
Does adjuvant intracameral triamcinolone acetonide increase the effectiveness of phacotrabeculectomy? A Case-Control Study
Authors:
F. Aslan; Ç. Öktem
Authors place of work:
Alaaddin Keykubat University Alanya Education and Research Hospital, Department of Ophthalmology, Antalya, TURECKO
Published in the journal:
Čes. a slov. Oftal., 76, 2020, No. 2, p. 68-76
Category:
Původní práce
doi:
https://doi.org/10.31348/2020/14
Summary
Aims: To investigate the effect of intracameral triamcinolone acetonide (TA) on surgical success in 5-fluorouracil (5-FU) supported primary phacotrabeculectomy (PT) cases.
Material and Methods: This retrospective study included 23 eyes (study group) of 23 patients who underwent TA during PT and 26 eyes (control group) of 26 patients without TA. PT patients in the study group received 1 mg TA intraoperatively at the end of surgery. Pre - and postoperative visual acuity, intraocular pressure (IOP), and number of antiglaucoma drugs used were compared. Postoperative complications and need for 5-FU injection were evaluated for both groups.
Results: Mean age was 64.1 2 ± 1.91 (48–86) years in the control group and 66.52 ± 2.02 (52–86) years in the study group (p = 0.824). Comparison of pre - and postoperative IOP values showed significant decreases in postoperative IOP levels at all-time points in both the control and study groups (p < 0.001).
The only significant difference between groups was on postoperative first day (study group: 9.22 ± 1.41 mmHg; control group: 6.35 ± 2.17 mmHg, p < 0.001). Need for postoperative 5-FU injection was significantly more common in the control group (p = 0.023).
Conclusion: Intracameral injection of 1 mg TA at the end of PT surgery did not yield superior results in postoperative IOP compared to PT alone, and the two groups showed similar IOP reduction. When given as an adjunct to PT, 1 mg TA suppresses anterior segment inflammation and reduces the need for 5-FU injection.
Keywords:
trabeculectomy – Phacotrabeculectomy – Triamcinolone acetonide – 5-Fluorouracil
None of the authors has a conflict of interest.
This study did not receive financial support from any pharmacological company.
The study was presented at the 41st winter symposium of the Turkish Ophthalmology Society in Antalya in January 2020.
INTRODUCTION
Trabeculectomy (T), which was first performed by Cairns in 1968, remains the gold standard in the surgical treatment of glaucoma [1]. Combined phacotrabeculectomy (PT) is becoming an ever more popular method for the treatment of cataract and glaucoma, which often occur concurrently in older adults. PT is beneficial for patients with regard to its lower cost, shorter time and lower exposure to anaesthesia. On the other hand, PT causes a greater reaction in the anterior chamber, because it is precisely the part of the procedure taking place in the anterior chamber that is longer and involves manipulation of the iris. This reaction may lead to fibrosis, which limits the success of the surgical procedure. Postoperative therapy with corticosteroids is used for the purpose of suppressing postoperative reaction of the anterior chamber.
Furthermore, in addition to their main anti-inflammatory effect in the anterior chamber, corticoids also reduce fibrosis thanks to their role in the further phases of healing of the surgical wound. Triamcinolone acetonide (TA) is a synthetic corticoid in the form of white crystals in water solution. Due to the fact that TA reaches high concentrations in the anterior chamber and in the subconjunctival space, if it is administered by means of intracameral injection during the course of trabeculectomy it is possible to expect it to have a sustainable anti-inflammatory and antifibrotic effect [2].
The aim of this study was to determine our surgical success within the framework of primary phacotrabeculectomy with the application of 5-fluorouracil (5-FU), with and without the use of intracameral injection of 1 mg of TA. According to our knowledge, this concerns the first study to evaluate the effectiveness of TA applied into the anterior chamber within the framework of a PT procedure, which is performed exclusively on patients with primary open-angle glaucoma (POAG).
