
Guava leaf extract and polyvinylpyrrolidone hydrogel for rabbit oral wounds
Authors:
I. G. A. B. Jayaningrum 1; A. R. R. Hariantana Hamid 1; I. G. P. Hendra Sanjaya 1; G. W. Samsarga 2; I. W. Niryana 3; I. M. Darmajaya 4; S. Diwyani Sudarsa 2; A. Lestari Suyata 2
Authors‘ workplace:
Division of Plastic Surgery Reconstruction and Aesthetic, IGNG Ngoerah General Hospital, Denpasar, Bali
1; Division of Plastic Surgery Reconstruction and Aesthetic, Udayana Hospital, Denpasar, Bali
2; Department of Neurosurgery, IGNG Ngoerah General Hospital, Denpasar, Bali
3; Department of Pediatric Surgery, IGNG Ngoerah General Hospital, Denpasar, Bali
4
Published in:
ACTA CHIRURGIAE PLASTICAE, 67, 3, 2025, pp. 180-188
doi:
https://doi.org/10.48095/ccachp2025180
Introduction
Wound healing restores tissue integrity through inflammatory, proliferative, and remodeling phases, with fibroblast proliferation playing a key role [1]. Maxillofacial trauma, including mandibular fractures, requires advanced trauma life support-based (ATLS) management due to its impact on airway function [2–4]. Surgical treatment often involves open reduction and internal fixation (ORIF) via intraoral or extraoral approaches, each with benefits and risks. Intraoral techniques minimize scarring but increase the risk of infection, while extraoral approaches improve visualization but may cause nerve injury and scarring [5]. A major complication is intraoral wound dehiscence, prolonging recovery and increasing costs [6].
Wound dehiscence management requires meticulous care, but persistent cases impair healing and quality of life [7,8]. Herbal medicine, including guava (Psidium guajava Linn) leaves, shows potential due to antimicrobial, anti-inflammatory, and astringent properties [9,10]. polyvinylpyrrolidone sodium hyaluronate (PVP-NaHA) hydrogel accelerates oral wound healing, but studies on its combination with guava leaf extract are limited [11]. This study explores their synergistic effects in promoting oral wound healing.
Material and methods
This experimental study used a randomized post-test only control group design with 28 rabbits divided into four groups: P1 group (guava leaf extract + PVP hydrogel + suturing), K1 (extract without suturing), P2 group (placebo + suturing), and K2 group (placebo without suturing). Rabbits were housed under controlled conditions, receiving standard feed and care. Anesthesia was administered intramuscularly using a ketamine-xylazine-acepromazine (Ket-A-Xyl®; Ethica, Indonesia) mixture. Standardized incisional wounds were created on the gingival mucosa, with suturing using 5-0 Vicryl where applicable. The guava leaf extract gel was prepared through ethanol maceration, followed by formulation with carboxymethylcellulose – natrium (Na-CMC), propylene glycol, nipagin, glycerin, and triethanolamine. The gel was applied twice daily. Euthanasia was performed on day 14 using high-dose ketamine (Ketalar®; PT Pfizer Indonesia, Indonesia) and xylazine (Xyla®; Interchemie Werken De Adelaar Nederland B.V., The Netherlands), with tissue samples collected for histopathological analysis of IL-6, VEGF, and fibroblast count. Statistical analysis included Shapiro-Wilk test for normality, Levene’s test for homogeneity, and one-way analysis of variance (ANOVA) with post-hoc comparisons using Tukey or Games-Howell tests. The data were analyzed in the Statistical Package for the Social Sciences (SPSS) 26.0, with significance set at P < 0.05. The study was conducted at Udayana University, Indonesia, from November to December 2024.This study was approved by the Committee of Research and Experimental, Udayana University, Bali, Indonesia, under the number of 2608/UN14.2.2.VII.14/LT/2024. There are no human subjects mentioned in this article, therefore no informed consent is applicable.
