Hospital in Prague, Czech Republic
5
Published in the journal:
Rozhl. Chir., 2026, roč. 105, č. 4, s. 157-161.
Category:
Původní práce
doi:
https://doi.org/10.48095/ccrvch2026157
Summary
Introduction: Head trauma is one of the most challenging injuries a trauma victim can suffer, as it can impair airway patency and complex neurological function. Most of these patients with gunshot head injuries do not reach the hospital alive. We conducted a survey about early mortality, comparing head injuries and their outcome to other injury locations.
Methods: All patients admitted between October 2000 and May 2005 to the Trauma Unit at Chris Hani Baragwanath Hospital, Soweto, Johannesburg, South Africa. The criteria for inclusion were an injury to the cerebrocranium or other body locations with a documented evaluation of a) systolic blood pressure on admission; b) inspection of the trauma and – in case of penetrating injury – the weapon type; and c) consciousness on admission (N = 214).
Results: After data analysis, there was a 50% share of penetrating injuries in the emergency department; with half gunshot wounds and half stab wounds occurring. While blunt injuries occurred at 39%, burns were at 4%. As can be deduced, of the three major injury mechanisms of gunshot wounds, stab and blunt injuries, there is a 5% to 6% mortality for gunshot wounds and blunt patients, while stab injuries carry an early 1% mortality. Patients with head injuries die after a longer interval and reach plateau, several hours later than other observed injuries.
Conclusion: In mixed blunt and penetrating trauma injuries, head injuries account for the highest mortality rate; especially gunshot wounds of the head, with an early demise of around 40%.
Keywords:
Neurotrauma – penetrating head-injury – gunshot headwounds
Introduction
Head trauma is one of the most challenging injuries a trauma victim can suffer, as it can impair airway patency, provoke aspiration, cause torrential bleeding, and compromise neurological function. Civilian penetrating head injuries are most commonly the result of low-velocity gunshot wounds and are frequently related to suicide attempts [1]. Mortality rate is high, particularly in high-force blunt head trauma and penetrating head injuries.
Facial injuries rarely cause life-threatening problems once the airway is secured; thereafter, arterial bleeding – if present – should be controlled. The use of all available neuroprotective measures already in the prehospital setting, including empirical pharmacotherapy, is essential for survival and for the prevention of secondary brain injury [2].
Most patients with gunshot wounds to the head do not reach the hospital alive. Prehospital mortality after gunshot wounds to the head has been reported to range from 73% [3], over 85% according to Hernesniemi et al. 1979 [4], to as high as 93% as reported by Cavaliere et al. 1998 [5]. However, even among the so-called “positively selected” patients who arrive at hospital alive, in-hospital mortality remains substantial. We therefore conducted a survey on early mortality, comparing head injuries with injuries to other body regions, and analysed outcomes across different mechanisms of head injury.
Methods
All patients admitted between October 2000 and May 2005 to the Trauma Unit at Chris Hani Baragwanath Hospital, Soweto, Johannesburg, South Africa, were examined and documented with respect to injury type and injury location. Out of N = 9,010 emergency department (ED) patients, N = 8,612 trauma patients were retrospectively evaluated for inclusion in the study.
Inclusion criteria were craniocerebral injuries (traumatic brain injury – TBI) and injuries to other organ systems, with documented evaluation of: a) systolic blood pressure (BP) on admission; b) wound inspection and – if a penetrating injury was present – the weapon type; and c) level of consciousness on admission (N = 214).
The level of consciousness was assessed using the Glasgow Coma Scale (GCS) and dichotomized into GCS > 6 and GCS ≤ 6. Systolic BP was subdivided into < 100 mmHg, 100–199 mmHg, and ≥ 200 mmHg. During wound inspection, the presence or absence of brain herniation was recorded. Accordingly, patients were categorized into those with cerebrospinal fluid (CSF) leakage and those without CSF leakage, including patients with exposed brain tissue or closed head wounds without brain herniation.
Patients who were dead on arrival were excluded. Prehospital resuscitation was performed by paramedics according to Prehospital Trauma Life Support (PTLS) protocols. In-hospital resuscitation followed Advanced Trauma Life Support (ATLS) guidelines. Admission BP, brain herniation, and the level of consciousness were assessed immediately on arrival. If head dressings had been applied, wound inspection was performed in the emergency room during initial exposure, at the latest during the secondary ATLS survey.
