
Primary orbital teratoma – case study
Authors:
M. Komínek 1; R. Autrata 1; I. Krejčířová 1; K. Šenková 1; B. Žajdlíková 1; K. Pernicová 1; A. Masariková 1; Marta Ježová 2
Authors place of work:
Dětská oční klinika, LF MU a FN Brno, Černopolní 9, 61300 Brno, přednosta: prof. MUDr. Rudolf Autrata, CSc., MBA.
1; Ústav patologie, LF MU a FN Brno, Jihlavská 20, 625 00 Brno, přednosta: doc. MUDr. Leoš Křen, Ph. D.
2
Published in the journal:
Čes. a slov. Oftal., 75, 2019, No. 1, p. 40-44
Category:
Kazuistika
doi:
https://doi.org/10.31348/2019/1/5
Summary
Teratomas are tumours deriving from embryonal stem cells. They consist of elements of all three germinal layers. Orbital localization of this type of tumour is very rare. Symptoms develop in the first months of life, rarely later, as cystoid components of the tumour grow in size. Surgical treatment is extremely difficult, eye is spared in individual cases. In our case study, we present baby girl with a diagnosis of primary intraorbital teratoma, who underwent partial resection of the tumour with not just the eye globe spared, but also with visual functions present after the surgery.
Keywords:
teratoma – orbit – proptosis – orbital surgery
INTRODUCTION
Teratomas are tumours originating from pluripotent embryonic stem cells, and are composed of elements derived from all three germinal layers [2, 4, 15, 19, 22, 23]. Localisation of this type of tumour in the orbit is very rare, and as a result there is little clinical experience [3, 12, 19, 22]. The incidence of primary orbital teratoma in girls is twice as high as in boys [2, 3, 14, 15]. A typical symptom is unilateral, usually massive proptosis of the eyeball [2, 12, 14-17, 21, 23]. Orbital teratomas are most frequently located intraconally, in close contact with the optic nerve and extraocular muscles [12, 23]. Orbital teratomas are usually well differentiated tumours of benign nature. However, they may cause facial deformities as a consequence of rapid growth, destructive exophthalmos or exposure keratopathy [12]. Teratomas do not have a specific finding upon examination by imaging methods. They contain various cystic elements, epithelia