
Overall and area-specific tactile recovery following different methods of surgical reinnervation in post-mastectomy breast reconstruction – a systematic review and meta-analysis
Authors:
R. C. Suteja 1; I. G. Prawista 1; A. Salim 1; I. K. Adiputra 1; G. V. Purnama 1; I. P. Suryanov 1; D. Junior 1; I. G. Diksha 1; S. Christian 1; G. W. Samsarga 2
Authors‘ workplace:
Faculty of Medicine, Udayana University, Bali, Indonesia
1; Plastic Reconstructive and Aesthetic Surgery Division, Department of Surgery, Faculty of Medicine, Udayana University/ Udayana University, Academic Hospital, Bali, Indonesia
2
Published in:
ACTA CHIRURGIAE PLASTICAE, 67, 3, 2025, pp. 189-202
doi:
https://doi.org/10.48095/ccachp2025189
Introduction
Breast cancer is the most prevalent type of cancer found in women. It is defined as an uncontrolled proliferation of any of the histologically heterogeneous tissues structurally forming the breast. Due to its high prevalence, breast cancer places a significant burden on both patients and the healthcare system. The American Cancer Society estimated that breast cancer accounts for up to 32% of newly diag - nosed cancers in the US in 2024 [1]. This translates to around 310 thousand new cases every year, doubling colorectal cancer, which is second on the list [1]. Treatments such as single or combined anti-cancer modalities such as radiotherapy, chemotherapy, hormonal therapy, and mastectomy are developed to decrease morbidity and mortality [2]. Although cancer-related mastectomy is a life-saving procedure, this procedure risks the ‘death’ of women from a social standpoint. Enache (2011) described the effect of mastectomy on a woman as equivalent to the loss of femininity, shapes the sense of inferiority, and prompts the feeling of embarrassment [3]. While counselling does alleviate some of this burden, breast reconstruction has always been a definitive treatment to recover the lost breast’s form and function [4–6]. This may be performed immediately or after a delay, not uncommonly years following initial mastectomy. Cosmetics may seem to be the most apparent concern during reconstruction; however, sensation recovery arguably carries a more critical role towards the increase in the patient’s quality of life. Studies reported that there is a robust correlation between breast sensation and better physical, psychosocial, and sexual wellbeing [7–9].
Recent advances in medical technology have thankfully allowed surgeons to use advanced modalities that enable microscopic reconstruction of tissues, vessels, and nerves, giving sensation to the newly reconstructed breast. Various methods of surgical reinnervation have been described in previous studies [10]. However, to the best of our knowledge, there has never been any systematic review and meta-analysis which aims to compare sensory recovery using different methods of surgical reinnervation during post-mastectomy breast reconstruction.
This study aims to measure and compare the overall and area-specific tactile recovery following different methods of surgical reinnervation following post-mastectomy breast reconstruction. Results from this study can be used as a consideration when choosing from the various methods of surgical reinnervation during post-mastectomy breast reconstruction.
Evaluation of the topic
Methods of data collection and processing
This study is a systematic review and meta-analysis written according to PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analysis) guidelines [33]. We searched online databases, which include PubMed, ClinicalTrials.gov, Scopus, and Science Direct, on 1 June 2024 for interventional studies that report tactile recovery following post-mastectomy breast reconstruction with surgical reinnervation. We only included studies written in English and published before March 2024. We excluded articles based on reasons ranked as follows:
1.
The study was not completed, and the results were not posted.
2.
The study was duplicated or is a previous version of a follow-up study derived fully/partially from the same set of patients.
3.
The study is not a peer-reviewed journal article.
4.
The study was not written in English.
5.
The study does not contain primary data.
6.
The study contains less than five subjects.
7.
The study does not report the population aimed to be observed in the study (post-mastectomy breasts).
8.
The study does not report the intervention/comparison aimed to be observed in the study (breast reconstruction with surgical reinnervation).
9.
The study does not report the outcome aimed to be observed in the study (tactile recovery).