Data analysis
A retrospective analysis of the data was performed. Data were expressed as standard error of the mean or as median with interquartile range. The two-sample Wilcoxon rank-sum test or the Kolmogorov-Smirnov test was used to compare continuous variables between groups. Correlations between quantitative variables were assessed using Spearman’s rank correlation coefficient. Logistic regression analyses (univariate and multivariate), including multivariate adaptive regression splines, were applied to assess associations between proportions and quantitative variables. The Chi--square test was used to compare proportions.
Statistical analyses were performed using SPSS for Windows (Version 14, SPSS GmbH, Munich, Germany) and R software (version 4.3.2) within the RStudio environment (version 2023.6.1.524). Statistical significance was defined as P < 0.05 (two-tailed). Survival analyses were performed using Kaplan-Meier estimates with pointwise 95% CI, as implemented in the R package “survival” (version 3.5–7). These analyses were performed for each defined therapeutic procedure. Results were plotted as percentage of recurrence-free outcomes with their 95% CI (Graph 1).
Results
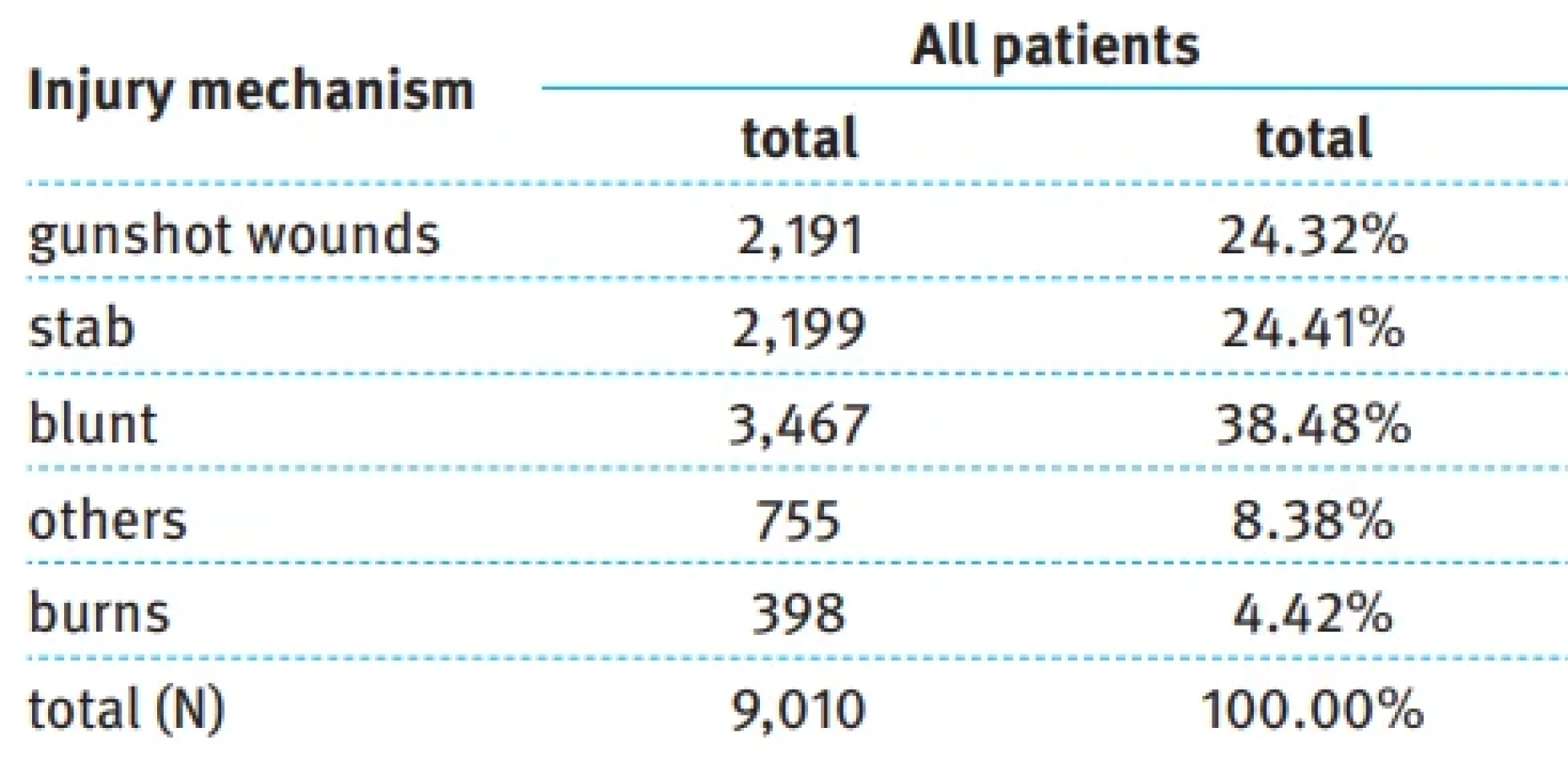
Analysis of the entire study population of all these patients with head injuries and other organ system traumas revealed that penetrating injuries accounted for approximately 50% of emergency room presentations, with gunshot wounds and stab wounds occurring in equal proportions. Blunt trauma accounted for 39% of