
Can anti-Müllerian hormone predict positive sperm retrieval in men with idiopathic non-obstructive azoospermia?
Authors:
M. C. Çolakoğlu 1; J. E. Horasanlı 2; M. Tül 3; B. Gencel 4; F. Akkuş 5
Authors‘ workplace:
Department of Obstetrics and Gynecology, Ankara Medipol Üniversitesi Faculty of Medicine, Ankara, Turkey
1; Department of Obstetrics and Gynecology, Necmettin Erbakan University Faculty of Medicine, Konya, Turkey
2; A Life Hospital Department of Urology, Ankara, Turkey
3; Department of Obstetrics and Gynecology, Korkuteli State Hospital, Antalya, Turkey
4; Department of Obstetrics and Gynecology, Perinatology Clinic, Kütahya City Hospital, Kütahya, Turkey
5
Published in:
Ceska Gynekol 2025; 90(4): 285-292
Category:
Original Article
doi:
https://doi.org/10.48095/cccg2025285
Overview
Objective: To evaluate whether serum anti-Müllerian hormone (AMH) levels can predict sperm retrieval (SR) outcomes in men with idiopathic non-obstructive azoospermia (iNOA) undergoing microdissection testicular sperm extraction (mTESE), and to develop a predictive model that may inform clinical decision-making. Materials and methods: This retrospective, multicenter cohort study included 72 men diagnosed with iNOA who underwent mTESE between December 2022 and May 2023 at two IVF centers in Turkey. Serum AMH and follicle stimulating hormone (FSH) levels were measured prior to surgery. Patients were categorized into TESE-positive (+SR) and TESE-negative (−SR) groups based on the presence of spermatozoa in testicular tissue. Hormonal and clinical parameters were compared between groups, and a multivariate logistic regression model was constructed to identify independent predictors of SR outcome. Receiver operating characteristic (ROC) curve analysis was performed to determine the diagnostic accuracy and optimal cutoff values for AMH and FSH. Results: Out of 72 patients, 37 (51.4%) had successful SR and 35 (48.6%) did not. Median AMH and FSH levels were significantly higher in the −SR group (P = 0.001 and P = 0.044, resp.). Multivariate logistic regression analysis identified serum AMH as the only independent predictor of positive SR outcome (P < 0.001). ROC analysis revealed excellent diagnostic performance for AMH (AUC = 0.909), with an optimal cutoff value of 3.4 ng/mL yielding 75.68% sensitivity, 91.43% specificity, 90.32% positive predictive value, and 78.05% negative predictive value (P = 0.001). Higher AMH levels were significantly associated with negative SR outcomes. Conclusion: Serum AMH level is a reliable, non-invasive biomarker for predicting SR outcomes in men with iNOA undergoing mTESE. An AMH level > 3.4 ng/mL is significantly associated with a lower probability of sperm retrieval. Incorporating AMH into preoperative assessment may help avoid unnecessary surgical procedures and guide clinical counseling in male infertility management.
Keywords:
Male infertility – biomarker – anti-Müllerian hormone – idiopathic non-obstructive azoospermia – microdissection testicular sperm extraction – sperm retrieval
Introduction
Azoospermia is defined as the absence of spermatozoa in the ejaculate and affects approximately 15% of men with infertility [1]. Aproximately 60% of azoospermic patients have non-obstructive azoospermia (NOA) due to intrinsic testicular spermatogenic insufficiency. Various genes and comorbid conditions have been linked to NOA. While the cause of NOA can sometimes be identified, it is often idiopathic [2,3]. For infertile patients, micro-TESE (testicular sperm extraction) is typically the only option for sperm retrieval. However, testicular sperm extraction is an invasive procedure. If a NOA patient undergoes an invasive procedure and sperm is still not retrieved, this is an undesirable outcome for both the patients and the andrologists. Sperm retrieval rates can vary widely, ranging from 30% to 60% [4,5]. Unfortunately, despite mTESE being associated with the highest theoretical sperm retrieval rate (SR), the sperm extraction procedure was still unsuccessful in approximately 50% of NOA patients [6]. Due to the lack of reliable biomarkers to predict successful sperm retrieval in mTESE, some patients may undergo unnecessary surgery [7].
