
Coincidental maternal mortality in Slovakia in the years 2007 – 2024
Authors:
D. Kotríková; M. Vargová; A. Adamec; A. Krištúfková; M. Korbeľ
Authors‘ workplace:
st Department of Obstetrics and Gynaecology, Faculty of Medicine, Comenius University in Bratislava, Slovak Republic
1
Published in:
Ceska Gynekol 2025; 90(4): 278-284
Category:
Original Article
doi:
https://doi.org/10.48095/cccg2025278
Overview
Objective: Analysis of coincidental maternal mortality in Slovakia in the years 2007–2024 from the database of the Slovak Gynecological and Obstetric Society (enhanced surveillance system). Methods: Retrospective population analysis of maternal mortality from 2007 to 2024 focused on coincidental maternal deaths. Analysis of coincidental maternal death cases was carried out according to the International Classification of Diseases (ICD-10) for Maternal Mortality (ICD-MM). Results: Between 2007 and 2024, a total of 123 women died. The maternal mortality ratio (MMR) was 12.46 per 100 000 live births. Fifteen women (12.20%) died from coincidental causes (MMR 1.52 per 100 000 live births). From direct causes, 51 women died (41.46%), from indirect causes, 54 women died (43.90%), and three women died (2.44%) from an unknown cause of death. Out of the coincidental deaths, 80.0% were due to polytrauma – car accidents (66.67%), train accident (6.67%), and entrapment in an elevator shaft (6.67%). Three cases of deaths were due to homicide (domestic violence) – 20%. Conclusion: The study highlights the problem of under-recognition of coincidental maternal deaths, despite its significant impact on public health. The Slovak Gynecological and Obstetrics Society attempts to identify and collect data on coincidental maternal mortality in Slovakia, which is not included in vital statistics. Addressing this overlooked issue is crucial for enhancing maternal health outcomes and ensuring comprehensive maternal safety worldwide.
Keywords:
polytrauma – Homicide – maternal mortality ratio – maternal deaths – coincidental maternal mortality
Introduction
Coincidental (in literature also mentioned as unintentional/accidental, incidental or non-obstetrical maternal deaths) maternal mortality (MM) refers to deaths occurring during pregnancy, labour or within the postpartum period due to causes unrelated to pregnancy or any medical condition. These include accidents, such as any kind of traffic accident, homicides or event of undetermined intent [1]. While direct and indirect MM have been extensively studied, coincidental maternal deaths often receive less attention, despite their significant contribution to overall maternal mortality rates [2,3]. Official data of the World Health Organisation (WHO) even exclude these deaths from its official maternal mortality statistic, as they are not considered preventable through medical care [4]. However, some coincidental deaths may be preventable through appropriate precautions, such as road safety measures to reduce fatal accidents or protective interventions to address violence against pregnant women [2,5].
Understanding the scope and causes of coincidental MM is crucial for improving maternal health outcomes and implementing targeted interventions. Despite its underreporting and exclusion from statistics, coincidental maternal deaths have a significant impact on the ability of policymakers to under-stand potential social and family situations [2].
Differences in classification criteria, inconsistent data collection methods, lack of standardized reporting, and misclassification of these deaths contribute to discrepancies in maternal mortality records. This results in underreporting of coincidental maternal deaths and the actual impact of these deaths may be underestimated, limiting awareness and restricting the development of effective prevention strategies [2,6].
This paper explores the causes of coincidental maternal deaths and their underreporting in Slovakia in 2007–2024. By analysing recent data and case studies, it aims to provide a clearer understanding of the impact of these deaths on maternal health frameworks. Recognizing and addressing coincidental MM is essential for comprehensive maternal healthcare policies and strategies aimed at reducing preventable maternal deaths.
