
Prenatal treatment of posterior urethral valves in a newborn with anorectal stenosis
Authors:
D. A. Miguel 1; E. Araujo Júnior 2,3; R. Ruano 4; R. A. M. De Sá 1,5
Authors‘ workplace:
Department of Obstetrics, Gynecology, and Fetal Medicine, Perinatal Maternity, Rio de Janeiro-RJ, Brazil
1; Department of Obstetrics, Paulista School of Medicine – Federal University of São Paulo (EPM-UNIFESP), São Paulo-SP, Brazil
2; Discipline of Woman Health, Municipal University of São Caetano do Sul (USCS), São Caetano do Sul-SP, Brazil
3; Division of Maternal-Fetal Medicine, Department of Obstetrics, Gynecology & Reproductive Sciences, University of Miami, Miller School of, Medicine, Miami-FL, USA
4; Division of Maternal-Fetal Medicine, Department of Obstetrics, Gynecology & Reproductive Sciences, University of Miami, Miller School of Medicine, Miami-FL, USA
4; Department of Obstetrics and Gynecology, Fluminense Federal University (UFF), Niterói-RJ, Brazil
5
Published in:
Ceska Gynekol 2025; 90(4): 323-327
Category:
Case Report
doi:
https://doi.org/10.48095/cccg2025323
Overview
Posterior urethral valves (PUV) account for most cases of lower urinary tract obstruction (LUTO) in male fetuses, with a prevalence of 1 in 5,000 live births. Prenatal ultrasound findings include bladder wall thickening, keyhole sign, oligohydramnios, and ureteral dilatation. If untreated, PUV can cause pulmonary hypoplasia and renal failure, often requiring dialysis or transplantation. Treatment options include vesicoamniotic shunting and fetoscopic laser fulguration. PUV is rarely associated with anorectal malformations, posing a diagnostic and therapeutic challenge. This case report describes a neonate diagnosed prenatally with PUV who underwent intrauterine procedures, followed by preterm cesarean section at 32 weeks. Postnatally, he exhibited renal dysplasia, cryptorchidism, and developed necrotizing enterocolitis. Despite multiple laparotomies and colostomy, the infant improved and was then discharged. At 4 months, imaging confirmed rectal stenosis. We highlight the diagnostic limitations of prenatal ultrasound in differentiating PUV from other LUTO causes and the benefits of fetal magnetic resonance imaging. Anorectal malformations have diverse phenotypic presentations and are linked to environmental risk factors. The rare association of PUV with anorectal anomalies requires careful prenatal counseling due to potential complications. This case highlights the importance of early diagnosis and multidisciplinary management for improved outcomes.
Keywords:
prenatal diagnosis – associated anomalies – posterior urethral valves – intrauterine treatment – postnatal follow-up
Introduction
Posterior urethral valve (PUV) account for approximately 70–80% of all causes of lower urinary tract obstruction (LUTO) detected in the prenatal and immediate postnatal period in male fetuses, with a reported incidence of 1 in 5,000 live births [1]. The most common antenatal ultrasound findings include dilatation and thickening of the bladder wall, keyhole sign, oligohydramnios and ureteral dilatation [2]. Neonates also have cryptorchidism and bowel malrotation due to a distended bladder that doesn’t allow normal bowel positioning or testicular descent.
