
INTRAVITREAL THERAPY OF ENDOGENOUS ENDOPHTALMITIS DUE TO UROSEPSIS – A CASE REPORT
Authors:
J. Valašková; J. Sitárová; V. Krásnik
Authors place of work:
Klinika Oftalmológie LF UK a UN v Bratislave, Prednosta: doc. MUDr. Vladimír Krásnik, Ph. D.
Published in the journal:
Čes. a slov. Oftal., 75, 2019, No. 5, p. 277-282
Category:
Kazuistika
doi:
https://doi.org/10.31348/2019/5/6
Summary
A case report of 58-year-old man with endogenous endophtalmitis due to urosepsis and bronchitis. Patient was hospitalized in Department of Internal Medicine another hospital. He was sent to consiliar examination to our Ophtalmology Department with worsening vision and pain in left eye one day after onset. The diagnose endogenous endophtalmitis was set. Visual aquity was a hand movement on the first visit. Intravitreal therapy was realized promptly that day, a combination of two antibiotic drugs (ceftazidim 2mg/ 0.1 ml a vankomycin 1 mg/ 0.1 ml) and antifungal agent (amfotericin B 10 μg/ 0.1 ml). This therapy was applicated 3x totally, in two weeks. Humour from anterior chamber was taken during first intravitreal application and was negative. Blood culture was positive for staphylococcus aureus. Intravenous treatment with antibiotics (gentamycin 240 mg i.v. á 24hours a amoxicilin with clavulan acid 1.2 g i.v. á 8 hod) was set for two weeks then continued antibiotic (ciprofloxacin 500 mg á 12 hours) and antifungal therapy (itrakonazol 100 mg á 12 hod) per os two months. Visual aquity of the left eye was 20/100 after four weeks and 20/40 after two months. We would like to highlight advantage of multidisciplinary co-operation.
Keywords:
endophtalmitis – intravitreal therapy – staphyloccocus aureus – urosepsis
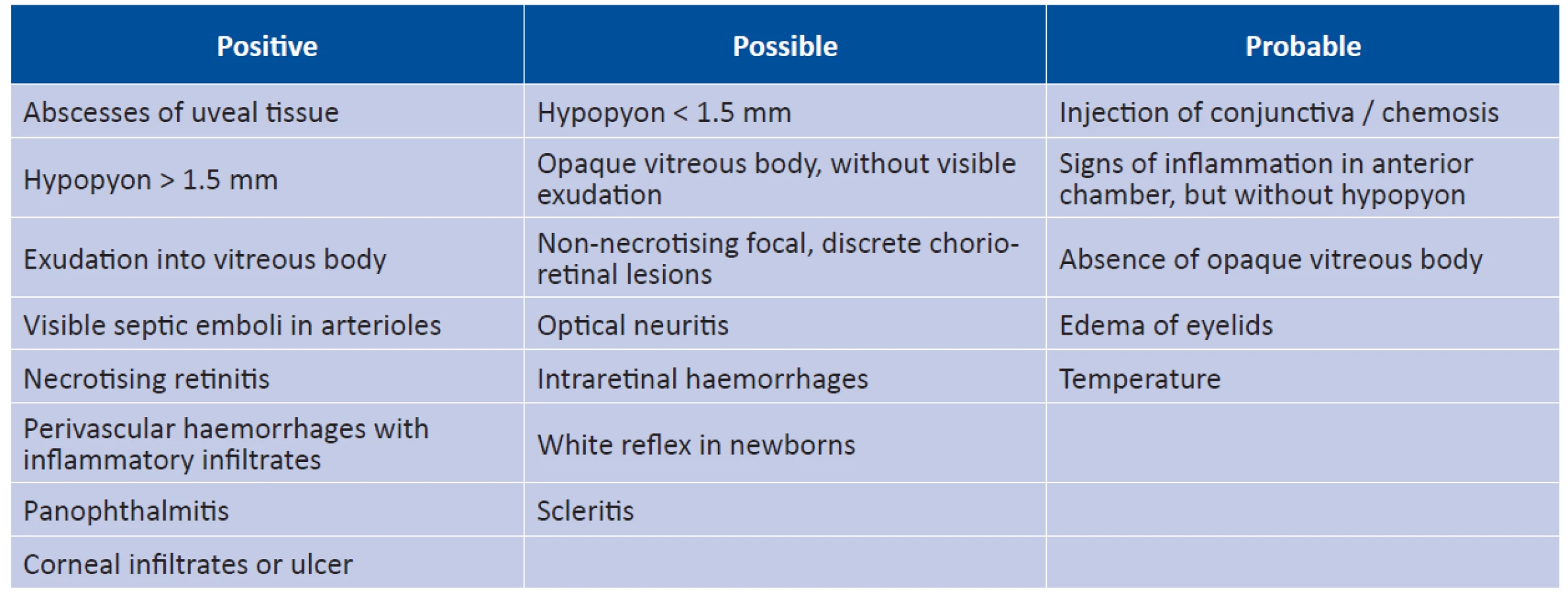
Endophthalmitis (E) is a purulent inflammation of the uvea and retina, with symptoms in the vitreous body and chamber fluid as a consequence of infection (9, 19, 27, 42). It is characterised by is progressive vitritis, histologically massive infiltration of the vitreous cavity with inflammatory cells. Endogenous endophthalmitis (EE) originates through a haematogenous dispersion of infectious agents from distal foci (8, 23, 25). Of all types of endophthalmitis it is the least common, 2-8% (5, 13, 14, 27, 36). Endogenous bacterial endophthalmitis (EBE) is a rare, acute sight-threatening condition, in the majority of cases occurring with systemic sepsis. The first