Results
The 28 male rabbits were divided into four groups. On day 3, fibroblast count was highest in P1 (64.50 ± 4.43) and lowest in K1/P2 (55.67 ± 4.04). By day 14, P1 increased to 76.75 ± 7.68, while K1/P2 remained at 66.67 ± 1.53. Epithelialization in P1 was 131.34 ± 3.88 on day 3, rising to 176.95 ± 11.99 by day 14, whereas K2 remained the lowest (83.21 ± 16.87 to 94.65 ± 14.37).
VEGF levels in P1 were highest (day 3 : 68.99 ± 4.77; day 14 : 81.95 ± 5.23), while K2 had the lowest increase (53.17 ± 8.26 to 58.87 ± 6.02). IL-6 levels in P1 were the lowest (day 3 : 38.28 ± 0.95; day 14 : 23.87 ± 1.88), while K1/P2 remained elevated (48.56 ± 1.10 to 47.40 ± 1.21). The results indicate significant improvements in fibroblast proliferation, epithelialization, and VEGF levels while reducing IL-6.
Data characteristics are summarized in Tab. 1.
The ANOVA analysis in Tab. 2 showed significant differences in fibroblast counts among groups on days 3 (P = 0.009) and 14 (P = 0.035). On day 3, P1 had a significantly higher fibroblast count than K1 (mean difference 8.833; P = 0.041; 95% CI 0.33–17.34). K1 had significantly lower counts than P2 (−12.083; P = 0.007; 95% CI −20.59 to −3.58) and K2 (−9.333; P = 0.044; 95% CI −18.42 to −0.24). By day 14, P1 maintained the highest fibroblast count, though differences with K1 (10.083; P = 0.33) and other groups were not significant. K1 remained lower than P2 (−17.833; P = 0.042; 95% CI −35.01 to −0.66), but no significant differences were found between K1 and K2 (P = 0.979) or P2 and K2 (P = 0.08).
The analysis in Tab. 3 showed significant differences in epithelial length on days 3 (P = 0.001) and 14 (P = 0.000), confirming the efficacy of P1 in accelerating epithelialization. On day 3, P1 had significantly longer epithelium than P2 (−40.57; P = 0.003; 95% CI 15.34–65.79) and K2 (−48.13; P = 0.001; 95% CI 20.88–75.38), while differences with K1 were not significant (P = 0.129). On day 14, P1 remained the highest, significantly differing from K1 (−47.47; P = 0.001; 95% CI 23.35–71.59), P2 (−56.8; P = 0.000; 95% CI 34.47–79.13), and K2 (−82.3; P = 0.000; 95% CI 58.18–106.42). K1 vs. P2 was not significant (P = 0.65), but K1 vs. K2 (−34.82; P = 0.009) and P2 vs. K2 (−25.49; P = 0.038) were.
P1 significantly enhanced epithelialization at both time points. Sutures in K1 did not consistently improve healing, as differences with K2 were only significant on day 14. P2 showed better healing than K2 but was less effective than P1.
The analysis in Tab. 4 showed a significant increase in VEGF levels in the treatment groups compared to controls on days 3 (P = 0.009) and 14 (P = 0.000), indicating enhanced angiogenesis and tissue regeneration. On day 3, P1 had significantly higher VEGF than K2 (+15.82; P = 0.033; 95% CI 1.26–30.38), while differences in K1 (P = 0.13) and P2 (P = 0.962) were not significant. P2 also had higher VEGF than K2 (+17.92; P = 0.016). On day 14, P1 had significantly higher VEGF than K1 (+35.47; P = 0.000; 95% CI 23.61–47.33) and K2 (+23.08; P = 0.001; 95% CI 11.22–34.94), while the difference in P2 was not significant (P = 0.469). P2 also had significantly higher VEGF than K1 (−40.88; P = 0.000) and K2 (+28.49; P = 0.000), but K1 vs. K2 was not significant (P = 0.056). These results confirm that P1 consistently enhances VEGF expression, particularly on day 14, supporting its role in promoting angiogenesis and tissue repair. The effect was more pronounced in sutured wounds, suggesting an optimal environment for VEGF activation.