Material and methods
This was a retrospective population--based descriptive study of MM cases in Slovakia from 2007 to 2024. Cases of coincidental maternal deaths are collected by the Slovak Gynaecology and Obstetrics Society (SGOS) from 2007 (enhanced surveillance system). Since coincidental maternal deaths in Slovakia are not reported properly, the majority of the presented data were obtained from active case searches from non-obstetrics hospital workplaces and mass media sources. Only a few of the presented cases were reported by hospitals after the death of the patient.
The analysis of coincidental cases maternal deaths was carried out according to the International Classification of Diseases (ICD-10) for Maternal Mortality (ICD-MM). This ICD-MM classification excludes suicides from coincidental causes [1].
Results are presented in absolute numbers, in percentages and in MMRs (maternal mortality ratio – the number of maternal deaths per 100,000 live births). Non-normally distributed continuous variables (based on the Shapiro-Wilks test and Q-Q plots) were reported as median (IQR – interquartile range).
The confidence intervals (CI 95%) for the MMRs were estimated using a Poisson distribution method. The age groups were compared using unadjusted relative risk (RR) with 95% CI. All statistical analyses were performed using MedCalc Software Ltd. Version 20.015 and Office Excel.
Results
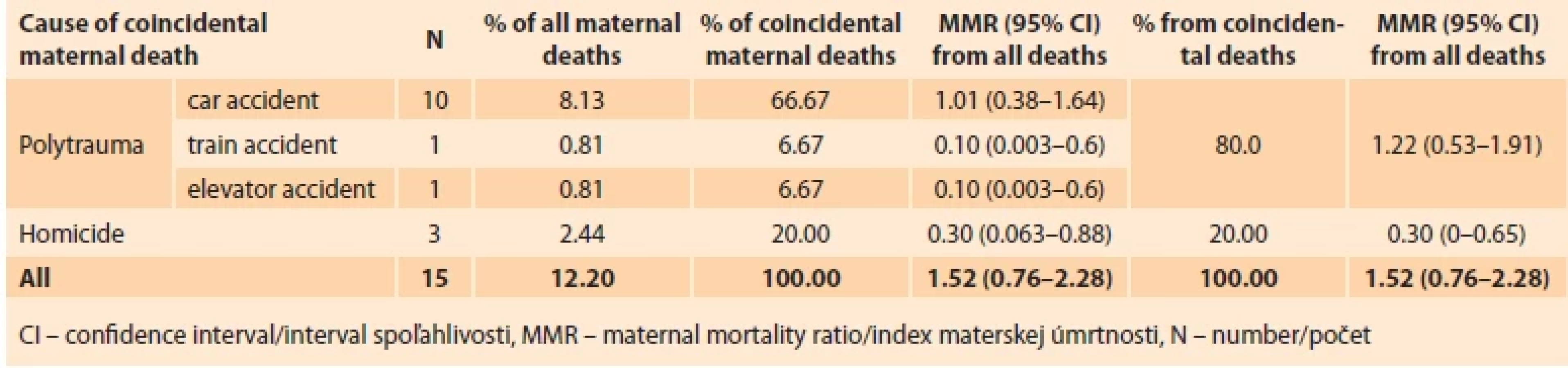
According to SGOS data, there were 987,181 live births in Slovakia between 2007 and 2024, and a total of 123 women died. The MMR (per 100,000 live births) in this period was 12.46. From coincidental causes 15 women died, which accounted for 12.20% of all maternal deaths in Slovakia, with MMR 1.52. There were 51 (41.46%) deaths from direct causes, 54 (43.90%) from indirect causes and three (2.44%) deaths from an unknown cause of death.
The most common cause of coincidental death was polytrauma (80% of coincidental maternal deaths) – 10 cases of car accident (66.67%), one case of train accident (6.67%) and one case of entrapment in an elevator shaft (6.67%). Three cases of deaths were homicide – domestic violence (20%) (Tab. 1).
The age of the 13 deceased women varied from 17 to 38 years. The age of two woman (13.33%) being unknown. Median age was 31 years (IQR 25 – 36 years). 13 women died during pregnancy (86.67%), one woman died three weeks after labour (6.67%) and one died after legal abortion (6.67%).