case study on EBE was published in 1856 (40), and the largest cohort of patients with EBE – 342 patients – was published in 2014 (15). The foci of the primary infection are located most frequently in the lungs, liver, endocardium, soft tissues and urinary tract. Causative pathogens of EE are mostly fungi (5, 36). The pathogens responsible for EBE are dependent on geographical localisation. In Europe and the USA these are gram-positive cocci (streptococci and staphylococci), in Asia there is a predominance of gram-negative cocci (22, 34, 36). EE is often linked with a quantity of basic systemic risk factors (5-7, 9, 12, 18, 20, 23, 30, 37, 44). Among the most common are hospitalisation, diabetes mellitus, infection of the urinary tract, immune suppression, drug dependency, presence of a catheter. Liver abscesses have been recorded in connection with infection by gram-negative bacteria – Klebsiella pneumoniae (10), in which diabetes mellitus was the basic systemic risk factor in the majority of cases (3, 35). One of the most serious pathologies with a predisposition for endophthalmitis in Europe and Asia is infectious endocarditis (4, 45). Routine colonoscopy ranks among the highest risk examinations (43). Patients with Aspergillosis pulmonary infection have an abnormally increased risk of development of EE (32, 41, 42). EE has been recorded also in immune competent patients, without a fundamental predisposing cause. EE can be a manifestation of a fundamental hidden systemic focus of infection in the case of negative systemic cultures (1, 21, 24, 26, 33). The clinical symptoms and visual symptoms of EE, described in Table 1, can be easily distinguished, however documentation of this condition is more complex, even if in recent years studies have been published accentuating the need for optical coherence tomography (OCT) in EE in the case of systemic infection by fungi and yeast (2, 31). The main symptom of EE is significant change of the vitreous cavity. The vitreous cavity upon Candide albicans is manifested as vitritis or cotton wool type white retinal lesions passing into the vitreous body (28). Aspergillosis lesions may be of a whitish-yellow focal or diffuse character (1). Severe damage to the vitreous body upon EBE may thus be manifested as subretinal or choroidal abscesses (11). Methicillin-resistant staphylococcus aureus (MRSA) is linked with a higher risk of retinal detachment (9).