We inserted search query results into Rayyan [11]. Two independent authors (RC and IGAMHP) manually excluded duplicated studies with the website’s assistance. Following the exclusion of duplicates, two independent authors (RC and IGAMHP) manually screened each study’s title and abstract for study eligibility. Following abstract exclusion, RC attempted to retrieve the full texts of studies eligible for full-text screening. Studies irretrievable were excluded. Two independent authors (RC and IGAMHP) manually screened each study’s full text for eligibility.
Data extracted from studies eligible for reporting and synthesis were recorded by two independent authors (RC and IGAMHP) in separate standardized Microsoft Excel® sheets. Any disagreement and uncertainty were resolved through discussion. The authors will extract data from the longest duration of follow-up when presented with paired measurements in both one article or within multiple articles (a follow-up study).
Random-effect models were used to pool effect sizes due to the assumption of considerable heterogeneity. Effect sizes were drawn from overall innervated breasts, innervated breasts classified by surgical reinnervation procedure, and all non-innervated breasts. A forest plot with a 95% confidence interval (CI) will then be drawn on the random-effects model, with analysis done to pool the overall tactile and area-specific sensory recovery. The results will be visualized on a heat map based on the outlier-adjusted pooled results. All statistical analyses were conducted using R version 2023.6.2+561. The risk of bias assessment will be conducted based on the ROBINS-I (Risk of Bias in Non-Randomized Studies of Interventions) for non-randomized studies and RoB2 (Risk of Bias 2) for randomized controlled trials and visualized using the ROBVIS tool [34]. Two independent authors (RC dan IGAMHP) assessed each study’s risk of bias.
Our literature search found 624 studies, of which 388 were from Science Direct, 109 were from PubMed, and 111 were from Scopus. Our search on ClinicalTrials.gov found 16 studies; however, 13 studies were yet to be completed. We then excluded 96 duplicate articles, 483 articles during the title and abstract screening, six articles being irretrievable, and 14 articles during full-text screening due to not meeting our eligibility criteria. During the full-text screening, three studies were excluded because they did not report the desired outcome, three were excluded because they did not perform or failed to specify intervention, two were excluded because of reporting less than five patients, two were excluded because of having a follow-up study, one was excluded because of not differentiating body part reconstructed, and one was excluded because of failing to differentiate the method of reconstruction. We were then left with twelve studies for reporting and data synthesis. PRISMA flowchart can be seen in Fig. 1.
Five studies were done in the Netherlands, four in the United States, and one each in Belgium, Japan, and Finland. These twelve studies report a total of 481 innervated breasts alongside 295 controls. Six studies used DIEP flap, three used TRAM, two used LTP, one used VRAM, one used implant, and another one did not specify what was used for the reconstruction. Specified mastectomy procedure varies from conventional, skin-sparing, and nipple-sparing up to modified radical mastectomy. The complete study profile can be seen in Tab. 1.
Of these twelve studies, nine measured the difference between breasts receiving end-to-end nerve coaptation and those receiving no surgical reinnervation. Two studies used allogeneic nerve grafts, while one used polyglycolic acid (PGA) nerve conduit. Coincidentally, these three studies employ Pressure Specified Sensory Device (PSSD) instead of Semmes-Weinstein Monofilament Test to measure tactile recovery. The other nine studies measured tactile recovery using the earlier-found Semmes-Weinstein monofilament test (SWMT). SWMT measures tactile recovery using a series of rods with a rod label size corresponding to the logarithmic value of ten times the force in milligrams required to buckle the monofilament rod [12]. Although interpolation towards pressure ‘stress’ values from point measurements described by Levin et al. can be done on the mean SWMT rod size, calculating rod size means before converting them will yield a statistically different value than converting them before calculating the means already in the pressure unit [13]. And since no study had reported individual patient data, direct comparison between studies using different measuring methods is not statistically correct and will not be done in this study. Tactile recovery results and follow-up can be seen in Tab. 2.