MATERIAL AND METHOD
A retrospective evaluation was conducted of medical reports of a group of patients operated on by the same surgeon specialising in glaucoma (F.A.), in the period from September 2014 to June 2019. The study group was composed of patients who had undergone primary PT with 5-FU, who were applied 1 mg of TA by means of intracameral injection at the end of the surgical procedure, while the control group comprised patients who had undergone PT with 5-FU, but without the application of an intracameral injection of TA. Both groups included patients diagnosed with POAG and patients who had undergone their first glaucoma operation. The study was approved by the review board of the ethical commission of the Faculty of Medicine of ******* University in Alanya (1–4, 2019). Written consent was obtained from all the subjects participating in the study in accordance with the Helsinki declaration.
Patients with secondary glaucoma (e.g. neovascular, uveal, traumatic glaucoma) were excluded from the study. The study also did not include patients with a medical history of intraocular surgery for glaucoma or for other reasons: patients who had undergone laser trabeculoplasty and patients who had been observed for a period of less than 3 months. Patients in whom perioperative rupture of the posterior chamber or loss of the vitreous body occurred were also excluded from the study.
The surgical indications for PT included inability to attain target intraocular pressure (IOP) or progression of glaucomatous changes on the optic nerve papilla and loss of the visual field despite multiple medical therapy, as well as failure to adhere to treatment and the presence of severe cataract with best corrected visual acuity of 20/40 or less.
Surgical procedure
All the operations were performed in subconjunctival anaesthesia. The operating surgeon sat behind the patient’s head, peritomy was performed with the base in the fornix, haemostasis in the region of the scleral flap was achieved by wet field cautery as in the case of standard trabulectomy. A 45 degree scalpel was used to create the edges of the scleral flap with a size of 4x4 mm to a depth of two thirds of the thickness of the sclera. The scleral flap was extended 2 mm beyond the limbus with the use of a half-moon shaped scalpel. Before the performance of paracentesis, triangular sponges cut in advance were saturated in 50 mg/ml 5-FU, and were then applied for 2 minutes to the episcleral region beneath the flap. Upon removal, the sponges were counted and the surgical wound was cleansed with approximately 50 ml of balanced salt solution (BSS). After the completion of preparation of the scleral flap, the procedure continued with the performance of a corneal incision at an angle of 45 degrees in the direction away from the flap. The same instrument technique (INFINITI® Vision System, AlconLabs, Fort Worth, TX, USA) was used within the framework of all the phacoemulsification procedures. After the implantation of an intraocular lens with the use of a 45 degree scalpel, a trabeculectomy block with a depth of 3x1 mm was removed, and peripheral iridectomy was performed with the use of Vannas scissors. The scleral flap and conjunctiva were closed within the framework of standard trabeculectomy.
After the removal of the viscoelastic material, a BSS solution was used to create an anterior chamber, and 1 mg (0.025 ml) of triamcinolone acetonide (TA) (Kenacort-A® IM, Bristol-Myers Squibb) was administered. In all patients who underwent a combined surgical procedure, the main corneal incisions were closed by 10–0 sutures using monophilic material. The conjunctiva was closed by 8–0 broken sutures (vicryl). Photographs of the anterior chamber 1 hour, 1 day and 1 week after the surgical procedure on a patient who underwent PT are presented in fig. 1a, 1b and 1c.



Abbreviations: IOP – intraocular pressure, PT – phacotrabulectomy, TA – triamcinolone acetonide
Record of postoperative follow-up examinations
After the surgical procedure, all patients were administered prednisolone acetate 1 % and moxifloxacin 0.5 % every 2 hours, as well as cyclopentolate hydrochloride 1 % every 8 hours. On the 1st day after surgery, the application of cyclopentolate was terminated on the condition that the depth of the anterior chamber was found to be sufficient, or alternatively its application continued if the chamber was still shallow. Treatment with steroids and antibiotics was reduced after the first week, and terminated completely after 3 weeks. A retrospective analysis was conducted on the findings from the follow-up examinations conducted 1 day, 1 week, 1, 3 and 6 months, 1, 2 and 3 years after the operation. Complete success was defined as untreated IOP of < 21 mmHg at subsequent follow-up examinations, partial success as IOP of < 21 mmHg with administering 1 – 2 medicaments and failure as the need for more than 2 medicaments or IOP of > 21 mmHg. Measurement of IOP was performed by an applanation tonometer in all patients.