CASE REPORT
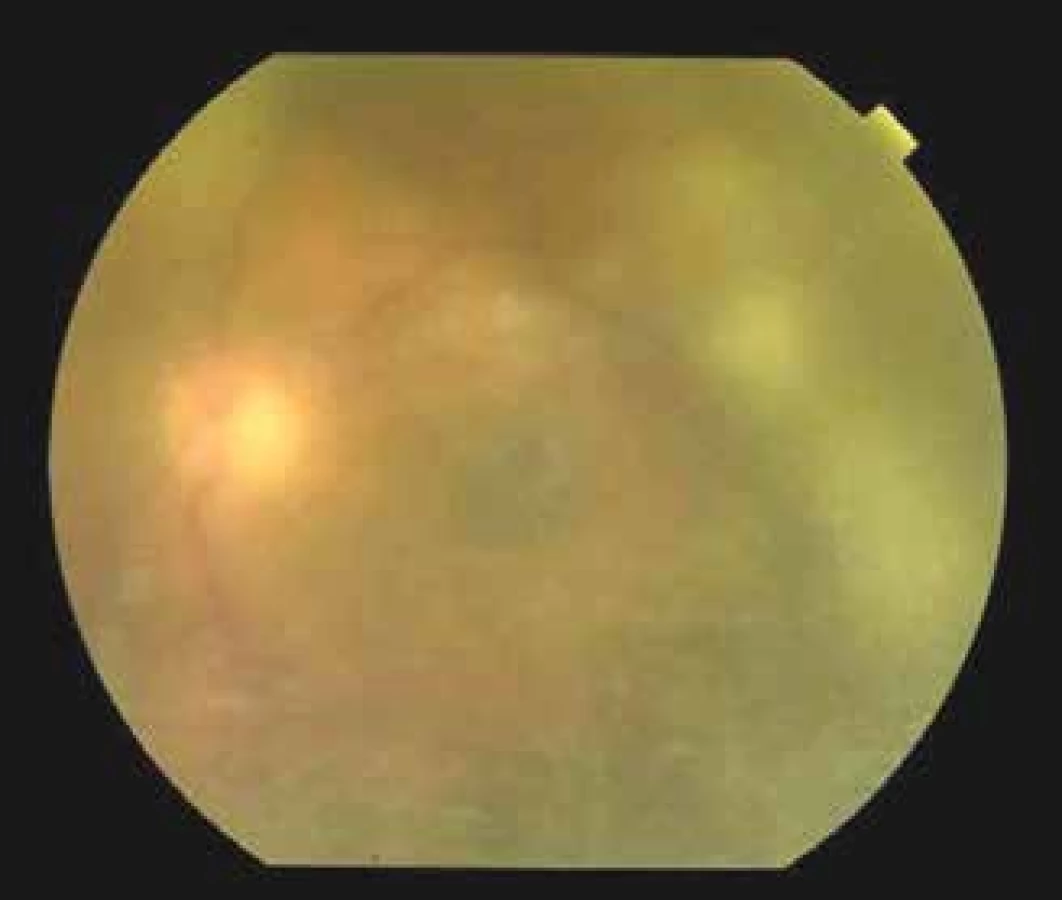
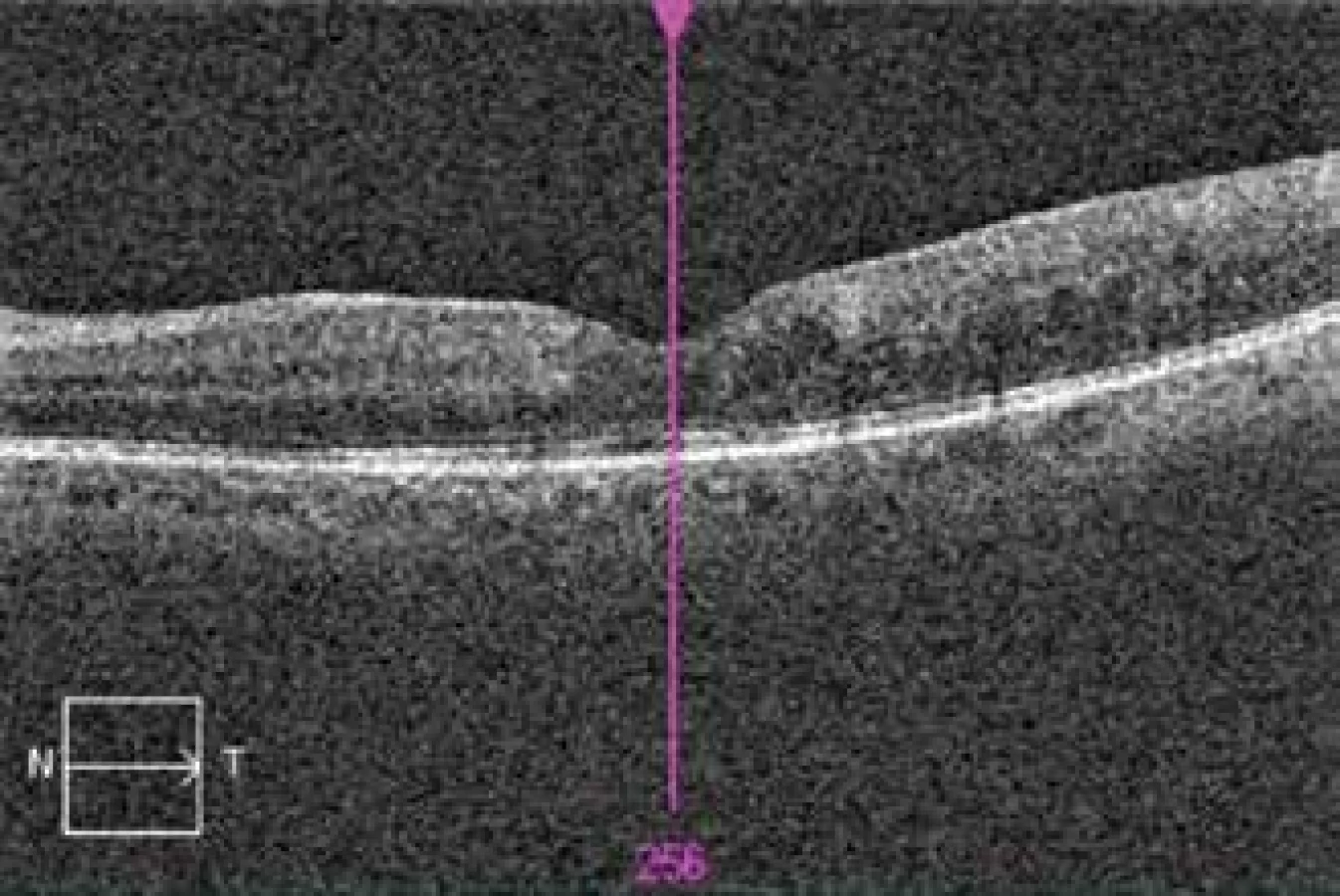
An outpatient consultation examination was conducted on a 58-year-old man with deteriorated vision and pain in the left eye (LE) which had persisted for one day. The patient was brought by ambulance from a department of internal medicine, where he had been hospitalised one day previously due to urosepsis and bronchitis, and had begun treatment with a dual combination of intravenous antibiotics ATB, gentamicin 240 mg i.v. every 24 hours and amoxicillin with clavulanic acid 1.2 g i.v. every 8 hours. The patient experienced difficulties urinating 5 days before hospitalisation, during the course of which he used ATB, cefixime orally. The patient was in an exhausted condition, with a temperature and pains, type II diabetic on insulin for 20 years, being treated for arterial hypertension. In the LE the patient could see only hand movement, intraocular pressure (IOP) of 12 torr, in the local finding there predominated ciliary injection of the eyeball, on the endothelium medium large white precipitates, hypopyon 2 mm, saturated iris with formation of posterior synechiae, pupil in 5 mm mydriasis (photo of LE, Fig. 1), lens slightly opaque, fibrotic vitreous body with inflammatory exudation (USG LO, Fig. 2), with opaque reflex of the ocular fundus. Following a local examination and taking of a blood sample, and after determining the diagnosis we decided to treat the patient with pharmaceuticals administered intravitreally in hospitalisation, together with general therapy at the department of internal medicine. During the first examination we applied a dual combination of antibiotics with an antimycotic agent intravitreally (Table 2). After disinfection of the operating field with 3% betadine solution we took a sample of the chamber fluid for a microbiological examination. We applied ceftazidime 2 mg/0.1 ml, vancomycin 1 mg/0.1 ml and amphotericin B 10 µg/0.1 ml to the vitreous cavity in a total quantity of 3x 0.05 ml. For general therapy applied at the department of internal medicine we also recommended the addition of fluconazole 200 mg i.v. á 24 hours