injuries, while burns represented 4%. The category “other” included train accidents, combined assaults, and unspecified mechanisms, as well as gastrointestinal emergencies, suicide attempts, animal attacks, and lightning strikes (Tab. 1).
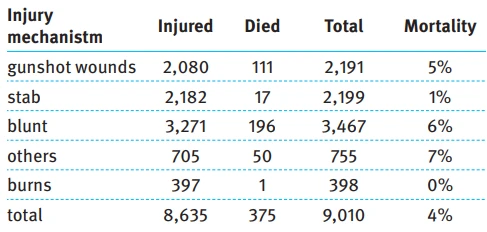
Early emergency room mortality varied according to the injury mechanism; the following table gives us numbers and frequency of deaths occurring in relation to injury mechanism (Tab. 2). Gunshot wounds and blunt trauma were associated with early mortality rates of approximately 5–6%, whereas stab wounds carried an early mortality of approximately 1%.
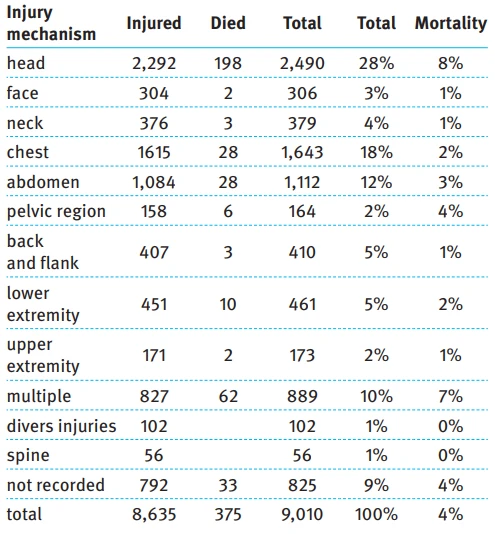
Injury location was heterogeneous, as can be seen from the following table (Tab. 3). Head injuries accounted for 28% of all admissions (2,490/9,010) and demonstrated the highest post-admission emergency room mortality compared with all other anatomical regions.
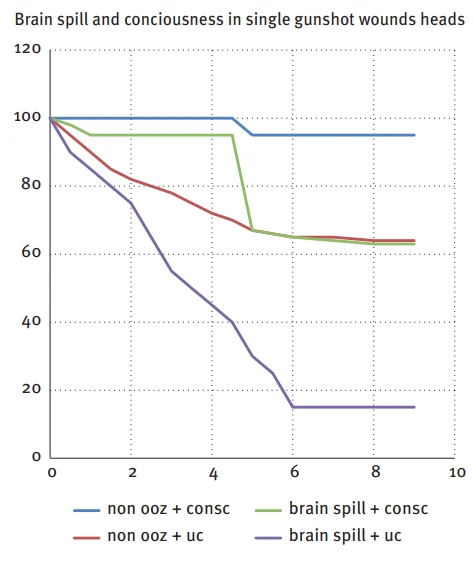
Survival characteristics not only determined overall mortality, but also the kinetics of demise. Fatal outcomes from neck, chest, and abdominal injuries occurred early after ED arrival, followed by a plateau (Fig. 1). In contrast, patients with head injuries exhibited a more protracted course, with deaths occurring over several hours before reaching a plateau, multiple hours later than other injuries (Fig. 2). Among head injuries, blunt trauma had a longer time to death compared with gunshot wounds, with 50% of deaths occurring within approximately 80 min after ED arrival.
