
Housing Improvements and Malaria Risk in Sub-Saharan Africa: A Multi-Country Analysis of Survey Data
Lucy Tusting and colleagues investigate the association between housing quality and malaria infection in children under 5 living in sub-Saharan Africa.
Published in the journal:
. PLoS Med 14(2): e32767. doi:10.1371/journal.pmed.1002234
Category:
Research Article
doi:
https://doi.org/10.1371/journal.pmed.1002234
Summary
Lucy Tusting and colleagues investigate the association between housing quality and malaria infection in children under 5 living in sub-Saharan Africa.
Introduction
Insecticide-treated nets (ITNs) and indoor residual spraying (IRS) have contributed to a 40% reduction in malaria incidence in endemic Africa since 2000 [1]. These are highly effective methods of vector control, but additional interventions are needed for long-term, sustainable malaria control and elimination. Evidence from some tropical settings indicates that modern, well-built housing protects against malaria [2], with two postulated mechanisms. First, house entry by mosquito vectors is reduced by physical barriers such as closed eaves (the gap between the roof and top of the wall), tiled or metal roofs instead of thatch, and door and window screening [2,3]. Second, daytime indoor temperature is higher in metal-roofed than thatch-roofed houses [4], which may impair parasite development if it exceeds an optimal temperature range [5]. House improvements could be an important pillar of malaria intervention as intersectoral approaches to malaria control and elimination are increasingly encouraged [6,7], especially given the new global target to ensure universal access to adequate, safe, and affordable housing by 2030 [8]. Africa’s rapid economic and population growth—its population is projected to increase from 1.2 billion in 2015 to 2.1 billion in 2050 [9], and it has the world’s fastest rate of urbanisation [10]—presents an unrivalled opportunity to build healthier homes.
Although housing improvements show promise for malaria control, the evidence base remains narrower than that for ITNs and IRS [11]. Observational and phase II experimental studies have examined the household-level association between individual house features and entomological and epidemiological malaria outcomes in a range of African settings [3,12–14], but only one randomised controlled trial has evaluated a housing intervention against epidemiological malaria outcomes [3]. For much of sub-Saharan Africa (SSA), there are no published data, limiting our understanding of how housing may affect malaria transmission across cultures and environments [2], and there has been no comparison between housing and established malaria interventions. Here, we narrow these knowledge gaps through a detailed multi-country analysis of the relationship between housing quality and malaria. Specifically, we use Demographic and Health Surveys (DHS) and Malaria Indicator Survey (MIS) data to test the hypothesis that modern, improved housing is associated with lower odds of malaria infection in children across SSA, compared to traditional, unimproved housing. To our knowledge, this is the most comprehensive study of the relationship between housing quality and malaria across SSA to date, and the first to provide a comparison of housing quality and ITN use in relation to malaria prevalence.
Methods
Data Source
The prospective analysis plan is included as S1 Appendix. All analyses were conducted in Stata 13 (StataCorp). We analysed all DHS and MIS surveys conducted in SSA and published up to 1 July 2016 that included data collection on malaria infection in children, measured by rapid diagnostic test (RDT) or microscopy using thick or thin blood smears. DHS and MIS surveys are cross-sectional surveys designed to collect nationally representative health and sociodemographic data [15,16]. Each survey is administered approximately every 5 y in each target country, meaning that multiple independent surveys conducted in different years may be available for individual countries. The survey designs are based on a set of standard questionnaires that are adapted by country, so that the variables collected vary between each survey. The surveys have a stratified two-stage cluster design in which (i) primary sampling units (PSUs) are randomly selected from census data and (ii) households are randomly selected within PSUs from an updated enumeration list.