![PRISMA fl owchart. A total of 624 studies across four databases were screened, resulting in the inclusion and synthesis of information from twelve studies [33]. For more information, see [36].](https://pl-master.mdcdn.cz/media/cache/media_object_image_large/media/image/8646bd7d61b486c424a19f02a0279e38.png)
ofdatabasesandregistersonly



End-to-end coaptation
Pooled overall SWMT rod size in breasts with end-to-end nerve coaptation was found to be 3.96 (95% CI 2.96–4.96) with high heterogeneity (I2 94%; P < 0.01). Pooled overall SWMT rod size in breasts without surgical reinnervation was found to be 5.27 (95% CI 4.93–5.60) with high heterogeneity (I2 80%; P < 0.01). Three studies in the analysis reported a significant difference between flaps receiving end-to-end nerve coaptation compared to flaps without surgical reinnervation. Other studies which were not included in the analysis included Bijkerk et al., which reported that DIEP/LTP flaps receiving end-to-end nerve coaptation had a significantly lower (P < 0.01) median (interquartile range) SWMT rod size of 4.42 (3.67–5.13) compared to flaps not receiving surgical reinnervation at 5.06 (4.60–5.44) [12]. Bubberman et al. reported a significantly lower (P < 0.01) mean SWMT rod size of 4.48 in flaps receiving end-to-end coaptation compared to flaps not receiving surgical reinnervation at 5.20 [14]. Similar results can also be seen in Puonti et al., Mori et al., and Blondeel et al., who reported these findings using methods specified in the respective studies [15–17]. Additionally, Puonti et al. reported that dual nerve coaptation resulted in better sensory recovery [16]. Different to other studies, Spiegel et al. measured tactile sensation in breasts receiving end-to-end coaptation using PSSD. They found a mean tactile threshold of 69.78 g/mm2 [18]. Forest plot of SWMT rod size in breasts with end-to-end nerve coaptation, which can be seen in Fig. 2, while breasts without surgical reinnervation are seen in Fig. 3.
We found a pooled standardized mean difference (SMD) of −1.53 (95% CI −2.62–0.43) with high heterogeneity (I2 87.2%; P < 0.05) between breasts receiving end-to-end coaptation and breasts not receiving innervation. The forest plot for the difference can be seen in Fig. 4.





Nerve allograft
Djohan et al. and Peled et al. reported sensory recovery following surgical reinnervation using an allogeneic nerve graft [19,20] Djohan et al. found a tactile threshold of 58.55 g/mm2, while Peled et al. found that 75% of subjects included in the study had a threshold of 0–20 g/mm2 and a few (21%) at 20–40 g/mm2 [19,20] This recovery as described by Peled et al. is very notable because it brings the reconstructed breast’s sensation to levels comparable to normal, healthy breasts as reported by Djohan et al. [19,20]. This difference can be attributed to the difference in follow-up duration, where breasts in Peled et al. had a follow-up of more than 12 months, while those in Djohan et al. had a mean follow-up time of around 11 months [19,20]. The results from these two studies were unable to be analyzed due to the difference in reporting methods, and these two studies also did not employ multiple treatment arms using different methods of surgical reinnervation.
Neither of these studies indeed compares sensory recovery in the same way. We have not made any statistical inference between the footage of this study; we only reported our findings without testing for statistical significance between the two groups. Additionally, we also remind the reader to interpret these findings with caution.
Nerve conduit
Spiegel et al. was the only study that performed surgical reinnervation with the polyglycolic acid (PGA) nerve conduit [18]. The sensory threshold was then found at 49.28 g/cm2 [18]. This was notably lower than the same observation done on breasts receiving end-to-end nerve coaptation and no surgical reinnervation, albeit a much shorter follow-up time. In fact, the follow-up time for the nerve conduit was 25% less than the follow-up time for end-to-end nerve coaptation and more than 50% less than the follow-up time for breasts not receiving reinnervation.