Since some of these cases were collected only from mass media sources, there is a lack of information about these patients. The coincidental deaths are summarised in Tab. 2, and the individual cases of death are described below.
Case 1
A 36-year-old woman at 35 weeks of pregnancy was involved in a car accident, resulting in uterine rupture with placental abruption, as well as rupture of the right atrium of the heart, lungs, liver, spleen, and a transverse lesion of the cervical spine. She was seated in the front passenger seat and was properly restrained with a seatbelt. After being transported to the hospital, an emergency caesarean section was performed – a dead eutrophic male fetus was born [7].
Case 2
A woman from Romania of unknown age (traveling across Slovakia), approximately in the 6th–7th month of pregnancy, was involved in a car accident that resulted in a high spinal cord injury with central nervous system failure. Information about seat-belt use is absent. The male foetus survived without any traumatic harm [8].
Case 3
A 30-year-old woman in the 6th month of pregnancy was involved in a car accident right before her wedding. Information about seat-belt use is absent [9].
Case 4
A 25-year-old woman in the 7th month of pregnancy died in a car accident. The young woman had been seated in the back seat, her mother in the front passenger seat, and her father was driving. The paramedics found the woman lying outside the vehicle and had likely been ejected from the car after the crash. The initiated cardiopulmonary resuscitation (CPR) was unsuccessful. The woman was not wearing seat belt. This case was reported to SGOS from regional obstetrical department [10].
Case 5
A 30-year-old woman in the 6th month of pregnancy died in a car accident with her husband and daughter after the car crossed into the opposite lane. All passengers were wearing seat belts [11].
Case 6
A woman in the 8th month of pregnancy died in a head-on collision between two cars. Information about seat-belt use is absent [12].

Case 7
A 34-year-old pregnant woman, mother of six children, died in a traffic accident. Firefighters found the pregnant woman about 10 meters out from the vehicle. The woman was not wearing a seat belt [13].
Case 8
A 27-year-old woman in the 7th month of pregnancy skidded on the road in her car after heavy snowfall and crashed into an oncoming vehicle. Information about seat-belt use is absent [14].
Case 9
A 37-year-old woman in her 6th month of pregnancy was hit by a car while attending a veteran car race as a spectator. One of the vintage cars veered off the road during a promotional ride and crashed into the crowd [15].
Case 10
A 36-year-old woman in the 5th month of pregnancy died after a collision between her scooter and a bus under unclear circumstances [16].
Case 11
A 38-year-old woman in the 27th week of pregnancy was struck by a train at a railway crossing. The woman, her husband and son were unlawfully present on the track. While the father and son managed to move out of the way in time, the woman misjudged a safe distance, and a passenger train hit her, knocking her to the ground, where she remained motionless. The paramedics performed CPR and the woman was transported to the hospital in an induced coma in critical condition. Doctors attempted to save the child by performing a caesarean section, but neither the woman nor the child could be saved. This case was reported to SGOS from the obstetrics department, where the woman had received care [17].
Case 12
A 25-year-old woman, three weeks postpartum after a spontaneous delivery, became crushed by an elevator with her infant. She was rescued from the elevator shaft after 20 minutes with multiple injuries and cardiopulmonary resuscitation with intubation was initiated. The woman was transferred to the Department of Anaesthesiology and Intensive Care due to a severe impairment of consciousness at the level of coma. In the absence of spontaneous breathing and the loss of reflexes, brain death was confirmed, and subsequent care was provided with consideration for organ donation (kidneys, pancreas, spleen, liver, heart and adrenal gland were donated). The autopsy confirmed traumatic asphyxia (Perte’s syndrome). This case was reported by Department of Anaesthesiology and Intensive Care, and also published in mass-media [18].
Case 13
An 18-year-old woman was murdered with knife by her partner in the 4th month of pregnancy. Later he tried to attempt a suicide [19].
