
Surgical site infection after breast reconstruction with silicone implant – a retrospective analysis of risk factors
Authors:
B. Englcová 1; J. Kulhánek 1; Z. Dvořák 2; D. Erhart 3
Authors‘ workplace:
Department of Plastic Surgery, Na Františku Hospital, Prague, Czech Republic
1; Department of Plastic and Aesthetic Surgery, Faculty of Medicine, Masaryk University, and St. Anne’s University Hospital, Brno, Czech Republic
2; Department of Surgery, Na Františku Hospital, Prague, Czech Republic
3
Published in:
ACTA CHIRURGIAE PLASTICAE, 67, 3, 2025, pp. 172-179
doi:
https://doi.org/10.48095/ccachp2025172
Introduction
Breast reconstruction using a silicone implant is a common and most frequently preferred method of breast reconstruction following mastectomy. It constitutes an integral part of multidisciplinary oncological care and has a significant impact on the patient’s quality of life. This technique often yields satisfactory aesthetic outcomes and can be performed in two forms – immediate (carried out at the time of mastectomy) and delayed (performed at a later interval following mastectomy) [1,2]. One of the main advantages of implant-based breast reconstruction is the relatively short recovery time. However, this method is not without complications, the most common and serious of which is infection. Infection may lead to reconstruction failure and necessitate explantation of the implant. Such outcomes can result in considerable psychological and physical distress for the patient. The reported incidence of infection following silicone implant-based breast reconstruction ranges from 5% to 35%, depending on a variety of factors, including the type of reconstruction chosen (immediate vs. delayed) [3–7]. Recently, immediate reconstruction has gained popularity and is more frequently approved by oncologists than in the past. Although immediate reconstruction has a positive impact on the patient’s psychological well-being by preserving body image, it is associated with a higher rate of complications – especially infections, which may necessitate repeated surgical interventions [8,9]. Delayed reconstruction is planned several months to years after primary treatment. It is associated with a lower complication rate and allows for better and more efficient preoperative planning. However, the disadvantage lies in the increased psychological distress on the patient [10].
The most frequent risk factors include smoking, diabetes mellitus, and radiotherapy. Another potential risk factor is coagulopathy, which may impair perioperative haemostasis and thus contribute to an increased rate of reoperations and prolonged hospital stay. Attention has also begun to focus on preventive strategies, among which the most commonly employed is lipotransfer, which is performed prior to implant-based reconstruction. This technique improves tissue quality and reduces fibrosis, thereby influencing the incidence of subsequent complications [11–13,14].
Lipotransfer (lipofilling/fat transfer) has, over the past decade, become established as a valuable tool in breast reconstruction, both as a standalone procedure and as an adjunct to implant-based reconstruction. Its principal benefit lies not only in improving the aesthetic outcome but also in the regenerative potential of the transferred adipose tissue. Fat grafts contain adipose-derived stem cells and growth factors that promote angiogenesis, extracellular matrix remodelling, and the regeneration of damaged tissue, particularly in irradiated areas [11,12,15]. This effect has also been supported by meta-analyses, which have shown that lipofilling contributes to improved skin elasticity, a reduced incidence of capsular contracture, and potentially a lower rate of infectious complications [16,17]. In appropriately selected cases, pre-implant fat transfer is therefore recommended, especially in patients with fibrotic or irradiated chest walls.
In the past two years, there has been a marked increase in the use of microtextured polyurethane-covered implants, which currently account for approximately 36% of all implant-based breast reconstructions. These implants were developed with the aim of reducing the incidence of capsular contracture and other associated complications. Due to their sponge-like surface, polyurethane--coated implants promote an irregular organisation of collagen fibres within the capsule, which has been associated with a lower rate of capsular contracture and infection in both the medium and long-term postoperative periods. However, once the polyurethane coating degrades, the risk of such complications may increase to levels comparable with other implant types. Long-term studies with follow-up periods of up to 30 years have confirmed the safety and aesthetic advantages of these implants. In recent years, their use has increased globally, particularly in patients considered to be at higher risk of complications. Some studies have reported a reduced incidence of seroma formation and infection, suggesting that polyurethane implants may offer promising approach to reducing complication rates in implant--based breast reconstruction [18–20].