and locally 1% Atropine gtt 3x1, moxifloxacin gtt (Vigamox) 5x1, dexamethasone gtt (Unidexa) 3x1 and nepafenac (Nevanac) 3x1. The patient was examined at our clinic every day. 48 hours after the 1st application of the medications, the patient subjectively felt better and stated less pain in the LE and better vision. Objectively visual acuity was unchanged, and the objective finding was the same, as a result of which we decided to apply a dual combination of ATB 2x intravitreally. Seven days after the 1st application the patient again stated better vision and reduction of pain of LE, visual acuity – the patient was able to count fingers in front of the eye and in the local finding there predominated regression of exudation in the vitreous body, with showing through of the disc of the optic nerve (Fig. 3). We decided to apply a dual combination of ATB 3x intravitreally. After seven days we had more results available. A sample from the anterior chamber during the first application of ATB produced a negative result, echocardiograph on the basis of suspicion of endocarditis was negative, tampon from the tonsils tested positive for Candida sp., resistant to fluconazole, which we immediately replaced with itraconazole, with positive sensitivity. The blood culture tested positive for staphylococcus aureus, on the basis of which we determined a diagnosis of endogenous bacterial endocarditis upon a background of urosepsis. With regard to the positive blood culture for bacteria and the negative results of the samples for viruses, we supported the therapy in the second week of treatment with dexamethasone 0.5 ml by parabulbar application and on the next day with triamcinolone 40 mg by retrobulbar application. Two weeks after the commencement of therapy central visual acuity (CVA) of the LE was 20/200, IOP 11 torr, and we performed OCT (Fig. 4). After two weeks of intravenous ATB therapy the patient was transferred to oral antibiotics and antimycotic agents (ciprofloxacin 500 mg á 12 hours and itraconazole 100 mg á 12 hours), which the patient used for 2 months. Four weeks after the commencement of therapy CVA in LE was 20/100, IOP 11 torr. After eight weeks CVA in LE was 20/40, IOP 11 torr, upon examination on a slit lamp the ocular fundus was without signs of inflammation (Fig. 5), which was confirmed on OCT of the macula (Fig. 6).