Case 14
A 32-year-old woman, one day after undergoing a legal abortion at 10th weeks of pregnancy, was stabbed by her partner. The man later also committed suicide. This case was reported to SGOS from the gynaecological department, where the abortion was managed. The case was published by mass media too, but with incorrect information about the patient [20].
Case 15
A 17-year-old woman with a stab wound, who was six months pregnant, was discovered at home. The murder suspect is her partner [21].
Discussion
Coincidental maternal deaths, although not directly related to pregnancy, represent a significant yet often overlooked part of MM. These deaths, resulting from causes such as traffic accidents, falls, drowning, and violence, are frequently ignored by many studies, since the WHO focusses its statistics on deaths that can be influenced by improvements in healthcare (direct and indirect maternal deaths) [4,22].
At present, there are only a few studies on coincidental deaths during pregnancy and puerperium in the world and we do not have relevant data from other countries. In the cases of coincidental maternal deaths, the patient rarely dies in the hospital ward and therefore obtaining information on these deaths is difficult. However, their inclusion in maternal health discussions is critical, as many of these deaths may be preventable through targeted public health interventions and require more care and attention from society [2].
According to the European Board and College of Obstetrics and Gynaecology (EBCOG), it is desirable in high--income countries, that all deaths are collected and analysed, including coincidental and late (more than 42 days but less than one year after termination of pregnancy) [23].
In Slovakia, the majority of coincidental maternal deaths were due to trauma. The most common cause of trauma was motor vehicle accidents, accounting for 68.8% of coincidental maternal deaths and 9% of all deaths.
The trauma incidence during pregnancy is approximately 6–8% worldwide and represents one of the most common non-obstetric causes of maternal deaths [24,25]. In the United States of America (USA), trauma is the leading non-obstetric cause of maternal death [26]. The leading cause of trauma-related deaths is motor vehicle accidents, which also include train accidents, and account for more than half of all maternal trauma (55–85%). It is followed by violence and assault in many countries [2,27–29].
In the USA, motor vehicle crashes are responsible for approximately one million injuries of pregnant women each year and the rate of injury has risen over time. This is mainly due to the increasing number of miles driven by pregnant women [5].
Among pregnant women, studies have shown that seat belts are effective at reducing the risk of adverse maternal and foetal outcomes. Given the evidence suggesting the benefits of seat belt use during pregnancy, it is important that all pregnant women wear belts and wear them properly while in a motor vehicle. Improper restraints can result in an increased risk of uterine rupture or abdominal injuries that may further result in excessive maternal bleeding and/or foetal death [5].
In the USA, an estimated 84.1% of pregnant women reported wearing seat belts. Women who refrain from wearing seat belts during pregnancy report that they find them uncomfortable or fear that they will cause injury to themselves or their foetus. Proper education about the importance of belts and correct placement can minimize concerns and correct misconceptions that prevent women from wearing belts and can increase proper belt use [5,30]. We do not possess the information about seat-belt use in majority of our group of patients that died in car accident, since these deaths were not reported and we do not have more details about the accidents. Out of the eight women, who were in the car during the traffic accident (cases 1–8), two were wearing a seatbelt (case 1 and 5), while other two were not (case 4 and 7). For the remaining four cases (cases 2, 3, 6 and 8), it is not known whether the women were wearing seatbelts.
Another case of trauma in Slovakia was due to entrapment in an elevator shaft (case 12). There is limited information and studies addressing the entrapment in elevator shafts involving pregnant or postpartum women, but some cases of death have been reported in the mass media. There is one similar case to our reported in Spain – entrapment in an elevator while being transported after caesarean section [31]. Other published elevator accidents were the fall of the elevator while being transported after spontaneous labour in India and elevator fire in Albania [32,33]. There is also a case of death of a woman, who fell to the escalator shaft in China [34]. These accidents happened because of lack of elevator control or poor quality of the elevator.