Area specific analysis
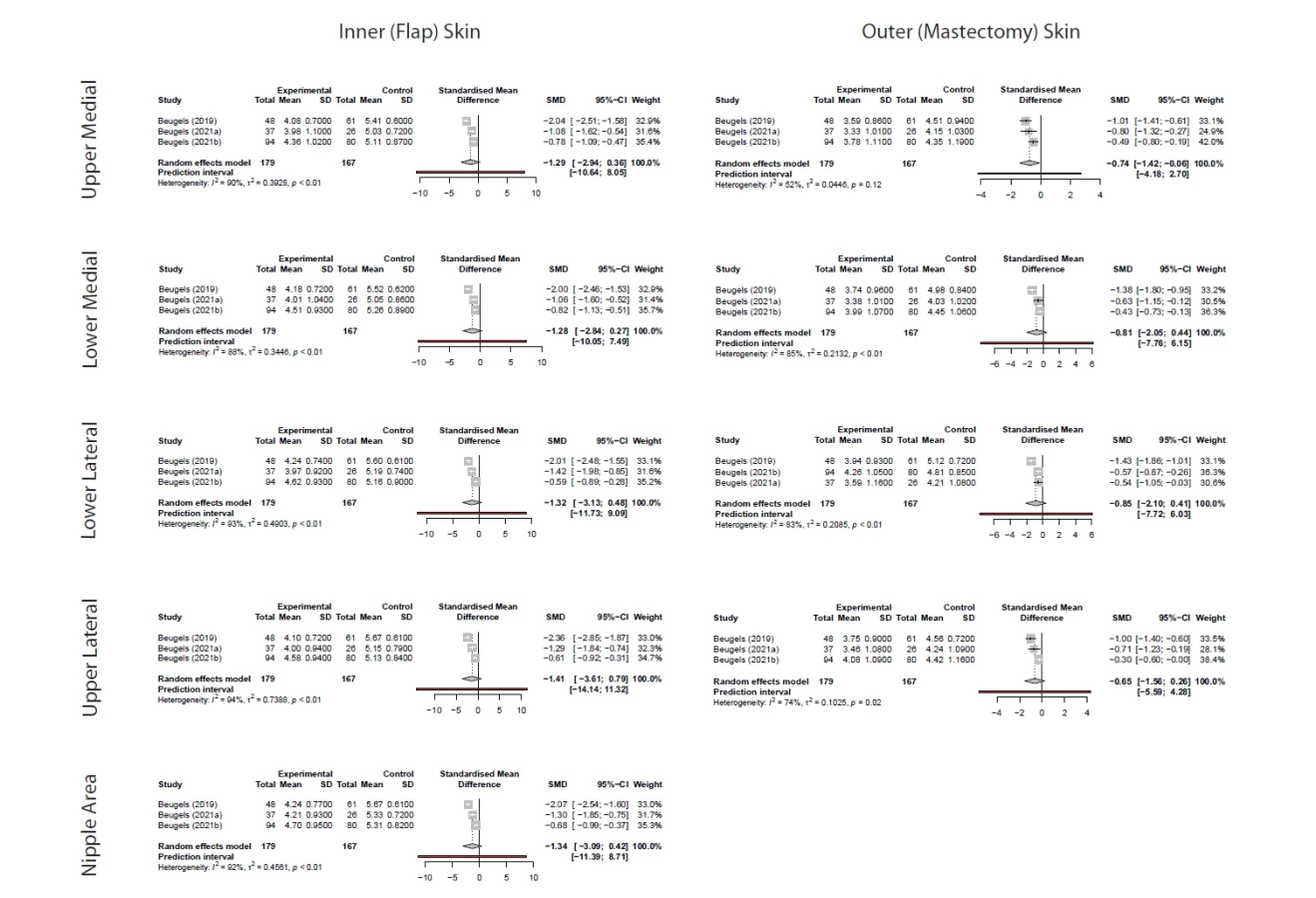
We then performed an area-specific analysis and found that the largest SWMT rod sizes were generally in the flap nipple area. Pooled mean (95% CI) of SWMT rod size following end-to-end coaptation in the flap nipple area was 4.39 (95% CI 3.70–5.09), while in those not receiving surgical reinnervation 5.45 (95% CI 4.93–5.97). Pooled mean rod sizes were generally much lower in the non-flap areas than in the reconstructed breast. We only included Beugels et al., Beugels et al., and Beugels et al. because only these studies reported area-specific sensory recovery [21–23]. Forest plot for SWMT rod size in breasts receiving end-to-end nerve coaptation towards breast receiving no surgical innervation can be seen in Fig. 5, 6.