of various types, fat tissue, skin adnexa, cartilage, sometimes also fragments of bones and teeth [3, 12, 22, 23]. Computer tomography (CT) and magnetic resonance imaging (MRI) are of use in clarifying the scope of the tumour, can accentuate components with various density and provide valuable information about any potential spread beyond the orbit [3, 12]. In therapy the method of choice is early excision of the tumour, if possible sparing the eyeball [2, 12, 14, 19, 22]. Complete removal of the tumour is very demanding due to its close linkage to the optic nerve and extraocular muscles.
CASE REPORT
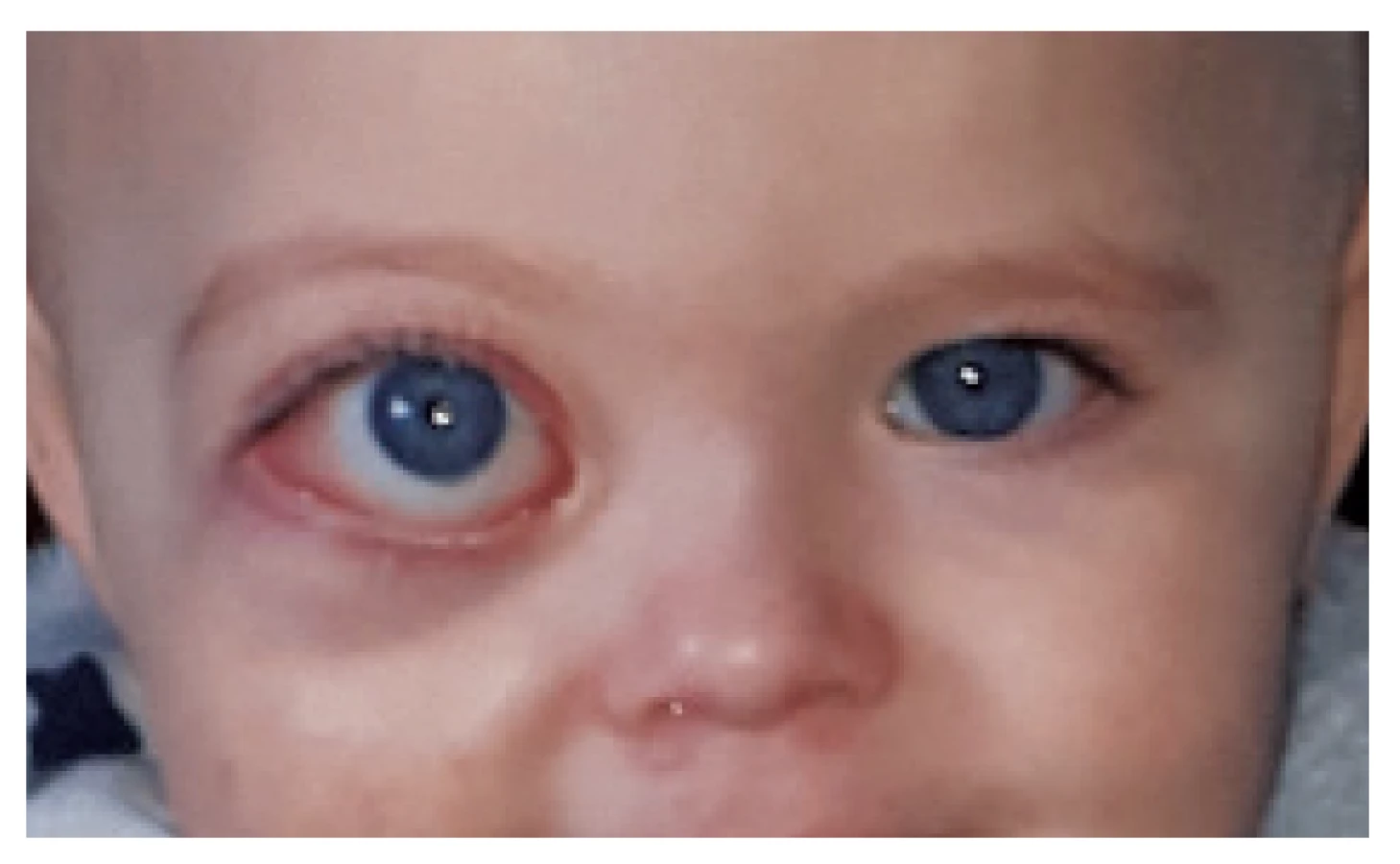
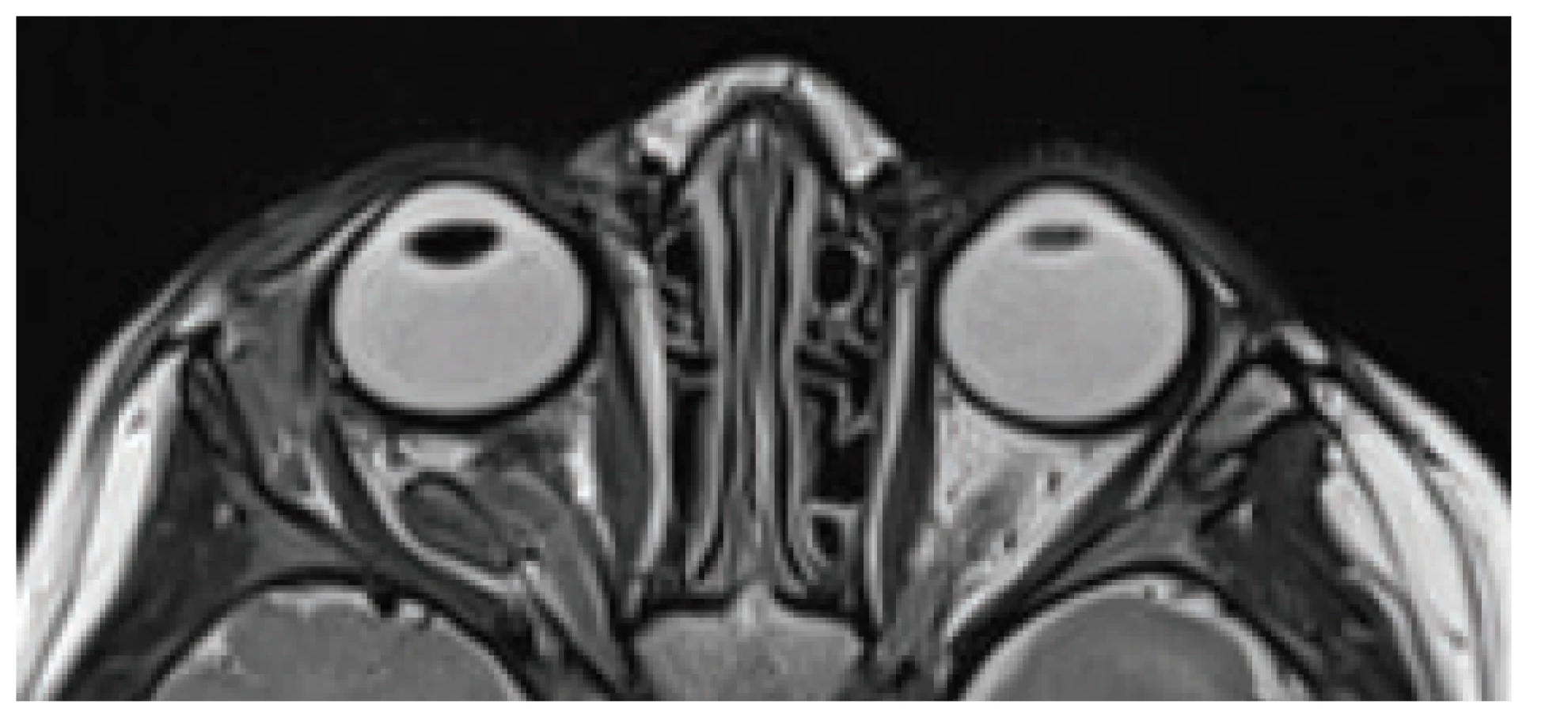
The case report relates to a girl born from a physiological pregnancy, without prenatal or perinatal risks, in whom the parents noticed a “manifestly larger” right eye at the age of four months. Proptosis of the right eyeball was objectively evident, with rapid progression (fig. 1). At the age of five months an MRI examination of the orbit was performed at the district centre, with a finding of pronounced proptosis of the eyeball with stretching of the optic nerve and enlargement of the right orbit with a content of matter of various density. At this point lymphangioma and lymphangioma hemangioma were considered in differential diagnostics. With regard to the localisation and close contact with the optic nerve, enucleation of the right eyeball with radical resection of the tumour was proposed. Within the framework of second-opinion the patient was taken to the Paediatric University Hospital Brno, where CT of the orbits, including CT angiography, was performed at the age of nine months. In local eye therapy, the girl's parents applied brinzolamide and lubricants to her right eye due to the risk of elevation of intraocular pressure as a result of compression of the eyeball by the tumour masses, and incipient lagophthalmos resulting from massive proptosis and chemosis of the conjunctiva. With regard to the result of CT of the orbits, the character of saturation and the course of the tubular structures in the tumour, the originally considered diagnoses were