Anti-Müllerian hormone (AHM) is a dimeric glycoprotein that belongs to the transforming growth factor-b superfamily [8,9]. Previous research has explored the potential of AMH, in effectively predicting both positive and negative SR outcomes in mTESE for idiopathic non-obstructive azoospermia (iNOA) [10,11]. AMH is produced by Sertoli cells in the testes of males. During fetal development and minipuberty, the hypothalamic-gonadotropic axis is active. Follicle stimulating hormone (FSH) promotes AMH expression, and testosterone cannot inhibit it because Sertoli cells lack androgen receptors. In boys with normal or precocious puberty, increased intratesticular androgen concentrations inhibit AMH expression, overriding FSH stimulation and leading to decreased blood AMH levels. The recent establishment of reference range values for serum AMH levels in both boys and men may improve the understanding of its role in gonadal development and its fluctuations during puberty. Pediatric endocrinologists, use AMH blood levels to evaluate the presence and function of testicular tissue in various medical conditions affecting children. For the same purpose, male reproductive specialists are investigating the potential of AMH levels as an indicator of male fertility [12]. However, there is currently limited focus on using this marker in the context of male infertility.
The ability to obtain crucial information about the outcome of mTESE through non-invasive methods prior to sperm extraction would enable more iNOA patients to benefit from the procedure.
While numerous studies have identified factors, either individually or in combination, that may predict the outcome of mTESE, conflicting results still exist [10,13,14]. The reliability of these predictors remains insufficient, as few studies have provided clinical correlations. Therefore, the aim of this study was to assess whether AMH levels could effectively predict the outcome and SR success of mTESE. The goal was to confirm the value of AMH as a predictive marker and assist INOA patients in making informed clinical decisions, potentially avoiding unnecessary surgery and testicular damage in the future.
Materials and methods
This cross-sectional, multicenter study included men diagnosed with iNOA. Infertility was defined according to the World Health Organization (WHO) criteria (2018) as the inability to conceive after at least 12 months of regular unprotected intercourse. Azoospermia was confirmed through at least three consecutive semen analyses. Following confirmation, mTESE was performed at participating IVF centers located in Konya and Ankara, Turkey. The diagnosis of iNOA was established after excluding all known causes of non-obstructive azoospermia, in accordance with current clinical guidelines [12].
Inclusion criteria
Male individuals from infertile couples diagnosed with infertility, and individuals diagnosed with iNOA were included in the study. Patients who satisfied all of the following criteria were included:
- absence of hypogonadotropic hypogonadism;
- no history of cancer or related treatments;
- no use of medications that affect sex hormone levels (e. g., exogenous testosterone, gonadotropins, aromatase inhibitors, selective estrogen receptor modulators) within the past 3 months;
- no history of testicular trauma;
- no obstructive factors.
Exclusion criteria
Patients with Klinefelter or Kallman syndrome; those who had undergone pituitary or testicular surgery and/or previous vasectomy, those with a history of previous tumors including testicular tumors; patients receiving testosterone treatment; individuals with known Y chromosome microdeletions, hypothalamic/pituitary defects; azoospermic patients with testicular factors (cryptorchidism; grade II and III varicocele); patients with genetic abnormalities previously associated with azoospermia, such as mutations and polymorphisms of the cystic fibrosis transmembrane conductance regulator (CFTR) gene and clinical features related to these mutations were excluded from the study. Patients were assessed through a comprehensive self-reported medical history, including age, body mass index (BMI), smoking habits, and comorbidities (diabetes mellitus, hypertension). For the specific purpose of this study, the volume of each testis and the average value of both sides were recorded.
Involving patients who satisfied the above-mentioned exclusion criteria and verification model conditions, we carried out a retrospective cohort study at two IVF centers in Konya and Ankara, Turkey. The cohort was made up of 48 qualifying patients found and treated between December 2022 and May 2023. The institutional ethics committee authorized the study; all clinical data came from medical records.