The aim of this study was to analyse the incidence of infections following implant-based breast reconstruction in a cohort of patients treated at Na Františku Hospital, and to compare the findings with data available in the current literature. The study further evaluated the influence of individual risk factors on infection development, provided an overview of preventive strategies, and assessed the potential protective effect of fat transfer in implant-based breast reconstruction.
Material and methods
Breast reconstruction using silicone implants requires a standardized protocol to minimize the risk of complications, particularly infections. At Na Františku Hospital, the following algorithm is consistently applied with regard to patient selection, antibiotic prophylaxis, drain management, wound care, and postoperative follow-up.
Patient selection
Delayed breast reconstruction is indicated in oncologically stable patients following mastectomy, who must present documented remission confirmed by their oncologist. Immediate reconstruction in patients with carcinoma is determined by the Breast Cancer Multidisciplinary Team at Na Františku Hospital, which includes oncologists, radiologists, pathologists, general surgeons, and plastic surgeons. In genetically high-risk patients, the decision to proceed with immediate reconstruction is made by the treating oncologist.
Assessment of risk factors is an essential part of preoperative evaluation and includes previous radiotherapy, smoking, diabetes mellitus, and coagulopathy. In selected high-risk patients, pre--implant fat transfer is considered to improve tissue quality. Fat transfer is also used in patients with minimal subcutaneous tissue in the planned reconstruction site.
Patients are advised to cease the use of tobacco products, including electronic cigarettes, for a minimum of four weeks before and after surgery to minimize the risk of complications. This recommendation is consistent with guidelines issued by the American Society of Plastic Surgeons [21].
Antibiotic prophylaxis and sterility
Preoperative antibiotic prophylaxis includes a single intravenous dose of Azepo® 2 g (Cefazolinum natricum, MEDOCHEMIE, Cyprus), administered 30–60 minutes prior to incision. In patients with known allergy, Clindamycin® 600–900 mg i.v. (Clindamycini hydrochloridum, Pfizer, USA) is administered. Postoperatively, patients receive Zinnat® 500 mg orally (Cefuroximum axetili, GlaxoSmithKline, UK), or another suitable cephalosporin antibiotic, for five days or until drain removal. In case of allergy, Dalacin® 600 mg orally (Clindamycini hydrochloridum, Pfizer, USA) is indicated.
All implantations were performed under strict sterile conditions. The surgical field was disinfected with alcohol-based antiseptic and appropriately draped. Implantation began with instrument re-disinfection, glove change, irrigation of the mastectomy pocket with povidone-iodine solution, and injection of the same solution into the implant container before opening. During implant handling, the “no-touch” technique was employed.
Drain placement
One or two Redon drains were inserted in the implant region. In cases where the implant was placed in a submuscular pocket with complete muscle coverage, one drain was positioned adjacent to the implant and a second one within the subcutaneous layer. Drains were typically removed when the 24-hour drainage output fell below 30 mL, usually between postoperative days 6 and 10. In patients with a higher risk of seroma formation or a history of radiotherapy, drains were retained for a longer period until adequate reduction of fluid output was achieved.
Wound care and hygiene
Postoperative wounds were dressed with a sterile elastic surgical tape, which remained in place for at least 7 days. In high-risk patients, particularly those following radiotherapy, a negative-pressure wound therapy system (Prevena®) was applied for 4–7 days, or alternatively, Opsite Post-Op Visible® for 7–10 days. All wounds were assessed daily for signs of infection, dehiscence, or delayed healing.
Following hospital discharge, patients were routinely monitored in the outpatient clinic. The first follow-up was typically scheduled for day 3 or 4 post-discharge, with subsequent visits at one and two weeks, and further reviews depending on clinical progress. Patients were instructed to present to the emergency plastic surgery outpatient clinic immediately in case of any signs of complications.