The patient from our study was crushed between the elevator and wall of the building with her child. She died because of mechanical asphyxia (Perte’s syndrome), in which respiration is limited due to external pressure on the chest/abdomen. Symptoms, in addition to external traumatic injuries, include cervicofacial cyanosis due to blood stasis, petechiae on the skin, subconjunctival haemorrhage, and neurological symptoms (altered consciousness, disorientation, loss of consciousness, and even coma). The prognosis depends on the extent of the injuries and the restoration of oxygenation and tissue perfusion. Chest compression lasting more than 10 minutes leads to cerebral anoxia [35]. In our case, the woman was extricated from the shaft after 20 minutes.
A big study of 239 cases of coincidental MM was conducted in China in the years 2009–2019. They reported a coincidental MMR of 2.8 per 100,000 live births. Higher MM was in rural areas. This study also included suicides in the statistics, which was the most common cause of accidental maternal death in China. Suicides were followed by traffic accidents, accidental poisoning/overdose and assault/homicide [2]. If suicides were excluded from the Chinese study, the MMR of coincidental mortality in China would be 1.8 per 100,000 live births. For such a large and populous country as China, this MMR is relatively low. In Slovakia, the MMR for coincidental maternal deaths was 1.52, which is lower, but given the significantly smaller population, this number is quite high. In our study, suicides were not included in coincidental maternal deaths, because the ICD-MM includes these deaths to direct MM (Direct deaths without an obstetric code in ICD-10) [1].
Interesting study from USA reported homicide as the leading cause of pregnancy associated coincidental death. Homicide deserves special attention because most of the cases are the result of partner violence [6,25]. Despite the fact that homicides do not have a physiologic relationship to pregnancy, some homicides, especially those due to intimate-partner violence, may not have occurred if the victim had not been pregnant [6]. In the USA, the risk of homicide was greater for younger women (under 24 years) and was 35% greater for pregnant and postpartum women than for their nonpregnant, non-postpartum counterparts [36,37]. In Chinese study, assault/homicide accounted for 5.4% of coincidental maternal deaths [2].
The majority of pregnancy-associated homicides were committed by current or former intimate partners, most commonly during the first 3 months of pregnancy. Younger women, under the age of 25, those from ethnic minority backgrounds, and women suffering domestic abuse appear to be most at risk. The most common perpetrator reported across all countries was an intimate partner, particularly one involved with drugs or alcohol. The prevention of intimate-partner homicide therefore could have a major effect on reducing the overall rate of pregnancy associated mortality [6,38,39].
There were three cases of homicide (20% of all coincidental MM) in Slovakia, all by intimate-partner.
Preventive measures to decrease coincidental maternal mortality
Because maternal trauma is likely the leading cause of maternal mortality, potential measures for improvement should be included. Prevention is the key to decreasing traumatic maternal mortality. Motor vehicle crashes and domestic violence are the most common preventable causes. One-third of pregnant patients do not use safety restraints properly, and only a minority of women report physician counselling on this topic.
Preventing maternal deaths due to motor vehicle accidents involves promoting the proper use of seatbelts, which is a crucial safety measure. Seatbelts significantly enhance passenger safety and reduce the risk of injury during a crash, yet it is essential to ensure they are used correctly. The lap belt should be positioned below the abdomen, across the pelvis, to avoid pressure on the uterus, while the shoulder belt should cross between the breasts and over the collarbone to minimize upper body injury. Wrong positioning of the seatbelts can be associated with the so-called “seat belt syndrome” (musculoskeletal and visceral injuries associated with the force transmitted by the seat belt – skin abrasions/bruising, fractures of the spine, ribs, sternum, clavicle, liver and spleen laceration, pulmonary/myocardial contusion) [40].
Pregnant women should avoid placing the lap belt over the stomach, as this notably increases the transmission of pressure to its surface, potentially leading to uterine and foetal injury. It is essential for a woman to wear a seatbelt not only when driving but also as a front - or rear-seats passenger. Additionally, improvements in vehicle safety features, such as airbags designed for pregnant women, can further reduce the risk of fatal outcomes from motor vehicle accidents [5,41].
