
Large urethral false passage during a routine catheterization – low threshold for better outcome
Authors:
S. Kakoti 1; M. De 2; S. S. Boro 2; R. Medhi 3
Authors‘ workplace:
Department of Urology, All India Institute of Medical Sciences, Guwahati, Assam, India
1; Department of Plastic, Reconstructive & Burns Surgery, All India Institute of Medical Sciences, Guwahati, Assam, India
2; Department of ENT, Head & Neck Surgery, All India Institute of Medical Sciences, Guwahati, Assam, India
3
Published in:
ACTA CHIRURGIAE PLASTICAE, 67, 4, 2025, pp. 273-274
Category:
doi:
https://doi.org/10.48095/ccachp2025273
Dear Sirs,
urethral catheterization is one of the most performed interventions in patients across all surgical and medical specialties. Unfortunately, this procedure still has high complications due to inadvertent urethral injury. We would like to highlight a case where catheterization led to creation of a false passage almost as large as the urethra. This is to emphasize that one cannot be careful enough to avoid such injuries and early intervention is key to a good outcome.
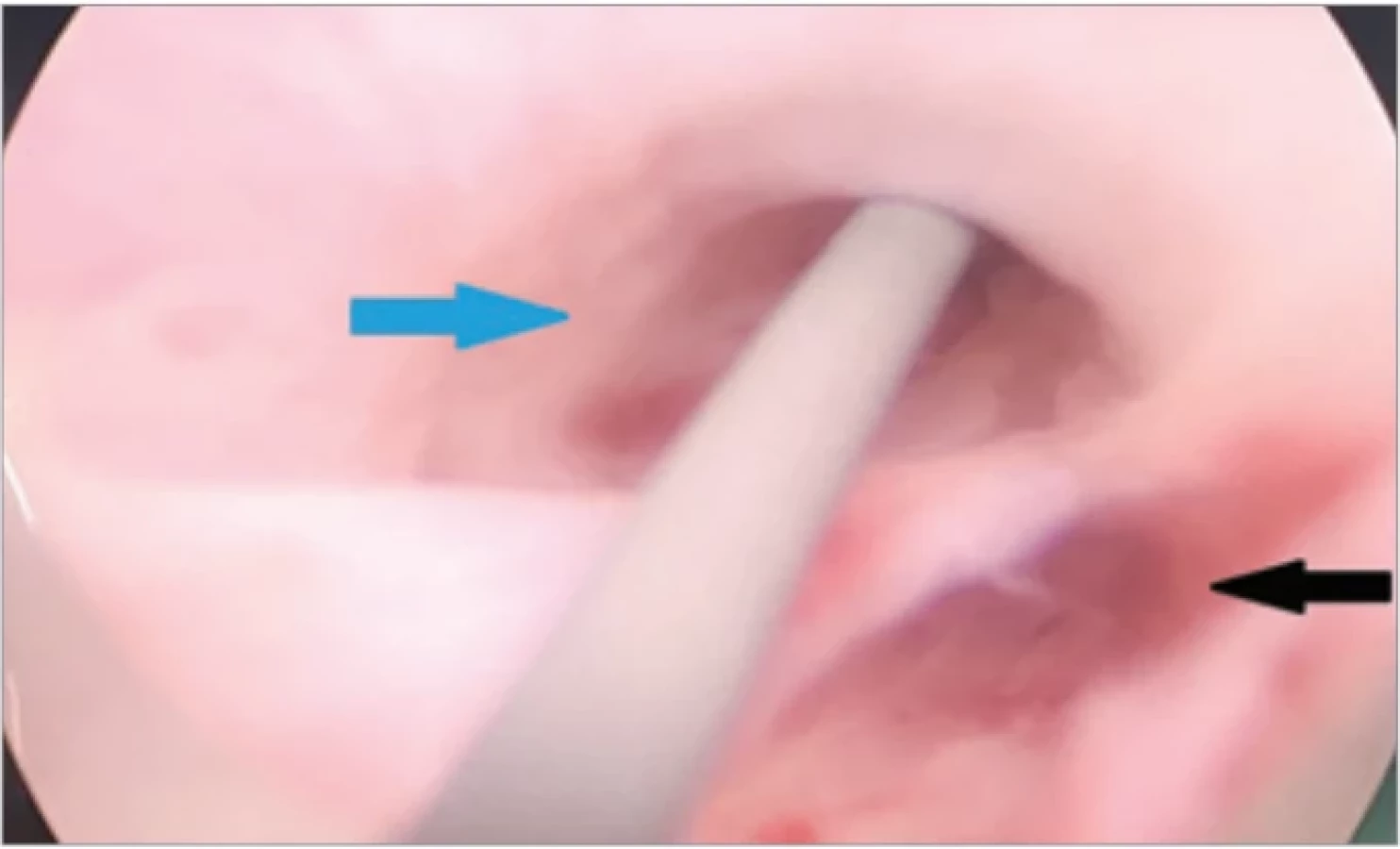
A 46-year-old man with well differentiated squamous cell carcinoma of the scalp was taken up in operation theater for resection and reconstruction. As patient was being prepped, the nursing officer tried to put a 16 Fr Foley’s urinary catheter. After failing to pass it through, attempts were made to pass with 14 Fr and 12 Fr catheters, but without success. At this point surgical teams were informed and on inspection, blood was seen at the tip of the meatus as well as along the length of the catheter introduced. A call was given to the urologist who came promptly. Upon doing urethroscopy, a large false passage almost the same caliber of the urethra was found (Fig. 1). No existing strictures were found. Under urethroscopic guidance, a guide wire was passed and catheterization was completed with 16 Fr silicone triple lumen catheter. On the advice of the urologist, the catheter was kept for 2 weeks and subsequently was removed without any complication.