Patient cohort description
A retrospective observational analysis was conducted to evaluate the incidence of infectious complications following breast reconstruction with silicone implants. In 2024, micropolyurethane-coated implants were newly introduced to the national reimbursement system. A total of 25 female patients who underwent implant-based breast reconstruction at the Department of Plastic Surgery, Na Františku Hospital, during 2024, were included in the study. The distal tip of each Redon drain was sent for culture immediately after removal for microbiological examination. Only patients with microbiological sampling performed were included. Eight patients were excluded due to missing drain samples, most commonly due to discharge on a weekend when sample collection could not be verified by the operating surgeon and the on-call physician lacked proper training. Eligible patients were aged between 37 and 60 years and had undergone either unilateral or bilateral mastectomy. The cohort included women diagnosed with breast carcinoma or carcinoma in situ, who were indicated by the institutional Breast Cancer Multidisciplinary Team for skin-sparing mastectomy with immediate reconstruction.
Follow-up and monitored variables
The analysed variables included patient age, type of reconstruction (immediate vs. delayed, or re-reconstruction), occurrence of infection, length of hospital stay, presence of risk factors (smoking, diabetes mellitus, radiotherapy, and coagulopathy), whether fat transfer was performed prior to implant reconstruction, the need for reoperation or implant explantation, and overall duration of hospitalization. Infections were categorized as superficial (requiring antibiotic treatment without surgical intervention) or deep (resulting in implant explantation). All data were extracted from the hospital information system and recorded in a standardized Excel spreadsheet for subsequent analysis.
Statistical analysis
Descriptive statistical analysis was performed to evaluate the dataset. Proportional and mean values were assessed across selected subgroups. The results were subsequently compared with data published in the scientific literature from 2005 to the present.
Results
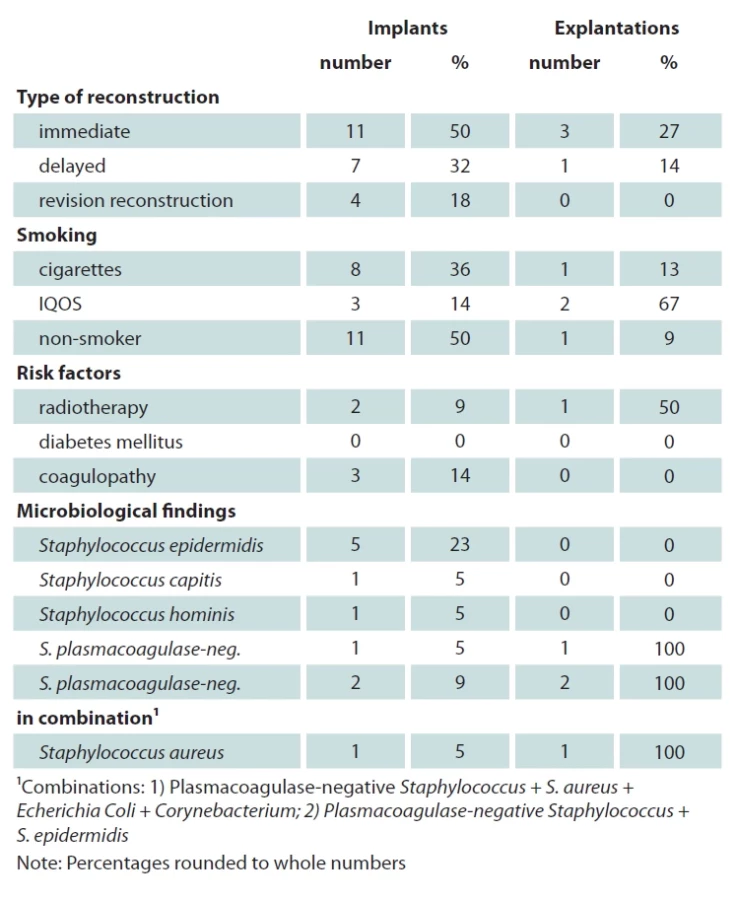
The retrospective analysis included 25 female patients who underwent implant-based breast reconstruction at the Department of Plastic Surgery, Na Františku Hospital, during the year 2024. Eight patients were excluded due to the absence of microbiological sampling from the drainage tip. In the final cohort of 17 patients, a total of 22 silicone breast implants were inserted, with five patients undergoing bilateral reconstruction. Three reconstructions were performed using micropolyurethane--coated implants – one bilaterally and one unilaterally. One of these polyurethane implants required explantation due to a late-onset infection following necrectomy in a patient with a history of radiotherapy and active use of heated tobacco products – IQOS (Tab. 1).