Forest plot and details of standardized mean difference in SWMT rod size in breasts with end-to-end nerve coaptation towards breasts receiving no surgical innervation can be seen in Fig. 7 and Tab. 3.
Heat map for area-specific pooled SWMT rod size in breasts with end-to-end nerve coaptation towards breasts receiving no surgical innervation can be seen in Fig. 8.
Risk of bias
Eleven studies synthesized were analyzed using the ROBINS-I tool, while Bubberman et al. was analyzed using the RoB2 tool [14]. All non-RCT studies were deemed to have an overall moderate risk of bias, while Bubberman et al. had some concerns about its overall risk of bias [14]. Overall risk of bias can be seen in Table 4, and the risk of bias traffic light plot can be seen in Fig. 9.




Discussion
Mastectomy is a life-saving procedure, but this procedure risks the ‘death’ of women from a social standpoint. The loss of breasts implies a non-negligible psychological distress and reduction in quality of life. While counselling and psychotherapy may help in psychological recovery, reconstruction is the definitive treatment for lost breast form and function [4–6]. Studies have reported that reconstruction, especially those emphasizing sensory recovery, strongly correlates with better physical, psychosocial, and sexual well-being [7–9]. Women in these studies reported better quality of life following breast reconstruction [7–9].
Surgical reinnervation
Reinnervation is a term that describes the restoration of neurological function – both sensory and recovery – towards a body part that is lost or damaged. This can be achieved both spontaneously or via surgery, hence termed surgical reinnervation. Although chances of complete restoration of lost physiological functions following extensive diastasis between proximal and distal sites were still deemed slim to none, various surgical techniques in peripheral nerve surgery have been developed to accommodate various nerve lesions [10], Tuturov described four techniques available for tissue reinnervation, namely (i) neurorrhaphy, ii) autotransplantation, (iii) recovery using conduits, and (iv) neurotization [10]. Each set of methods was described to have its indications and contraindications.
Neurorrhaphy involves anastomosis of residual nerves in the proximal (healthy) and distal (denervated) tissues. Although nerve anastomosis may be done from end-to-end (ETE), end-to-side (ETS), and side-to-side (STS), the latter was less studied and performed [10,24]. Although anastomosis involving the sides and not the end of a nerve may not be an obvious option, recent studies on termino-lateral regeneration and sprouting of collateral nerves alongside had opened the possibility of using ETS and STS [10,24]. However, studies such as those done by Rönkkö et al. and Viterbo et al. demonstrated conflicting results of whether ETE is superior to ETS and STS; although all agreed that ETS and STS is a viable option when conserving donor nerve function as a priority [24–26].
Autotransplantation involves an ETE of nerves in the proximal and distal tissues; however, it involves a nerve donor from another part of the body covering the diastatic segment [10]. However, reports by Bibbo et al. and Bhangra et al. reported that this method had long-term complications such as the formation of neuroma in anastomotic sites, varying degrees in loss of sensitivity, and rotation to kinking of bundles of nerve fibers [27,28]. Furthermore, donor site tissues innervated by the nerve graft are prone to neurologic morbidity. Even after considering all the risks, the donor nerve’s diameters may as well not match the recipient nerve due to differences in anatomical features and function of tissues innervated by the respective nerves [10,28]. The use of conduits mimics autotransplantation but with an artificial conductor instead of a nerve donor. This eliminates the shortcomings from autotransplantation, particularly those involving donor site morbidity [10].
Neurotization involves the direct attachment of proximal nerve endings into muscle tissue [10]. This technique is used if no distal nerve can be identified, or is deemed not viable for anastomosis [10]. However, forming new neuromuscular junctions (NMJs) involves a multi-step process of morphologically transforming muscle tissues serving as the attachment site into those resembling a normal NMJ. Results following this surgery were found to be conflicting, and it is the least used surgical technique compared to those previously mentioned [10].