The patients were applied injections of 5-FU if signs of excessive scarring were determined upon examination on a slit lamp, such as a progressive growth of vascularisation of the conjunctiva covering the place of the surgical procedure, flattening of the filtration cushion, sudden increase of IOP or bordering of the filtration cushion. Every day an injection of 5-FU was administered in the form of adjuvant therapy, i.e. 2–5 mg with the aid of a needle 0.4 mm x 20 mm beneath an angle of 180° from the surgical wound. The dosage and number of injections was stipulated individually by the same surgeon.
Statistical analysis
Categorical variables were presented as frequency and percentage values. Continuous variables were expressed as the mean, standard deviation, median, minimum and maximum values. The correlations between the categorical variables were evaluated with the use of a chi-quadrant test. Where appropriate, the categorical variables were evaluated with the use of a Fisher-Freeman-Halton test. The Fleiss’ kappa was calculated for evaluating feasibility. Independent continuous variables were observed between the groups, with normal distribution with the use of an independent T-test. A Mann-Whitney U test was used for comparison of the variables, which did not demonstrate a normal distribution between the two independent groups. As regards dependent variables, a Wilcoxon signed-rank test was used for a comparison of the two groups and a Friedman test for comparison of a larger number of repeated measurements. The value of p < 0.05 was considered statistically significant.
Data analyses were conducted with the use of a NCSS 11 system (Number Cruncher Statistical System, statistical software 2017) and the statistical software MedCalc version 18 (MedCalc software bvba, Ostend, Belgium; http://www.medcalc.org; 2018).
Abbreviations: IOP – intraocular pressure, BCVA – best corrected visual acuity, logMAR – logarithm of minimum angle of resolution, PT – phacotrabeculectomy, TA – triamcinolone acetonide
RESULTS
The study group comprised 23 patients, who underwent PT + intracameral TA, and a control group consisting of 26 patients who underwent PT. The average age was 64.12 ± 1.91 (48–86) years in the control group and 66.52 ± 2.02 (52–86) years in the study group (p = 0.824). There was no significant difference in the sex distribution between the control and study group (p = 0.821).
Preoperative IOP was 27.17 ± 1.22 (20–43) mmHg in the study group and 26.96 ± 0.92 (19–37) mmHg in the control group (p = 0.944). The number of anti-glaucomatous drugs used postoperatively was analogous in both groups (p = 0.579). Table 1 summarises the demographic characteristics of the patients in both groups.

** Chi-quadrant test
***Fisher-Freeman-Halton test
Abbreviations: IOP – intraocular pressure, BCVA – best corrected visual acuity, logMAR – logarithm of minimum angle of resolution, PT – phacotrabeculectomy, TA – triamcinolone acetonide
Preoperative visual acuity evaluated with the aid of a logMAR optotype table was lower in the study group of patients who underwent PT with TA, though this difference was not statistically significant. Average visual acuity was 1.09 ± 0.08 (0.4–1.8) logMAR in the study group and 0.82 ± 0.02 (0.2–1.2) logMAR in the control group (p = 0.538). All PT patients showed a significant improvement of postoperative visual acuity thanks to extraction of cataract.