Housing Quality
DHS and MIS surveys classify wall, roof, and floor materials as “natural”, “rudimentary”, or “finished” [17]. While definitions vary by country and year, finished wall materials typically include cement, stone with lime or cement, bricks, cement blocks, covered adobe, and wood planks or shingles, and natural or rudimentary wall materials typically include cane, palm, dirt, bamboo or stone with mud, uncovered adobe, plywood, cardboard, and reused wood planks. Finished roof materials typically include metal, wood, calamine or cement fibre, ceramic tiles, cement, and roofing shingles, and natural or rudimentary roof materials typically include thatch, palm leaf, sod, rustic matting, bamboo, wood planks, and cardboard. Finished floor materials include parquet or polished wood, vinyl or asphalt strips, ceramic tiles, cement, and carpet, and natural or rudimentary floor materials include earth, sand, dung, wood planks, palm, and bamboo [17]. We used the DHS/MIS definitions of finished, rudimentary, and natural materials to create a binary housing quality variable comparing “modern” with “traditional” housing. Houses built with a finished wall, finished roof, and finished floor material were classified as modern, and all other houses were classified as traditional. However, in contrast to the DHS and MIS methods, we considered wood and wood shingles to be natural materials (not finished) because they may contain openings permeable to mosquitoes. We also considered sheet metal always to be a finished material because it is likely to increase indoor temperature and reduce house entry points for mosquitoes (S2 Appendix) [18]. We used the chi-squared test to compare the prevalence of modern housing in urban and rural areas and among wealthier and poorer households.
Insecticide-Treated Net Use
ITNs were defined as (i) long-lasting insecticidal nets that were ≤3 y old at the time of survey or (ii) conventional ITNs that were ≤1 y old or were retreated within the year before the survey [19].
Household Wealth
DHS and MIS household wealth index scores are developed using principal component analysis that typically includes variables describing durable asset ownership, access to utilities and infrastructure, and house construction materials [20]. We constructed a modified wealth index for each survey using the variables described in S2 Appendix. This index was to adjust for confounding and as such did not include variables related to house construction, to avoid inducing a circularity that could cause an underestimation of the association between housing quality and malaria. The assets included in the index varied by survey because of differences in survey design and because we excluded assets where <5% or >95% of households owned the asset [21]. As well as being assigned a wealth index score, households were ranked by their wealth score and grouped into tertiles to give a categorical measure of socioeconomic position for each survey.
Association between Housing Quality and Malaria Infection
For each national DHS or MIS survey, we modelled the association between housing quality (modern versus traditional) and the odds of malaria infection in children aged 0–5 y using conditional logistic regression, adjusting for (i) age, (ii) gender, (iii) ITN use, (iv) IRS in the past 12 mo, and (v) household wealth index score. The analysis was restricted to the age group 0–5 y because DHS/MIS surveys measure malaria parasitaemia within this child age range only. Age and household wealth index score were included as restricted cubic spline functions with six knots (i.e., six cut points) located at percentiles 5, 23, 41, 59, and 95 [22]. The restricted cubic spline splits the continuous variables into categories and uses separate cubic relationships to model the association within each category, except in the first and last category, where a linear relationship is assumed. The restricted cubic spline allows non-linearities to be modelled while keeping variables continuous. We used conditional logistic regression to enable the association between house type and malaria infection to be estimated within geographical clusters (PSUs), so that the analysis eliminated confounding due to inter-cluster variation in malaria transmission intensity and house construction (e.g., traditional houses might be more common in clusters with high transmission). Individual survey odds ratios (ORs) were combined to determine a summary OR across all surveys using a random effects meta-analysis. Individual and summary ORs are displayed in forest plots. We used random effects meta-regression to compare ORs between children who used ITNs and those who did not, i.e., to test for effect modification by ITN use. In this analysis, ORs were adjusted for (i) age, (ii) gender, (iii) IRS in the past 12 mo, (iv) household wealth index score, and (v) geographic cluster.
Association between Insecticide-Treated Net Use and Malaria Infection
To compare the observed association between housing quality and malaria with that between ITN use and malaria, we additionally modelled the association between reported ITN use the night before the survey and the odds of malaria infection, adjusting for (i) age, (ii) gender, (iii) IRS in the past 12 mo, (iv) household wealth index score, and (v) house type. Age and household wealth index score were included as restricted cubic spline functions with six knots. We used a conditional logistic model to adjust for cluster-level confounding.