DISCUSSION
Endogenous endophthalmitis is a local complication of a basic pathology, at the outset mostly of unknown etiology. It is optimal to seek the cause of the general pathology in the case of onset of complications and subsequent configuration of therapy within the framework of the competences and options of the department of internal medicine, in consultation together with other specialists. In the case of suspicion of staphylococcus bacteria, on a background of the general clinical picture and confirmation on the basis of positive blood cultures, the available published works with results are not encouraging. Staphylococcus bacteria (SAB) is a serious cause of morbidity and mortality (39). Four out of 15 patients with endophthalmitis in connection with SAB died within 12 weeks of the onset of symptoms according to a prospective study from South Korea (16). According to the available studies, staphylococcus endophthalmitis, an ocular complication of staphylococcus bacteria, is linked mostly with subretinal or choroidal abscesses, for example in osteomyelitis (38) or axillary phlegmon (17), the etiology of urosepsis in the available studies was not promising. It is an advantage that ocular complications can be treated and monitored in outpatient care, with hospitalisation of the patient at a department corresponding to the basic pathology. From the perspective of the success of the local intravitreal treatment itself an important factor is time, meaning fast application of the pharmaceuticals. With regard to the unknown etiology at the outset, a wide spectrum of therapy is recommended, a dual combination of antibiotics for gram-positive and gram-negative bacteria, and antimycotic agents. Repetition of intravitreal antibiotics on the basis of the available studies is possible maximally 3x due to retinotoxicity, the second application after 24-48 hours, the third after 48-72 hours, repetition of antimycotic therapy after 20 days (29).