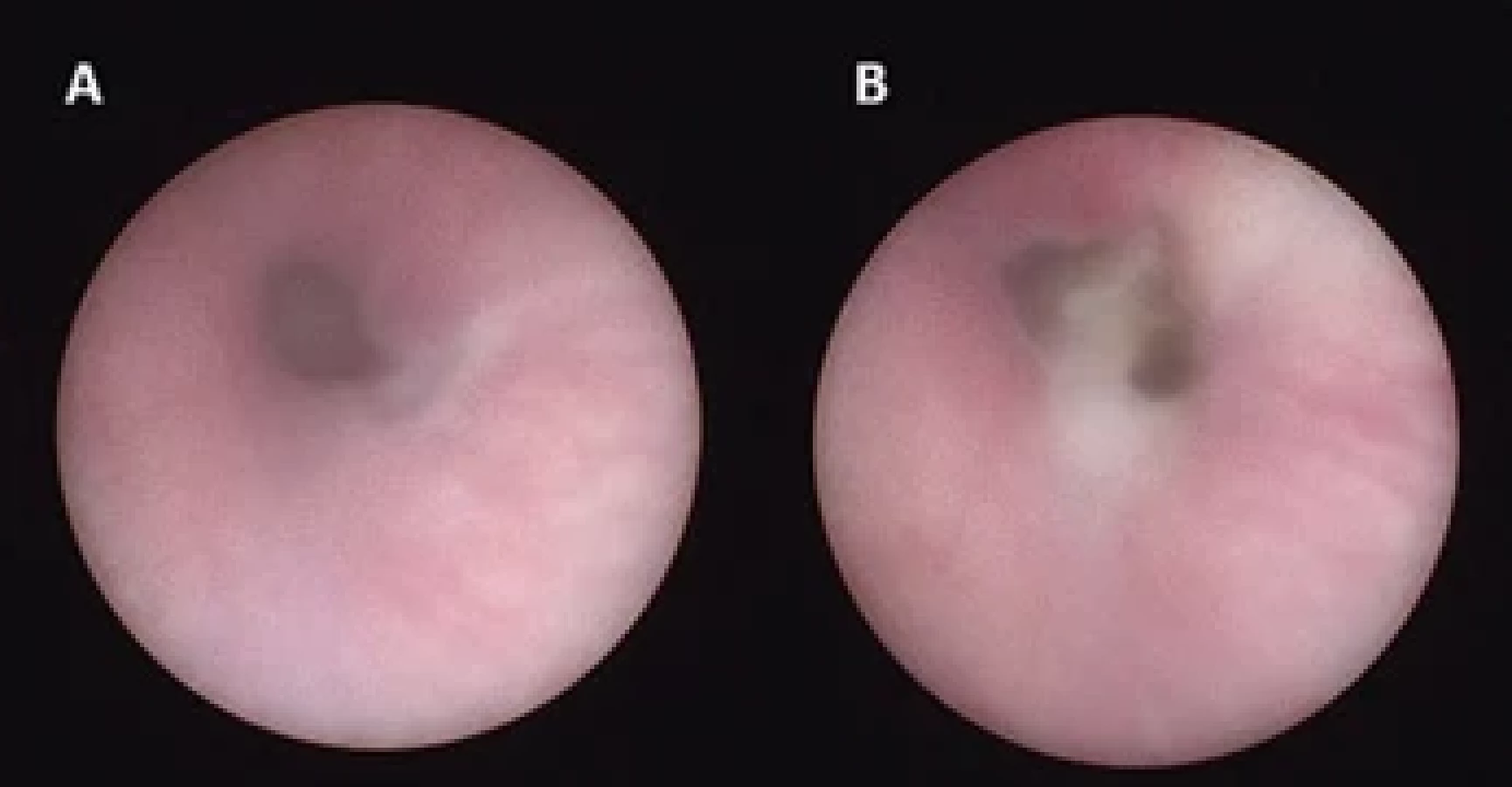
Obr. 1. Endoskopická vizualizace plodového močového měchýře.
A) Otevření močové trubice. B) Laserová fulgurace zadních uretrálních chlopní.

Untreated PUV can lead to fetal consequences due to severe oligohydramnios such as low set ears, flat nose, wrinkles under the eyes, congenital clubfoot and pulmonary hypoplasia. Survival of these neonates depends on the degree of lung hypoplasia, which usually results in severe respiratory failure. Even in survivors, the postnatal course is complicated by progression of renal cortical damage to end-stage renal disease requiring dialysis and/or transplantation [3]. Prenatal treatment options include percutaneous vesicoamniotic shunt, open fetal cystostomy or fetoscopic laser fulguration of the PUV, the latter being comparatively less invasive and with less need for reapproach, thus reducing maternal and/or fetal complications [4].
PUV has been associated with several conditions, including cardiovascular anomalies, absence of external auditory meatus, bilateral adrenal agenesis, hypospadias, micro/macrocephaly and anterior urethral valves [5]. However, the association of PUV with anorectal malformations is extremely rare and may present a diagnostic and therapeutic challenge.