The median length of hospitalization was 9 days (range: 4–34 days), with extended stays observed in patients requiring reoperation or presenting with significant comorbidities or infection. The standard deviation was 7.1 days. One patient required three reoperations due to complications.
The types of reconstruction performed included delayed (N = 4), secondary (revision) reconstruction (N = 4), and immediate reconstruction (N = 9). A total of 5 patients (41.2%) required reoperation, of whom three underwent implant removal. Four of these 5 reoperated cases (80%) had undergone immediate reconstruction. Two reoperations were performed due to oncologically positive surgical margins, one due to postoperative haemorrhage, and two due to progressive necrosis and wound dehiscence.
Infectious complications occurred in 7 out of 17 patients (23.5%). The most commonly isolated pathogens included Staphylococcus epidermidis, Staphylococcus capitis, and coagulase-negative staphylococci. Most infections occurred within 30 days postoperatively. A single patient developed a late infection 3 months after surgery caused by Staphylococcus aureus, which necessitated implant removal. Four patients required explantation due to deep infection, while the remaining three cases were classified as superficial infections and managed successfully with antibiotic therapy.
Radiotherapy was identified as a major risk factor. In this cohort, two patients (11.8%) had a history of radiotherapy. One of them developed an infectious complication despite having undergone two prior fat grafting procedures. This patient ultimately required implant explantation after multiple revisions (Fig. 1).
Smoking was another notable risk factor. Nine patients (52.9%) reported current or recent smoking – seven smoked cigarettes and two used heated tobacco products (IQOS). A positive microbiological culture was found in 6 of these 9 cases (66.7%). Three patients (two using IQOS and one smoking cigarettes) developed infectious complications that led to implant removal. In one of the patients who smoked IQOS, repeated necrectomy had to be performed prior to implant removal (Fig. 2, 3). The definitive reconstruction using a TRAM flap was carried out at another institution (Fig. 4). Smoking status was not documented in two cases. Among the smokers, four of them reported consumption of 15 or more cigarettes daily, one smoked five per day, and two were occasional smokers.
Diabetes mellitus, a frequently cited risk factor in the literature, was not present in any of the patients in this cohort. One patient reported a history of hyperglycaemia; her microbiological culture yielded Staphylococcus epidermidis.
Two patients in our cohort had a documented MTHFR gene mutation, and one had a diagnosed hypercoagulable state. Although none of these patients required surgical revision, all had positive microbiological cultures.
In total, 4 implants out of 22 reconstructed breasts were explanted (18.2%). Only one patient whose implant was removed had no identifiable risk factors. Her medical history included only gestational diabetes, with normoglycemia recorded during the perioperative period.
Autologous fat grafting (lipotransfer) appeared to be a potential protective factor, though its effect should be verified in a larger sample. Lipotransfer was performed in 4 patients with known risk factors. One underwent delayed reconstruction, and three had secondary (revision) procedures. Only one of these patients developed an infectious complication, which occurred after initial revision surgery requiring necrosectomy. The primary microbiological culture from the drain tip was negative in this case.