abandoned. The structure of the tumour was described as markedly heterogeneous, with numerous tubular and cystoid formations with isolated calcifications and pronounced multiplication of fat tissue. The expansive character of the tumour masses was also spatially clarified by means of 3D reconstruction (fig. 2). In differential diagnostics we considered intraorbital teratoma or dermoid cyst. At the age of ten months, a biopsy of the tumour masses was conducted, as well as a supplementary MRI examination of the orbits (fig. 3). Macroscopically, the sampled tissue had the appearance of multiple pink particles of elastic consistency, with occasional slits, with a content of viscous yellow matter. Microscopically there was a dominance of fat tissue, also cystic formations covered by the squamous epithelium, skin adnexa – sebaceous glands and hair follicles. All the tissues were merely mature, of highly organised arrangement. Due to constantly growing proptosis, the girl was at risk of loss of visual functions. Partial resection of the tumorous matter was indicated, with an endeavour to preserve the right eyeball including visual functions. At the age of fourteen months the girl underwent partial surgical resection of the tumour in the right orbit under general anaesthesia. Course of operation: following peritomy of conjunctiva in the lower temporal quadrant and fixation of the inferior oblique muscle, the tumour masses in this region were partially removed. There followed fixation of the lateral rectus muscle and resection of a number of cystic formations, the largest of which reached the dimensions of approximately 4 cm in diameter, others had a dermoid appearance or contained whitish mucoid matter. Cartilage was found perioperatively in one of the cystic formations. Following resection of the cystic formations, there was evident impression of the bone of the edge of the orbit on its lower edge. In the place of the resected cysts there were evident cavities. The operation was completed by suturing of the conjunctiva. At the end of the operation the right eyeball was without proptosis, in symmetrical position with the left eyeball (fig. 4).



