
A systematic review of the use of corticosteroid injections with and without local anaesthetic for trigger finger
Authors:
G. J. Hourston 1; K. R. Quinn 2; J. Chan 2; A. Mckee 3
Authors‘ workplace:
Department of Trauma and Orthopaedic Surgery, Cambridge University Hospitals NHS Foundation Trust, Cambridge, UK
1; Leicester Medical School, Leicester, UK
2; Department of Trauma and Orthopaedic Surgery, North West Anglia NHS Foundation Trust, Peterborough, UK
3
Published in:
ACTA CHIRURGIAE PLASTICAE, 67, 3, 2025, pp. 203-209
doi:
https://doi.org/10.48095/ccachp2025203
Introduction
Trigger finger (also known as stenosing tenosynovitis) is caused by inflammation and hypertrophy of the digital flexor tendon sheath. Trigger finger occurs in 2–3% of the adult population; this increases to 5–20% in those diagnosed with diabetes mellitus [1]. The most commonly affected is the first annular pulley (A1) at the metacarpophalangeal (MCP) joint. This is thought to be due to the high forces and pressure exerted on this pulley when gripping. The aetiology of trigger finger remains unknown although repetitive hand movements and trauma have been suggested as a contributing factor. Trigger finger is 6-times more prevalent in women than men and other associated risk factors include those diagnosed with rheumatoid arthritis, hypothyroidism, carpal tunnel syndrome, de Quervain’s disease, amyloidosis and renal disease [2,3]. As the condition progresses, the tendon sheath narrows, restricting the movement of the pulley system through the sheath. This causes locking, pain, and stiffness in the affected phalange. Trigger finger is a clinical diagnosis, based on symptomatic reports and examination findings.
Prior to surgical intervention, initial management for trigger finger involves pain relief with non-steroidal anti-inflammatory drugs (NSAIDS), splinting, and corticosteroid injections. Splints are used to immobilise the metacarpophalangeal (MCP) or distal interphalangeal (DIP) joint to prevent friction in the pulley system, allowing time for inflammation to settle and therefore relief of symptoms. Surgical intervention (either percutaneous or open trigger finger release) is considered if the trigger finger becomes recurrent or in cases of locked trigger finger, fixed flexion contracture, history of failed injection in prior trigger fingers, and those with allergy to steroids, with conservative management failing to resolve symptoms.
Corticosteroid injections reduce inflammation, consequently widening the lumen of the flexor tendon sheath resulting in smoother movement and less catching. Surgeons routinely add local anaesthetic to the corticosteroid injection with the objective of reducing the pain of the injection. Local anaesthetic is acidic and is therefore known to cause irritation to the surrounding tissue, causing pain. We hypothesize that omitting local anaesthetic may produce a less painful injection and would also reduce the cost of the injection to the NHS, and so we carried out a systematic review exploring this.
Evaluation of the topic
Methods
A systematic review of the literature following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines was conducted for patients undergoing injection for trigger finger. We searched PubMed, Cochrane Library, and Embase databases for randomised control trials or cohort studies of any form investigating the effect on pain in patients with trigger finger treated with corticosteroid injection with and without local anaesthetic. Included search terms were “steroid”, “corticosteroid”, “trigger finger”, “trigger digit”, “stenosing tenosynovitis”, “anaesthetic”, “anaesthetic”, “local anaesthetic”, “local anaesthetic”, “lidocaine”, and “lignocaine”. The search strategy is shown in Appendix 1.
This systematic review was registered with PROSPERO, the international prospective register of systematic reviews. PROSPERO registration: CRD420245 02361. Protocol not published.
Using COVIDENCE, we imported the 216 studies identified by our searches over each database and an initial duplicate screen was run by the software. Two reviewers then independently selected the trials that were eligible, completing abstract and title screening then full paper screening. Any disagreement was resolved by discussion between the two reviewers. The study selection flow diagram is shown in Scheme 1.

Inclusion and exclusion criteria
The level of evidence required for inclusion was determined based upon recommendations by the Centre for Evidence-based Medicine [4]. This included high-quality randomized controlled trials (level I) or lesser quality randomized controlled trials and prospective comparative studies (level II). Lower levels of evidence such as case--control studies, retrospective studies, case series and case reports were excluded.