Violence against women by their partners during pregnancy is a major public health concern [42]. According USA study, violence prevention efforts may not only directly prevent homicide during pregnancy and postpartum (a leading single cause of maternal death), but may also indirectly reduce maternal mortality from obstetric causes through the elimination of a psychosocial environmental stressor [43].
It is not clear what sort of intervention best serves women and infants during pregnancy and after giving birth to ensure their safety. Preventing domestic violence and homicide among pregnant women requires a comprehensive approach that integrates healthcare screening, legal measures, and social support systems. Interventions that might work include counselling and psychological therapy to give women more confidence and to encourage them to make plans to avoid abuse [42]. Routine screening for intimate partner violence (IPV) in the health care setting could identify women at risk of or experiencing IPV and lead to interventions that reduce violence and improve maternal and child outcomes [44]. Access to specialized support services, including shelters, legal assistance, social workers, and psychological counselling, plays a crucial role in ensuring the safety of pregnant women facing IPV [42].
Limitation of this study is the accuracy of data on coincidental maternal mortality, which is highly dependent on the quality and completeness of reporting systems. However, the data quality on maternal mortality in Slovak vital statistics is poor. Maternal deaths in Slovakia in vital statistics are highly underreported (69.7% in comparison to an enhanced surveillance system), and coincidental maternal deaths in vital statistics are not reported. The retrospective nature of the study and not reporting these deaths are the reasons for incomplete medical records and insufficient information (demographic, socioeconomic, obstetric) about deceased women. We also cannot entirely rely on the information found in the mass media to be true (e. g., case 15).
Despite these limitations, this is the first study to analyse the characteristics of coincidental maternal deaths in Slovakia, addressing a critical gap in the literature. By highlighting potential preventive measures, it contributes to public health efforts aimed at reducing avoidable maternal deaths. This study high--lights the need for improved data collection and classification and advocates for more precise surveillance systems to enhance maternal health outcomes globally.
Conclusion
Coincidental maternal mortality remains an underrecognized contributor to maternal deaths worldwide, despite its significant impact on public health. In Slovakia between 2007 and 2024, out of 123 maternal deaths were 15 coincidental (12.20%) with MMR 1.52 per 100,000 live births. Out of 15 coincidental deaths, only four were officially reported, while other 11 were found by active search in the mass media. SGOS attempts to identify and collect data on coincidental maternal mortality, recognising that in some cases, maternal death may be potentially preventable through proper safety measures. Strengthening data collection and classification methods is essential to accurately assess the true burden of these deaths and inform public health policies aimed at reducing preventable maternal fatalities.
Sources
1. WHO. The WHO application of ICD-10 to deaths during pregnancy, childbirth and puerperium: ICD MM. 2012 [online]. Available from: https: //www.who.int/publications/i/item/ 9789241548458.
2. Kong F, Wang A, Su J et al. Accidental death during pregnancy and puerperium from 2009 to 2019 in Hunan, China: a cross-sectional study. BMJ Open 2021; 11 (9): e047660. doi: 10.1136/bmjopen-2020-047660.
3. Cheung KW, Seto MT, Wang W et al. Characteristics of maternal mortality missed by vital statistics in Hong Kong, 2000–2019. JAMA Netw Open 2023; 6 (2): e230429. doi: 10.1001/jamanetworkopen.2023.0429.
4. WHO. Trends in maternal mortality 2000 to 2020: estimates by WHO, UNICEF, UNFPA, World Bank Group and UNDESA/Population Division. 2023 [online]. Available from: https: //iris.who.int/bitstream/handle/10665/366225/9789240068759-eng.pdf?sequence=1.
5. Vladutiu CJ, Weiss HB. Motor vehicle safety during pregnancy. Am J Lifestyle Med 2012; 6 (3): 241–249. doi: 10.1177/1559827611421304.
6. Wallace ME, Hoyert D, Williams C et al. Pregnancy-associated homicide and suicide in 37 US states with enhanced pregnancy surveillance. Am J Obstet Gynecol 2016; 215 (3): 364.e1–364.e10. doi: 10.1016/j.ajog.2016.03.040.
7. Korbeľ M, Borovský M, Danko J et al. Analýza materskej mortality v SR za rok 2007. Gynekol prax 2009; 7 (1): 26–29.
8. Korbeľ M, Borovský M, Danko J et al. Maternal mortaity in the Slovak republic in the year 2009 – II. (Indirect and accidental or incidental maternal deaths). Gynekol prax 2014; 12 (1): 37–43.
9. Topky.sk. 2012 [online]. Available from: https: //www.topky.sk/cl/1000068/1294137/.
10. Noviny.sk. 2012 [online]. Available from: https: //www.noviny.sk/krimi/110184-.
11. Tvnoviny.sk. 2023 [online]. Available from: https: //tvnoviny.sk/domace/clanok/844430-.
12. Domov.sme.sk. 2008 [online]. Available from: https: //domov.sme.sk/c/3708811/.
13. Zemplin.korzar.sme.sk. 2007 [online]. Available from: https: //dolnyzemplin.korzar.sme.sk/c/4445524/.
14. Cas.sk. 2010 [online]. Available from: https: // www.cas.sk/clanok/148994/.
15. Spravy.pravda.sk. 2012 [online]. Available from: https: //spravy.pravda.sk/domace/ clanok/247669--.
16. Cas.sk. 2015 [online]. Available from: https: //www.cas.sk/clanok/321643/.
17. Noviny.sk. 2023 [online]. Available from: https: //www.noviny.sk/krimi/753851-.
18. Tvnoviny.sk. 2021 [online]. Available from: https: //tvnoviny.sk/domace/clanok/132418-.
19. Noviny.sk. 2011 [online]. Available from: https: //www.noviny.sk/slovensko/87441-.
20. Spravy.pravda.sk. 2020 [online]. Available from: https: //spravy.pravda.sk/regiony/ clanok/714187-
21. Noviny.sk. 2022 [online]. Available from: https: //www.noviny.sk/krimi/717449-.
22. Huang R, Spence A, Abenhaim H. Racial disparities in national maternal mortality trends in the United States from 2000 to 2019: a population-based study on 80 million live births. Arch Gynecol Obstet 2024; 309 (4): 1315–1322. doi: 10.1007/s00404-023-06999-6.
23. Kallianidis AF, Velebil P, Alexander S et al. European Board and College of Obstetrics and Gynaecology position statement on maternal mortality surveillance in Europe. Eur J Obstet Gynecol Reprod Biol 2024; 299 : 345–349. doi: 10.1016/j.ejogrb.2024.05.022.
24. Maganha CA, Ribeiro MA Jr, Mattar R et al. Trauma and pregnancy. Rev Bras Ginecol Obstet 2023; 45 (10): 622–632. doi: 10.1055/s-00 43-1777339.
25. Romero VC, Pearlman M. Maternal mortality due to trauma. Semin Perinatol 2012; 36 (1): 60–67. doi: 10.1053/j.semperi.2011.09.012.
26. Oxford CM, Ludmir J. Trauma in pregnancy. Clin Obstet Gynecol 2009; 52 (4): 611–629. doi: 10.1097/GRF.0b013e3181c11edf.
27. Irving T, Menon R, Ciantar E. Trauma during pregnancy. BJA Educ 2021; 21 (1): 10–19. doi: 10.1016/j.bjae.2020.08.005.
28. Hill CC. Trauma in the obstetrical patient. Womens Health (Lond) 2009; 5 (3): 269–285. doi: 10.2217/WHE.09.6.
29. Morikawa M, Yamada T, Kogo H et al. Effect of an educational leaflet on the frequency of seat belt use and the rate of motor vehicle accidents during pregnancy in Japan in 2018: a prospective, non-randomised control trial with a questionnaire survey. BMJ Open 2019; 9 (9): e031839. doi: 10.1136/bmjopen-2019 - 031839.