Surgical reinnervation during breast reconstruction
Many studies have described the reconstruction outcome with reinnervation performed on other body parts, ranging from small, particular tongue tissues to the larger, more common breast tissues [29]. The consensus is that reconstruction, which includes reinnervation, provides better sensory recovery. Most studies reported in Table 1 found a significant difference in sensory recovery between breasts in the two groups. This is confirmed by our analysis, which found an overall significant standardized mean difference in sensory recovery between breasts in the two groups, albeit only including four studies.
Published studies done on different parts of the body generally validate our findings. For example, a study by Lee et al. reported that in patients with facial nerve palsy, dual innervation of the trigeminal nerve improves the dynamic movement of paralyzed facial muscles and shortens recovery [30]. Another study by Gil et al. reported that in patients with proximal ulnar nerve injury, patients receiving end-to-side nerve coaptation demonstrated superior strength and improved upper extremity function compared to those not receiving limb reinnervation [31]. Yuan et al. reported that patients receiving finger pulp reconstruction and nerve coaptation following reconstruction using reverse digital artery island flap yielded better static two-point discrimination and overall higher sensory function grades. A meta-analysis by Hardcastle et al. reported that in patients receiving surgical reinnervation via nerve graft and nerve transfer following brachial plexus injury, reanimation of shoulders showed better, although not statistically significant, functional recovery of shoulder function [32].
While there has been an increase in the number of studies reporting sensory outcomes following end-to-end nerve coaptation, non-preliminary studies done on other forms of reinnervation (STE and STS nerve coaptation, nerve conduits, and nerve grafts) were still scarce. Further investigation is needed to elucidate the specific impact of each surgical method on sensory recovery.
Limitations
This study does not include grey literature. There has been no adequate number of studies to statistically analyze the differences in sensory recovery outcomes based on the reinnervation surgical technique.
Conclusion
In conclusion, overall sensory recovery was significantly better in breasts receiving surgical reinnervation, particularly with end-to-end coaptation compared to not receiving surgical reinnervation. This shows a promising solution to sensory recovery following mastectomy. Area-specific analysis found this difference especially significant in the upper medial portion of the mastectomy skin. Further research is needed to investigate recovery by other surgical reinnervation methods, particularly end-to-side coaptation, side-to-side coaptation, neurotization, anastomosis using conduits, and nerve grafts.
Roles of the authors
Richard Christian Suteja – conceptualization, data curation, funding acquisition, methodology, resources, software, visualization, writing original and review editing; I Gusti Ayu Maha Hiranandini Prawista – conceptualization, investigation, methodology, project administration, resources, and software; Albert Salim – formal analysis, investigation, project administration, I Komang Hotra Adiputra – data curation, funding acquisition, and writing original draft; Giovanca Verentzia Purnama – resources, writing original and review editing, I Putu Divanaya Suryanov – conceptualization, formal analysis, funding acquisition, and investigation; Darren Junior – methodology, software and validation; I Gusti Ngurah Ariestha Satya Diksha – data cuuration, investigation, resources, and software; Steven Christian – data curation, project administration, writing original and review editing; Gede Wara Samsarga – supervision, validation, and writing review editing.
Conflict of interests
The author declared no conflict of interest.
Funding
No funding was used on this study.
Sources
1. Siegel RL., Giaquinto AN., Jemal A. Cancer statistics, 2024. CA Cancer J Clin. 2024, 74 (1): 12–49.
2. Moo TA., Sanford R., Dang C., et al. Overview of breast cancer therapy. PET Clin. 2018, 13 (3): 339–354.
3. Rodica E. The relationship between anxiety, depression and self-esteem in women with breast cancer after surgery. Proc Soc Behav Sci. 2012, 33 : 124–127.
4. Fortunato L., Loreti A., Cortese G., et al. Regret and quality of life after mastectomy with or without reconstruction. Clin Breast Cancer. 2021, 21 (3): 162–169.