Surgical technique and sperm cryopreservation
All patients underwent mTESE at one of the IVF centers. The mTESE procedure was carried out as outlined by Almajed et al. [15]. In cases where SR was negative (−SR) in one testis, the contralateral testis was surgically explored. During the mTESE, the tissue was placed in 5 mL of Quinn’s™ Sperm Washing Medium (Origio, Måløv, Norway) and mechanically minced using sterile slides. The resulting sample was then transferred to a Falcon tube, centrifuged at 600 g for 10 minutes at room temperature. After centrifugation, the pellet was resuspended in a minimum volume of 0.5 ml of Quinn’s™ Sperm Washing Medium. Sperm retrieval was evaluated under an inverted microscope at × 400 magnification. Sperm counts were recorded, and SR was reported as the number of sperm per high-power field (HPF). The sample was then cryopreserved. A positive SR (+SR) was defined as the successful retrieval of at least one spermatozoon per 100 HPF (1 spz/100 HPF), as assessed by experienced embryologists. Sperm motility and vitality (assessed via the swelling test) were also documented for all patients before the cryopreservation process.
Blood parameters and hormone levels
Venous blood samples were collected from each patient between 8 and 10 AM after an overnight fast. FSH and LH levels were measured in serum using a heterogeneous competitive magnetic separation assay. AMH levels were measured by an ELISA.
Statistical analyses
Statistical analysis was done using IBM SPSS Statistics version 29.0 (IBM Corp., Armonk, NY, USA) and JASP version 0.18.3.0. Continuous variable distribution was assessed using the Shapiro--Wilk test. Variables with a normal distribution, expressed as mean ± standard deviation (SD), were compared using the independent samples T-test. Non--normally distributed variables, shown as medians (Min.–Max.), were analyzed using the Mann-Whitney U-test. Categorical variables were expressed as frequencies and percentages [N (%) ]; the Chi-square test or Fisher’s exact test, when relevant, was used for comparison. The relationship between serum AMH levels and the likelihood of successful sperm retrieval (TESE positivity) was also modeled using a generalized linear model (GLM) with a binomial distribution and logit link function. The model produced a predicted probability curve with 95% confidence intervals. Receiver Operating Characteristic (ROC) curve analysis was used to assess the predictive accuracy of AMH and FSH levels for successful sperm retrieval outcomes. Calculations were done to find the area under the curve (AUC), optimal cutoff points, negative predictive value (NPV), positive predictive value (PPV), specificity, sensitivity, and so forth. A P value of under 0.05 defined statistical significance.
Results
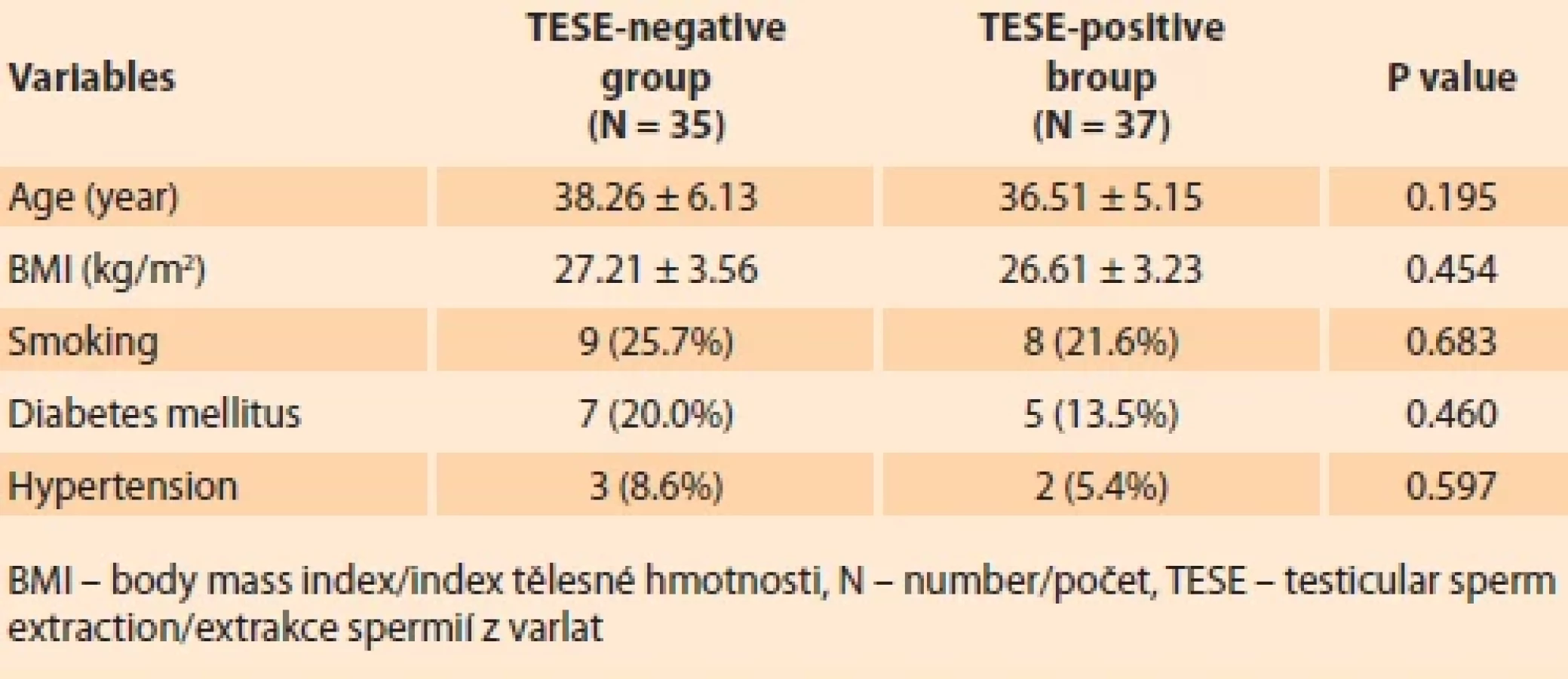
A total of 72 patients with iNOA undergoing mTESE were included in the study. Of the total cohort, 35 patients (48.6%) were classified in the TESE-negative group and 37 patients (51.4%) in the TESE-positive group. Demographic and clinical characteristics are shown in Tab. 1. There were no statistically significant differences between the TESE-negative and TESE-positive groups with regard to age (P = 0.195), BMI (P = 0.454), smoking status (P = 0.683), diabetes mellitus (P = 0.460) or hypertension (P = 0.597).