The analysis in Tab. 5 indicates that the combination gel significantly reduces IL-16 levels, a pro-inflammatory cytokine, during wound healing (P = 0.000 for both day 3 and day 14). On day 3, P1 had significantly lower IL-16 than K1 (−10.28; P = 0.000; 95% CI −14.17 to −6.40) and K2 (−11.09; P = 0.000; 95% CI −14.98 to −7.21), indicating reduced inflammation. However, P1 had higher IL-16 than P2 (+8.09; P = 0.000). Among controls, K1 and K2 showed no significant difference (P = 0.931), but P2 had significantly higher IL-16 than K2 (+19.19; P = 0.000). On day 14, P1 maintained lower IL-16 than K1 (−23.54; P = 0.000; 95% CI −28.01 to −19.06) and K2 (−5.06; P = 0.027; 95% CI −9.53 to −0.58). No significant difference was observed between P1 and P2 (P = 0.325). K1 had significantly higher IL-16 than P2 (+25.98; P = 0.000), and K1 vs. K2 also showed a significant difference (+18.48; P = 0.000).These findings confirm that P1 consistently reduces IL-16 levels, with a more pronounced effect in sutured wounds.
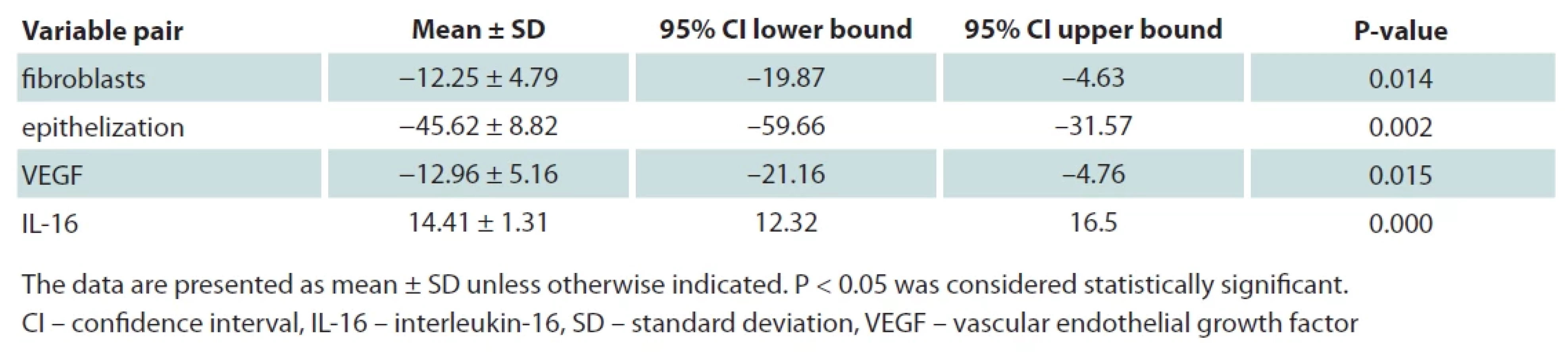
The analysis in Tab. 6 reveals significant changes in fibroblast count, epithelial length, VEGF, and IL-16 levels in group P1 between days 3 and 14 (P < 0.05, paired t-test), reflecting gingival wound healing dynamics. Fibroblast count significantly decreased by −12.25 ± 4.79 (P = 0.014; 95% CI −19.87 to −4.63), indicating a transition from the proliferative to the maturation/remodeling phase as collagen synthesis demand declines. Epithelial length decreased by −45.62 ± 8.82 (P = 0.002; 95% CI −59.66 to −31.57), suggesting rapid epithelialization peaking at day 3 and stabilizing by day 14, marking near-complete tissue regeneration. VEGF dropped by −12.96 ± 5.16 (P = 0.015; 95% CI −21.16 to −4.76), indicating reduced angiogenesis demand as vascularization stabilizes, highlighting the gel’s role in early wound healing. IL-16 increased by +14.41 ± 1.31 (P = 0.000; 95% CI 12.32 to 16.5), possibly reflecting residual inflammation during ongoing healing, warranting further investigation.