Results
Study Population
A total of 15 DHS surveys and 14 MIS surveys conducted between 2008 and 2015 were included in the analysis (Table 1). These surveys were conducted in 21 countries: Angola, Benin, Burkina Faso, Burundi, Cameroon, Côte d’Ivoire, Democratic Republic of the Congo, The Gambia, Ghana, Guinea, Kenya, Liberia, Madagascar, Malawi, Mali, Mozambique, Nigeria, Rwanda, Senegal, Togo, and Uganda. A further two surveys (Angola 2006–2007 MIS and Rwanda 2007–2008 DHS) that measured malaria parasitaemia were excluded from the analysis because data on main wall and roof material were not recorded. Of 245,806 total households surveyed, 149,803 households had at least one resident child aged 0–5 y, yielding a total population of 284,532 children aged 0–5 y. Of these, 139,318 total children resident in 84,153 households were tested for malaria infection using microscopy (n = 131,652) or RDT (n = 138,540). Across all surveys, the average age of the children was 2.5 y, and 49.5% were female.

Housing Quality and Intervention Coverage
The proportion of houses classified as modern (versus traditional) was 34% overall and ranged from 12% (Democratic Republic of the Congo 2013–2014) to 66% (Ghana 2014). The proportion of urban (versus rural) households was 35% overall and ranged from 15% (Uganda 2009) to 50% (Ghana 2014) (Table 1). Across all surveys, a greater proportion of houses were classified as modern in urban areas (66%) than in rural areas (17%) (p < 0.001) and in the wealthiest tertile of households (68%) than in the middle (26%) and poorest tertiles (9%) (p < 0.001). ITN usage (the proportion of children reported to have slept under an ITN the night before the survey) was 47% overall and ranged from 13% (Cameroon 2011) to 75% (Burkina Faso 2014) (Table 1). There was no difference in the proportion of children sleeping under ITNs in urban areas compared to rural areas. IRS coverage (the proportion of households with IRS in the past 12 mo) was 13% overall and ranged from less than 1% (Burkina Faso 2014) to 46% (Madagascar 2011). IRS data were not recorded in eight of 29 surveys.
Malaria Infection
A total of 131,652 blood smears were taken in 28 surveys, of which 30,625 (23%) had visible malaria parasites (Table 1). Malaria infection prevalence measured by microscopy ranged from 0.5% (The Gambia 2013) to 65% (Burkina Faso 2010). A total of 138,540 RDTs were done in 29 surveys, of which 40,541 (29%) were positive. Infection prevalence by RDT ranged from 2% (The Gambia 2013; Senegal 2013–2014) to 76% (Burkina Faso 2010).
Risk Factors for Malaria Infection
Housing quality
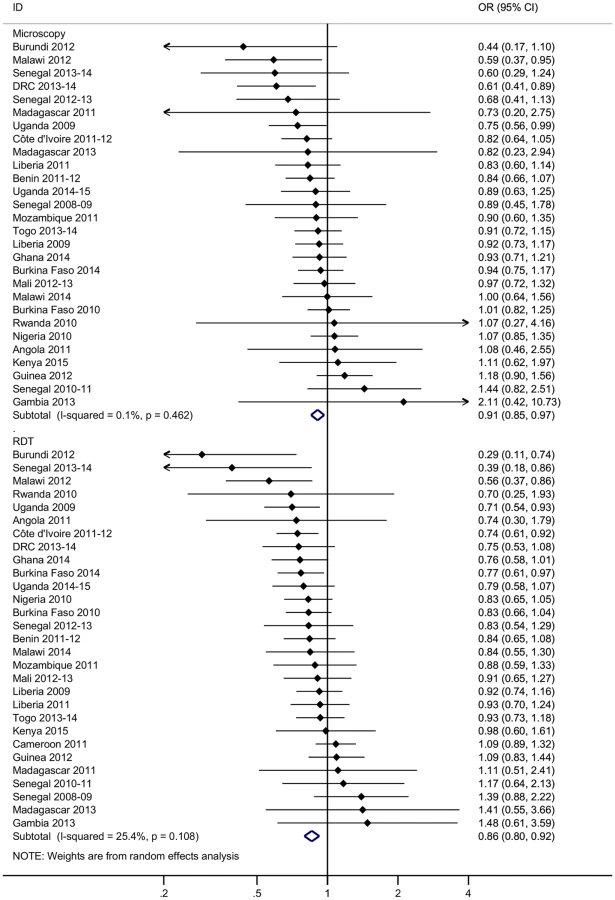
Across all surveys, adjusting for age, gender, ITN use, IRS coverage (where measured), household wealth, and cluster-level variables such as urban/rural status, modern housing was associated with a 9% reduction in the odds of malaria infection as measured by microscopy (adjusted OR 0.91, 95% CI 0.85–0.97, p = 0.003) and a 14% reduction in the odds of malaria infection as measured by RDT (adjusted OR 0.86, 95% CI 0.80–0.92, p < 0.001) (Fig 1). Unadjusted ORs and malaria prevalence in exposed and unexposed groups are provided by survey in S3 Appendix. Malaria prevalence measured by microscopy ranged from 0.4% (Madagascar 2011) to 45.5% (Burkina Faso 2010) among children living in modern houses and from 0.4% (The Gambia 2013) to 70.6% (Burkina Faso 2010) among those living in traditional houses; malaria prevalence measured by RDT ranged from 0.3% (Senegal 2013–2014) to 61.2% (Burkina