CONCLUSION
Endogenous endophthalmitis as a complication of a basic pathology, in this case staphylococcus bacteria, is an acute condition not only in the sense of the threat of loss of sight, but also in terms of the threat of loss of life. It is a diagnostic challenge for a broad spectrum of specialists. This is a rare diagnosis, in which there are no unequivocal, universally accepted recommendations for management of therapy. Using the example of this case report we wished to demonstrate that multi-disciplinary co-operation between an internal medicine specialist, ophthalmologist and pharmacologist, with rapid commencement of general and local therapy, can produce a favourable outcome.
The authors of the study declare that no conflict of interest exists in the compilation, theme and subsequent publication of this professional communication, and that it is not supported by any pharmaceuticals company.
Received: 18. 2. 2019
Accepted: 5. 11. 2019
Available on-line: 17. 2. 2020

MUDr. Jela Valášková
Klinika Oftalmológie LFUK a UN v Bratislave
Ružinovská 6,
82606 Bratislava
Zdroje
1. Agarwal, M., Biswas, J., Mathur, U. et al.: Aspergillus iris granuloma in a young male: a case report with review of literature. Indian J Ophthalmol, 55; 2007 : 73-4.
2. Amphornphruet, A., Silpa-Archa, S., Preble, J.M. et al.: Endogenous Cryptococcal Endophthalmitis in Immunocompetent Host: Case Report and Review of Multimodal Imaging Findings and Treatment. Ocul Immunol Inflamm, 26; 2018 : 518-522.
3. Ang, M., Jap, A., Chee, S.P.: Prognostic factors and outcomes in endogenous Klebsiella pneumoniae endophthalmitis. Am J Ophthalmol, 151; 2011 : 338-44 e2.
4. Buzzacco, D.M., Carroll, C.P.: Intravitreal daptomycin in a case of bilateral endogenous endophthalmitis. Arch Ophthalmol, 130; 2012 : 940-1.
5. Connell, P.P., O’Neill, E.C., Fabinyi, D. et al.: Endogenous endophthalmitis: 10-year experience at a tertiary referral centre. Eye (Lond), 25; 2011 : 66-72.
6. de Lima, L.M., Cecchetti, S.A., Cecchetti, D.F. et al.: Endophthalmitis: a rare but devastating metastatic bacterial complication of hemodialysis catheter-related sepsis. RenFail, 34; 2012 : 119-22.
7. Durand, M.L.: Endophthalmitis. Clin Microbiol Infect, 19; 2013 : 227-34.
8. Grixti, A., Sadri, M., Datta, A.V.: Uncommon ophthalmologic disorders in intensive care unit patients. J Crit Care, 27; 2012 : 746 e9-22.
9. Ho, V., Ho, L.Y., Ranchod, T.M. et al.: Endogenous methicillin-resistant Staphylococcus aureus endophthalmitis. Retina, 31; 2011 : 596-601.
10. Hu, C.C., Ho, J.D., Lou, H.Y. et al.: A one-year follow-up study on the incidence andrisk of endophthalmitis after pyogenic liver abscess. Ophthalmology, 119; 2012 : 2358-63.
11. Chen, K.J., Chao, A.N., Hwang, Y.S. et al.: Prognostic factors and outcomes in endogenous Klebsiella endophthalmitis. Am J Ophthalmol, 151; 2011 : 1105-6; author reply 1106-7.
12. Cheng, H.H., Ding, Y., Wu, M. et al.: Endogenous aspergillus endophthalmitis after kidney transplantation. Int J Ophthalmol, 4; 2011 : 567-71.