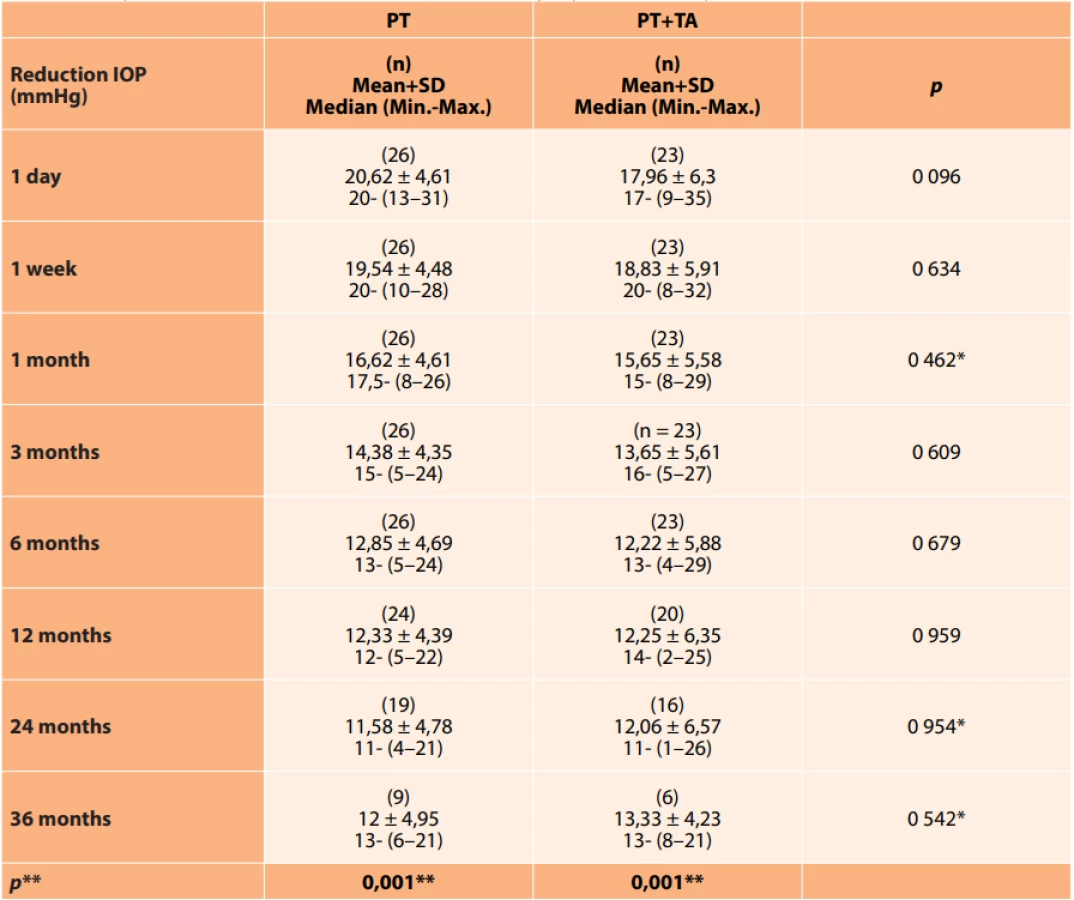
Upon a comparison of preoperative and postoperative values of IOP, a significant postoperative reduction of IOP was demonstrated at all follow-ups, in both the control and the study group (p < 0.001) (Table 2). In the control group a more significant reduction of IOP was achieved during the course of the first 2 years than in the study group. However, this difference was not statistically significant. Whereas the reduction of IOP was identical after 2 years, a greater reduction was recorded in the study group within the framework of later follow-ups; however, this difference was not statistically significant (Graph 1).
* Mann Whitney U test
**Friedman test

Abbreviations: IOP – intraocular pressure, PT – phacotrabeculectomy, TA – triamcinolone acetonide
In comparisons of postoperative levels of IOP in the control and study groups at identical points in time, the only significant difference appeared 1 day after surgery (study group: 9.22 ± 1.41 mmHg, control group: 6.35 ± 2.17 mmHg, p < 0.001) (Table 3). The degree of complete success in the study and control group reached 94.31 % and 86.96 % after 6 months, 79.17 % and 70 % after 1 year and 63.16 % and 57.75 % after 2 years. The degree of partial success in the study and control group reached 7.69 % and 13.4 % after 6 months, 20.83 % and 30 % after 1 years and 6.25 % and 10.53 % after 2 years.