As shown in Tab. 2, the median FSH level was significantly higher in the TESE-negative group [13.85 mIU/mL (range: 3.67–38.00) ] than in the TESE--positive group [9.54 mIU/mL (range: 2.63–35.00); P = 0.044] (Fig. 1). Similarly, the median AMH level was significantly higher in the TESE-negative group [5.62 ng/mL (range: 2.97–9.23) ] compared to the TESE-positive group [2.80 ng/mL (range: 1.34–6.75); P = 0.001] (Fig. 2).


a TESE-pozitivní skupinou u pacientek s idiopatickou
neobstrukční azoospermií.

A generalised linear model (GLM) with binomial distribution and logit link function was used to assess the association between serum AMH levels and TESE results. As shown in Fig. 3, there was a significant inverse association between serum AMH levels and the likelihood of a positive TESE result. Low AMH levels were associated with an increased like--lihood of sperm retrieval, whereas high AMH levels significantly decreased this likelihood. The shaded area in the figure represents the 95% confidence interval of the model prediction (Fig. 3).
ROC curve analysis was performed to evaluate the diagnostic performance of serum AMH and FSH levels in predicting sperm retrieval success in patients with non-obstructive azoospermia. The area under the curve (AUC) for AMH was 0.909 (95% CI 0.844–0.974), indicating excellent discriminatory ability, while the AUC for FSH was 0.638 (95% CI 0.501–0.776), indicating limited predictive value (Fig. 4). The optimal threshold for AMH was 3.4 ng/mL with a sensitivity of 75.68%, specificity of 91.43%, positive predictive value (PPV) of 90.32% and negative predictive value (NPV) of 78.05% (P = 0.001). The optimal threshold for FSH was 9.69 mIU/mL with 59.46% sensitivity, 85.71% specificity, 81.48% PPV and 66.67% NPV (P = 0.044). These findings suggest that AMH is a more reliable marker than FSH for predicting TESE positivity in patients with non-obstructive azoospermia (Tab. 3, Fig. 4).
Discussion
A significant clinical challenge is determining accurate predictors of positive SR outcomes in men with iNOA undergoing mTESE. Reliable prediction models are essential for identifying the best surgical indications and for improving patient counseling about the chances of a successful sperm retrieval. A significant percentage of men with iNOA continue to have unpredictable negative SR outcomes, necessitating needless surgical procedures, even with continuous efforts to improve patient selection criteria. Despite being regarded as a minimally invasive and generally safe procedure, mTESE is not risk-free. Patients may experience a variety of intraoperative, perioperative, and postoperative complications, such as infection, hematoma formation, persistent testicular pain, and the possibility of developing a long-term testosterone deficiency as a result of unintentional harm to Leydig cell populations. Additionally, poor surgical outcomes can exacerbate psychological distress in a patient population that is already at risk, highlighting the necessity of better preoperative risk assessment. Thus, finding noninvasive, easily available, and trustworthy biomarkers to forecast mTESE success continues to be a top priority in the treatment of iNOA patients [16].