Faso 2010) in modern houses and from 1.5% (The Gambia 2013) to 79.8% (Burkina Faso 2010) in traditional houses. Although modern housing was associated with a greater reduction in the odds of malaria infection among children using ITNs (microscopy: adjusted OR 0.87, 95% CI 0.79–0.96, p = 0.007; RDT: adjusted OR 0.83, 95% CI 0.75–0.92, p < 0.001) than among children not using ITNs (microscopy: adjusted OR 0.92, 95% CI 0.82–1.03, p = 0.14; RDT: adjusted OR 0.91, 95% CI 0.82–1.01, p = 0.07), there was no evidence of effect modification by ITN use (S4 Appendix).
Insecticide-treated net use
Children who were reported to have slept under an ITN the previous night had 15% to 16% lower odds of malaria infection than those not reported to have done so, adjusting for age, gender, IRS coverage (where measured), household wealth, house type, and geographic cluster (microscopy: adjusted OR 0.84, 95% CI 0.79–0.90, p < 0.001; RDT: adjusted OR 0.85, 95% CI 0.80–0.90, p < 0.001) (Fig 2).

Discussion
We have conducted a comprehensive analysis of the relationship between housing quality and malaria across SSA and, to our knowledge, provided the first direct comparison with ITNs. Our analysis of 29 DHS and MIS surveys found living in a modern house to be associated with 9% to 14% lower odds of malaria infection in children aged 0–5 y, compared to living in a traditional house. As a comparison, ITN use was associated with a 15% to 16% reduction in the odds of malaria infection. Our study indicates that poor housing quality is an important risk factor for malaria in SSA and that improved housing is a promising intervention for malaria control and elimination and prevention of reintroduction.
Well-built housing with fewer entry points for mosquitoes can help reduce malaria transmission by lowering human exposure to infectious bites [3,23]; specific features thought to deter Anopheles gambiae entry include closed eaves [12], the presence of a ceiling, and screened doors and windows [3,24]. In addition, daytime indoor temperature may be higher in houses with metal roofs and no ceilings than in traditional thatched homes [4], which, if exceeding a certain threshold [5], could lower mosquito survival [5] and reduce parasite development within the mosquito [5,25]. Our analysis was limited to assessing wall, roof, and floor material only, but finished materials are often associated with modern housing styles that incorporate other protective features such as closed eaves [14]. Since we examined only those differences in housing quality naturally present within communities, a larger difference in infection prevalence may be observed with direct interventions that specifically target house entry by mosquitoes. The results of this study concur with those of a recent systematic review and meta-analysis of housing quality and malaria, which found that residents of modern houses had 47% lower odds of malaria infection and 45%–65% lower odds of clinical malaria compared to residents of traditional houses [2]. While the reduction in the odds of malaria infection associated with modern housing was greater among ITN users than non-users, the meta-regression gave no evidence that the effect of house type varied by ITN use. Further research is needed to understand the interaction between house design and other indoor interventions. Overall, our findings are consistent with incremental house improvements having a major cumulative potential to reduce malaria transmission at the continental scale, as SSA continues to develop economically.