Case report
A male neonate born to a primigravida mother with a history of pregestational diabetes and hypothyroidism was diagnosed with LUTO due to a PUV on second trimester scan. Amniocentesis was performed and a 46,XY karyotype was identified. The fetus underwent two intrauterine procedures: vesicoamniotic shunt and fetoscopy laser fulguration of the PUV due to recurrence of megabladder and bilateral hydronephrosis after the vesicoamniotic shunt (Fig. 1–3). Preterm cesarean section was performed at 32 weeks and 4 days after corticosteroid therapy due to deterioration of the fetal renal ultrasound appearance. The neonate weighed 1,890 g, required ventilatory support in the delivery room after a difficult extraction, with an Apgar score of 5,7, and 8 at the 1st, 5th, and 10th minute, resp.
During neonatal intensive care unit (NICU) admission, abdominal ultrasound revealed renal dysplasia with bilateral dilatation of the renal calyces and pelvis, dilated and tortuous ureters and thickening of the bladder walls, confirming the presence of PUV. In addition to the described findings, bilateral cryptorchidism was also noted. Six days after delivery, a bilateral pyelostomy was performed by the pediatric surgical team as an initial approach. The neonate developed abdominal distension associated with necrotising enterocolitis. A zero diet was introduced and antibiotic therapy was started with vancomycin and tazocin, which was later adjusted and maintained for 14 days following the growth of Serratia marcescens in a urine culture.
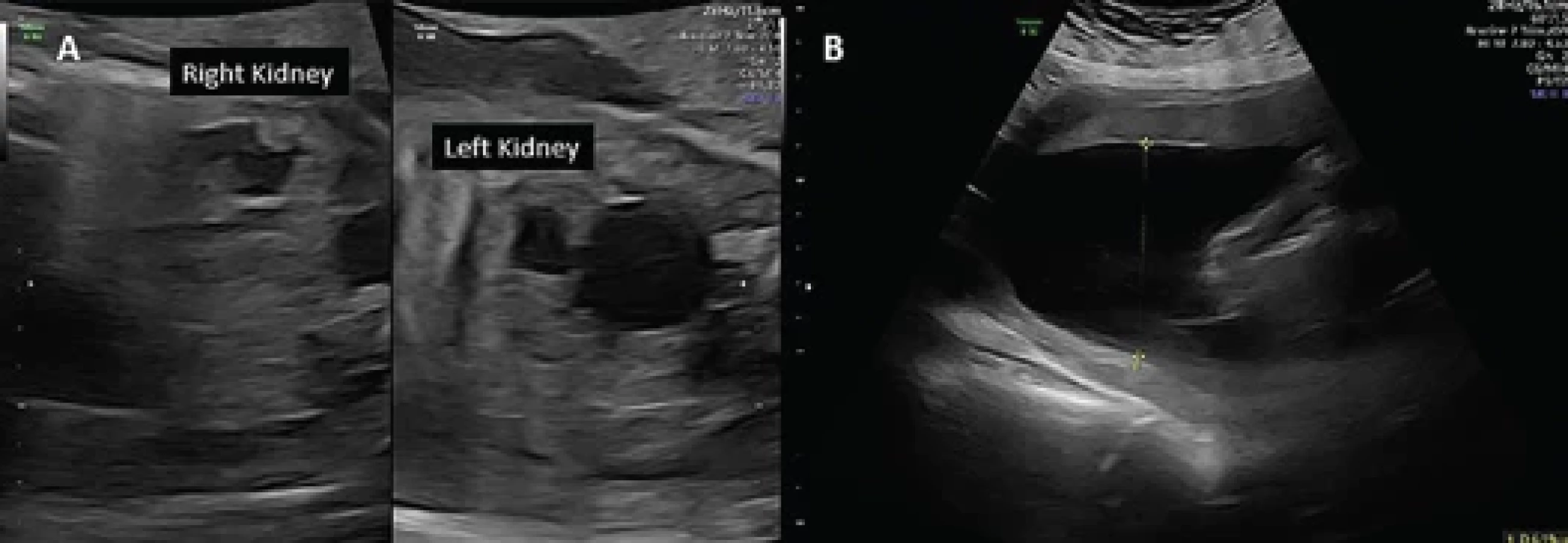
Obr. 3. Ultrazvuk 15 dní po laserové fulguraci zadních uretrálních chlopní.
A) Koronální rovina zobrazující zachovanou kůru obou ledvin. B) Normalizace objemu plodové vody.
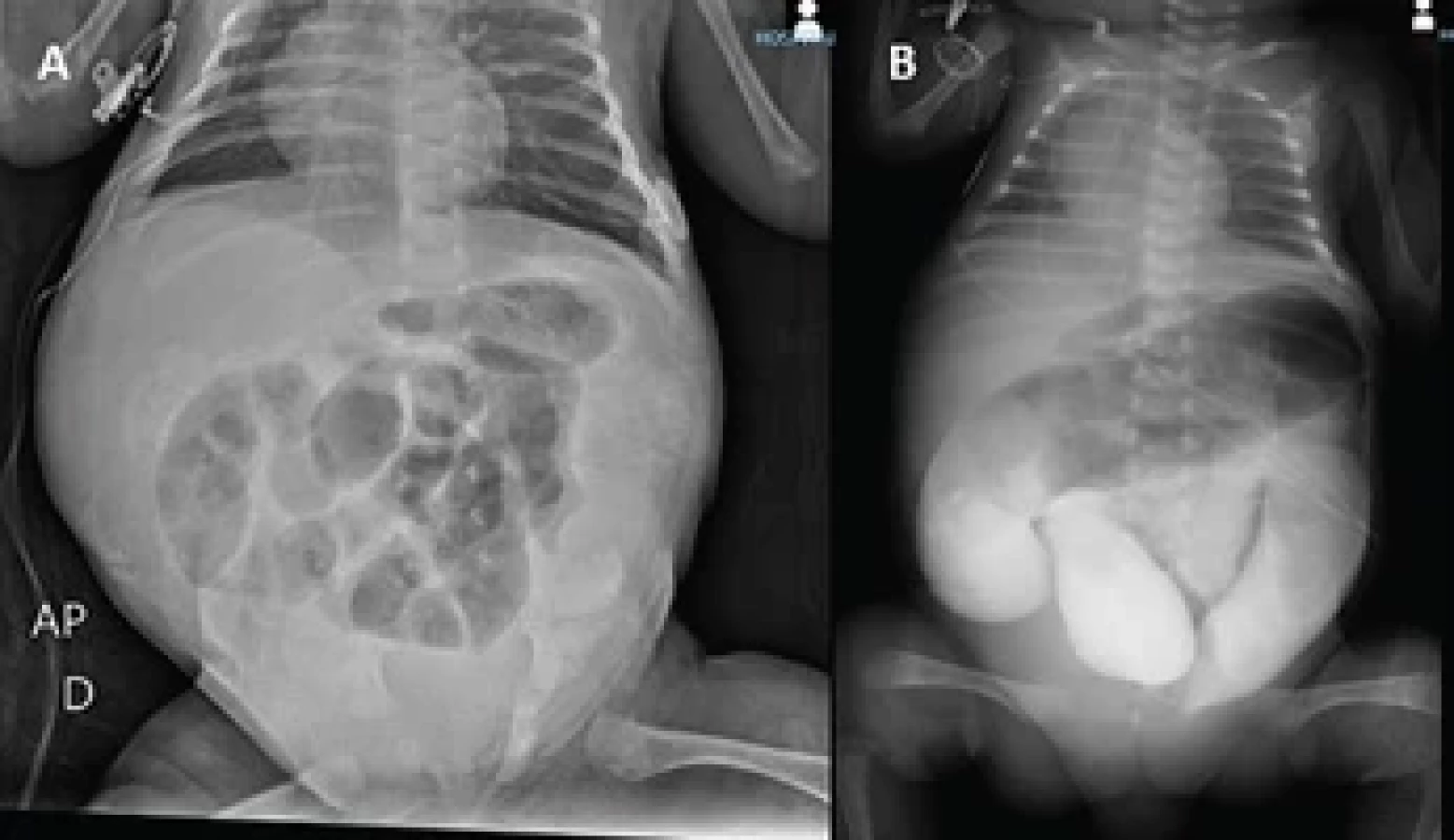
Given the worsening of the condition after the return to diet, the hypothesis of functional bowel obstruction or post-enterocolitis stenosis was raised, and an exploratory laparotomy was performed, during which a stenosis in the proximal third of the rectum was identified and a colostomy was created. Two days later, a new laparotomy was performed for perforation of the left colon with resection of 5.0 cm of the segment. Fifty days later, the neonate required a third exploratory laparotomy, which revealed diffuse necrotising enterocolitis and perforation of the proximal jejunum and terminal ileum, resulting in resection of 10 cm of each segment and enteroanastomosis, maintaining the colostomy. After a satisfactory course, the newborn was discharged from the NICU with progressive clinical improvement (Fig. 4).
An opaque enema performed at 4 months of age and showed a progressive reduction in the caliber of the proximal third of the rectum, with a funicular aspect, extending to approximately 16 mm and measuring approximately 3 mm at its narrowest point, approximately 26 mm from the anal margin, configuring a rectal stenosis.
Discussion
PUV present with some characteristic antenatal ultrasound findings including bladder wall dilatation and thickening, keyhole sign, oligohydramnios and ureteral dilatation. Despite this, the sensitivity of prenatal ultrasound diagnosis of PUV has been reported to be 94%, but the specificity is only 43%. The low specificity of prenatal ultrasound diagnosis reflects its poor ability to differentiate PUV from other causes of fetal LUTO, including urethral atresia and prune belly syndrome. Maternal obesity, unfavorable fetal position, and oligohydramnios further limit the ability of prenatal ultrasound to delineate fetal urinary tract anomalies [6].
Compared to prenatal ultrasound, fetal magnetic resonance imaging (MRI) provides superior anatomic detail and better assessment of ureteral and posterior urethral dilatation without significant interference from amniotic fluid volume or fetal position, and can more reliably differentiate PUV from other etiologies of hydronephrosis. Like prenatal ultrasound, fetal MRI is not without limitations [7]. Some centers recommend that fetal MRI be performed between 28 and 32 weeks of gestation to improve image quality. By this time, irreversible fetal renal damage may have occurred, limiting the benefit of prenatal intervention.
Anorectal malformations are a complex group of congenital anomalies resulting from abnormal development of the posterior intestine, allantois, and Muller’s duct resulting in complete or partial anorectal septal malformations. There is a wide variety of phenotypic expression and more than 75% of children have other associated malformations. The spectrum of lesions ranges from relatively small lesions – such as anal stenosis – to some of the more complicated urogenital lesions, such as anal agenesis, rectal agenesis and rectal atresia, as well as complex anomalies, the degree of which is determined by the relationship with the pelvic floor [8,9]. Although information is rather scarce, there is some evidence that prenatal maternal exposure to nicotine, alcohol, caffeine, illicit drugs, occupational hazards, overweight/obesity and diabetes mellitus are possible environmental risk factors.
The association of PUV with anorectal malformations is extremely rare and presents a diagnostic challenge both prenatally and postnatally. Banever et al. [10] described a neonate delivered at 37 weeks of gestation by cesarean section because of sudden onset of oligohydramnios. Physical examination revealed a distended abdomen and an imperforate anus. Postnatal ultrasound did not reveal hydroureteronephrosis. The presence of PUV was only diagnosed postoperatively due to oliguria caused by urine drainage into a large rectourethral fistula, which led to vesicourethrocystography and confirmation of the diagnosis. Shiraishi et al. [11] described the case of a 14-year-old boy who had an imperforate anus repaired at birth and subsequently presented with recurrent orchiepididymitis. Vesicourethrocystography revealed the posterior urethral valve, which was ablated endoscopically, and the teenager had a favorable outcome.
McGrath et al. [5] described the case of a premature male neonate (35 weeks of gestation) with PUV, bilateral renal dysplasia, and imperforate anus who was treated with a Blocksom vesicostomy and left upper quadrant loop colostomy to avoid contamination of the bladder stoma. Mohamed et al. [2] described the case of a premature neonate (34+6 weeks of gestation) who underwent emergency cesarean section for oligohydramnios and dilated bowel loops and was postnatally diagnosed with imperforate anus, PUV with urinary reflux through a coexisting rectourethral fistula and pyloric stenosis. In the presented case, we performed an early preterm delivery due to prenatal ultrasound findings suggesting deterioration of fetal renal function. However, despite good pulmonary and renal development, the neonate developed intestinal obstruction with rectal stenosis after pyelostomy.
Conclusion
We presented a case report of prenatal diagnosis of PUV with associated finding of anorectal stenosis in the postnatal period. This case highlights the importance of parental counseling in cases of prenatal diagnosis of PUV, because of the adverse perinatal outcomes.
Sources
1. Robyr R, Benachi A, Daikha-Dahmane F et al. Correlation between ultrasound and anatomical findings in fetuses with lower urinary tract obstruction in the first half of pregnancy. Ultrasound Obstet Gynecol 2005; 25 (5): 478–482. doi: 10.1002/uog.1878.
2. Richter J, Shinar S, Erdman L et al. Use of prenatal ultrasound findings to predict postnatal outcome in fetuses with lower urinary tract obstruction. Ultrasound Obstet Gynecol 2024; 64 (6): 768–775. doi: 10.1002/uog. 29129.
3. Mohamed AO, Eradi B, Owen A et al. Rare associations with posterior urethral valves. Case Rep Urol 2021; 2021 : 6647692. doi: 10.1155/ 2021/6647692.
4. Ruano R, Duarte S, Bunduki V et al. Fetal cystoscopy for severe lower urinary tract obstruction – initial experience of a single center. Prenat Diagn 2010; 30 (1): 30–39. doi: 10.1002/pd. 2418.
5. McGrath M, Alnaqi AA, Braga LH. Vesicostomy and colostomy in a premature neonate with posterior urethral valves, bilateral dysplastic kidneys, and high imperforate anus: the challenge of stoma placement. Urology 2016; 93 : 191–193. doi: 10.1016/j.urology.2016. 02.031.
6. Rodriguez MM. Congenital Anomalies of the Kidney and the Urinary Tract (CAKUT). Fetal Pediatr Pathol 2014; 33 (5–6): 293–320. doi: 10.3109/15513815.2014.959678.
7. Faure A, Panait N, Panuel M et al. Predicting postnatal renal function of prenatally detected posterior urethral valves using fetal diffusion-weighted magnetic resonance imaging with apparent diffusion coefficient determination. Prenat Diagn 2017; 37 (7): 666–672. doi: 10.1002/pd.5063.
8. Moore SW. Associations of anorectal malformations and related syndromes. Pediatr Surg Int 2013; 29 (7): 665–676. doi: 10.1007/s00383 - 013-3306-8.
9. Hakalmaz AE, Topuzlu Tekant G. Anorectal malformations and late-term problems. Turk Arch Pediatr 2023; 58 (6): 572–579. doi: 10.5152/TurkArchPediatr.2023.23090.
10. Banever GT, Moriarty KP. Posterior urethral valves in a newborn with imperforate anus: clinical presentation and management. J Pediatr Surg 2005; 40 (8): 1332–1334. doi: 10.1016/j.jpedsurg.2005.05.035.
11. Shiraishi K, Takihara H. Recurrent epididymo-orchitis caused by posterior urethral valve associated with imperforate anus. Int J Urol 2004; 11 (1): 58–60. doi: 10.1111/j.1442-2042. 2004.00734.x.
Labels
Paediatric gynaecology Gynaecology and obstetrics Reproduction medicineArticle was published in
Czech Gynaecology
2025 Issue 4
Most read in this issue
- HIV infection and adverse perinatal outcomes – a meta-analysis of premature births, low birth weights, and small for gestational age newborns
- Role of tru-cut bio psy in the management of myometrial lesions
- Early detection of recurrent ovarian cancer, current use of oncomarkers, imaging methods, and future perspectives
- Robotic-assisted cesarean scar defect repair