Our inclusion criteria included: the population of adults (>18 years old) with a diagnosis of trigger finger, the intervention of corticosteroid injections with local anaesthetic compared to without local anaesthetic, the outcome comparing initial visual analogue scale (VAS) pain scores of the injection, only English language articles and studies that have been published.
Two studies were identified as eligible for inclusion in our review [5,6]. 101 patients were enrolled and 98 patients included in the studies (135 injections). A summary of patient demographics is given in Tab. 1. The VAS pain score outcomes are presented and summarised in Tab. 2. The Green Trigger Finger scores are presented in Tab. 3. Two reviewers independently quality assessed these papers using the Cochrane RoB1 criteria and extracted the data, then discussing any discrepancies after completion.


VAS pain scores
Patients included in the study by Patrinely Jr. et al. [5] had one or more trigger fingers diagnosed by history and examination by a fellowship-trained hand surgeon. Patients who were excluded elected for open trigger finger release or had contraindications to the contents of the injection. Demographic data was collected for the age, sex, hand affected, finger affected, prior injection history and comorbidities of each patient (Tab. 1).
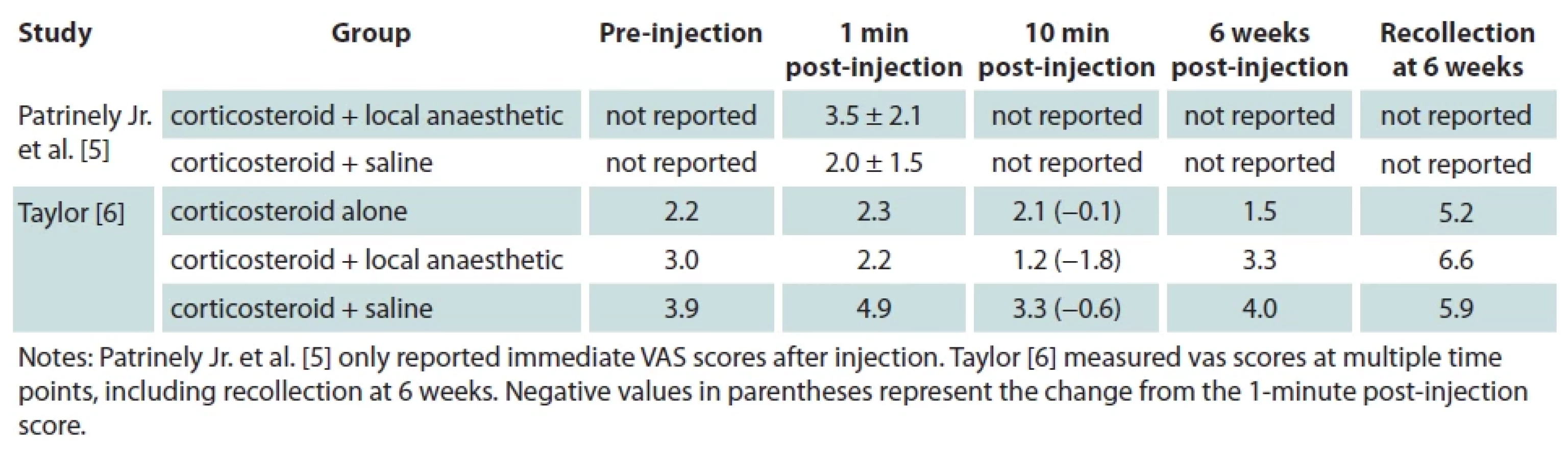
Immediate VAS pain scores were collected by the injecting surgeon and adverse outcomes were reported at the 6 week follow up appointment (Tab. 2). The results indicated that omitting local anaesthetic in corticosteroid injections had a lower initial VAS pain score at 2 compared with 3.5 with local anaesthetic, without any adverse outcomes.