These considerations underscore the critical need for accurate preoperative predictors, especially given that 48.6% of men with iNOA in our cohort experienced a negative SR outcome despite undergoing mTESE. To this end, we performed a multivariate logistic regression analysis, accounted for multiple potential clinical confounders, and identified serum AMH levels as the only clinical biomarker independently associated with a positive SR outcome in this patient population.
Previous studies have suggested that AMH, whether used alone or alongside other hormones, provides limited predictive value for sperm extraction in NOA patients [13,7]. One of these studies concluded that seminal AMH and Inhibin B (INB) levels did not vary according to TESE outcomes in a cohort of 139 men with NOA who underwent mTESE. However, the study included men diagnosed with Klinefelter syndrome and those with Y microdeletions, which may have significantly impacted their findings [18]. Serum INB and the INB/AMH ratio were found to be useful indicators in forecasting the success of sperm retrieval in 168 male patients with iNOA in a different study by Zhao et al. [19]. According to this study, patients with an INB/AMH ratio ≥ 3.19 had an 86.3% sensitivity and a 53.8% specificity for a positive sperm finding. In comparison to INB levels alone, the researchers found that the INB/AMH ratio provides a greater clinical benefit.
Our study showed that serum AMH levels are a reliable biomarker for predicting whether patients with idiopathic nonobstructive azoospermia will be able to obtain sperm through microTESE. Excellent discriminative ability was indicated by the ROC curve analysis, which yielded an AUC value of 0.909 for AMH. 3.4 ng/mL was found to be the ideal threshold value, yielding 75.68% sensitivity, 91.43% specificity, 90.32% positive predictive value, and 78.05% negative predictive value. These results suggest that AMH levels can be used to select patients in clinical practice and can help cut down on needless surgeries. According to earlier research in the literature, AMH levels are a useful indicator for forecasting mTESE success. For instance, a 2017 study by Massimo Alfano et al. found that sperm findings could be predicted with 93% accuracy using an AMH threshold value of less than 4.62 ng/mL [20]. Our study’s lower threshold value of 3.4 ng/mL could be the result of variations in sample size, laboratory measurement techniques, or patient demographics. Serum AMH levels can be used as an auxiliary parameter in clinical decision-making processes for cases of non-obstructive azoospermia, according to the current findings, which are generally in line with the literature. It is believed that these findings should be confirmed with larger sample sizes in the future, and that the variations in threshold values across studies carried out at various centers should be taken into consideration.
Another possible interpretation of the differences observed between sperm retrieval-positive and sperm retrieval--negative iNOA patients is that these groups may represent distinct stages of testicular development or maturation within the gonadal endocrine system. In males, serum AMH levels are characteristically high from infancy through the prepubertal period, reflecting the immature state of Sertoli cell function. As individuals transition into puberty and subsequently reach adulthood, AMH concentrations progressively decline, ultimately falling to approximately 3–4% of neonatal levels [21]. This dynamic change is closely associated with the physiological processes of testicular maturation. During infancy and early childhood, AMH secretion is primarily driven by FSH stimulation, independent of androgenic influence [22,23]. However, with the onset of puberty and the corresponding rise in intratesticular testosterone production, AMH secretion by Sertoli cells is markedly suppressed, highlighting a shift in the regulatory mechanisms governing testicular endocrine function.
In adulthood, the regulatory relationship between AMH and the testicular microenvironment becomes more complex. Unlike during prepubertal development, adult serum AMH levels are significantly downregulated by the presence of testosterone, reflecting the maturation of Sertoli cells and the establishment of spermatogenic capacity [24]. Furthermore, experimental studies have demonstrated that AMH itself may exert paracrine effects within the testicular milieu, particularly by inhibiting steroidogenesis in Leydig cells [25]. This suggests that in adult males, AMH no longer serves a systemic endocrine role, but rather contributes to the local regulation of testicular homeostasis through paracrine signaling pathways. Accordingly, the persistence of elevated AMH levels in adult iNOA patients may indicate an immature Sertoli cell phenotype and a disrupted paracrine network, both of which could adversely affect spermatogenesis and, consequently, the likelihood of successful sperm retrieval during microTESE procedures.