* Mann Whitney U test
**Friedman test
Abbreviations: IOP – intraocular pressure, PT – phacotrabeculectomy, TA – triamcinolone acetonide
The number of anti-glaucomatous drugs administered at the last follow-up examination in the study and control group was 0 in 69.23 % (n = 18) and 47.83 % (n = 11), 1 drug in 19.23 % (n = 5) and 30.43% (n = 7), 2 drugs in 3.85 % (n = 1) and 13.04 % (n = 3) and 3 drugs in 7.69 % (n = 2) and 8.70 % (n = 2) patients. Although the number of drugs had a tendency to be higher in the study group, this difference was not statistically significant (p = 0.458).
The need for injection application of 5-FU during the course of the follow-up was determined in 30.77 % (n = 8) patients in the study group and in 63.64 % (n = 15) patients in the control group (p = 0.023). Three or more injection applications of 5-FU were required in 12.5 % (n = 1) patients in the study group and 21.43 % (n = 3) in the control group. Needling was essential in 7 patients (27 %) in the study group and 8 patients (34.7 %) in the control group.
With regard to complications, 4 patients (15.4 %) in the control group had flare in the anterior chamber, which however did not require a repeated surgical procedure, and regression took place after a few days following the local application of an increased dose of steroids. Hyphema was determined in 1 patient (3.8 %), and was treated conservatively. Ablation of the choroid was determined in 2 patients (7.6 %); spontaneous regression occurred in one of these. The other patient had a shallow anterior chamber, and resuturing was required for its restoration and adjustment of excess filtration.
Within the framework of the study group, increased IOP was recorded in 2 patients (8.6 %), which required repeated trabeculectomy 3 years after the operation, 1 patient (4.3 %) had pseudohypopyon and in 2 patients (8.6 %) a shallow anterior chamber persisted. In one patient the complaints were resolved by the application of viscoelastic material into the anterior chamber, but in the other eye it was necessary to perform resuturing due to excess filtration. One patient in the study group had optic capture and underwent surgical correction of an IOL. None of the patients in the study group manifested hyphema. Neither endophthalmitis nor flare were determined in either group.
DISCUSSION
Thanks to advances in the surgical treatment of cataract and the development of phacoemulsification with small incisions, a combination of cataract removal and trabeculectomy has now become the easiest and most common method. However, several studies have demonstrated that trabeculectomy alone helps achieve a more significant reduction of IOP than combined PT [2,3].
In a study from 2003, Lochend et al. compared PT and trabeculectomy without accessory antimetabolites in patients with chronic open-angle glaucoma, who were observed on average for a period of 29 months; reduction of postoperative IOP by 11.0 ± 1.4 mmHg in the case of trabeculectomy and 6.7 ± 2.1 mmHg in the case of PT (p = 0.0017) [2]. The authors recorded perioperative complications in only one patient from the PT group. On the other hand, Choy recorded a level of IOP of 15.00 ± 4.86 and 14.3 ± 4.28 mmHg within the framework of a follow-up examination 3 months after surgery in a study which compared 18 T and 20 PT procedures without antimetabolites in patients of Chinese origin with primary open-angle glaucoma (POAG) and secondary glaucoma [3].
In our study, after 3 months the average IOP values in patients with POAG who had undergone PT and PT plus TA reached the level of 12.58 ± 1.9 and 13.52 ± 2.25 mmHg. The main difference between our study and the above-presented study is the homogeneity of our group of patients (POAG) and the use of adjuvant TA in PT procedures in patients from our study group.
In a study from 2006, in which patients were applied mytomycin C (MMC) over an average observation period of 2 years, Murthy et al. recorded a reduction of IOP by 10.87 ± 8.33 mmHg within the framework of T + MMC and by 6.15 ± 7.01 mmHg within the framework of PT + MMC performed in a single location [4]. No difference in the degree of complications was determined between the two groups. In another study from 2006, they compared the results of T+5-FU and PT+5-FU, and determined that preoperative IOP was higher in the T group. After one year IOP was reduced by 11.2 mmHg in the T group and by 7.3 mm Hg in the PT group. Furthermore, within the framework of the subsequent follow-up examinations, the PT group required more 5-FU injection applications [5].