Patients included in the unpublished study by Taylor [6] were aged between 18–90 years old, had a clinically diagnosed trigger finger, were able to provide written informed consent and were willing to attend follow up appointments. Patients who were excluded were outside of the specified age range, pregnant, not able to speak English, had a history of drug allergy, injection contents contraindicated, had prior injections, surgeries or an open wound on the affected digit or a diagnosis of complex regional pain syndrome (CRPS) or reflex symptomatic dystrophy (RSD). Minimal demographic data was collected with only age and sex analysed (Tab. 1). VAS pain scores were collected at regular intervals (pre-injection, 1 minute, 10 minutes and 6 weeks post-injection and a recollection of initial pain of the injection at that 6-week follow up) (Tab. 2). The only group that showed an initial (1-minute post-injection) average decrease in pain was the group with local anaesthetic and the same group also shows the largest average decrease in pain at 10 minutes post-injection. This contradicts our hypothesis that the addition of local anaesthetic increases the initial pain of the injection. However, at the 6 week follow up, the corticosteroid alone group have the lowest maintained VAS pain score at 1.5 (pre-injection 2.2) compared to the addition of local anaesthetic at 3.3 (pre-injection 3.0) and with saline at 4.0 (pre-injection 3.9).
Green Trigger Finger scores
The Green classification of the triggering digit was analysed pre-injection and 6 weeks post-injection in this study (Tab. 3). Using corticosteroid alone maintained the same degree of triggering of 1.7 whereas at 6 weeks the addition of local anaesthetic and saline increased the average green score to 2.6 (pre-injection 1.9) and at 2.3 (pre-injection 2.1) respectively. It is important to acknowledge the small group size that were analysed in this study of only 25 patients.
Quality assessment
The study by Patrinely Jr. et al. [5] used random allocation to assign treatment arms with a coin flip. This meant there was no control over the number of patients allocated to each group, although a 50% chance of being assigned to either (low risk of selection bias). The two treatment arms in this study were corticosteroid with local anaesthetic (triamcinolone (1 mL of 40 mg/mL) plus 1% lidocaine with 1 : 100 000 epinephrine (1 mL)) and corticosteroid with saline (triamcinolone (1 mL of 40 mg/mL) and normal saline (1 mL)). Both the patient and the surgeon administering the injection were blinded to the treatment arm, with the study coordinator preparing the injection. Therefore, the risk of researcher bias was low. The VAS pain score data was collected by the surgeon using an image of the Wong-Baker Pain FACES Pain Rating Scale [7]. Outcome data was complete with 75 patients enrolled but 2 declined in order to opt for open surgical treatment (low risk of attrition bias). This resulted in 73 patients included in the study with 110 injections in total: 57 corticosteroid with local anaesthetic and 53 corticosteroid with saline. The study acknowledges other factors that may alter the pain of the injection including: the volume of the injection, the use of epinephrine, the neutralising effect of sodium bicarbonate, needle placement and injecting anaesthetic prior to the injection. It also addressed the potential confounding factors of the patient cohort being predominantly men with a high incidence of insulin-dependent diabetes mellitus (who are therefore familiar with injections and so may have a higher pain tolerance). The study used lidocaine with epinephrine (pH 4.5) as this was the standard practice for their centre. However, it was acknowledged that using a buffer or a more neutral local anaesthetic may have altered the stinging pain of the injection, although with a short-term benefit.
The other study by Taylor [6] randomly drew sealed envelopes to allocate treatment arms which were then stored in a secure area (low risk of selection bias). This allowed some control over the number of patients allocated to each group. There were three treatment arms in this study: corticosteroid alone (1 mL dexamethasone sodium phosphate (4 mg/mL)), corticosteroid with local anaesthetic (1 mL dexamethasone sodium phosphate (4 mg/mL) and 1 mL 1% xylocaine) and corticosteroid with saline (1 mL dexamethasone sodium phosphate (4 mg/mL) and 1 ml 0.9% injectable sodium chloride). A total of 26 patients were enrolled and 25 patients were included. One patient withdrew due to “physician decision”. Six patients were allocated to corticosteroid alone group, 11 to corticosteroid with local anaesthetic and 8 to corticosteroid with saline. The data collector and the patient were both blinded to the treatment arm, although the study investigator who prepared and performed the injection was unblinded (increasing risk of performance bias). Outcome data was completed up to the 6-week follow-up; however, the study was terminated early due to recruitment problems. The corticosteroid with local anaesthetic group containing 11 participants also has some incomplete data, with only 10 responses for some outcomes. The results of this study were not analysed as it was terminated prematurely, although the data collected remains relevant to our review.
A summary of the risk of bias assessment for both studies is presented in Tab. 4. While the study by Patrinely Jr. et al. [5] generally has a low risk of bias, with strong blinding and complete outcome data, there was a minor concern regarding allocation concealment. However, the study by Taylor [6] has a moderate to high risk of bias due to early termination, missing data, and the unblinded investigator administering the injection.