This is the first study to our knowledge to provide a comparison between housing and ITNs across a range of transmission settings in SSA, and the findings are likely to be generalisable across the continent. We found ITN use to be associated with a 15% to 16% reduction in the odds of malaria infection compared to non-use. Our analysis builds on an earlier study of the association between ITN use and malaria prevalence in children aged 0–5 y, which analysed seven DHS and MIS surveys and found that sleeping under an ITN was associated with a 24% reduction in malaria infection prevalence (adjusted OR 0.76, 95% CI 0.58–0.99, p = 0.001) [26]. We included 22 more surveys—and consequently a much larger sample of children—and may have better controlled for confounding due to geographical differences in transmission intensity, survey timing, and urbanicity by adjusting for geographical cluster, while the previous study adjusted for those factors individually. The association between ITNs and malaria prevalence we observed is similar to the effect found in a Cochrane review of randomized trials, where ITNs reduced malaria prevalence by 13% [27]. The association between ITNs and malaria prevalence provides a useful baseline against which housing quality compares favourably.
In response to the Sustainable Development Goals, it is now widely acknowledged that malaria must be tackled across sectors, in conjunction with national plans for economic development [6,7] and the control of other vector-borne diseases [28]. If effective in reducing malaria morbidity, improved housing could reduce transmission by vectors that have developed resistance to the insecticides currently available for IRS and long-lasting insecticidal nets [29] and therefore provide a sustainable means to contribute to malaria elimination. Rapid population growth, urbanisation, and economic development in SSA also present a major opportunity to reduce malaria transmission [30]. The urban population of Africa is expected to increase from 400 million in 2010 to 1.26 billion by 2050 and reach 50% of the total population by 2035 [31]. This growth, in the context of the New Urban Agenda for sustainable global urban development [10] and the wider suppression of malaria transmission in urban environments [32], provides an opportunity for effective long-term intervention against malaria. Indeed, we observed no difference in ITN use between urban and rural areas, but found modern housing to be more prevalent in urban areas than rural areas, and among wealthier households than poorer households. This suggests that improved housing as a malaria intervention may be complementary to the processes of urbanisation and economic development ongoing in SSA. However, this observation should not be universally generalised since urban slums can contain dense housing of poor quality, with poor drainage and environmental management, enabling malaria vectors to proliferate. Reducing urban poverty and upgrading slums is therefore of central importance to reducing malaria and other environment-linked health outcomes. In addition, metal-roofed housing is not a traditional African architectural style and may be hotter in the daytime than existing housing, so there is an ongoing need to work with housing programmes and urban planners to incorporate protective features into locally appropriate and comfortable housing designs, so that the intervention may be universally acceptable.
This study has several limitations. First, although the analysis controlled for household wealth, there may still be residual confounding if the wealth index did not fully capture differences in socioeconomic position that are associated with housing quality. While it is possible that the higher indoor temperature in metal-roofed housing without ceilings reduces mosquito survival, it is also feasible that wealthier households are more likely to contain fans or air conditioning that reduce indoor feeding by vectors. Reverse causation is also possible, if households with a greater malaria burden are consequently poorer and less able to invest in improving their homes. Second, DHS and MIS surveys are designed to be nationally representative, but matching on PSU caused observations to be dropped when the outcome did not vary within sampling units, reducing the total sample size. Therefore, our study may underestimate differences between residents of modern and traditional homes, and ITN users and non-users. Third, we observed that modern housing was associated with increased odds of malaria infection in some surveys and found an inconsistent pattern in the association of house type with malaria prevalence over time within some countries (e.g., Senegal). It is possible that our definition of the housing quality variable was sensitive to small differences in questionnaire design and did not fully capture those differences in housing quality relevant to malaria. Differences within country surveys may also have resulted from sampling differences. Together, these observations highlight the need for field studies to clarify the potential protective effect of improved housing in specific settings. Yet, overall, the use of national survey data offers the advantage of eliminating many biases typically associated with pooling observational data, including publication, selection, and measurement bias and selective outcome reporting, which were perceived to be problematic in a recent systematic review and meta-analysis of housing and malaria [2].
In conclusion, housing quality is an important risk factor for malaria across a range of transmission settings in SSA. Incremental improvements to African housing linked to socioeconomic development should be considered a major opportunity to reduce malaria transmission and a promising strategy to contribute to achieving and sustaining elimination in the long term.
Supporting Information
Zdroje
1. Bhatt S, Weiss D, Cameron E, Bisanzio D, Mappin B, Dalrymple U, et al. The effect of malaria control on Plasmodium falciparum in Africa between 2000 and 2015. Nature. 2015;526 : 207–11. doi: 10.1038/nature15535 26375008
2. Tusting LS, Ippolito M, Kleinschmidt I, Willey B, Gosling R, Dorsey G, et al. The evidence for improving housing to reduce malaria: a systematic review and meta-analysis. Malaria J. 2015;14 : 209.