The extirpated tumorous masses and cystic formations were sent for a histological examination. In the histological examination, a mixed tumour was described in the first sample of the biopsy, in which mature fat tissue predominated. The second most frequently occurring component macroscopically was narrow slits filled with wax, histologically covered by a keratinising squamous epithelium of skin including skin adnexas. A solid-cystic tumour of variegated appearance was determined in the second sample. It was formed by various mature tissues which could be derived from all three germinal layers (“tridermoma”): squamous skin epithelium with adnexa (derivates of ectoderm), intestinal and stomach epithelium (derivates of endoderm), muscle tissue, fat tissue, cartilage and bone (derivates of mesoderm). They were arranged in a highly organoid manner, and so were reminiscent of the structure of normal organs, e.g. the wall of the stomach. None of the biopsy samples contained immature or malignant tissues. On the basis of the histological examination, a definitive diagnosis of mature primary orbital teratoma was determined (fig. 5).

In the postoperative period there was a progressive resorption of the postoperative swelling, haematoma of the eyelids and chemosis of the conjunctiva. Six weeks after the operation an examination of preferential vision was conducted with the following result: Concentration of attention 1; Eye contact 1; Cardiff test: Vision to 1 m binocularly 1.0; the girl responds binocularly and monocularly reliably even to the thinnest lines. At the same time a follow-up MRI examination of the orbits was performed, which confirmed a significant regression of the proptosis with regression of the tumorous content of the orbit, with residue in the cone of the orbit in close contact with the now sigmoid-coiled optic nerve, infrabulbar residue and in the surrounding area of the lateral rectus muscle (fig. 6). The condition in long-term, 6-month observation is stationary. The cosmetic effect is very favourable with only slight facial asymmetry, on the right there is very discrete enopthalmos visible and persistent medium-wide pupil with slightly delayed photo-reaction. Motility of the right eyeball is without restriction, the cornea is smooth, glossy and transparent (fig. 7).

DISCUSSION
Teratomas are congenital tumours from germinal cells, which contain components of three germinal layers. They are classified as “mature” or “immature” according to the degree of cell differentiation [5, 17, 21, 24]. Teratomas in childhood primarily appear in extragonadal location. The most common are teratomas of the sacrococcygeal region, head and neck [2, 3, 8]. Extragonadal teratomas originate from pluripotent primordial germinal cells. A number of theories exist concerning the pathogenesis of these extragonadal tumours. One theory presumes an abnormal migration of germinal cells into the region “close to the median line” (head, mediastinum, sacrococcygeal region), with their subsequent further proliferation. Another hypothesis indicates their origin rather from basic somatic cells with full genetic coding, in which these somatic cells could theoretically produce other types of cells without them being germinal cells [2, 3, 12].
Orbital teratomas, unlike very frequent dermoid cysts, appear very rarely [3, 17]. A teratoma may grow secondarily into the orbital space from the paranasal cavities, cavernous sinus or pterygopalatine fossa. Teratomas may spread via the periorbital sinus or via the upper orbital fissure, and the condition may be further complicated by intracranial spread of the tumour [2, 3].
Histopathologically, orbital teratomas are usually well differentiated tumours of a benign nature. In 90% of cases, teratomas contain all 3 embryonic layers [2, 3]. This also applied to our patient. Alkatan states that 20% to 40% of paediatric teratomas may contain also a small amount of immature (undifferentiated) tissue [3]. A small admixture of undifferentiated cells in a small child does not worsen the prognosis [2, 3]. Malignant, thus predominantly undifferentiated teratomas occur rather in older children, and their incidence is low [2, 3]. Multiloculation, formation of cysts, calcification, ossification and admixture of fat tissue are indicators of benign teratoma [2, 3]. A malignant reversal over the course of time is manifested only in a very small percentage of benign teratomas [2, 3].