Discussion
The results of our study confirm that implant-associated infections following breast reconstruction represent a significant complication closely associated with several well-established risk factors. The observed infection rate of 23.5% in our cohort is consistent with published reports indicating an incidence of 5–35%, depending on surgical technique, implant material, presence of risk factors, institutional experience, and postoperative care protocols [3,4,7,9,22]. The most commonly isolated pathogens were Staphylococcus epidermidis, S. hominis, and S. capitis. These are components of normal skin flora but can act as opportunistic pathogens, especially in the presence of foreign bodies. Coagulase--negative staphylococci (CoNS) are frequently identified as causative agents of late-onset implant-related infections, whereas Staphylococcus aureus tends to be associated with early infections and is known for a more aggressive clinical course [23,24]. In our sample, however, this temporal pattern was reversed: patients with CoNS developed early infections, while S. aureus was isolated in a case of delayed infection occurring three months postoperatively.
The duration of hospitalisation at Na Františku Hospital following implant-based breast reconstruction ranged from 4 to 34 days, which is longer than the hospital stays reported in some studies, typically ranging from 3 to 5 days [3,25]. This deviation may be attributed to a heightened emphasis on patient safety and strict adherence to discharge criteria, including drain output below 30 mL in 24 hours. Timely diagnostics, microbiological analysis, and appropriate antibiotic therapy are key to reducing complication rates and shortening hospital stays [26,27].
Preoperative chest wall radiotherapy was documented in 11.8% of patients in our study. One developed an infectious complication, and both had prolonged wound healing. These findings are consistent with the work of Kruger et al. [6] and Cordeiro et al. [4], who highlight the significantly increased risk of infection and reconstructive failure in patients with prior irradiation. Linear data suggest that previous radiotherapy increases the likelihood of infection, wound dehiscence, and capsular contracture by up to 2.7fold [23,28]. Radiotherapy impairs tissue perfusion, alters the microenvironment, and compromises the immune response [29,30].
Active smoking was documented in 52.9% of patients in our cohort. Consistent with previous studies [31,32], we found that smokers had a significantly higher risk of postoperative complications, including infections, wound dehiscence, and delayed healing. Nicotine and combustion by-products negatively affect microcirculation and skin reparative capacity. In both patients (three implants in total, including one case of bilateral reconstruction) who reported IQOS smoking, infectious complications developed, and implant removal was subsequently required in both cases (in the bilateral case, the explantation concerned the irradiated side). Although specific data on IQOS use are currently lacking, it is reasonable to assume that the use of any tobacco product may adversely affect the outcomes of breast reconstruction. While our sample size is limited, the 100% complication rate among IQOS users suggests a need for further research on this topic in a larger patient population.
None of our patients were diagnosed with diabetes mellitus. However, both diabetes and perioperative hyperglycaemia may impair leukocyte function, promote biofilm formation, and hinder angiogenesis, resulting in poor wound healing. The biofilm structure substantially reduces the efficacy of antibiotic treatment, often necessitating explantation [33,34]. A study by Rosen et al. [35] also confirms the association between diabetes and infectious complications, attributing it to impaired phagocytosis and angiogenesis.
All three patients in our cohort with coagulation disorders had positive microbiological cultures. According to the literature, coagulation abnormalities can lead to either excessive bleeding or increased thrombus formation, potentially resulting in secondary infections or wound dehiscence [36]. Some studies have identified postoperative haematoma as an independent risk factor for infection after breast reconstruction. Additionally, patients on anticoagulant therapy require meticulous perioperative planning, as inappropriate discontinuation or inadequate management may lead to serious complications. Although the incidence of coagulation disorders in our study was low, we recommend including coagulation screening in preoperative evaluation and coordinating care with a haematologist when necessary [14,37].
An interesting finding in our study was the possible protective effect of autologous fat transfer (lipotransfer) prior to implant-based breast reconstruction. Although performed in only four patients, none initially developed infectious complications. The literature suggests that lipotransfer enhances the quality of irradiated tissue, supports angiogenesis, and reduces fibrosis, thereby lowering the risk of capsular contracture and infection [11–13]. Yoshimura et al. [13] also highlight the regenerative potential of adipose-derived stem cells. Our results are consistent with international findings and support the importance of thorough preoperative risk assessment. Despite the limited number of patients, lipotransfer appears to have potential as a preventive measure in high-risk patients.