Discussion
This analysis of 9,010 ED resuscitation room admissions from the busiest trauma centres in the Southern Hemisphere highlights several clinically relevant findings. Trauma constituted the predominant workload, with more than three-quarters of patients presenting with penetrating or blunt injuries. Gunshot wounds and blunt trauma were associated with higher mortality than stab wounds. Among patients arriving alive – even with minimal vital signs – do head injuries carried the highest emergency room mortality of all injury locations.
Gunshot wounds to the head were associated with particularly high early in-hospital mortality, approaching 40% within the first 6 hours despite optimal care. These patients therefore require immediate attention, although in mass-casualty scenarios they may be triaged as “delayed urgent” after airway stabilization.
So, gunshot wounds to the head deserve our utmost attention, knowing that in case of mass casualty their care may be seen in the “delayed urgent” category after intubation; however, gunshot wounds to the head must be distinguished from gunshot injuries to the face or neck without involvement of the neurocranium. In the absence of cervical spine injury, airway protection and haemorrhage control are the primary priorities in facial and cervical gunshot wounds. Glapa et al. reported that in a series of N = 55 facial gunshot wounds, only N = 28 patients required intubation in the ER and only N = 2 required cricothyroidotomy, with zero mortality [6].
While radiological predictors of poor outcome – such as hemispheric involvement, cerebral oedema, midline shift, and cisternal haemorrhage – are well established, rapid clinical parameters available in the emergency room are crucial for early prognostication. Admission BP, brain herniation, and level of consciousness form the basis of the ABC score proposed by Stoffel et al. [7,8], allowing rapid triage decisions in resource-limited or high-volume settings. So timely attention and early triage seem to be key in gunshot wounds of head injuries.
In a separate series of gunshot wounds of head from south Africa, Glapa analyzed 72 isolated gunshot wounds of head in N = 3,925 trauma patients in Milpark hospital in Johannesburg (11.3% of all gunshot wounds and 1.8% of all trauma patients) [6]. Of these 58 males and 14 female patients, 10 died in the ER, and 32/72 died after a median of 2 days (44%). Analyzing the outcome in 22 survivors, the most common complications were wound infection and hydrocephalus, pneumocephalus and CSF infection.
In the field, consciousness is a powerful prognostic sign for survival and for outcome [9–11]. It was Aldrich et al. who found that GCS is the far strongest predictor of mortality [12]. Of course, detailed diagnostics may follow in hospital if there is unlimited capacity for further diagnostics.
But in the field, at war, at the trauma site and if there is a mass casualty situation, the fast clinical assessment with the ABC score seems to be advantageous, if known. In an overcrowded situation, surgical time focuses on lifesaving airway and circulation interventions. The procedures focus on the Temporary Abbreviated Surgical Control (TASC) method, which conserves valuable resources such as time, operating table space, and blood [12].
Burr holes as well as craniectomies in case of brain oedema are performed, and CT diagnostics are reserved for penetrating mediastinal and abdominopelvic patients.
Limitations
This is an unselected cohort covering 4.5 years from a very busy trauma emergency department resuscitation room, comprising N = 9,010 patients. In gunshot wounds, no detailed data on calibre or weapon type were collected. All clinical notes were recorded by nursing staff during patient care. It cannot be excluded that some wound locations were incompletely documented. Nevertheless, as mortality represents a clear endpoint, we are confident that the reported mortality rates are unbiased. Patients could not have been missed, as every patient was registered even without known identity, making overestimation of mortality highly unlikely. The treatment followed ATLS and Definitive Surgical Trauma Care (DSTC) protocols, ensuring priority-driven lifesaving treatment 24/7, despite potential minor delays in mass casualty situations.