Clinically, orbital teratomas are usually manifested very soon after birth [7, 17]. Proptosis of the eyeball is often evident already in the first weeks of life, and progresses as a consequence of an accumulation of fluid or epithelial cells in blind cystic formations [1, 2, 4, 12, 14, 15, 22, 23]. Despite the fact that this mostly concerns tumours of a benign nature, they may cause facial deformities as a result of rapid growth, destructive exophthalmos or exposure keratopathy, corneal ulcers and in extreme cases perforations [3, 4, 12, 14, 15, 19, 22, 23]. In the preoperative period, it is appropriate to apply local anti-glaucomatous agents and lubricants in order to prevent complications, as was the case of our patient. With regard to the fact that teratomas may contain variously differentiated tissues in various ratios, they do not have a specific finding upon examination by imaging methods. They may contain various cystic components, epithelia of diverse types, fat, skin and skin adnexa, cartilage, and sometimes also fragments of bones and teeth [3, 12, 22, 23]. Kostolná states that upon a finding of a tooth in the tumorous mass it is necessary to differentiate the teratoma from an odontogenic dermoid cyst similar to teratoma, which however as a rule does not contain all three germinal layers [17]. Upon ultrasonic examination, teratomas manifest fluctuating echogeneity, there are evident potential deposits of calcifications or bone fragments which can be identified by a simple X-ray image [1, 12]. CT and MRI are highly beneficial and clarify the scope of the tumour, accentuate the components of various density and provide valuable information about any applicable extraorbital spreading [3, 12].
In therapy, early surgical excision is recommended, if possible with preservation of the eyeball [2, 12, 14, 19, 22]. With regard to the close linkage to the optic nerve and extraocular muscles, complete removal of the tumour is highly demanding. Resection of the tumour eases perioperative aspiration of fluid from the cystic formations [12]. In some cases, a radical surgical solution is indicated in the form of enucleation of the eyeball or exenteration of the orbit, with subsequent application of epithesis. A radical surgical solution is applied more frequently in the case of malignities of the orbit [6, 9-11, 13, 16, 18, 21, 24]. Upon affliction of the intracranial cavities, combined craniotomy with orbitotomy is required for the removal of the tumour [7, 12].
The scope of the orbital teratoma and the size of the proptosis often excludes the possibility of preservation of the eyeball. Alkatan and Baydia document total resection of a congenital orbital teratoma with the necessity of enucleation of the eyeball [3, 4]. However, in rare cases it is possible to preserve the visual functions in the affected eye. Chang and Mee document excision of an orbital teratoma with the preservation of visual functions [8, 20]. In our patient we succeeded in performing a partial sight-preserving resection of the orbital teratoma, in which the examination of preferential vision in the postoperative period documents preservation of visual functions. The long-term prognosis depends upon a histological differentiation of teratoma tissues and the scope of the tumour [2, 12]. The tumour residue may in isolated cases lead to later recurrence and in rare cases even to malignant reversal [2, 4, 12, 22, 23]. The scope of the tumour in our patient did not enable the performance of total resection of the teratoma with preservation of the eyeball. With regard to the very favourable histological differentiation, later recurrence and malignant reversal of the small orbital residue of the teratoma in our patient is improbable. The benefit of partial sight-preserving resection of the orbital teratoma in our patient consists in the excellent postoperative cosmetic appearance and preservation of visual functions.
CONCLUSION
Professional ophthalmologists should have an awareness of the possible incidence of rare orbital tumours in childhood age, in which heterogeneous histological characteristics are typical. In pathological and radiological diagnostics, orbital teratoma is attested to by a complex of pathological tissue including fat areas and calcifications. Timely and accurate diagnosis enables early surgical resection of the orbital teratoma with a satisfactory cosmetic result, consisting in preservation of the eyeball and visual functions.
The case report was presented as a lecture at the professional event VI. Trendy v dětské oftalmologii a strabologii [VI. Trends in Pediatric Ophthalmology and Strabismus], 26 – 27 October 2018, Litomyšl.
The authors of the study declare that no conflict of interest exists in the compilation, theme and subsequent publication of this professional communication, and that it is not supported by any pharmaceuticals company.
Received by the Editorial Department on: 26 November 2018
Accepted for printing on: 21 January 2019
MUDr. Martin Komínek
Children's Ophthalmology Clinic,
Faculty of Medicine,
Masaryk University and University Hospital Brno,
Černopolní 9,
613 00, Brno.
Zdroje
1. Aiyub, S., Chan, W., Szetu, J. et al.: Congenital orbital teratoma. Indian J Ophthalmol, 61; 2013 : 767-769.
2. Alkatan, HM., AlObaidan, OS. et al.: Orbital immature teratoma: a rare entity with diagnostic challenges. Saudi J Ophthalmol, 32; 2018 : 75-78.
3. Alkatan, HM., Chaudhry, I., Alayoubi, A.: Mature teratoma presenting as orbital cellulitis in a 5-month-old baby. Ann Saudi Med, 33; 2013 : 623-626.
4. Baidya, K.P., Ghosh, S., Datta, A. et al.: Huge congenital teratoma containing tooth in a three-day-old neonate. Oman J Ophthalmol, 7; 2014 : 13-15.
5. Bajčiová, V., Štěrba, J., Tomášek, J. et al.: Nádory adolescentů a mladých dospělých. Praha, Grada, 2011, 400 s.
6. Baráková, D. et al.: Nádory oka. Praha, Grada, 2002, 152 s.
7. Berlin, A., Rich, LS., Hahn, JF.: Congenital orbital teratoma. Pediatr Neurosurg, 10; 1983 : 208-216.
8. Chang, DF., Dallow, RL., Watton, DS.: Congenital orbital teratoma: report of case with visual preservation. J Pediatr Ophthalmol Strabismus, 17; 1980 : 88-95.
9. Furdová, A., Ferková, A. et al.: Exenterácia očnice pre malígny melanóm choroidey v štádiu t4; možnosti epitetického riešenia. Cesk Slov Oftalmol, 71; 2015 : 150-157.
10. Furdová, A., Horkovičová, K. et al.: Exenterácia očnice pre bazocelulárny karcinóm. Cesk Slov Oftalmol, 71; 2015 : 209-216.
11. González, C., Restrepo, C. et al.: Congenital orbital teratoma. Case report. Colombia MéDica, 43; 2012 : 82-85.
12. Hoyt, CS., Taylor, D. et al.: Pediatric ophthalmology and strabismus 4th ed, Oxford, Elsevier, 2012, 1168 p.
13. Justusová, P., Štubňa, M. et al.: Exenterácia orbity u pacienta s generalizovaným choroidálnym melanómom. Cesk Slov Oftalmol, 72; 2016 : 92-96.
14. Kharosekar, HU., Jasmit, S., Velho, V. et al.: Congenital orbital teratoma up to posterior fossa. J Pediatr Neurosci, 9; 2014 : 182-184.
15. Kivelä, T., Tarkkanen, A.: Orbital germ cell tumors revisited: a clinicopathological approach to classification. Surv Ophthalmol, 38; 1994 : 541-554.
16. Klener, P. et al.: Klinická onkologie. Praha, Galén, 686 s.
17. Kostolná, B., Gerinec, A. et al.: Odontogénna dermoidná cysta orbity. Cesk Slov Oftalmol, 67; 2011 : 101-103.
18. Krásný, J., Novák, V., Otradovec, J.: Orbitální protéza po exenteraci očnice se zachováním víček a spojivkového vaku. Cesk Slov Oftalmol, 62; 2006 : 94-99.
19. Levin, ML., Leone, CR. Jr., Kincaid, MC.: Congenital orbital teratomas. Am J Ophthalmol, 102; 1986 : 476-481.
20. Mee, JJ., McKelvie, PA., McNab, AA. : Orbital teratoma: late presentation with normal vision. Clin Exp Ophtalmol, 30; 2002 : 41-43.
21. Otradovec, J.: Choroby očnice. Praha, Avicenum, 1986, 312 s.
22. Pellerano, F., Guillermo, E. et al.: Congenital orbital teratoma. Ocul Oncol Pathol, 3; 2017 : 11-16.
23. Prakash, MV., Indira, R., Radhakrishnan, M. et al.: Malignant orbital teratoma in a neonate: a clinicopathological case report. J Postgrad Med, 63; 2017 : 203-205.
24. Šlapák, I., Vlková, E.: Tumory orbity. Brno, Masarykova univerzita, Brno, 1993, 69 s.
Štítky
OftalmologieČlánek vyšel v časopise
Česká a slovenská oftalmologie

2019 Číslo 1
- Selektivní laserová trabekuloplastika nesnižuje nitroční tlak více než argonová laserová trabekuloplastika
- Progresi glaukomu je třeba hodnotit strukturálními i funkčními parametry
- Ztráta centrálního vidění po filtrujících operacích glaukomu
- Od PGF-2 alfa-isopropyl esteru k latanoprostu: přehled vývoje Xalatanu
- Compliance u pacientů s glaukomem
Nejčtenější v tomto čísle
- Late postoperative capsular bag distension syndrome
- Primary orbital teratoma – case study
- Treatment of idiopathic choroidal neovascular membrane with ranibizumab - our experience
- RADIATION MACULOPATHY AFTER ONE-DAY SESSION STEREOTACTIC RADIOSURGERY IN PATIENTS WITH CILIARY BODY AND CHOROIDAL MELANOMA
Zvyšte si kvalifikaci online z pohodlí domova
Mazová zátka a její řešení
nový kurzVšechny kurzy