In our study, we achieved a reduction of IOP by 12.33 mmHg in the PT group and by 12.25 mmHg in the PT + TA group 1 year after the performance of the surgical procedure. These values were higher than the values referred by Chang et al., which can be attributed to the difference in the postoperative levels of IOP and the heterogeneity of their study group [5]. The average preoperative level of IOP was 23.4 mmHg in the PT group in the study by Chang et al., in comparison with 27.17 mmHg in the PT group in our study. In accordance with their findings, we also recorded a significantly higher need for 5-FU during the course of subsequent follow-ups in our PT group (p = 0.023). Reduction of the number of 5-FU injection applications and the frequency of use of intracameral injections of 1 mg TA indicates that TA has a sufficient antifibrotic impact on the healing of subconjunctival and episcleral wounds. According to our knowledge, this concerns the first study to evaluate the effectiveness of TA applied into the anterior chamber within the framework of a PT procedure performed on patients with POAG.
Studies evaluating trabulectomy and PT separately have recorded average postoperative IOP of the level of 13 mmHg and an average reduction of IOP by 10 mmHg in the case of trabeculectomy without accessory antimetabolites [6]. As regards trabeculectomy performed with the use of accessory antimetabolites, average IOP did not exceed 12 mmHg [7,8]. IOP values also increase with a longer period of subsequent follow-up examinations [9,10]. In the case of UP, the average postoperative increase of IOP reached 15 mmHg, and the average reduction was 6–7 mmHg [11,12]. In our study, the average increase of IOP in the PT group was 12 mmHg, in the PT + TA group 13 mmHg.
In contrast with other studies comparing T and PT procedures, the IOP values recorded in our study on the first day after surgery were significantly higher in the PT + TA group compared with the PT group. However, at further subsequent follow-ups we did not record this difference in IOP values. We believe that this initial increase of pressure may be linked with mechanical occlusion TA in the trabecular region as a consequence of its particle structure rather than due to the effect of steroids.
Although no difference in the level of IOP has been referred in the case of one-side and two-side PT, it has been demonstrated that the one-side method required a shorter operation time and caused less damage to the corneal endothelium [13]. A meta-analysis evaluating 10 different studies on PT determined that the results relating to IOP, visual acuity and administration of medicaments after surgery [14] were similar. Within the framework of our combined procedure, we used the two-side method.
However, after phacoemulsification and implantation of an IOL before the removal of viscoelastic material from the anterior chamber, the corneal incision was closed by 10–0 sutures using monophilic material. We are convinced that these safety sutures support the more rapid regeneration of the anterior chamber following the performance of a surgical procedure. We are also convinced that TA administered by injection following the removal of viscoelastic material may be retained in the anterior chamber only upon closure of the chamber by suture. In patients in whom we did not close the chamber in this manner, we observed a leakage of TA from the anterior chamber (surgeon’s observation).
Steroids are often applied locally or by subconjunctival injection, for the purpose of suppressing ocular pathology and postoperative inflammation. With regard to the fact that it suppresses inflammation and reduces vascular permeability, TA is regularly used in the case of ocular pathologies and surgical procedures, usually in intravitreal form or in the form of injection into the sub-Tenon space. The use of intracameral TA during the course of paediatric cataract surgery is linked with better control of inflammation in the region of the anterior segment, and a lower frequency of complications in connection with inflammation. Furthermore, it has been demonstrated that TA does not cause any postoperative changes of IOP or fundamental complications if it is used in the manner stated above [15].
Although suppression of postoperative inflammation with the use of steroids is not a new concept, we still have limited knowledge with regard to its use in surgical procedures on patients with glaucoma. The use of TA in surgical procedures on patients with glaucoma was first published in 1986 in a study by Giangiacomo et al. [16]. In this study the authors referred to surgical success with the use of a subconjunctival injection of 4 mg TA in the period of 0–7 days before the procedure in 14 out of 15 eyes which were considered high risk with regard to the formation of an episcleral scar. In 2006 Tham et al. used injection application of 0.03 TA (40 mg/ml) directly into the filtration cushion of 6 eyes which had undergone trabeculectomy [17]. They referred to the results of this pilot study as beneficial, without demonstration of loss of endothelial cells or progression of cataract.