This study is limited by the small sample size and further constrained by the exclusion of 8 patients for whom drain tip cultures were not obtained. Nevertheless, the findings underscore the importance of preoperative optimisation, selection of appropriate reconstructive techniques, and comprehensive patient counselling on potential risks. Published data also support our conclusion that successful outcomes rely on detailed patient preparation and risk stratification.
A similar preoperative antibiotic protocol is described by Phillips et al. Although common in several European countries, the optimal duration of antibiotic prophylaxis remains a topic of ongoing debate. Some studies recommend short-term prophylaxis (less than 24 hours), citing increasing antimicrobial resistance and a lack of strong evidence supporting extended therapy [38,39]. According to Phillips et al., prolonged prophylaxis does not reduce infection rates [38,39]. However, other authors advocate for extended antibiotic coverage in high-risk patients or institutions with elevated rates of early postoperative infections [24]. Current recommendations by the American Society of Plastic Surgeons limit prophylactic antibiotic use to 24 hours unless there is a clear indication for continuation [21]. Our findings support an individualised approach to antibiotic prophylaxis based on each patient’s risk profile rather than a universal protocol.
Our drain management protocol is similar to that described by Lee et al. [40], though with a longer average duration of drainage. The author removes drains when output is less than 30 mL in 24 hours for two consecutive days.
Conclusion
Our retrospective analysis revealed an infection rate of 23.5% following implant-based breast reconstruction, with smoking – especially in combination with other risk factors – emerging as the most significant contributor. The most severe case of impaired healing occurred in a patient with a history of radiotherapy who also smoked IQOS. These findings align with recent studies indicating that these factors substantially impair healing and immune response.
Immediate reconstruction itself may also represent a risk factor. Three out of four explantations occurred in patients who underwent immediate reconstruction. For patients presenting with multiple risk factors, a two-stage or even multi-stage approach – including pre-reconstruction fat transfer – should be considered. The success of immediate reconstruction relies heavily on careful patient selection, elimination of modifiable risk factors, and an adapted surgical approach.
In addition to smoking, radiotherapy, and diabetes mellitus, our findings suggest that coagulation disorders constitute an important yet underreported risk factor in the literature.
Preoperative optimisation, appropriate antibiotic prophylaxis, adequate drainage, and most importantly an individualised approach to high-risk patients form the cornerstone of prevention.
Fat transfer performed prior to implant placement may offer a protective effect, as suggested by both our data and recent literature. Among the four patients who received lipofilling, only one experienced an infectious complication, and this occurred after a secondary procedure involving necrosectomy. The initial cultures were negative. Although our study is limited by its retrospective design and small sample size, the data clearly emphasise the importance of a personalised approach in reconstructive planning. Optimising glycaemic control, encouraging smoking cessation, and considering pre-reconstruction fat transfer in high-risk patients may help reduce complications and improve outcomes.
Multidisciplinary collaboration among surgeons, plastic surgeons, radiation oncologists, and oncologists is crucial to ensure favourable long-term results. For high-risk patients, a two-stage reconstruction should be recommended.
Future directions include a prospective multicentre study to confirm the protective potential of fat transfer and validate our findings in a larger cohort. Further investigation into the impact of IQOS smoking on reconstructive outcomes is also warranted. Additionally, the standardisation of diagnostic and therapeutic protocols and the assessment of long-term patient satisfaction and quality of life following reconstruction should be considered.
Disclosure
The authors have no conflicts of interest to disclose. The authors declare that this study has received no financial support. All procedures performed in this study involving human participants were in accordance with ethical standards of the institutional and/or national research committee and with the Helsinki declaration and its later amendments or comparable ethical standards.
Roles of authors
B. Englcová and J. Kulhánek conducted the literature search, designed the flowchart and analysed the collected data. Z. Dvořák wrote the manuscript with the input from all authors. D. Erhart conceived the study and revised it critically for important intellectual content. All the authors approved the version to be published.
Sources
1. Song DH., Kim H., Jung H., et al. Postoperative complication rates and patient satisfaction following direct-to-implant breast reconstruction: a prospective study. Ann Plast Surg. 2014, 72 (3): 296–301.