Conclusions
In this study, a regression model was developed to predict sperm retrieval outcomes in men with iNOA and serum AMH level was defined as the only indepen - dent predictor. An AMH level > 3.4 ng/mL was significantly associated with a negative sperm retrieval outcome and showed optimal predictive performance in the model. The application of this model may contribute to the prevention of unnecessary surgical interventions by allowing the early identification of patients who are unlikely to benefit from mTESE.
Sources
1. Gashti NG, Sadighi Gilani MA, Abbasi M. Sertoli cell-only syndrome: etiology and clinical management. J Assist Reprod Genet 2021; 38 (3): 559–572. doi: 10.1007/s10815-021-02063-x.
2. Azizi H, Karoii DH, Skutella T. Whole exome sequencing and in silico analysis of human sertoli in patients with non-obstructive azoospermia. Int J Mol Sci 2022; 23 (20): 12570. doi: 10.3390/ijms232012570.
3. Lee JY, Dada R, Sabanegh E et al. Role of genetics in azoospermia. Urology 2011; 77 (3): 598–601. doi: 10.1016/j.urology.2010.10.001.
4. Rohan P, Daly N, O’Kelly A et al. Evaluation of microdissection testicular sperm extraction (mTESE), outcomes and predictive factors in Ireland: the gold standard for men with non-obstructive azoospermia. J Reprod Infertil 2021; 22 (2): 103–109. doi: 10.18502/jri.v22i2.5795.
5. Bernie AM, Mata DA, Ramasamy R et al. Comparison of microdissection testicular sperm extraction, conventional testicular sperm extraction, and testicular sperm aspiration for nonobstructive azoospermia: a systematic review and meta-analysis. Fertil Steril 2015; 104 (5): 1099.e1–1103.e3. Doi: 10.1016/j.fertnstert. 2015.07.1136.
6. Zhang YX, Yao CC, Huang YH et al. Efficacy of stepwise mini-incision microdissection testicular sperm extraction for nonobstructive azoospermia with varied etiologies. Asian J Androl 2023; 25 (5): 621–626. doi: 10.4103/aja2022125.
7. Tradewell MB, Cazzaniga W, Pagani RL et al. Algorithms for predicting the probability of azoospermia from follicle stimulating hormone: design and multi-institutional external validation. World J Mens Health 2022; 40 (4): 600–607. doi: 10.5534/wjmh.210138.
8. Rey R, Lukas-Croisier C, Lasala C et al. AMH/MIS: what we know already about the gene, the protein and its regulation. Mol Cell Endocrinol 2003; 211 (1–2): 21–31. doi: 10.1016/ j.mce.2003.09.007.
9. Posastiuc FP, Diaconescu AI, Constantin NT et al. Potential biomarkers for testicular cancer in dogs – groundwork for innovative screening programs: a review. Scientific Works. Series C. Veterinary Medicine 2022; 68 (1): 100–107.
10. Benderradji H, Prasivoravong J, Marcelli F et al. Contribution of serum anti-Müllerian hormone in the management of azoospermia and the prediction of testicular sperm retrieval outcomes: a study of 155 adult men. Basic Clin Androl 2021; 31 (1): 15. doi: 10.1186/s12610 - 021-00133-9.
11. Song J, Gu L, Ren X et al. Prediction model for clinical pregnancy for ICSI after surgical sperm retrieval in different types of azoospermia. Hum Reprod 2020; 35 (9): 1972–1982. doi: 10.1093/humrep/deaa163.
12. Goulis DG, Tsametis C, Iliadou PK et al. Serum inhibin B and anti-Müllerian hormone are not superior to follicle-stimulating hormone as predictors of the presence of sperm in testicular fine-needle aspiration in men with azoospermia. Fertil Steril 2009; 91 (4): 1279–1284. doi: 10.1016/j.fertnstert.2008.01.010.
13. Toulis KA, Iliadou PK, Venetis CA et al. Inhibin B and anti-Müllerian hormone as markers of persistent spermatogenesis in men with non-obstructive azoospermia: a meta-analysis of diagnostic accuracy studies. Hum Reprod Update 2010; 16 (6): 713–724. doi: 10.1093/humupd/dmq024.