Discussion
The results of this systematic review indicate that the addition of local anaesthetic to corticosteroid injections for trigger finger may influence the pain experienced by patients, though the available literature presents conflicting findings. Patrinely Jr. et al. [5] demonstrated that omitting local anaesthetic resulted in lower immediate pain scores, suggesting that the acidic pH and additional volume of the anaesthetic solution may exacerbate initial discomfort. Conversely, the unpublished study by Taylor suggested that local anaesthetic may lead to a decrease in pain scores at 10 minutes post-injection, which supports the hypothesis that local anaesthetic could provide early post-procedural pain relief [6]. However, this study also found that patients who received corticosteroid alone had the lowest pain scores at six weeks post-injection.
These results highlight the complex interplay between injection composition, pain perception, and long-term outcomes. The differences in reported outcomes could be attributed to several methodological variations, including the specific corticosteroid and anaesthetic used, the volume of the injection, and the timing of pain assessments. For instance, Patrinely Jr. et al. [5] used triamcinolone with lidocaine and epinephrine, while Taylor used dexamethasone with either lidocaine or saline [6]. The pH differences among these substances, as well as the buffering effect of sodium bicarbonate, could impact patient discomfort.
Furthermore, the method of injection delivery, including needle gauge and placement technique, could also contribute to variations in pain perception. Some studies suggest that buffering lidocaine with sodium bicarbonate may help reduce injection pain [8,9]. Additionally, the presence of comorbidities such as diabetes, which is common among patients with trigger finger, could influence pain perception and treatment response [10]. Volume has been indicated as a significant factor in injection pain previously, although speed of injection had no effect in the same trial [11].
The SToICAL trial protocol has been published which will attempt to address this question further [12]. The SToICAL trial is a single-site, patient - and assessor-blinded, non-inferiority randomized controlled trial designed to evaluate whether the pain experienced during the 24 hours following a corticosteroid injection into the hand or wrist is no worse than the pain experienced after a combined corticosteroid and local anaesthetic injection. The study focuses on patients diagnosed with trigger finger, de Quervain’s tenosynovitis, or carpal tunnel syndrome. Participants are randomly assigned to receive either a 1 ml triamcinolone (40 mg/mL) injection alone or the same corticosteroid combined with 1 mL of 1% lidocaine. The primary outcome measure is the difference in pain levels, assessed using VAS, at one hour post-injection. Secondary outcomes include pain assessments over the subsequent 24 hours. The trial aims to determine if omitting the local anaesthetic provides a comparable pain experience, potentially simplifying the injection procedure and reducing associated costs [12].
Overall, while there is evidence that local anaesthetic may increase initial injection pain due to its acidic nature and volume effect, it may provide short-term pain relief. However, the long-term benefits or drawbacks remain unclear due to limited high-quality studies addressing this specific question. Given the heterogeneity in study design and outcome reporting, it is difficult to draw definitive conclusions.
Corticosteroid injection remains a widely used first-line treatment for trigger finger, with the addition of local anaesthetic commonly implemented to reduce procedural pain. This systematic review found that while omitting local anaesthetic may reduce immediate injection pain, its role in post-procedural pain relief remains uncertain. The existing literature suggests that the effects of local anaesthetic on pain perception are influenced by multiple factors, including injection volume, pH, and buffering agents. Given the limited number of high-quality studies available and the inconsistencies in reported outcomes, further well-designed, randomized controlled trials are necessary to provide definitive guidance on this issue. The StoICAL trial, if implemented, may provide such guidance. Future studies should standardize injection techniques, anaesthetic compositions, and pain assessment timepoints to enable more robust comparisons. Until such evidence is available, clinicians should weigh the potential benefits and drawbacks of adding local anaesthetic based on individual patient preferences and clinical circumstances.
Disclosure: The authors do not have any potential conflicts of interest with respect to this manuscript. The authors received no financial support for the preparation, research, authorship, and/or publication of this manuscript.
Declaration of ethical approval and informed consent: Not applicable
Roles of the authors: GH, KQ & JC researched the literature. KQ & JC wrote the first draft. GH revised the first draft. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of use of AI and AI-assisted technologies
We used ChatGPT for the purpose of summarising our findings in the quality assessment of included articles. The content generated by the AI tool was reviewed and edited and we are responsible for all the content in our manuscript.