3. Kirby M, Ameh D, Bottomley C, Green C, Jawara M, Milligan P, et al. Effect of two different house screening interventions on exposure to malaria vectors and on anaemia in children in The Gambia: a randomised controlled trial. Lancet. 2009;374 : 998–1009. doi: 10.1016/S0140-6736(09)60871-0 19732949
4. Knudsen J, von Seidlein L. Healthy homes in tropical zones: improving rural housing in Asia and Africa. Stuttgart: Edition Axel Menges; 2014.
5. Murdock CC, Sternberg ED, Thomas MB. Malaria transmission potential could be reduced with current and future climate change. Nature Sci Rep. 2016;6 : 27771.
6. Roll Back Malaria Partnership. Action and investment to defeat malaria 2016–2030. Geneva: Roll Back Malaria Partnership; 2015 [cited 2017 Jan 13]. http://www.rollbackmalaria.org/about-rbm/aim-2016-2030.
7. Roll Back Malaria Partnership, United Nations Development Programme. Multisectoral action framework for malaria. Geneva: Roll Back Malaria Partnership; 2013 [cited 2017 Jan 13]. http://www.rollbackmalaria.org/files/files/about/MultisectoralApproach/Multisectoral-Action-Framework-for-Malaria.pdf.
8. United Nations. Sustainable Development Goals—goal 11: make cities inclusive, safe, resilient and sustainable. New York: United Nations; 2015 [cited 2017 Jan 13]. http://www.un.org/sustainabledevelopment/cities/.
9. United Nations Department of Economic and Social Affairs Population Division. World population prospects: key findings and advance tables—2015 revision. New York: United Nations; 2015 [cited 2017 Jan 13]. https://esa.un.org/unpd/wpp/publications/files/key_findings_wpp_2015.pdf.
10. United Nations Human Settlements Programme. World cities report 2016. Urbanisation and development: emerging futures. Nairobi: United Nations Human Settlements Programme; 2016 [cited 2017 Jan 13]. http://wcr.unhabitat.org/.
11. Vector Control Working Group. Housing and malaria consensus statement. Geneva: Roll Back Malaria Partnership; 2015 Nov [cited 2017 Jan 13]. http://www.rollbackmalaria.org/files/files/working-groups/VCWG/RBM%20VCWG%20Housing%20and%20Malaria%20Consensus%20Statement_final.pdf.
12. Njie M, Dilger E, Lindsay SW, Kirby MJ. Importance of eaves to house entry by Anopheline, but not Culicine, mosquitoes. J Med Entomol. 2009;46 : 977–84.
13. Liu JX, Bousema T, Zelman B, Gesase S, Hashim R, Maxwell C, et al. Is housing quality associated with malaria incidence among young children and mosquito vector numbers? Evidence from Korogwe, Tanzania. PLoS ONE. 2014;9:e87358. doi: 10.1371/journal.pone.0087358 24505285
14. Wanzirah H, Tusting LS, Arinaitwe E, Katureebe A, Maxwell K, Rek J, et al. Mind the gap: house construction and the risk of malaria in Ugandan children. PLoS ONE. 2015;10:e0117396. doi: 10.1371/journal.pone.0117396 25635688
15. DHS Program. Survey search. Rockville (Maryland): ICF International; 2017 [cited 2017 Jan 13]. http://dhsprogram.com/What-We-Do/survey-search.cfm.
16. United Nations Children’s Fund. MICS surveys. New York: United Nations Children’s Fund; 2016 [cited 2017 Jan 13]. http://mics.unicef.org/surveys.
17. ICF International. DHS methodology. Rockville (Maryland): ICF International, 2017 [cited 2017 Jan 13]. http://dhsprogram.com/What-We-Do/Survey-Types/DHS-Methodology.cfm.