Conclusion
In a mixed trauma population, head injuries are associated with the highest mortality. Gunshot wounds to the head are associated with an early emergency department mortality rate of approximately 40%. In single-patient scenarios, maximal attention should be focused on airway protection, blood pressure control, and haemorrhage management. In mass-casualty situations, these patients may be triaged as “delayed urgent” but require continuous reassessment.
Conflict of interests
The authors declare that they have no conflict of interest related to the creation of this article, and that this article has not been published in any other journal with access to congress abstracts.
Zdroje
1. Wall N, McCrum ML, Evans HL. Surgical strategies in trauma to the head, face and neck. In: Degiannis E, Doll D, Velmahos GC (eds). Penetrating trauma. Bern: Springer 2024. 249–258.
2. Knor J, Pekara J, Pavlíček P. Závažné kraniotrauma v dětském věku: význam včasné ofenzivní terapie severe head injury in childhood: the importance of early offensive therapy. Acta Chir Orthop Traumatol Cech 2022; 89 (4): 309–311.
3. Kaufman HH, Makela ME, Lee KF et al. Gunshot wounds to the head: a perspective. Neurosurgery 1986; 18 (6): 689–695. doi: 10.1227/00006123-198606000-00002.
4. Hernesniemi J. Penetrating craniocerebral gunshot wounds in civilians. Acta Neurochir (Wien) 1979; 49 (3–4): 199–205. doi: 10.1007/BF01808959.
5. Cavaliere R, Cavenago L, Siccardi D et al. Gunshot wounds of the brain in civilians. Acta Neurochir (Wien) 1988; 94 (3–4): 133–136. doi: 10.1007/BF01435866.
6. Glapa M, Kourie JF, Doll D et al. Early management of gunshot injuries to the face in civilian practice. World J Surg 2007; 31 (11): 2104–2110. doi: 10.1007/s00268-007-9220-2.
7. Stoffel M, Hüser N, Kayser K et al. Cerebral gunshot wounds: a score based on three clinical parameters to predict the risk of early mortality. ANZ J Surg 2009; 79 (11): 789–793. doi: 10.1111/j.1445-2197.2009.05096.x.
8. Vachata P, Bolcha M, Lodin J et al. Atlanto-occipital dissociation. Rozhl Chir 2020; 99 (1): 22–28. doi: 10.33699/PIS.2020.99.1.22-28.
9. Levy ML, Masri LS, Lavine S et al. Outcome prediction after penetrating craniocerebral injury in a civilian population: aggressive surgical management in patients with admission Glasgow Coma Sscale scores of 3, 4, or 5. Neurosurgery 1994; 35 (1): 77–84. doi: 10.1227/00006123-199407000-00012.
10. Martins RS, Siqueira MG, Santos MT et al. Prognostic factors and treatment of penetrating gunshot wounds to the head. Surg Neurol 2003; 60 (2): 98–104. doi: 10.1016/s0090-3019 (03) 00302-1.
11. Shaffrey ME, Polin RS, Phillips CD et al. Classification of civilian craniocerebral gunshot wounds: a multivariate analysis predictive of mortality. J Neurotrauma 1992; 9 (Suppl 1): S279–S285.
12. Boffard KD, White J. Manual of definitive surgical trauma care. London: CRC Press 2011.
Štítky
Chirurgie všeobecná Ortopedie Urgentní medicínaČlánek vyšel v časopise
Rozhledy v chirurgii

2026 Číslo 4
- Aktuální evropská doporučení pro léčbu renální koliky v důsledku urolitiázy
- Rána vizitkou (nejen) chirurga
- Patogeneze vzniku keloidní jizvy
- Klinické studie neprokázaly vyšší účinnost obvazů s obsahem stříbra nebo medu při hojení bércových vředů
Nejčtenější v tomto čísle
- Myocardial protection during cardiac surgery – a history and review of cardioplegic solutions
- Complications in thyroid surgery – retrospective analysis
- Intensive care of the surgical patient: a perspective on high-risk interventions and common pitfalls in the surgical intensive care unit
- Neurotrauma and its mortality
Zvyšte si kvalifikaci online z pohodlí domova
Mazová zátka a její řešení
nový kurzVšechny kurzy