30. Beck LF, Gilbert BC, Shults RA. Prevalence of seat belt use among reproductive-aged women and prenatal counseling to wear seat belts. Am J Obstet Gynecol 2005; 192 (2): 580–585. doi: 10.1016/j.ajog.2004.07.027.
31. BBC.com. 2017 [online]. Available from: https: //www.bbc.com/news/world-europe - 40999568.
32. Timesofindia.indiatimes.com. 2024 [online]. Available from: https: //timesofindia.indiatimes.com/india/after-giving-birth-woman-dies-as-hospital-lift-belt-snaps/articleshow/116057177.cms.
33. Telegrafi.com. 2016 [online]. Available from: https: //telegrafi.com/en/the-woman-who-burned-in-the-elevator-was-6-months-pregnant/.
34. Edition.cnn.com. 2015 [online]. Available from: https: //edition.cnn.com/2015/07/27/ china/chinese-mother-killed-escalator/index.html.
35. Karamustafaoglu YA, Yavasman I, Tiryaki S et al. Traumatic asphyxia. Int J Emerg Med 2010; 3 (4): 379–380. doi: 10.1007/s12245-010 - 0204-x.
36. Wallace ME. Trends in pregnancy-associated homicide, United States, 2020. Am J Public Health 2022; 112 (9): 1333–1336. doi: 10.2105/AJPH. 2022.306937.
37. Campbell J, Matoff-Stepp S, Velez ML et al. Pregnancy-associated deaths from homicide, suicide, and drug overdose: review of research and the intersection with intimate partner violence. J Womens Health (Larchmt) 2021; 30 (2): 236–244. doi: 10.1089/jwh.2020.8875.
38. Cheng D, Horon IL. Intimate-partner homicide among pregnant and postpartum women. Obstet Gynecol 2010; 115 (6): 1181–1186. doi: 10.1097/aog.0b013e3181de0194.
39. Cliffe C, Miele M, Reid S. Homicide in pregnant and postpartum women worldwide: a review of the literature. J Public Health Policy 2019; 40 (2): 180–216. doi: 10.1057/s41271-018 - 0150-z.
40. Huecker MR, Chapman J. Seat Belt Injury. Updated 2023. In: StatPearls [online]. Available from: https: //www.ncbi.nlm.nih.gov/books/ NBK470262/.
41. Kepák J. Dopravní polytrauma a těhotenství – nezbytnost a možnosti prevence. Prakt Gynekol 2004; 8 (1): 14–18.
42. Jahanfar S, Howard LM, Medley N. Interventions for preventing or reducing domestic violence against pregnant women. Cochrane Database Syst Rev 2014; 2014 (11): CD009414. doi: 10.1002/14651858.CD009414.pub3.
43. Wallace ME, Friar N, Herwehe J et al. Violence as a direct cause of and indirect contributor to maternal death. J Womens Health (Larchmt) 2020; 29 (8): 1032–1038. doi: 10.1089/jwh.2019.8072.
44. Alhusen JL, Ray E, Sharps P et al. Intimate partner violence during pregnancy: maternal and neonatal outcomes. J Womens Health (Larchmt) 2015; 24 (1): 100–106. doi: 10.1089/jwh.2014.4872.
Labels
Paediatric gynaecology Gynaecology and obstetrics Reproduction medicineArticle was published in
Czech Gynaecology
2025 Issue 4
Most read in this issue
- HIV infection and adverse perinatal outcomes – a meta-analysis of premature births, low birth weights, and small for gestational age newborns
- Role of tru-cut bio psy in the management of myometrial lesions
- Early detection of recurrent ovarian cancer, current use of oncomarkers, imaging methods, and future perspectives
- Robotic-assisted cesarean scar defect repair