5. Ng SK., Hare RM., Kuang RJ., et al. Breast reconstruction post mastectomy patient satisfaction and decision making. Ann Plast Surg. 2016, 76 (6): 640–644.
6. Pirzadi L., Vakilian K., Azar FF., et al. Effect of solution-focused counseling on depression and quality of life in women under mastectomy: a randomized clinical trial. Open Public Health J. 2024, 16 (1).
7. Hammond JB., Kandi LA., Armstrong VL., et al. Long-term breast and nipple sensation after nipple-sparing mastectomy with implant reconstruction: relevance to physical, psychosocial, and sexual well-being. J Plast Reconstr Aesthetic Surg. 2022, 75 (9): 2914–2919.
8. Wei CH., Scott AM., Price AN., et al. Psychosocial and sexual well-being following nipple-sparing mastectomy and reconstruction. Breast J. 2016, 22 (1): 10–17.
9. Bykowski MR., Emelife PI., Emelife NN., et al. Nipple–areola complex reconstruction improves psychosocial and sexual well-being in women treated for breast cancer. J Plast Reconstr Aesthetic Surg. 2017, 70 (2): 209–214.
10. Tuturov AO. The role of peripheral nerve surgery in a tissue reinnervation. Chin Neurosurg J. 2019, 5 : 5.
11. Rayyan: AI-powered systematic review management platform. 2025 [online]. Available from: www.rayyan.ai.
12. Bijkerk E., van Kuijk SMJ., Lataster A., et al. Breast sensibility in bilateral autologous breast reconstruction with unilateral sensory nerve coaptation. Breast Cancer Res Treat. 2020, 181 (3): 599–610.
13. Levin S., Pearsall G., Ruderman RJ. Von Frey’s method of measuring pressure sensibility in the hand: an engineering analysis of the Weinstein-Semmes pressure aesthesiometer. J Hand Surg Am. 1978, 3 (3): 211–216.
14. Bubberman JM., Brandts L., van Kuijk SMJ., et al. The efficacy of sensory nerve coaptation in DIEP flap breast reconstruction – preliminary results of a double-blind randomized controlled trial. Breast. 2024, 74 : 103691.
15. Mori H., Okazaki M. Is the sensitivity of skin-sparing mastectomy or nipple-sparing mastectomy superior to conventional mastectomy with innervated flap? Microsurgery. 2011, 31 (6): 428–433.
16. Puonti HK., Jääskeläinen SK., Hallikainen HK., et al. Improved sensory recovery with a novel dual neurorrhaphy technique for breast reconstruction with free muscle sparing TRAM flap technique. Microsurgery. 2017, 37 (1): 21–28.
17. Blondeel PN., Demuynck M., Mete D., et al. Sensory nerve repair in perforator flaps for autologous breast reconstruction: sensational or senseless? Br J Plast Surg. 1999, 52 (1): 37–44.
18. Spiegel AJ., Menn ZK., Eldor L., et al. Breast reinnervation: DIEP neurotization using the third anterior intercostal nerve. Plast Reconstr Surg. 2013, 1 (8): e72.
19. Djohan R., Scomacao I., Knackstedt R., et al. Neurotization of the nipple-areola complex during implant-based reconstruction: evaluation of early sensation recovery. Plast Reconstr Surg. 2020, 146 (2): 250–254.
20. Peled AW., von Eyben R., Peled ZM. Sensory outcomes after neurotization in nipple-sparing mastectomy and implant-based breast reconstruction. Plast Reconstr Surg Glob Open. 2023, 11 (12): e5437.
21. Beugels J., Cornelissen AJM., van Kuijk SMJ., et al. Sensory recovery of the breast following innervated and noninnervated DIEP flap breast reconstruction. Plast Reconstr Surg. 2019, 144 (2): 178e–188e.
22. Beugels J., van Kuijk SMJ., Lataster A., et al. Sensory recovery of the breast following innervated and noninnervated lateral thigh perforator flap breast reconstruction. Plast Reconstr Surg. 2021, 147 (2): 281–292.