14. Zhu ZG, Zhao ZG, Pang QY et al. Predictive significance of serum inhibin B on testicular haploid gamete retrieval outcomes in non--obstructive azoospermic men. Asian J Androl 2019; 21 (2): 137–142. doi: 10.4103/aja.aja_ 94_18.
15. Almajed W, Alharbi M, Zini A. Use of mini‐incision microdissection testicular sperm extraction in men with cryptozoospermia and non‐-obstructive azoospermia. Andrology 2020; 8 (5): 1136–1142. doi: 10.1111/andr.12795.
16. Achermann AP, Pereira TA, Esteves SC. Microdissection testicular sperm extraction (micro--TESE) in men with infertility due to nonobstructive azoospermia: summary of current literature. Int Urol Nephrol 2021; 53 (11): 2193–2210. doi: 10.1007/s11255-021-02979-4.
17. El-Halawaty S, Azab H, Said T et al. Assessment of male serum anti-Mullerian hormone as a marker of spermatogenesis and ICSI outcome. Gynecol Endocrinol 2011; 27 (6): 401–405. doi: 10.3109/09513590.2010.495433.
18. Mitchell V, Boitrelle F, Pigny P et al. Seminal plasma levels of anti-Müllerian hormone and inhibin B are not predictive of testicular sperm retrieval in nonobstructive azoospermia: a study of 139 men. Fertil Steril 2010; 94 (6): 2147–2150. doi: 10.1016/j.fertnstert.2009. 11.046.
19. Deng C, Liu D, Zhao L et al. Inhibin B-to-anti--Mullerian hormone ratio as noninvasive predictors of positive sperm retrieval in idiopathic non-obstructive azoospermia. J Clin Med 2023; 12 (2): 500. doi: 10.3390/jcm12020500.
20. Alfano M, Ventimiglia E, Locatelli I et al. Anti-Mullerian hormone-to-testosterone ratio is predictive of positive sperm retrieval in men with idiopathic non-obstructive azoospermia. Sci Rep 2017; 7 (1): 17638. doi: 10.1038/s415 98-017-17420-z.
21. Aksglæde L, Sørensen K, Boas M et al. Changes in anti-Mullerian hormone (AMH) throughout the life span: a population-based study of 1027 healthy males from birth (cord blood) to the age of 69 years. J Clin Endocrinol Metab 2010; 95 (12): 5357–5364. doi: 10.1210/jc. 2010-1207.
22. Young J, Chanson P, Salenave S et al. Testicular anti-mullerian hormone secretion is stimulated by recombinant human FSH in patients with congenital hypogonadotropic hypogonadism. J Clin Endocrinol Metab 2005; 90 (2): 724–728. doi: 10.1210/jc.2004-0542.
23. Chemes HE, Rey RA, Nistal M et al. Physiological androgen insensitivity of the fetal, neonatal, and early infantile testis is explained by the ontogeny of the androgen receptor expression in Sertoli cells. J Clin Endocrinol Metab 2008; 93 (11): 4408–4412. doi: 10.1210/jc.2008-0915.
24. Edelsztein NY, Grinspon RP, Schteingart H et al. Anti-Müllerian hormone as a marker of steroid and gonadotropin action in the testis of children and adolescents with disorders of the gonadal axis. Int J Pediatr Endocrinol 2016; 2016 : 20. doi: 10.1186/s13633-016-0038-2.
25. Teixeira J, Maheswaran S, DonahoeP PK. Mullerian inhibiting substance: an instructive developmental hormone with diagnostic and possible therapeutic applications. Endocr Rev 2001; 22 (5): 657–674. doi: 10.1210/edrv.22.5.0445.
Labels
Paediatric gynaecology Gynaecology and obstetrics Reproduction medicineArticle was published in
Czech Gynaecology
2025 Issue 4
Most read in this issue
- HIV infection and adverse perinatal outcomes – a meta-analysis of premature births, low birth weights, and small for gestational age newborns
- Role of tru-cut bio psy in the management of myometrial lesions
- Early detection of recurrent ovarian cancer, current use of oncomarkers, imaging methods, and future perspectives
- Robotic-assisted cesarean scar defect repair