Appendix 1. Search strategy.
Title & Abstract “ ((steroid) OR (corticosteroid)) AND ((trigger finger) OR (trigger digit) OR (stenosing tenosynovitis)) AND ((anaesthetic) OR (anesthetic) OR (local anaesthetic) OR (local anesthetic) OR (lidocaine) OR (lignocaine)) ”
Sources
1. Gil JA., Hresko AM., Weiss AP. Current concepts in the management of trigger finger in adults. [online]. Available from: https: //journals.lww.com/jaaos/fulltext/2020/08010/current_concepts_in_the_management_of_trigger.5.aspx.
2. Makkouk AH., Oetgen ME., Swigart CR., et al. Trigger finger: etiology, evaluation, and treatment. [online]. Available from: https: //pmc.ncbi.nlm.nih.gov/articles/PMC2684207/.
3. Akhtar S., Bradley MJ., Quinton DN., et al. Management and referral for trigger finger/thumb. [online]. Available from: https: //pmc.ncbi.nlm.nih.gov/articles/PMC558536/.
4. CEBM. [online]. Available from: https: //www.cebm.net/2009/06/oxford-centre-evidence-based-medicine-levels-evidence-march-2009/.
5. Patrinely Jr JR., Johnson SP., Drolet BC. Trigger finger corticosteroid injection with and without local anesthetic: a randomized, double-blind controlled trial. [online]. Available from: https: //pmc.ncbi.nlm.nih.gov/articles/PMC84 61190/.
6. Taylor K. Pain with trigger finger injection: a comparison of steroid alone versus steroid/lidocaine mixture. [online]. Available from: https: //clinicaltrials.gov/study/NCT024 21419
7. Wong DL., Baker CM. Wong-Baker FACES pain rating scale. [online]. Available from: https: //doi.apa.org/doi/10.1037/t05330-000.
8. Bartfield JM, Gennis P., Barbera J., et al. Buffered versus plain lidocaine as a local anesthetic for simple laceration repair. Ann Emerg Med. 1990, 19 (12): 1387–1389.
9. Lee HJ., Cho YJ., Gong HS., et al. The effect of buffered lidocaine in local anesthesia: a prospective, randomized, double-blind study. J Hand Surg. 2013, 38 (5): 971–975.
10. Akintoye OO., Owoyele BV., Fabunmi OA., et al. Diabetic neuropathy is associated with increased pain perception, low serum beta-endorphin and increase insulin resistance among Nigerian cohorts in Ekiti State. [online]. Available from: https: //www.ncbi.nlm.nih.gov/pmc/articles/PMC7358268/.
11. Heise T., Nosek L., Dellweg S., et al. Impact of injection speed and volume on perceived pain during subcutaneous injections into the abdomen and thigh: a single-centre, randomized controlled trial. Diabetes Obes Metab. 2014, 16 (10): 971–976.
12. Jones M., Evans J., Fullilove S., et al. The SToICAL trial: study protocol for the soft tissue injection of corticosteroid and local anaesthetic trial – a single site, non-inferiority randomised control trial evaluating pain after soft tissue corticosteroid injections with and without local anaesthetic. [online]. Available from: https: //www.ncbi.nlm.nih.gov/pmc/articles/PMC8479928/.
George J. M. Hourston, MA MB BChir MRCS (Eng) PGCert (MedEd)
Academic clinical fellow
Department of Trauma and Orthopaedic Surgery
Cambridge University Hospitals NHS Foundation Trust
Cambridge, UK
gjmh3@cam.ac.uk
Submitted: 27. 3. 2025
Accepted: 21. 9. 2025
Labels
Plastic surgery Orthopaedics Burns medicine TraumatologyArticle was published in
Acta chirurgiae plasticae

2025 Issue 3
Most read in this issue
- Overall and area-specific tactile recovery following different methods of surgical reinnervation in post-mastectomy breast reconstruction – a systematic review and meta-analysis
- Brachymetacarpia – our experience with internal device for distraction osteogenesis in adolescent patients
- The importance of sentinel node biopsy and examination in malignant melanoma of the head and neck
- Case report of severe complications after gel injection breast augmentation – treatment and use of hemostatic net for effective management