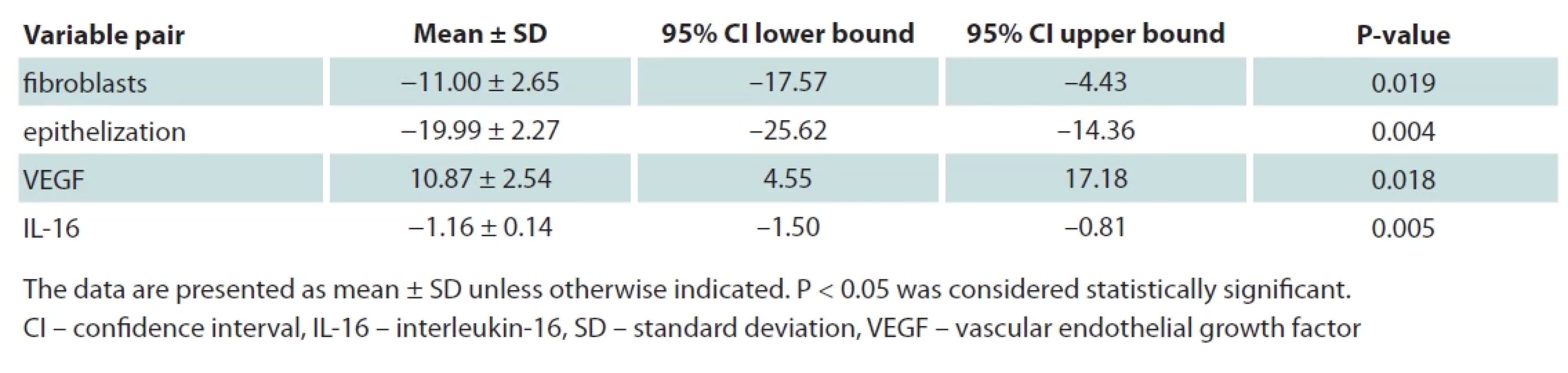
The analysis in Tab. 7 reveals significant changes in fibroblast count, epithelial length, VEGF, and IL-16 levels in the control group (K1) between days 3 and 14 (P < 0.05, paired t-test), reflecting natural wound healing without active intervention. Fibroblast count decreased by −11.00 ± 2.65 (P = 0.019; 95% CI −17.57 to −4.43), indicating a transition from proliferation to maturation. Compared to the treatment group (P1), fibroblast regeneration was slower, highlighting the gel’s role in accelerating this phase. Epithelial length decreased by −19.99 ± 2.27 (P = 0.004; 95% CI −25.62 to −14.36), suggesting slower epithelialization than the treatment group, indicating that the placebo had minimal effect in enhancing tissue regeneration. VEGF increased by 10.87 ± 2.54 (P = 0.018; 95% CI 4.55 to 17.18), reflecting ongoing angiogenesis in the control group.
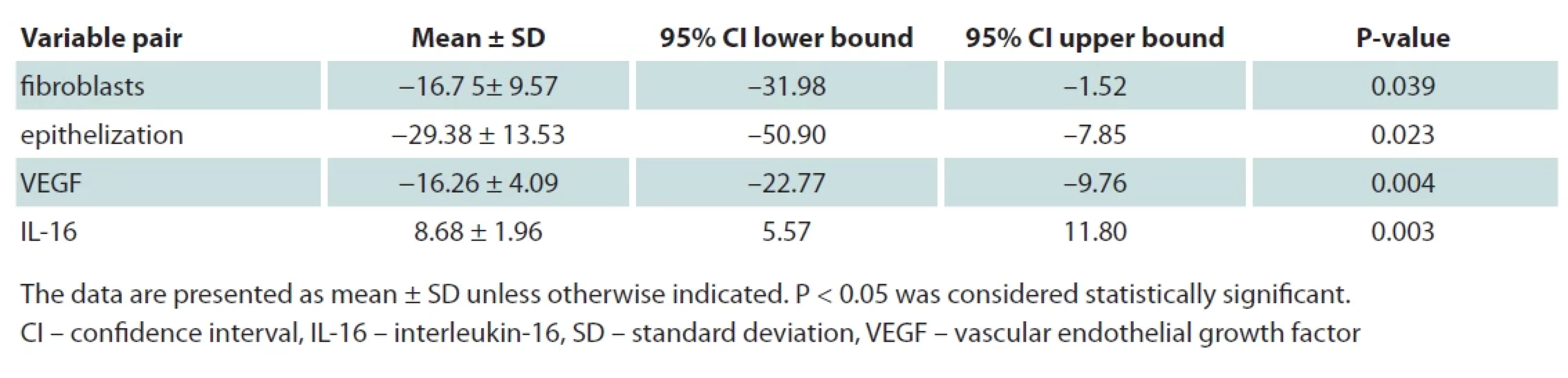
The analysis in Tab. 8 demonstrates the gel’s effectiveness in wound healing without sutures, though healing was slower than in P1. Fibroblast count decreased by −16.75 ± 9.57 (P = 0.039), indicating transition to maturation, with a greater decline than in P1, suggesting mechanical stabilization enhances fibroblast activity. Epithelial length decreased by −29.38 ± 13.53 (P = 0.023), reflecting slowed epithelialization after day 3, confirming sutures create a more favorable healing environment. VEGF declined by −16.26 ± 4.09 (P = 0.004), suggesting reduced angiogenesis as vas - cular stabilization occurs, with a sharper decline than P1, implying sutures aid gel distribution. IL-16 increased by 8.68 ± 1.96 (P = 0.003), indicating persistent inflammation at day 14, suggesting the gel is less effective in controlling inflammation without sutures. Overall, P2 showed significant wound healing, but at a slower rate than P1, highlighting the role of mechanical stabilization in optimizing regeneration and reducing inflammation.