13. Chhablani, J.: Fungal endophthalmitis. Expert Rev Anti Infect Ther, 9; 2011 : 1191-201.
14. Jackson, T.L., Eykyn, S.J., Graham, E.M. et al.: Endogenous bacterial endophthalmitis: a 17-year prospective series and review of 267 reported cases. Surv Ophthalmol, 48; 2003 : 403-23.
15. Jackson, T.L., Paraskevopoulos, T., Georgalas, I.: Systematic review of 342 cases of endogenous bacterial endophthalmitis. Surv Ophthalmol, 59; 2014 : 627-35.
16. Jung, J., Lee, J., Yu, S.N. et al.: Incidence and Risk Factors of Ocular Infection Caused by Staphylococcus aureus Bacteremia. Antimicrob Agents Chemother, 60; 2016 : 2012-7.
17. Kansal, V., Rahimy, E., Garg, S. et al.: Endogenous methicillin-resistant Staphylococcus aureus endophthalmitis secondary to axillary phlegmon: a case report. Can J Ophthalmol, 52; 2017: e97-e99.
18. Keyashian, K., Malani, P.N.: Endophthalmitis associated with intravenous drug use. South Med J, 100; 2007 : 1219-20.
19. Khan, F.A., Slain, D., Khakoo, R.A.: Candida endophthalmitis: focus on current and future antifungal treatment options. Pharmacotherapy, 27; 2007 : 1711-21.
20. Lamaris, G.A., Esmaeli, B., Chamilos, G. et al.: Fungal endophthalmitis in a tertiary care cancer center: a review of 23 cases. Eur J Clin Microbiol Infect Dis, 27; 2008 : 343-7.
21. Lee, J.H., Kim, J.S., Park, Y.H.: Diagnosis and treatment of postpartum Candida endophthalmitis. J Obstet Gynaecol Res, 38; 2012 : 1220-2.
22. Lim, H.W., Shin, J.W., Cho, H.Y. et al.: Endogenous endophthalmitis in the Korean population: a six-year retrospective study. Retina, 34; 2014 : 592-602.
23. Lingappan, A., Wykoff, C.C., Albini, T.A. et al.: Endogenous fungal endophthalmitis: causative organisms, management strategies, and visual acuity outcomes. Am J Ophthalmol, 153; 2012 : 162-6 e1.
24. Logan, S., Rajan, M., Graham, E. et al.: A case of aspergillus endophthalmitis in an immuncompetent woman: intra-ocular penetration of oral voriconazole: a case report. Cases J, 3; 2010 : 31.
25. Lynn, W.A., Lightman, S.: The eye in systemic infection. Lancet, 364; 2004 : 1439-50.
26. Mamandhar, A., Bajracharya, L.: Endogenous Aspergillus endophthalmitis in a healthy individual. Nepal J Ophthalmol, 4; 2012 : 179-83.
27. Novosad, B.D., Callegan, M.C.: Severe bacterial endophthalmitis: towards improving clinical outcomes. Expert Rev Ophthalmol, 5; 2010 : 689-698.
28. Oude Lashof, A.M., Rothova, A., Sobel, J.D. et al.: Ocular manifestations of candidemia. Clin Infect Dis, 53; 2011 : 262-8.
29. Radhika, M., Mithal, K., Bawdekar, A. et al.: Pharmacokinetics of intravitreal antibiotics in endophthalmitis. J Ophthalmic Inflamm Infect, 4; 2014 : 22.
30. Reedy, J.S., Wood, K.E.: Endogenous Pseudomonas aeruginosa endophthalmitis: a case report and literature review. Intensive Care Med, 26; 2000 : 1386-9.
31. Rodrigues, I.A., Jackson, T.L.: A high-definition view of endogenous fungal endophthalmitis. Lancet Infect Dis, 14; 2014 : 358.
32. Sahu, C., Kumar, K., Sinha, M.K. et al.: Review of endogenous endophthalmitis during pregnancy including case series. Int Ophthalmol, 33; 2013 : 611-8.
33. Shankar, K., Gyanendra, L., Hari, S. et al.: Culture proven endogenous bacterial endophthalmitis in apparently healthy individuals. Ocul Immunol Inflamm, 17; 2009 : 396-9.