23. Beugels J., Bijkerk E., Lataster A., et al. Nerve coaptation improves the sensory recovery of the breast in DIEP flap breast reconstruction. Plast Reconstr Surg. 2021, 148 (2): 273–284.
24. Cage TA., Simon NG., Bourque S., et al. Dual reinnervation of biceps muscle after side-to-side anastomosis of an intact median nerve and a damaged musculocutaneous nerve. J Neurosurg. 2013, 119 (4): 929–933.
25. Rönkkö H., Göransson H., Taskinen HS., et al. Comparison of peripheral nerve regeneration with side-to-side, end-to-side, and end-to-end repairs: an experimental study. Plast Reconstr Surg Glob Open. 2016, 4 (12): e1179.
26. Viterbo F., Brock RS., Maciel F., et al. End-to-side versus end-to-end neurorrhaphy at the peroneal nerve in rats. Acta Cir Bras. 2017, 32 (9): 697–705.
27. Bibbo C., Rodrigues-Colazzo E., Finzen AG. Superficial peroneal nerve to deep peroneal nerve transfer with allograft conduit for neuroma in continuity. J Foot Ankle Surg. 2018, 57 (3): 514–517.
28. Bhangra KS., Busuttil F., Phillips JB., et al. Using stem cells to grow artificial tissue for peripheral nerve repair. Stem Cells Int. 2016, 2016 : 7502178.
29. Baas M., Duraku LS., Corten EML., et al. A systematic review on the sensory reinnervation of free flaps for tongue reconstruction: does improved sensibility imply functional benefits? J Plast Reconstr Aesthetic Surg. 2015, 68 (8): 1025–1035.
30. Lee YS., Ahn JH., Park HJ., et al. Dual coaptation of facial nerve using masseteric branch of trigeminal nerve for iatrogenic facial palsy: preliminary reports. Ann Otol Rhinol Laryngol. 2020, 129 (5): 505–511.
31. Gontre G., Polmear M., Carter JT., et al. Primary repair versus reverse end-to-side coaptation by anterior interosseous nerve transfer in proximal ulnar nerve injuries. Plast Reconstr Surg. 2023, 152 (2): 384–393.
32. Hardcastle N., Texakalidis P., Nagarajan P., et al. Recovery of shoulder abduction in traumatic brachial plexus palsy: a systematic review and meta-analysis of nerve transfer versus nerve graft. Neurosurg Rev. 2020, 43 (3): 951–956.
33. Page MJ., McKenzie JE., Bossuyt PM., et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021, 372 : 71. doi: 10.1136/bmj.n71.
34. Sterne JA., Hernán MA.., Reeves BC., et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ, 2016; 355 : 4919. doi: 10.1136/bmj.i4919“10.1136/bmj.i4919.
35. http: //www.prisma-statement.org/.
36. Yap LH., Whiten SC., Forster A., et al. Sensory recovery in the sensate free transverse rectus abdominis myocutaneous flap. Plast Reconstr Surg. 2005, 115 (5): 1280–1288. doi: 10.1097/01.prs.0000156988.78391.d6.
Richard Christian Suteja
Faculty of Medicine, Udayana University,
Jl. Raya Kampus UNUD
Bukit Jimbaran, Kuta Selatan, Badung
Bali 80361
Indonesia
richardcs88@gmail.com
Submitted: 20. 9. 2024
Accepted: 20. 6. 2025
Labels
Plastic surgery Orthopaedics Burns medicine TraumatologyArticle was published in
Acta chirurgiae plasticae

2025 Issue 3
Most read in this issue
- Overall and area-specific tactile recovery following different methods of surgical reinnervation in post-mastectomy breast reconstruction – a systematic review and meta-analysis
- Brachymetacarpia – our experience with internal device for distraction osteogenesis in adolescent patients
- The importance of sentinel node biopsy and examination in malignant melanoma of the head and neck
- Case report of severe complications after gel injection breast augmentation – treatment and use of hemostatic net for effective management