The analysis in Tab. 9 illustrates natural wound healing without treatment or mechanical stabilization. Fibroblast count decreased by −4.00 ± 1.00 (P = 0.02), indicating a transition to maturation, but with minimal support for fibroblast activity. Epithelial length decreased by −11.45 ± 3.23 (P = 0.026), reflecting slower epithelialization compared to treated and sutured groups, confirming that both mechanical stabilization and active treatment accelerate healing. VEGF declined by −5.37 ± 1.82 (P = 0.036), showing reduced angiogenesis, with a smaller decline than active treatment groups, suggesting prolonged vascular maturation. IL-16 increased by 20.45 ± 4.94 (P = 0.019), indicating prolonged inflammation at day 14, delaying the transition to proliferation.
Histological analysis of rabbit gingival mucosa on day 3 post-treatment with guava leaf ethanol gel and polyvinylpyrrolidone hydrogel is shown in Fig. 1. The treatment group (P1) exhibited greater epithelial thickness (128.61–129.98 µm) than controls (69–97 µm), indicating enhanced epithelialization. Flavonoids, tannins, and saponins in guava extract stimulated keratinocyte migration and collagen synthesis, while hydrogel maintained wound moisture, promoting regeneration. Reduced IL-16 levels accelerated the transition to the proliferative phase, with improved tissue organization and angiogenesis marked by increased VEGF expression
Histological analysis on day 14 post-treatment is shown in Fig. 2, indicating near-complete healing in the treatment group (P1), with thicker, well-organized epithelium (161.74–173.22 µm) compared to controls (128.53–136.82 µm). Fibroblast activity declined, marking the transition to the maturation phase with stabilized collagen synthesis and the extracellular matrix (ECM) organization. VEGF levels decreased, indicating sufficient vascularization, while IL-16 levels were significantly lower, suggesting reduced inflammation. Unlike the untreated control (K2), which still showed inflammation, P1 exhibited optimal regeneration, confirming the gel’s effectiveness in accelerating wound healing.