34. Sharma, S., Padhi, T.R., Basu, S. et al.: Endophthalmitis patients seen in a tertiary eye care centre in Odisha: a clinico-microbiological analysis. Indian J Med Res, 139; 2014 : 91-8.
35. Sheu, S.J., Kung, Y.H., Wu, T.T. et al.: Risk factors for endogenous endophthalmitis secondary to klebsiella pneumoniae liver abscess: 20-year experience in Southern Taiwan. Retina, 31; 2011 : 2026-31.
36. Schiedler, V., Scott, I.U., Flynn, H.W., Jr. et al.: Culture-proven endogenous endophthalmitis: clinical features and visual acuity outcomes. Am J Ophthalmol, 137; 2004 : 725-31.
37. Sridhar, J., Flynn, H.W., Jr., Kuriyan, A.E. et al.: Endogenous fungal endophthalmitis: risk factors, clinical features, and treatment outcomes in mold and yeast infections. J Ophthalmic Inflamm Infect, 3; 2013 : 60.
38. Steeples, L.R., Jones, N.P.: Staphylococcal endogenous endophthalmitis in association with pyogenic vertebral osteomyelitis. Eye (Lond), 30; 2016 : 152-5.
39. Tong, S.Y., Davis, J.S., Eichenberger, E. et al.: Staphylococcus aureus infections: epidemiology, pathophysiology, clinical manifestations, and management. Clin Microbiol Rev, 28; 2015 : 603-61.
40. Tsai, A.S., Lee, S.Y., Jap, A.H.: An unusual case of recurrent endogenous Klebsiella endophthalmitis. Eye (Lond), 24; 2010 : 1630-1.
41. Vergoulidou, M., Krause, L., Foerster, M.H. et al.: Endogenous filamentous fungal endophthalmitis--single-centre survey in patients with acute leukaemia or postallogeneic stem cell transplantation and review of the literature. Mycoses, 54; 2011: e704-11.
42. Vilela, R.C., Vilela, L., Vilela, P. et al.: Etiological agents of fungal endophthalmitis: diagnosis and management. Int Ophthalmol, 34; 2014 : 707-21.
43. Wu, A.Y., Oestreicher, J.H.: Endogenous bacterial endophthalmitis after routine colonoscopy. Can J Ophthalmol, 46; 2011 : 556-7.
44. Wu, Z.H., Chan, R.P., Luk, F.O. et al.: Review of Clinical Features, Microbiological Spectrum, and Treatment Outcomes of Endogenous Endophthalmitis over an 8-Year Period. J Ophthalmol, 2012; 2012 : 265078.
45. Yonekawa, Y., Chan, R.V., Reddy, A.K. et al.: Early intravitreal treatment of endogenous bacterial endophthalmitis. Clin Exp Ophthalmol, 39; 2011 : 771-8.
Štítky
OftalmologieČlánek vyšel v časopise
Česká a slovenská oftalmologie

2019 Číslo 5
- Selektivní laserová trabekuloplastika nesnižuje nitroční tlak více než argonová laserová trabekuloplastika
- Progresi glaukomu je třeba hodnotit strukturálními i funkčními parametry
- Ztráta centrálního vidění po filtrujících operacích glaukomu
- Od PGF-2 alfa-isopropyl esteru k latanoprostu: přehled vývoje Xalatanu
- Compliance u pacientů s glaukomem
Nejčtenější v tomto čísle
- Molecular genetic cause of achromatopsia in two patients of Czech origin
- INTRAVITREAL THERAPY OF ENDOGENOUS ENDOPHTALMITIS DUE TO UROSEPSIS – A CASE REPORT
- Sensitivity and specificity of spectral OCT in patients with early glaucoma.
- The long-term monitoring of sympathetic ophthalmia in the diagnostic and terapeutic view. Review Department of Ophthalmology
Zvyšte si kvalifikaci online z pohodlí domova
Mazová zátka a její řešení
nový kurzVšechny kurzy