2. Cordeiro PG., McCarthy CM. A single surgeon’s 12-year experience with tissue expander/implant breast reconstruction: part I. A prospective analysis of early complications. Plast Reconstr Surg. 2006, 118 (4): 825–831.
3. McCarthy CM., Mehrara BJ. Complications in postmastectomy breast reconstruction using expanders and implants. Plast Reconstr Surg. 2008, 121 (1): 1–6.
4. Cordeiro PG., Pusic AL., Disa JJ., et al. Irradiation after immediate tissue expander/implant breast reconstruction: outcomes, complications, aesthetic results, and satisfaction among 156 patients. Plast Reconstr Surg. 2004, 113 (3): 877–881.
5. Spear SL, Onyewu C. Staged breast reconstruction with saline-filled implants in the irradiated breast: recent trends and therapeutic implications. Plast Reconstr Surg. 2000, 105 (3): 930–942.
6. Krueger EA., Wilkins EG., Strawderman M., et al. Complications and patient satisfaction following expander/implant breast reconstruction with and without radiotherapy. Int J Radiat Oncol Biol Phys. 2001, 49 (3): 713–721.
7. Pittet B., Montandon D., Pittet D. Infection in breast implants. Lancet Infect Dis. 2005, 5 (3): 94–106.
8. Kronowitz SJ. Immediate versus delayed reconstruction in the setting of postmastectomy radiation: a meta-analysis. Ann Plast Surg. 2016, 76 (2): 219–224.
9. Lee KT. Risk factors for surgical site infection after breast reconstruction surgery. J Plast Reconstr Aesthet Surg. 2020, 73 (3): 573–581.
10. Dietz JR. Risk factors for surgical site infection after breast surgery. Breast J. 2019, 25 (3): 401–406.
11. Choi M. Autologous fat grafting and tissue regeneration. Gland Surg. 2017, 6 (1): 9–24.
12. Tiron EA. Role of lipofilling in breast reconstructive surgery. J Clin Med. 2019, 8 (10): 1532.
13. Yoshimura K., Sato K., Aoi N., et al. Cell-assisted lipotransfer for cosmetic breast augmentation: supportive use of adipose-derived stem/stromal cells. Aesthetic Plast Surg. 2008, 32 (1): 48–55.
14. Davison SP. Complications of implant-based reconstruction after mastectomy. Ann Plast Surg. 2008, 60 (3): 246–250.
15. Delay E. Fat injection to the breast: technique, results, and complications. Ann Chir Plast Esthet. 2009, 54 (6): 534–543.
16. Tiron EA., Bruce S., Atisha DM. Fat grafting in breast reconstruction: a literature review of technique, outcomes, and applications. Ann Plast Surg. 2019, 83 (6): 713–721.
17. Choi M., Small K., Levovitz C., et al. The use of autologous fat grafting for breast reconstruction: a systematic review with meta-analysis. J Plast Reconstr Aesthet Surg. 2013, 66 (12): 1642–1653.
18. Sforza M., Hammond DC., Botti G., et al. A 14-year experience with polyurethane-covered breast implants. Aesthetic Plast Surg. 2014, 38 (2): 290–296.
19. Montemurro P., Tay V., Svanberg T., et al. One-stage breast reconstruction with polyurethane-coated implants after skin-sparing mastectomy: a prospective study of complications and outcomes. Aesthet Surg J. 2024, 44 (5): 491–499.
20. Manders EK., Keller KM. Polyurethane implants in 2-stage breast reconstruction: 9-year clinical experience. Aesthet Surg J. 2017, 37 (2): 171–178.
21. American Society of Plastic Surgeons. Clinical practice guideline: smoking cessation and plastic surgery. ASPS; 2019.
22. Chun YS., Verma K., Rosen H., et al. Implant-based breast reconstruction using acellular dermal matrix and the risk of postoperative complications. Plast Reconstr Surg. 2010, 125 (2): 429–436.
