
Antimicrobial resistance: The complex challenge of measurement to inform policy and the public
Didier Wernli and colleagues discuss the role of monitoring in countering antimicrobial resistance.
Published in the journal:
. PLoS Med 14(8): e32767. doi:10.1371/journal.pmed.1002378
Category:
Policy Forum
doi:
https://doi.org/10.1371/journal.pmed.1002378
Summary
Didier Wernli and colleagues discuss the role of monitoring in countering antimicrobial resistance.
Summary points
Antimicrobial resistance (AMR) is developing in many pathogenic bacteria, threatening to compromise the effectiveness of crucial medical treatments.
Member States of the United Nations (UN) have reiterated their commitment to tackle AMR at the UN General Assembly held in New York City on 21 September 2016. The main challenge is now implementation of the Global Action Plan (GAP) adopted by the World Health Organization (WHO) in 2015.
There are currently large information gaps about the global governance of AMR regarding both the magnitude of the problem and national responses.
Expanding national and subnational monitoring by integrating measurements ranging from assessments of drivers of AMR to responses can increase political buy-in, societal participation, and implementation of agreed policies.
WHO should lead the way to expand monitoring of progress regarding AMR control, but a broad coalition of global health actors is needed to build a robust approach in a significant number of countries.
Antimicrobial resistance (AMR) is increasing in a wide range of pathogens, causing morbidity and mortality globally, and threatening modern medicine. While the long-term impact of AMR on human societies remains uncertain [1], the conservation of antimicrobials’ effectiveness has become an urgent priority. Tackling this ubiquitous problem requires coordination among countries and across sectors that include human and animal health, the environment, development, and trade. Previous attempts at orchestrating such a response have been insufficient, but growing concern about AMR culminated in the adoption of a Global Action Plan (GAP) by the World Health Organization (WHO) in 2015 [2], followed by a political declaration at the General Assembly of the UN in 2016 [3]. Both documents recognize AMR as an interlinked biological and social problem driven by rising world population, exacerbated by the misuse of antimicrobials in human and animal health, compounded by globalization, and made more pressing by the lack of development of new drugs. In many developing countries, a high burden of infectious diseases, rising consumption in human and animal health, limited access to quality medicine, and poor public health infrastructure create conditions for the problem to worsen [4]. Governments, which have the ultimate responsibility to tackle the problem, have now started to deliver their national strategies based on the GAP [5]. To support implementation of the GAP, we see an immediate need to expand monitoring of countries’ commitments through an integrated approach to measure AMR.
Current situation
Progress has been accomplished regarding AMR monitoring. First, knowledge about the causes, consequences, and magnitude of the problem has improved through research and better surveillance [6]. Second, the amount and quality of relevant data on AMR from local, national, or regional centers for disease control have been enhanced. Third, we understand better what needs to be measured and how to do it. A generic set of national performance indicators has been proposed [7], and WHO, which recently released a list of pathogens for which new antimicrobials are urgently needed [8], has also suggested indicators for monitoring implementation of the GAP. Additional relevant metrics include the drug resistance index, which aggregates data on bacterial resistance to multiple antibiotics and provides a useful measure of the severity of AMR [9]; and the defined daily dose per capita per year, which makes antimicrobial consumption comparable across countries [10].
However, major information gaps in the global governance of AMR—i.e., how we attempt to limit AMR globally—remain. First, surveillance data are lacking for low - and middle-income countries (LMICs). There are also more epidemiological data than WHO has access to, particularly from private hospitals and laboratories, which limits international reporting [6]. In 2014, for example, WHO reported data for carbapenem resistance in Klebsiella pneumoniae for only 71 countries out of 194 [11]. Second, variety in methodology and data collection hampers comparability across regions. Third, our understanding of the overall clinical and public health burden of AMR is limited. Fourth, few data are available on the state of national responses by countries. Finally, more needs to be done to integrate measurements on the multiple dimensions of the problem, as it is currently difficult to say whether AMR requires more attention in Italy or Canada, in Mexico or Thailand.
Rationale
Addressing these information gaps is critical for successful implementation of the GAP. First, harmonized data collection will provide useful measures for individual countries to benchmark their national and subnational performance against others and help them tackle the problem based on the best scientific evidence. This could stimulate both domestic and transnational policy debates and help AMR remain on the political agenda. Second, as for many problems of international cooperation in which countries can free ride on the efforts of others, improved monitoring will reduce information uncertainty about the current situation and responses and create better conditions for cooperation through joint effort to produce global public goods [12]. This is extremely important because the increasing global movement of people and goods means that the preservation of antibiotic susceptibility depends largely on the magnitude of the weakest national efforts. Third, regular data collection across different countries could serve as a basis for a longitudinal assessment of AMR control and contribute to improve our understanding of where, when, how, and why particular interventions work, guiding the implementation of national and subnational policies. Fourth, better monitoring may result in greater involvement of and advocacy from health professionals, patients, and consumers, whose participation is critical to tackle AMR. Ultimately, the goal of expanded monitoring is to trigger a virtuous circle in which the collection of data constantly improves our understanding and capacity to tackle AMR, which in turn calls for new evidence.
How to expand monitoring?
Because AMR control is complex, the goal should be to measure the problem and progress across its multiple dimensions while at the same time making it more tractable to policy makers and the public. Over the last decade, several instruments aimed at measuring performance in the economic, education, environmental, and health sectors have been developed [13]. Lessons learnt from their implementation—including concerns about the validity of composite indexes, which seek to summarize many dimensions in one number—call for a robust approach to ensure their effectiveness [14,15]. From the more general to the more specific, 5 design challenges are important to expand monitoring of AMR control.
The first is to choose an appropriate scientific approach to conceptualize AMR and related control efforts. Drawing from the growing literature on AMR determinants and interventions [7,16,17], a social-ecological approach that corresponds to “an integrated perspective of humans-in-nature” [18] could be adapted. The Driver-Pressure-State-Impact-Response (DPSIR) framework, which has been used by the European Environment Agency to respond to multifactorial problems, has been highly instrumental in developing pragmatic system-wide indicators in conservation biology [19]. Such a framework seems particularly appropriate to address AMR, as it integrates many variables from both the ecological and social dimensions of the problem.
The second challenge is to define what to measure. As there are different levels of economic development and multiple models of organization for the health, social, and political systems, it is critical to recognize that intrinsic diversity is an important parameter. Even ecological determinants of AMR might differ significantly across countries because of climate and other causes. Given this diversity among and within countries, AMR monitoring should be based on 3 main components: (1) the epidemiological situation and its impact on human health and societies (outcomes); (2) current drivers and practices (process), including antibiotic over-, mis-, or underuse; and (3) regulations and control policies (structures) [20]. Assessing performances within the 3 components for every country will help to identify different patterns of countries, which might be useful for screening countries at risk—for example, when a country has a weak regulatory framework, increasing antibiotic use, and a growing burden of AMR.
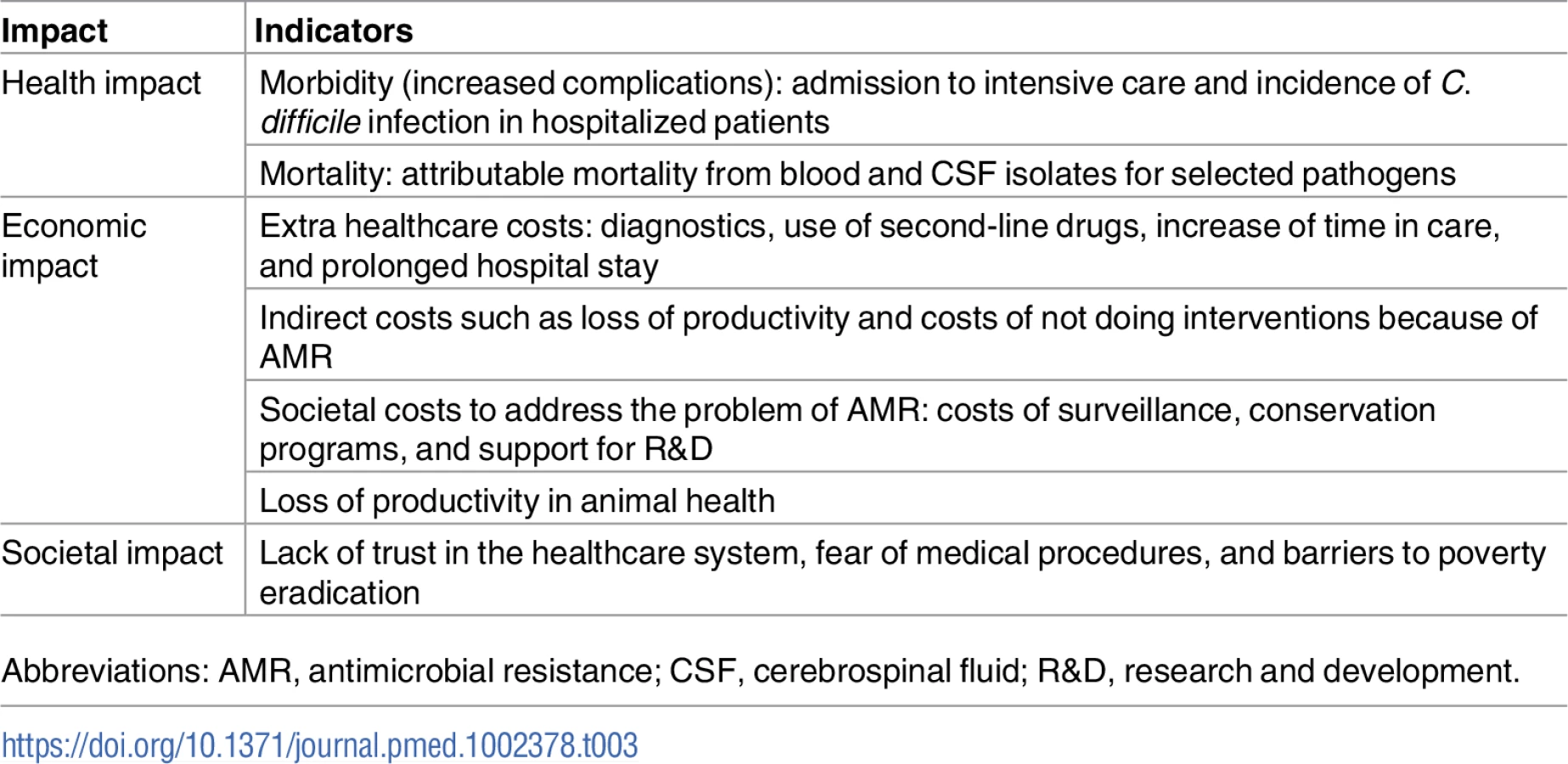
The third challenge is to select appropriate measurements from human, animal, and planetary health, as illustrated in Tables 1–3. Potential measurements that reflect the multidimensional nature of the problem are characterized in Table 1. Following the description above, the first column is organized around process, outcomes, and structures, and the second column further divides these components into the 5 categories of the DPSIR framework. The result is that measurements of process encompass both the primary “driving forces” in the use of antibiotics, such as the burden of infectious diseases or access to sanitation, and “pressures” that characterize the use of antibiotics both quantitatively and qualitatively. Measurements of outcomes can be divided into the current “state” of the problem in terms of the epidemiology of the most significant pathogens in human health and their “impact,” such as mortality and morbidity (potential measurements of state and impact are further detailed in Tables 2 and 3, respectively). Finally, measurements of structures are about the “responses,” which include the adoption of a national action plan and the enactment of regulations in human medicine and agriculture. The existence of regulations is not sufficient, as enactment does not equal enforcement. Measurements of implementation such as awareness campaigns, antibiotic stewardship programs, or surveillance capacities are critical for this component. In addition, over-the-counter availability of antibiotics can provide information about the level of enforcement. Importantly, given the delays between enactment and the effects of policies to tackle AMR, the proposed framework includes metrics appropriate to different points in the development of AMR control programs—from the early stages of the process (e.g., changes in law, knowledge, attitudes, and norms) to the outcomes (e.g., modifications of key health indicators such as the rate of multidrug-resistant bloodstream infections) [21].


The fourth challenge is data. Developing surveillance capacities is one of the core legal requirements of the International Health Regulations [27]. However, many countries have so far failed to meet this requirement. Multilateral initiatives such as the global health security agenda, a partnership of over 50 countries, can support the capacity to collect data in LMICs [28]. In addition, as surveillance programs for some specific diseases such as tuberculosis have already achieved significant coverage [29], synergies can be exploited to expand AMR surveillance. A global sentinel point prevalence study would also fill important epidemiological data gaps in LMICs. Moreover, citizen science projects have a potential for collecting more data on AMR, particularly regarding levels of resistance in the normal microbial flora [30]. Finally, the use of the DPSIR framework will help generate important new data on the regulatory component, as evaluation of this component is currently lacking. This in turn will aid the development of appropriate policies against AMR for the many countries that currently lack them.
The fifth challenge is reporting. Methodological issues should be addressed transparently, and results should be presented to avoid conveying simplistic and misleading policy messages. To ensure transparency, a data platform is needed in which information about each country will be collected and synthesized. A dashboard of indicators is likely to be necessary for a problem as complex as AMR. Because monitoring aims at informing policy, special attention must be devoted to communicating the findings online to make the most of data visualization for each country. Indicators—for example, those tracking countries’ actions against AMR—can be associated with appropriate visualization methods (e.g., traffic lights) to reflect countries’ responses so far. To increase the benefit for policy makers, countries with high or rapidly rising AMR levels will require further investigation and analysis, such as in-depth qualitative case studies that shed light on why particular AMR interventions do or do not succeed.
Next steps
Fostering a global transformation to deal with AMR [31] requires political commitment and relevant governance mechanisms [32]. An effective mechanism to curb AMR globally would be the adoption of binding targets limiting antimicrobial use [10]. While it may take a long time for states to adopt these targets, expanding monitoring of AMR control will reduce information gaps and help governments maintain their commitments to tackle the problem. WHO, in collaboration with other relevant international organizations including the World Organization for Animal Health (OIE), the Food and Agriculture Organization (FAO), and the recently created UN Interagency Coordination Group on AMR should lead the process internationally.
As the first step is to define the scope of AMR monitoring, the DPSIR framework provides an integrated approach that matches the complex nature of the problem. The creation of an independent monitoring mechanism coordinated by WHO will be the next step. The recent difficulties that have hobbled the implementation of the International Health Regulations underscore the limits of countries’ self-assessment [33], but the work conducted by the Strategic Advisory Group of Experts on Immunization demonstrates that independent monitoring is possible within the remit of the organization [34]. Since expanded monitoring will help identify countries most in need of support, it should be linked to an international funding mechanism to support conservation efforts in LMICs [35].
A robust approach to expand AMR monitoring demands a wide participation of global health actors. The recent launch of the “Conscience of Antimicrobial Resistance Accountability” (CARA), which aims to monitor the state of national responses, is a step in this direction [36]. Drawing from environmental governance, in which civil society has been playing a recognized role in collecting and evaluating policy responses by public actors [37], an international legal mechanism empowering civil society to participate in monitoring could further serve as a model for AMR governance [38]. As many high-income countries already collect AMR data on a yearly basis, academic institutions could use the DPSIR framework to develop case studies about these countries. Finally, financial support from countries and donors at the forefront of the fight against AMR is needed to strengthen WHO, the work of which has been hampered by unpredictable funding, leading (inter alia) to counterproductive internal competition. In line with the broad mandate conferred by its constitution and the recent UN political declaration [3], strong leadership by WHO is critical to orchestrate the expansion of AMR monitoring and contribute to successful AMR governance.
Zdroje
1. de Kraker MEA, Stewardson AJ, Harbarth S. Will 10 Million People Die a Year due to Antimicrobial Resistance by 2050? PLoS Med. 2016;13(11):e1002184. doi: 10.1371/journal.pmed.1002184 27898664
2. World Health Organization. Global action plan on antimicrobial resistance. Geneva: WHO 2015. Available from: http://www.who.int/iris/bitstream/10665/193736/1/9789241509763_eng.pdf?ua=1
3. United Nations. Political declaration of the high-level meeting of the General Assembly on antimicrobial resistance. New York: United Nations; 2016. Available from: http://www.un.org/pga/71/wp-content/uploads/sites/40/2016/09/DGACM_GAEAD_ESCAB-AMR-Draft-Political-Declaration-1616108E.pdf
4. Laxminarayan R, Chaudhury RR. Antibiotic Resistance in India: Drivers and Opportunities for Action. PLoS Med. 2016;13(3):e1001974. doi: 10.1371/journal.pmed.1001974 26934098
5. World Health Organization. Library of national action plans. Not dated. [cited 2017 10 July]. http://www.who.int/antimicrobial-resistance/national-action-plans/library/en/
6. Gelband H, Miller-Petrie M, Pant S, Gandra S, Levinson J, Barter D, et al. The State of the World's Antibiotics. Washington DC: The Center for Disease dynamics, Economics & Policy; 2015. Available from: https://cddep.org/sites/default/files/swa_2015_final.pdf
7. Ardal C, Outterson K, Hoffman SJ, Ghafur A, Sharland M, Ranganathan N, et al. International cooperation to improve access to and sustain effectiveness of antimicrobials. Lancet. 2016; 387(10015):296–307. doi: 10.1016/S0140-6736(15)00470-5 26603920.
8. World Health Organization. Global priority list of antibiotic-resistant bacteria to guide research, discovery, and development of new antibiotics. Geneva: WHO; 2017. Available from: http://www.who.int/medicines/publications/WHO-PPL-Short_Summary_25Feb-ET_NM_WHO.pdf?ua=1
9. Laxminarayan R, Klugman KP. Communicating trends in resistance using a drug resistance index. BMJ Open. 2011;1(2):e000135. doi: 10.1136/bmjopen-2011-000135 22102636
10. Laxminarayan R, Sridhar D, Blaser M, Wang M, Woolhouse M. Achieving global targets for antimicrobial resistance. Science. 2016; 353(6302):874–5. doi: 10.1126/science.aaf9286 27540009
11. World Health Organization. Antimicrobial resistance: Global report on surveillance. Geneva: WHO; 2014. Available from: http://apps.who.int/iris/bitstream/10665/112642/1/9789241564748_eng.pdf?ua=1
12. Koremenos B. The continent of international law: explaining agreement design. Cambridge, United Kingdom: Cambridge University Press; 2016.
13. Kelley JG, Simmons BA. Politics by number: Indicators as social pressure in international relations. Am J Polit Sci. 2015; 59(1):55–70. doi: 10.1111/ajps.12119
14. Lancet The. Why rank countries by health performance? Lancet. 2001; 357(9269):1633. doi: 10.1016/S0140-6736(00)04853-4 11425360
15. Gisselquist RM. Developing and evaluating governance indexes: 10 questions. Policy Studies. 2014; 35(5):513–31. doi: 10.1080/01442872.2014.946484
16. Holmes AH, Moore LS, Sundsfjord A, Steinbakk M, Regmi S, Karkey A, et al. Understanding the mechanisms and drivers of antimicrobial resistance. Lancet. 2016; 387(10014):176–87. doi: 10.1016/S0140-6736(15)00473-0 26603922
17. Harbarth S, Samore MH. Antimicrobial resistance determinants and future control. Emerg Infect Dis. 2005; 11(6):794–801. Epub 2005/06/21. doi: 10.3201/eid1106.050167 15963271.
18. Folke C, Biggs R, Norström AV, Reyers B, Rockström J. Social-ecological resilience and biosphere-based sustainability science. Ecol Soc. 2016; 21(3):41. doi: 10.5751/ES-08748-210341
19. Tittensor DP, Walpole M, Hill SLL, Boyce DG, Britten GL, Burgess ND, et al. A mid-term analysis of progress toward international biodiversity targets. Science. 2014; 346(6206):241–4. doi: 10.1126/science.1257484 25278504
20. Donabedian A. The quality of care. How can it be assessed? JAMA. 1988; 260(12):1743–8. 3045356.
21. Burris SC, Wagenaar A, Swanson JW, Ibrahim JK, Wood J, Mello MM. Making the Case for Laws that Improve Health: A Framework for Public Health Law Research. Milbank Q. 2010; 88(2):169–210. doi: 10.1111/j.1468-0009.2010.00595.x 20579282
22. Van Boeckel TP, Brower C, Gilbert M, Grenfell BT, Levin SA, Robinson TP, et al. Global trends in antimicrobial use in food animals. Proc Natl Acad Sci U S A. 2015;112(18):5649–54. doi: 10.1073/pnas.1503141112 25792457
23. Van Boeckel TP, Gandra S, Ashok A, Caudron Q, Grenfell BT, Levin SA, et al. Global antibiotic consumption 2000 to 2010: an analysis of national pharmaceutical sales data. Lancet Infect Dis. 2014; 14(8):742–50. doi: 10.1016/S1473-3099(14)70780-7 25022435.
24. Morgan DJ, Okeke IN, Laxminarayan R, Perencevich EN, Weisenberg S. Non-prescription antimicrobial use worldwide: a systematic review. Lancet Infect Dis. 2011;11(9):692–701. doi: 10.1016/S1473-3099(11)70054-8 21659004
25. World Health Organization. Worldwide country situation analysis: response to antimicrobial resistance. Geneva: WHO; 2015. Available from: http://apps.who.int/iris/bitstream/10665/163468/1/9789241564946_eng.pdf?ua=1&ua=1
26. Centers for Disease Control and Prevention. Antibiotic resistance threats in the United States. Atlanta: CDC; 2013. Available from https://www.cdc.gov/drugresistance/pdf/ar-threats-2013-508.pdf
27. World Health Organization. International health regulations (2005). Geneva: WHO; 2008. Available from http://apps.who.int/iris/bitstream/10665/246107/1/9789241580496-eng.pdf?ua=1
28. Global Health Security Agenda. Antimicrobial Resistance Action Package. Not dated. [cited 2017 18 March]. Available from: https://www.ghsagenda.org/packages/p1-antimicrobial-resistance.
29. World Health Organization. Drug-resistant TB: surveillance and response: supplement to global tuberculosis report. Geneva: WHO; 2014. Available from: http://www.who.int/tb/publications/global_report/gtbr14_supplement_web_v3.pdf
30. Freeman S, Okoroafor NO, Gast CM, Koval M, Nowowiejski D, O’Connor E, et al. Crowdsourced data indicate widespread multidrug resistance in skin flora of healthy young adults. J Microbiol Biol Educ. 2016; 17(1):172–82. doi: 10.1128/jmbe.v17i1.1008 27047615.
31. Jorgensen PS, Wernli D, Carroll SP, Dunn RR, Harbarth S, Levin SA, et al. Use antimicrobials wisely. Nature. 2016;537(7619):159–61. Epub 2016/09/09. doi: 10.1038/537159a 27604934.
32. Young OR. Governing complex systems: social capital for the anthropocene. Cambridge: The MIT Press; 2017.
33. Heymann DL, Chen L, Takemi K, Fidler DP, Tappero JW, Thomas MJ, et al. Global health security: the wider lessons from the west African Ebola virus disease epidemic. Lancet. 2015; 385(9980):1884–901. doi: 10.1016/S0140-6736(15)60858-3 25987157
34. Strategic Advisory Group of Experts on Immunization. Midterm review of the global vaccine action plan. Geneva: World Health Organization, 2016. Available from: http://www.who.int/immunization/sage/meetings/2016/october/1_Draft_GVAP_Assessment_report_2016_for_Yellow_Book_28_Sep_2016.pdf?ua=1
35. Mendelson M, Dar OA, Hoffman SJ, Laxminarayan R, Mpundu MM, Rottingen JA. A Global Antimicrobial Conservation Fund for Low - and Middle-Income Countries. Int J Infect Dis. 2016; 51 : 70–2. Epub 2016/09/21. doi: 10.1016/j.ijid.2016.09.016 27647658.
36. Gelband H. CARA: The Conscience of Antimicrobial Resistance Accountability, and the next big thing for CDDEP. 2016 [cited 2017 4 April]. Available from: http://www.cddep.org/blog/posts/cara_conscience_antimicrobial_resistance_accountability_and_next_big_thing_cddep#sthash.nSbsM5bO.dpuf.
37. Gemmill B, Bamidele-Izu A. The role of NGOs and civil society in global environmental governance. In: Esty DC, MH I, editors. Global environmental governance: Options and opportunities. Yale Center for Environmental Law & Policy; 2002.
38. United Nations Economic Commission for Europe. Convention on Access to Information, Public Participation in Decision-making and Access to Justice in Environmental Matters. Aarhus: UNECE; 1998. Available from: https://www.unece.org/fileadmin/DAM/env/pp/documents/cep43e.pdf.
Štítky
Interní lékařstvíČlánek vyšel v časopise
PLOS Medicine
2017 Číslo 8
- Ivabradin zlepšuje kvalitu života starších pacientů se srdečním selháním
- Fixní kombinace kandesartan/amlodipin v terapii arteriální hypertenze
- Inovace v hojení ran: krytí Zetuvit Plus Silicone Border pro optimální management exsudátu z ran
- Prognostický význam hladiny natriuretických peptidů při léčbě empagliflozinem
- Hypertrofická obstrukční kardiomyopatie ve světle moderní farmakoterapie – kazuistika
Nejčtenější v tomto čísle
- Childhood adiposity and risk of type 1 diabetes: A Mendelian randomization study
- Benefits and safety of gabapentinoids in chronic low back pain: A systematic review and meta-analysis of randomized controlled trials
- Lay worker-administered behavioral treatments for psychological distress in resource-limited settings: Time to move from evidence to practice?
- Evaluating the impact of Affordable Care Act repeal on America's opioid epidemic
Zvyšte si kvalifikaci online z pohodlí domova
Mazová zátka a její řešení
nový kurzVšechny kurzy