Discussion
Wound healing involves inflammation, proliferation, and remodeling, with fibroblasts playing a crucial role in ECM production, collagen synthesis, and immune regulation [12]. This study demonstrated that a combination of ethanol extract of guava leaves (Psidium guajava Linn) and PVP hydrogel significantly enhances fibroblast proliferation, VEGF expression, and epithelialization while reducing inflammation. On day 3, fibroblast counts in the treatment group (P1) were 64.50 ± 4.43, significantly higher than controls (P = 0.041), with further increases by day 14 (76.75 ± 7.68 vs. 66.67 ± 1.53) [13]. The hydrogel sustained fibroblast activity into the remodeling phase, minimizing fibrosis [14]. VEGF, a key angiogenic factor, was also significantly elevated in P1 (68.99 ± 4.77 vs. 57.34 ± 1.54 on day 3; 81.95 ± 5.23 vs. 58.87 ± 6.02 on day 14), suggesting enhanced vascularization and oxygen supply [15,16]. The gel also modulated inflammation by reducing IL-6 (38.28 ± 0.95 on day 3 to 23.87 ± 1.88 on day 14; P < 0.000), expediting the transition to proliferation [17]. Additionally, IL-16, an inflammatory marker, decreased by 45% in P1 by day 3, reaching 27.34 ± 1.21 pg/mL on day 14 compared to 41.78 ± 2.87 pg/mL in controls, fostering a favorable environment for regeneration [18]. The hydrogel’s moisture-retaining properties supported keratinocyte migration and gradual bioactive release, further enhancing healing efficiency [19]. Histological analysis confirmed superior epithelialization in P1, with epithelial thickness reaching 176.95 ± 11.99 µm by day 14 compared to 129.48 ± 7.29 µm in controls [20]. Guava leaf extract’s flavonoids and tannins played essential roles in reducing oxidative stress, forming a protective barrier, and enhancing collagen deposition [21,22]. The antibacterial effects against Staphylococcus aureus and Pseudomonas aeruginosa further reduced infection risks, crucial for chronic wound management [18]. These findings suggest that integrating herbal bioactive compounds with biomaterials like PVP hydrogel provides a promising therapeutic strategy for enhancing wound healing, optimizing fibroblast activity, angiogenesis, and inflammation control [15,23,24].








Conclusion
The combination of guava leaf ethanol gel and PVP hydrogel significantly enhances gingival wound healing in rabbits by increasing fibroblast count, epithelialization, VEGF levels, and reducing IL-16 compared to controls. Faster epithelialization was observed in the treatment group, particularly on day 14, indicating accelerated tissue regeneration. IL-16 levels decreased significantly at both time points, demonstrating effective inflammation control and a favorable wound microenvironment. The synergy between bioactive compounds (flavonoids, tannins, terpenoids) and PVP hydrogel improves bioavailability, maintains moisture, promotes angiogenesis, and prevents excessive inflammation. Sutures combined with the gel enhance results by ensuring uniform distribution and better wound stabilization. This innovative therapy shows high potential for accelerating wound healing, particularly in chronic or non-healing wounds, with minimal inflammation and scarring risks.
Conflicts of interest
None declared. No financial support.
Roles of the authors
All authors contribute to the creation of this original article. IGAABJ designed the study, collected the data, drafting the manuscript and funding the research. ARRHH and IGPHS also designed the study and contribute in drafting the manuscript. GWS, IWN, IMD, SDS, and ALS supervised the whole process and gave revision on the writing on this journal. All authors reviewed and approved the final manuscript.
Sources
1. Gonzalez AC., Costa TF., Andrade ZD., et al. Wound healing – a literature review. [online]. Available from: https: //pmc.ncbi.nlm.nih.gov/articles/PMC5087220/
2. Khan TU., Rahar S., Khan ZA., et al. Etiology and pattern of maxillofacial trauma. [online]. Available from: https: //pmc.ncbi.nlm.nih.gov/articles/PMC9522305/.
3. Singh V., Malkunje L., Mohammad S., et al. The maxillofacial injuries: a study. [online]. Available from: https: //pmc.ncbi.nlm.nih.gov/articles/PMC3700151/.
4. Esmaeelinejad M. Maxillofacial fractures: from diagnosis to treatment. [online]. Available from: https: //www.intechopen.com/chapters/60520.
5. Yadav A. Principles of internal fixation in maxillofacial surgery. [online]. Available from: https: //link.springer.com/chapter/10.1007/ 978-981-15-1346-6_51.
6. Oksa M., Haapanen A., Marttila E., et al. Postoperative wound dehiscence in mandibular fractures. Acta Odontol Scand. 2023; 81 (7): 555–561.
17. Kumar JN., Ravi P. Postoperative care of the maxillofacial surgery patient. [online]. