
Hematological parameters and colposcopic lesion area in precursor lesions of cervical cancer
Authors:
P. T. S. Mantoani 1,2; G. A. Melo 1; J. H. Vieira 3; T. Corrêa Magalhães 1; M. P. O. Franco 1; A. C. Mac Do Barcelos 1; M. A. Michelin 3; E. F. Candido Murta 1; R. Simões Nomelini 1,2
Authors‘ workplace:
Laboratory of Applied Sciences for Women (LaCam)/ Department of Gynecology and Obstetrics, Federal University of Triângulo Mineiro, Av. Getúlio Guaritá, s/ n, Bairro Abadia, Uberaba-MG, Brazil
1; Graduate Program in Gynecology and Obstetrics of the Ribeirão Preto Medical School of the University of São Paulo (FMRP-USP), Ribeirão Preto-SP, Brazil
2; Research Institute of Oncology (IPON), Discipline of Immunology, Federal University of Triângulo Mineiro R. Vigário Carlos, Uberaba-MG, Brazil
3
Published in:
Ceska Gynekol 2025; 90(4): 309-314
Category:
Original Article
doi:
https://doi.org/10.48095/cccg2025309
Overview
Objectives: To evaluate whether there is an association between the colposcopic lesion area and hematological parameters in patients with cervical intraepithelial neoplasia (CIN) 2/3. Material and methods: Women with CIN 2/3 were included in the study (N = 62). Colposcopic lesion area was measured by Image J software. Genotyping for human papillomavirus (HPV) 16, 18, 45 and 52 was performed by PCR. Hematologic parameters were evaluated. Results: The cut-off value of monocytes was ≤ 490.77/mm3, with a sensitivity of 92.3%, and a specificity of 44% (AUC = 0.662; P = 0.048). For red cell distribution width (RDW), the cut-off value was > 12.9%, with a sensitivity of 84.6% and a specificity of 55.1% (AUC = 0.661; P = 0.028). In univariate analysis, monocyte count ≤ 490.77/mm3 and RDW > 12.9% were associated with a colposcopic area > 0.88 cm2 (P = 0.035; P = 0.015, resp.). After multivariate analysis, considering the cofactors age, CIN grade, smoking and HPV type, only RDW remained independent factor OR (95% CI) = 12.825 (1.348–121.971), P = 0.026. Conclusion: Monocyte count and RDW are associated with the lesion colposcopic area. The blood count is a simple, minimally invasive and inexpensive test, associated with the growth of precursor lesions of cervical cancer, and may, in the future, have the potential to be used in the public health system.
Keywords:
human papillomavirus – blood cell count – colposcopy – high-grade squamous intraepithelial lesion
Introduction
Colposcopy is used to evaluate lesions of the female genital tract, especially cervical intraepithelial neoplasia (CIN), being an important tool for analyzing the extent and severity of these lesions. Based on the study by Jarmulowicz et al., the area of the colposcopic lesion is directly related to the cytological status. The larger the lesion area, the greater the likelihood of cytological abnormalities. Therefore, colposcopy plays a crucial role in identifying and monitoring these injuries, allowing decisions to be made about treatment and appropriate management [1].
Currently, in-depth knowledge of immunology remains the main tool in the study of pathophysiology and progression, as well as the treatment of pre-neoplastic cervical lesions. Mantoani et al. emphasize that the cellular immune response is one of the determining factors in the persistence or elimination of HPV infections and their evolution into pre-neoplastic lesions. Although the extent to which it occurs is not entirely clear, it is known that the progression of cervical neoplastic lesions promotes changes in the pattern of cytokine secretion, with the active participation of regulatory T-lymphocytes [2].
One study investigated the role of monocyte-derived dendritic cells (DCs) in patients with cervical intraepithelial lesions (CINs). Activated DCs were able to produce IL-12, an important cytokine in the antitumor immune response. In addition, its differentiation and response were affected by the extent of the cervical lesions. Immunology plays a crucial role in the context of CINs, and understanding the mechanisms of DC differentiation can contribute to more effective therapeutic strategies. In this context, therapeutic vaccines are a promising area of research, although there are still challenges to be overcome, where well-designed clinical studies are needed to evaluate the safety, efficacy, and immunogenicity of these vaccines in patients with high-grade CIN [3].
Knowledge of the changes in the immune pattern that occur during the carcinogenic process helps in the search for potential therapeutic targets in patients susceptible to the use of checkpoint inhibitors [4].
Uterine cervical cancers present higher levels of leukocytosis, neutrophilia, and lymphopenia compared to cervical intraepithelial neoplasias, with neutrophilia being the best biomarker of invasive disease [5]. Patients with cervical intraepithelial neoplasias undergoing surgical treatment experience increased neutrophilia. Increased neutrophil-lymphocyte ratio (NLR) can be used as a predictor of recurrence in patients surgically treated for CIN 2/3, as well as high levels of the platelet-lymphocyte ratio (PLR) [6].
One study concluded that a higher NLR was associated with a worse prognosis in patients with cervical cancer. In addition to the NRL, researchers also analyzed other indices, such as PLR, lymphocyte-monocyte ratio (LMR), thrombocyte-lymphocyte ratio (TLR), CRP/albumin ratio (CAR), and the immune response index [7].
The combined marker multiplication of neutrophils and monocytes (MNM) before treatment is low cost and may be a good candidate as a marker for cervical neoplasia, and also as a predictor of worse prognosis [8]. In addition to MNM, the red cell distribution value (RDW) was significantly higher in cases of cervical cancer, with great potential as a tool in managing cervical cancer risk [9].
There are associations between the colposcopic lesion area in high-grade intraepithelial neoplasia with the blood count ratios (neutrophil-lymphocytes and platelets-lymphocytes) and absolute number of leukocytes. These findings reflect a systemic inflammatory response, even in patients with premalignant cervical lesions. The evaluation of these parameters is simple and low-cost and can help predict the evolution of high-grade CIN [10].
The search for prognostic markers, especially in cervical pre-neoplastic lesions, is of fundamental importance to prevent progression to cervical cancer. The appropriate association of low-cost markers with other data such as the colposcopic lesion area, age, parity, and co-risk factors for progression of HPV-induced lesions could help in therapeutic decisions that are more appropriate for each patient’s profile.
In the public health system, the search for low-cost and accessible markers is essential. Biomolecular tests for HPV have emerged as an important method for screening and post-treatment, but they are still expensive and their access is still limited in developing countries. To our knowledge, this is the first manuscript in the literature that relates hematological parameters with the colposcopic lesion area, demonstrating that even in premalignant lesions restricted to the cervix there is already a systemic inflammatory response.
The objective of the study was to evaluate whether there is a relationship between the lesion area recorded by colposcopy and hematological parameters.
Materials and methodology
A study was carried out at the Gynecological Oncology Service. Women with a confirmed histological diagnosis of cervical intraepithelial neoplasia grades 2/3 (CIN 2/3) through colposcopy and cervical biopsy were included in the study. Exclusion criteria were pregnancy, presence of acute infections, immunosuppressive diseases, infectious diseases (except HPV infection), and use of immunosuppressive medications. Therefore, 62 patients were included in the study.
Research Ethics Committee approved the study (protocol number 37116220.0. 0000.5154). All patients included in the study signed a consent form.
All patients in the study underwent a colposcopy examination. The examination targeted the best locations for an appropriate cervical biopsy. Colposcopic images were captured and archived in a study database. Subsequently, the images were analyzed to measure the area of the lesion. The Image J program was used to calculate the area of the lesions in cm2. When the lesions were multiple, the areas of all lesions were added together, calculating the total area of the lesion. All photos were recorded with the same colposcope at the same magnification (16×) (Fig. 1).
All patients with a confirmed diagnosis of CIN2/3 underwent surgical treatment (high-frequency surgery – LEEP, cold conization, or rarely hysterectomy, except for one patient with CIN 2 who opted for follow-up). Blood counts were recorded in a database specific to the study.
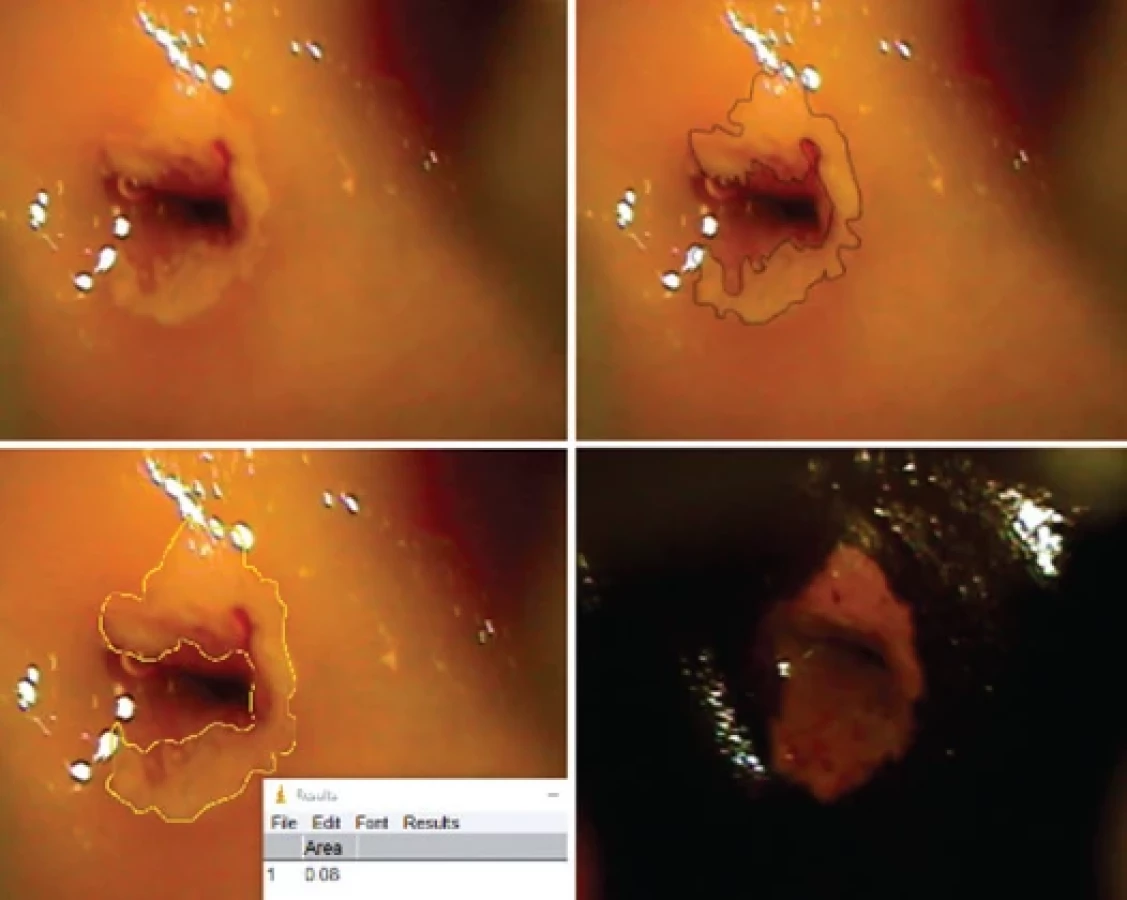
analýza ukázala CIN 3.
CIN – cervical intraepithelial neoplasia/cervikální intraepiteliální neoplazie
Blood count parameters evaluated were: hemoglobin, hematocrit, red blood cells, RDW, absolute number of leukocytes, neutrophils, band neutrophils, segmented neutrophils, eosinophils, monocytes, basophils, lymphocytes, and platelets. Subsequently, neutrophil-lymphocyte ratio (NLR), platelet-lymphocyte ratio (PLR), and lymphocyte-monocyte ratio (LMR) were calculated.
NLR was calculated by dividing the absolute number of neutrophils by the absolute number of lymphocytes. To calculate the PLR, the absolute number of platelets was divided by the absolute number of lymphocytes. When calculating LMR, the absolute number of lymphocytes was divided by the absolute number of monocytes.
Genotyping for HPV 16, 18, 45, and 52 was performed by PCR. Samples were stored in Trizol at –80 °C and thawed when DNA extraction was accomplished. At this time, 200 mL of chloroform was added for each 1.0 mL of Trizol collected. DNA was added to an amplification solution according to the protocol suggested by the manufacturer (Invitrogen, Carlsbad, USA). Characteristics of the indicators synthesized to amplify specific DNA fragments (sequence, size of the amplified product, and temperature annealing) were obtained according to Sarkar & Crissman [11], Tamim et al. [12] and Dictor & Warenholt [13]. Carrying out the PCR reaction, amplification products were subjected to electrophoresis in 14% polyacrylamide gels stained with silver. The Trackit 1 kB DNA ladder (Invitrogen, Carlsbad, USA) was used to estimate the size of the amplified product and the Beta-actina as a positive control of samples; 10.0 mL of amplified sample and 3.0 mL of buffer were homogenized and placed in each opening of a 14% polyacrylamide gel. The gel was run at 90 volts for approximately one hour and then placed in fixative solution for 15 min. This solution was discarded and silver solution was added for 15 min, followed by washing it in Milli-Q H2O and incubating the solution under development for approximately 15 min. The gel was returned to the fixative solution for 15 min, after which the resulting bands were observed.

RDW – red cell distribution width, ROC – receiver operating curve
Data were analyzed using MedCalc and IBM SPSS Statistics Software. The lesion area chosen as the cut-off value was 0.88 cm2, which was the average of the lesion areas. The cut-off value of the blood count parameters was defined using Receiver Operating Characteristic (ROC) curves (checking whether there is a cut-off value for the hematological parameters used in lesions with an area smaller or larger than 0.88 cm2). When there were significant results, a multivariate analysis was performed. The cofactors used were a type of CIN (CIN 2 or CIN 3), age, smoking, and HPV type (16, 18, 45, and 52). Statistical significance was considered when P < 0.05.
Results
In the study, 62 patients were evaluated. All had a confirmed histological diagnosis of cervical intraepithelial neoplasia grades 2/3 (CIN 2/3) by colposcopy and cervical biopsy.
The median age was 34 years (18–68 years) and the median age at sex - ual initiation was 16 years (10–23 years). Twenty-two patients (32.35%) were smokers. Forty-eight patients (76.19%) used hormonal methods for contraception. LEEP treatment was performed in 35 patients (56.45%), where only 17 (27.42%) and 6 (9.68%) patients were treated with knife conization and hysterectomy, resp. Only 4 patients (6.45%) were not treated surgically: 3 of them (4.84%) refused the proposed treatment and 1 (1.61%) patient with CIN 2 opted for clinical follow-up.
When the ROC curves were drawn, there was statistical significance with the absolute value of monocytes and RDW. Regarding the absolute value of monocytes, the cut-off value was ≤ 490.77/mm3, with a sensitivity of 92.3%, and a specificity of 44% (AUC = 0.662; P = 0.048). For RDW, the cut-off value was > 12.9%, with a sensitivity of 84.6% and a specificity of 55.1% (AUC = 0.661; p = 0.028). There was no statistical significance in the evaluation of the other blood count parameters. These data are shown in Fig. 2.
In the univariate analysis, monocyte count ≤ 490.77/mm3 and RDW >12.9% were associated with a colposcopic area greater than 0.88cm2 (P = 0.035; P = 0.015, resp.). Subsequently, a multivariate analysis was performed. The variables evaluated were: type of CIN (CIN 3 vs. CIN 2), age (> 30 y vs. ≤ 30 y), smoking (yes vs. no), monocyte count (≤ 490.77/ mm3 vs. > 490.77/ mm3), RDW (> 12.9 vs. ≤ 12.9), and HPV type (16, 18, 45, and 52). After the multivariate analysis, only RDW remained as an independent factor [OR (95% CI) = 12.825 (1.348–121.971); P = 0.026] (Tab. 1).
Discussion
Studies indicate that the microenvironment of cervical lesions caused by HPV is highly dynamic in relation to the production of hematological and immunological mediators. These mediators influence the cellular immune profile, infiltrating and acting on these lesions [14]. Immunosuppressive mechanisms intrinsic to the injury that enable genome instability, mutations, and activation of proto-oncogenes crucial in the development of cervical cancer are already present in premalignant intraepithelial stages [15]. There are also data that demonstrate action in the other direction of this pathway: distinct systemic immunological profiles that can interfere with the evolution of pre-neoplastic intraepithelial lesions [16].

Studies of the systemic profiles of circulating immune cells and their activity in cervical lesions are still limited [17], but it appears that the severity of intraepithelial cervical lesions may be related to immune cell differentiation processes [3]. We did not find data in the literature regarding systemic profiles related to the size of the area of a high-grade intraepithelial lesion measured with a colposcopic examination. The results of this study did not show an association between the absolute counts of leukocytes, neutrophils, lymphocytes, and platelets, and neither did the NLR, PLR, and LMR relationships with the area of the high - -grade lesions. However, higher NLR and PLR values have already been demonstrated in cervical cancer compared to precursor lesions, including higher values in stage III and IV cervical cancer compared to stage I lesions [18]. Another study demonstrated that peripheral lymphocyte, neutrophil, and platelet counts may reflect the local immune response and be associated with the extent of cervical tumors and the prognosis of cervical cancer [17]. These data can be very important for choosing the treatment of the lesion, since the extent of the pre-neoplastic lesion on colposcopic imaging is a factor that influences the choice of surgical treatment to be offered.
Monocytes are circulating mononuclear phagocytes. They can extravasate to sites of inflammation, and then differentiate into macrophages derived from monocytes and dendritic cells [19]. Higher circulating monocyte counts were reported to be related to higher mortality rates in cervical cancer [20]. Our study found that lower monocyte counts were associated with a larger area of a cervical intraepithelial lesion. This type of relationship was also not found in the literature. However, another study showed that monocyte counts appear to have potential as biomarkers in cervical cancer 8 and higher neutrophil/lymphocyte ratios (NLR), while higher platelet/lymphocyte ratios (PLR) appear to indicate worse prognoses for patients with cervical cancer [7]. One hypothesis would be that at the beginning of the lesions, an inflammatory response is triggered with the systemic production of monocytes, but the immune system tries to overcome this response, leading to a subsequent reduction in levels in larger lesions, in an attempt to prevent progression to invasive cancer. However, more studies and data will be needed to better define this relationship.
Our results showed a positive correlation between higher RDW values and larger cervical cancer precursor lesions. We did not find any studies in the literature that made this comparison. RDW has already been studied as a parameter associated with the diagnosis of cervical cancer, demonstrating significantly higher values in cases of patients with cervical cancer than in controls [15], which was independently associated with worse prognoses and lower overall survival [9]. Higher RDW values were found in invasive lesions than in premalignant intraepithelial lesions [18]. Therefore, the RDW value can be an important marker of the prognosis of cervical injury and potential progression to neoplasia, and can be used in the future as a decision factor in the management and monitoring of patients.
Conclusion
Even cervical pre-malignant lesions can trigger a systemic inflammatory response that is reflected in blood count parameters. The results obtained in this study contribute to the progression of knowledge of the patterns of hematological, immunological, and inflammatory changes that occur during the development of pre-malignant cervical intraepithelial lesions and their progression to cervical cancer. Our results may assist in new search of prognostic markers that can support the choice of effective therapies with lower risks and fewer impacts on the reproductive lives of patients. The blood count is a simple, accessible, minimally invasive and inexpensive test associated with the growth of precursor lesions of cervical cancer, and may, in the future, have the potential to be used in the public health system.
Sources
1. Jarmulowicz MR, Jenkins D, Barton SE et al. Cytological status and lesion size: a further dimension in cervical intraepithelial neoplasia. Br J Obstet Gynaecol 1989; 96 (9): 1061–1066. doi: 10.1111/j.1471-0528.1989.tb03381.
2. Mantoani PT, Siqueira DM, Jammal MP et al. Immune response in cervical intraepithelial neoplasms. Eur J Gynaecol Oncol 2021; 42 (5): 973–981. doi: 10.31083/j.ejgo4205146.
3. Lopes AM, Michelin MA, Murta EF. Monocyte-derived dendritic cells from patients with cervical intraepithelial lesions. Oncol Lett 2017; 13 (3): 1456–1462. doi: 10.3892/ol.2017.5595.
4. Wang Y, He M, Zhang G et al. The imune landscape during the tumorigenesis of cervical cancer. Cancer Med 2021; 10 (7): 2380–2395. doi: 10.1002/cam4.3833.
5. Tavares-Murta BM, Mendonça MA, Duarte NL et al. Systemic leukocyte alterations are associated with invasive uterine cervical cancer. Int J Gynecol Cancer 2010; 20 (7): 1154–1158. doi: 10.1111/IGC.0b013e3181ef8deb.
6. Farzaneh F, Faghih N, Hosseini MS et al. Evaluation of neutrophil-lymphocyte ratio as a prognostic factor in cervical intraepithelial neoplasia recurrence. Asian Pac J Cancer Prev 2019; 20 (8): 2365–2372. doi: 10.31557/APJCP.2019.20.8. 2365.
7. Han X, Liu S, Yang G et al. Prognostic value of systemic hemato-immunological indices in uterine cervical cancer: a systemic review, meta--analysis, and meta-regression of observational studies. Gynecol Oncol 2021; 160 (1): 351–360. doi: 10.1016/j.ygyno.2020.10.011.
8. Cho H, Kim JH. Multiplication of neutrophil and monocyte counts (MNM) as na easily obtainable tumour marker for cervical cancer. Biomarkers 2009; 14 (3): 161–170. doi: 10.1080/13547500902777616.
9. Li Y, Li Z, Zhang G. Clinical utility of red blood cell distribution width for the diagnosis and prognosis of cervical cancer. Int J Gen Med 2022; 15 : 2597–2606. doi: 10.2147/IJGM.S354569.
10. Mantoani PT, Vieira JF, Menchete TT et al. CIN extension at colposcopy: relation to treatment and blood parameters. J Obstet Gynaecol Can 2022; 44 (3): 255–260. doi: 10.1016/ j.jogc.2021.10.008.
11. Sarkar FH, Crissman JD. Detection of human papilloma virus DNA sequences by polymerase chain reaction. Biotechniques 1990; 9 (2): 180–185.
12. Tamim H, Finan RR, Sharida HE et al. Cervicovaginal coinfections with human papillomavirus and Chlamydia trachomatis. Diagn Microbiol Infect Dis 2002; 43 (4): 277–281. doi: 10.1016/s0732-8893 (02) 00403-0.
13. Dictor M, Warenholt J. Single-tube multiplex PCR using type-specific E6/E7 primers and capillary electrophoresis genotypes 21 human papillomaviruses in neoplasia. Infect Agent Cancer 2011; 6 (1): 1. doi: 10.1186/1750-9378-6-1.
14. Yuan Y, Cai X, Shen F et al. HPV post-infection microenvironment and cervical cancer. Cancer Lett 2020; 497 : 243–254. doi: 10.1016/j.canlet.2020.10.034.
15. Wang L, Jia J, Lin L et al. Predictive value of hematological markers of systemic inflammation for managing cervical cancer. Oncotarget 2017; 8 (27): 44824–44832. doi: 10.18632/oncotarget.14827.
16. Swangphon P, Pientong C, Sunthamala N et al. Correlation of circulating CD64+/CD163+ monocyte ratio and stroma/peri-tumoral CD163+ monocyte density with human papillomavirus infected cervical lesion severity. Cancer Microenviron 2017; 10 (1–3): 77–85. doi: 10.1007/s12307-017-0200-2.
17. Huang H, Liu Q, Zhu L et al. Prognostic value of preoperative systemic immune-inflammation index in patients with cervical cancer. Sci Rep 2019; 9 (1): 3284. doi: 10.1038/s41598-019-39150-0.
18. Vaz de Lima PS, Mantoani PT, Murta EF et al. Laboratory parameters as predictors of prognosis in uterine cervical neoplasia. Eur J Obstet Gynecol Reprod Biol 2021; 256 : 391–396. doi: 10.1016/j.ejogrb.2020.11.044.
19. Geissmann F, Jung S, Littman DR. Blood monocytes consist of two principal subsets with distinct migratory properties. Immunity 2003; 19 (1): 71–82. doi: 10.1016/s1074-7613 (03) 0 0174-2.
20. Lee YY, Choi CH, Sung CO et al. Prognostic value of pre-treatment circulating monocyte count in patients with cervical cancer: comparison with SCC-Ag level. Gynecol Oncol 2012; 124 (1): 92–97. doi: 10.1016/j.ygyno.2011.09.034.
Labels
Paediatric gynaecology Gynaecology and obstetrics Reproduction medicineArticle was published in
Czech Gynaecology
2025 Issue 4
Most read in this issue
- HIV infection and adverse perinatal outcomes – a meta-analysis of premature births, low birth weights, and small for gestational age newborns
- Role of tru-cut bio psy in the management of myometrial lesions
- Early detection of recurrent ovarian cancer, current use of oncomarkers, imaging methods, and future perspectives
- Robotic-assisted cesarean scar defect repair