In another study evaluating PT in patients to whom TA had been applied preoperatively into the anterior chamber, results relating to postoperative inflammation and visual acuity were compared in 4 groups: patients who had been administered TA in doses of 0.5 mg, 1 mg and 2 mg, as well as patients who had not received any TA [18]. The authors determined that intracameral injection of TA was highly effective with regard to the control of postoperative inflammation following PT, in which 1 mg of TA recorded the best postoperative result.
In a study from 2016, Alagöz et al. referred to results of trabeculectomy in which MMC was used, and where an intracameral injection of 0.1–0.3 ml of TA was routinely applied in a dose of 4 mg/ml (Kenacort-A) [19]. At a follow-up examination 21 months after the procedure they attained an overall success rate of the surgical procedure with TA at 68.4 % and without TA at 52.4 %. Although the group treated with TA recorded lower IOP values and a lesser requirement for anti-glaucomatous drugs within the framework of all the subsequent follow-ups, this difference was not statistically significant. No difference was determined between the TA group and the control group with regard to postoperative complications.
However, the authors were not able to standardise which TA dose was applied to which patient, and so stated only the range of doses.
The main limitation of our study is that it concerned a retrospective study, and the number of patients was limited. Due to the retrospective nature of the study, we were not able to evaluate the surgical results of different doses of intracameral application of TA. Statistically significant rehabilitation of sight was demonstrated in the case of all applications of PT in the study and the control group after the surgical procedure. However, we cannot clearly interpret the comparison of the groups, because we cannot fully document the degree of preoperative opacification of the lens in all patients. Furthermore, in similar studies the interpretation was hampered by the occurrence of various types of glaucoma. The advantage of our study is that both groups comprised exclusively patients with POAG, which improves the interpretation of the results of 1 mg of TA applied into the anterior chamber.
CONCLUSION
According to our experience, the application of an intracameral injection of 1 mg of TA at the end of the surgical procedure of PT did not produce better results with regard to the postoperative level of IOP in comparison with PT alone, and both groups recorded a similar reduction of IOP. Upon application of 1 mg of TA as an adjuvant agent for PT, inflammation in the anterior chamber is suppressed, with a reduction of the need for injection application of 5-FU. For more detailed assessment of the impacts of TA on the postoperative results of PT it is necessary to conduct a prospective study using different doses of TA in larger groups of patients.
Zdroje
1. Cairns, JE.: Trabeculectomy, Preliminary report of a new method. Am J Ophthalmol. 1968 Oct;66(4):673–9.
2. Lochhead, J., Casson, RJ., Salmon, JF.: Long term effect on intraocular pressure of phacotrabeculectomy compared to trabeculectomy. Br J Ophthalmol. 2003 Jul;87(7):850–852.
3. Choy, BNK.: Comparison of surgical outcome of trabeculectomy and phacotrabeculectomy in Chinese glaucoma patients. Int J Ophthalmol. 2017 Dec;10(12):1928–1930.
4. Murthy, SK., Damji, KF., Pan Y., Hodge, WG.: Trabeculectomy and phacotrabeculectomy, with mitomycin-C, show similar two-year target IOP outcomes. Can J Ophthalmol. 2006 Feb;41(1):51–59.
5. Chang, L., Thiagarajan, M., Moseley, M., et al.: Intraocular pressure outcome in primary 5FU phacotrabeculectomies compared with 5FU trabeculectomies. J Glaucoma. 2006 Dec;15(6):475–81.
6. Stalmans, I., Gillis, A., Lafaut, As., Zeyen, T.: Safe trabeculectomy technique: long term outcome. Br J Ophthalmol. 2006 Jan;90(1):44–7.
7. Palanca-Capistrano, AM., Hall, J., Cantor, LB., Morgan, L., Hoop, J., Wudunn, D.: Long-term outcomes of intraoperative 5-fluorouracil versus intraoperative mitomycin C in primary trabeculectomy surgery. Ophthalmology. 2009 Feb;116(2):185–90.