18. Bradley J, Rehman AM, Schwabe C, Vargas D, Monti F, Ela C, et al. Reduced prevalence of malaria infection in children living in houses with window screening or closed eaves on Bioko Island, Equatorial Guinea. PLoS ONE. 2013;8:e80626. doi: 10.1371/journal.pone.0080626 24236191
19. Burgert CR, Bradley SEK, Eckert E, Arnold F. Improving estimates of insecticide treated mosquito net coverage from household surveys: using geographic coordinates to account for endemicity and seasonality. DHS Analytical Studies 32. Calverton (Maryland): ICF International; 2012 Sep [cited 2017 Jan 13]. https://dhsprogram.com/pubs/pdf/AS32/AS32.pdf.
20. Rutstein SO. Steps to constructing the new DHS Wealth Index. Rockville (Maryland): ICF International; 2015 [cited 2017 Jan 13]. https://dhsprogram.com/programming/wealth%20index/Steps_to_constructing_the_new_DHS_Wealth_Index.pdf.
21. Vyas S, Kumuranayake L. Constructing socio-economic status indices: how to use principal component analysis. Health Policy Plan. 2006;6 : 459–68.
22. Harrell FE. Regression modeling strategies: with applications to linear models, logistic regression, and survival analysis. New York: Springer; 2001.
23. Kirby MJ, Green C, Milligan P, Sismanidis C, Jasseh M, Conway DJ, et al. Risk factors for house-entry by malaria vectors in a rural town and satellite villages in The Gambia. Malaria J. 2008;7 : 2.
24. Ogoma SB, Kannady K, Sikulu M, Chaki PP, Govella NJ, Mukabana WR, et al. Window screening, ceilings and closed eaves as sustainable ways to control malaria in Dar es Salaam, Tanzania. Malaria J. 2009;8 : 1.
25. Lindsay SW, Wilkins HA, Zieler RJ, Daly V, Petrarca V, Byass P. Ability of Anopheles gambiae mosquitoes to transmit malaria during the dry and wet seasons in an area of irrigated rice cultivation in The Gambia. J Trop Med Hyg. 1991;94 : 313–24. 1942209
26. Lim SS, Fullman N, Stokes A, Ravishankar N, Masiye F, Murray CJL, et al. Net benefits: a multicountry analysis of observational data examining associations between insecticide-treated mosquito nets and health outcomes. PLoS Med. 2011;8:e1001091. doi: 10.1371/journal.pmed.1001091 21909249
27. Lengeler C. Insecticide-treated bed nets and curtains for preventing malaria. Cochrane Database Syst Rev. 2004;2:CD000363.
28. World Health Organization. Handbook for integrated vector management. Geneva: World Health Organization; 2012 [cited 2017 Jan 13]. http://apps.who.int/iris/bitstream/10665/44768/1/9789241502801_eng.pdf.
29. Ranson H, Lissenden N. Insecticide resistance in African Anopheles mosquitoes: a worsening situation that needs urgent action to maintain malaria control. Trends Parasit. 2016;32 : 187–96.
30. Tusting LS, Willey B, Lines J. Building malaria out: improving health in the home. Malaria J. 2016;15 : 1–3.
31. United Nations Human Settlements Programme. The state of African cities 2014: re-imagining sustainable urban transitions. Nairobi: United Nations Human Settlements Programme; 2014 [cited 2017 Jan 13]. http://unhabitat.org/books/state-of-african-cities-2014-re-imagining-sustainable-urban-transitions/.
32. Tatem A, Gething P, Smith D, Hay S. Urbanization and the global malaria recession. Malaria J. 2013;12 : 133.
Štítky
Interní lékařstvíČlánek vyšel v časopise
PLOS Medicine
2017 Číslo 2
- Proces hojení ran krok za krokem a co ho může zkomplikovat
- Limity glykovaného hemoglobinu a význam dalších glykovaných proteinů
- Korelace dávky levothyroxinu s titrem autoimunitních protilátek u primární hypotyreózy
- Plicní hypertenze – syndrom mnoha tváří – vyžaduje přesnou diagnostiku a specializovanou léčbu
- Rána vizitkou (nejen) chirurga
Nejčtenější v tomto čísle
- Precision oncology: Charting a path forward to broader deployment of genomic profiling
- Taxes and Subsidies for Improving Diet and Population Health in Australia: A Cost-Effectiveness Modelling Study
- Refining Lung Cancer Screening Criteria in the Era of Value-Based Medicine
- Renewing ’s editorial board in times of global distraction
Zvyšte si kvalifikaci online z pohodlí domova
Mazová zátka a její řešení
nový kurzVšechny kurzy