Iatrogenic urethral injury is not uncommon. In male patients, it is as high as 13.4 per 1000 patients [1]. It is especially common in patients needing intermittent catheterization due to some spinal injury or bladder obstruction surgeries and in patients with pre-existing strictures [2]. Urethral false passage by the catheter tip is only second to urethral injury due to balloon inflation within the urethra when it comes to injuries caused by urinary catheterisation [1]. Despite being a well-known and well talked about entity, the incidence of such injuries does not show any decreasing trend. This underlines the significance of awareness and low threshold to do a urethroscopy for early diagnosis and management. Sotolongo and Gribetz reported a case of large caliber urethral false passage occurring after routine catheterization for an abdominoperineal resection surgery where the false passage was so large that it was mistaken for the distal urethra and required multiple investigations and prolonged management [3]. Gupta et al. reported a similar case where retrograde urethrography revealed two similar caliber distal urethra like structures and it was possible to identify the true urethra only by urethroscopy [4]. Generally, a urinary catheter kept as a temporary stent works well and is an excellent first line of management. However, some patients refuse prolonged catheterization as it hampers with sexual function. In them temporary urethral stenting maybe a viable option [5].
Learning points
- Even a seemingly common procedure in the operation theater like the urethral catheterization can have significant complication.
- False passage can occur even without pre-existing strictures due to improper technique of catheterization.
- Availability of a urologist and prompt urethroscopy can detect complications like urethral false passage early and aid in early intervention.
- Instead of persisting with attempts and reattempts that might increase the extent of injury, it is always better to seek help early.
Acknowledgement
Dr. Ashok Puranik (HOD, Surgical Disciplines & Executive Director, AIIMS-Guwahati) for advice and guidance. All operation room staff for support during the procedure.
Conflict of interest: none
Funding: none
Disclosure: All procedures performed in this study involving human participants were in accordance with ethical standards of the institutional and/or national research committee and with the Helsinki declaration and its later amendments or comparable ethical standards.
Sources
1. Davis NF., Bhatt NR., MacCraith E., et al. Long-term outcomes of urethral catheterisation injuries: a prospective multi-institutional study. World J Urol. 2020, 38 (2): 473–480.
2. Koleilat N., Sidi AA., Gonzalez R. Urethral false passage as a complication of intermittent catheterization. J Urol. 1989, 142 (5): 1216–1217
3. Sotolongo JR., Gribetz ME. Large caliber urethral false passage after catheterization: a case report. J Urol. 1982, 128 (4): 819–820.
4. Gupta KK., Pandey S., Mehdi S., et al. Case of wide calibre false urethral passage in a patient of urethral stricture. BMJ Case Rep. 2019, 12 (3): e229362.
5. Gökalp A., Yildirim I., Aydur E., et al. How to manage acute urethral false passage due to intermittent catheterization in spinal cord injured patients who refused insertion of an indwelling catheter. J Urol. 2003, 169 (1) : 203 – 206.
Ass. Prof. Moumita De
Department of Plastic, Reconstructive & Burns surgery
All India Institute of Medical Sciences, Guwahati
Assam, India - 781101
drmoumitade@gmail.com
Submitted: 14. 4. 2025
Accepted: 2. 12. 2025
Labels
Plastic surgery Orthopaedics Burns medicine TraumatologyArticle was published in
Acta chirurgiae plasticae

2025 Issue 4
Most read in this issue
- Treatment and outcomes of rectus diastasis in post-bariatric patients and postpartum women – a systematic review
- Anterior approach to posterior auricular artery in microvascular anastomosis – a new concept in replanting amputated ears – experience from four successful cases and literature review
- Association between the maxillofacial injury severity score to helmet types, neutrophil lymphocyte ratio and length of stay
- Post-otoplasty keloid scars – treatment strategies and case reports