8. Reibaldi, A., Uva, MG., Longo, A.: Nine-year follow - up of trabeculectomy with or without low dosage mitomycin-c in primary open angle glaucoma. Br J Ophthalmol. 2008 Sep;92(12):1666–70.
9. Ehrnrooth, P., Lehto, I., Puska, P., Laatikainen, L.: Long-term outcome of trabeculectomy in terms of intraocular pressure. Acta Ophthalmol Scand. 2002 Jun;80(3):267–71.
10. The AGIS Investigators − The Advanced Glaucoma Intervention Study (AGIS): 7. The relationship between control of intraocular pressure and visual field deterioration. Am J Ophthalmol. 2000 Oct;130(4):429–40.
11. Jin, GJ., Crandall, AS., Jones, JJ.: Phacotrabeculectomy: assessment of outcomes and surgical improvements. J Cataract Refract Surg. 2007 Jul;33(7):1201–8.
12. Rao, HL., Maheshwari, R., Senthil, S., Prasad, KK., Garudadri, CS.: Phacotrabeculectomy without mitomycin C in primary angle-closure and open angle glaucoma. J Glaucoma. 2011 Jan;20(1):57–62.
13. Cotran, PR., Roh, S., McGwin, G.: Randomized comparison of 1-Site and 2-Site phacotrabeculectomy with 3-year follow-up. Ophthalmology. 2008 Mar;115(3):447–454.
14. Gdih, GA., Yuen, D., Yan, P., Sheng, L., Jin, YP., Buys, YM.: Meta-analysis of 1 - versus 2-Site Phacotrabeculectomy. Ophthalmology. 2011 Jan;118(1):71–6.
15. Allam, G., Ellakkany, R., Ellayeh, A., Mohsen, T., Abouelkheir, HE., Gaafar, W.: Outcome of pediatric cataract surgery with intraocular injection of triamcinolone acetonide: Randomized controlled trial. Eur J Ophthalmol. 2018 Nov;28(6):633–638.
16. Giangiacomo J., Dueker DK., Adelstein E.: The effect of preoperative subconjunctival triamcinolone administration on glaucoma filtration. I.Trabeculectomy following subconjunctival triamcinolone. Arch Ophthalmol. 1986 Jun;104(6):838–841.
17. Tham CC., Li FC., Leung DY.: et al. Intrableb triamcinolone acetonide injection after bleb-forming filtration surgery (trabeculectomy, phacotrabeculectomy, and trabeculectomy revision by needling): a pilot study. Eye (Lond). 2006 Dec;20(12):1484–1486.
18. Wang B., Dong N., Xu B., Liu J., Xiao L.: Efficacy and safety of intracameral triamcinolone acetonide to control postoperative inflammation after phacotrabeculectomy. J Cataract Refract Surg. 2013 Nov;39(11):1691–7.
19. Alagöz N., Alagöz C., Yıldırım Y., et al.: The Effect of Adjuvant Intracamaral Triamcinolone Acetonid on Surgical Results of Trabeculectomy with Mitomycin C. Turk J Ophthalmol. 2016 Aug;46(4):169–174.
Štítky
OftalmologieČlánek vyšel v časopise
Česká a slovenská oftalmologie

2020 Číslo 2
- Patofyziologie glaukomu
- Co by váš pacient měl vědět o výběru kontaktních čoček?
- Selektivní laserová trabekuloplastika nesnižuje nitroční tlak více než argonová laserová trabekuloplastika
- Progresi glaukomu je třeba hodnotit strukturálními i funkčními parametry
- Ztráta centrálního vidění po filtrujících operacích glaukomu
Nejčtenější v tomto čísle
- Non-arteritic anterior ischaemic optic neuropathy: treatment and risk factors
- Vzpomínka na doc. MUDr. Cigánka, CSc.
- Betaxolol, Brimonidin and Carteolol in the Therapy of Normal-Tension Glaucoma
- Aflibercept for Vascularised Serous Pigment Epithelial Detachment: One-Year Anatomical and Functional Results
Zvyšte si kvalifikaci online z pohodlí domova
Mazová zátka a její řešení
nový kurzVšechny kurzy