23. Olsen MA., Nickel KB., Fox IK., et al. Incidence of surgical site infection following mastectomy with and without immediate reconstruction using private insurer claims data. Infect Control Hosp Epidemiol. 2015, 36 (8): 907–914.
24. Tamboto H. Microbiology and antibiotic treatment of breast implant infections. ANZ J Surg. 2010, 80 (9): 651–656.
25. Wixtrom RN. Surgical site infections after breast surgery: a 10-year analysis. Am J Surg. 2014, 208 (5): 846–852.
26. Tanna N. Understanding and managing infection after implant-based breast reconstruction. Gland Surg. 2017, 6 (2): 194–202.
27. Rosen H., Lester ME., Wenke JC., et al. Predictors of complications in immediate breast reconstruction. Am J Surg. 2017, 214 (4): 671–675.
28. Lin KY. Risk factors for wound complications in immediate breast reconstruction. Plast Reconstr Surg. 2011, 127 (3): 1080–1087.
29. Krueger EA., Wilkins EG., Strawderman M., et al. The impact of radiation on complications in expander-implant breast reconstruction. Int J Radiat Oncol Biol Phys. 2020, 106 (1): 109–116.
30. Santosa KB., et al. Postmastectomy radiation therapy and breast reconstruction: a literature review and meta-analysis. Plast Reconstr Surg. 2016, 138 (1): 1–10.
31. Song DH., McCarthy CM., Young VL., et al. The effect of smoking on reconstructive complications. Ann Plast Surg. 2014, 72 (1): 56–60.
32. Spear SL., Ducic I., Cuoco F., et al. The effect of smoking on flap and implant-based breast reconstruction. Plast Reconstr Surg. 2010, 125 (1): 25–30.
33. Fischer JP. Diabetes and complications in breast reconstruction. Plast Reconstr Surg. 2013, 131 (6): 1119–1127.
34. Gdalevitch P. Diabetes as a predictive factor for complications in breast reconstruction. J Plast Reconstr Aesthet Surg. 2012, 65 (3): 362–366.
35. Rosen H., Krishnan NM. Diabetes and infection risk in implant-based breast reconstruction: a comprehensive review. J Plast Reconstr Aesthet Surg. 2017, 70 (5): 678–685.
36. Omranipour R. Complications of breast implant surgery in patients receiving antithrombotic therapy. Eur J Plast Surg. 2015, 38 : 175–180.
37. Kitzinger HB. Perioperative management of antithrombotic therapy in plastic surgery: a review of the literature. J Plast Reconstr Aesthet Surg. 2015, 68 (4): 421–428.
38. Phillips BT., Fourman MS., Bishawi M., et al. Are prophylactic postoperative antibiotics necessary for immediate breast reconstruction? Results of a prospective randomized clinical trial. J Am Coll Surg. 2016, 222 (6): 1116–1124.
39. Phillips BT., Halvorson EG., Khan SU., et al. Clinical practice guideline: breast reconstruction with expanders and implants. Plast Reconstr Surg. 2016, 138 (3): 585–594.
40. Lee KT., Mun GH. Updated evidence of risk factors for surgical site infections after breast reconstruction: a meta-analysis. Aesthetic Plast Surg. 2020, 44 (1): 36–44.
Barbora Englcová, MD, MSc.
Na Františku Hospital
Na Františku 847/8
110 00 Prague 1
Czech Republic
englcova@nnfp.cz
Submitted: 12. 8. 2025
Accepted: 31. 10. 2025
Labels
Plastic surgery Orthopaedics Burns medicine TraumatologyArticle was published in
Acta chirurgiae plasticae

2025 Issue 3
Most read in this issue
- Overall and area-specific tactile recovery following different methods of surgical reinnervation in post-mastectomy breast reconstruction – a systematic review and meta-analysis
- Brachymetacarpia – our experience with internal device for distraction osteogenesis in adolescent patients
- The importance of sentinel node biopsy and examination in malignant melanoma of the head and neck
- Case report of severe complications after gel injection breast augmentation – treatment and use of hemostatic net for effective management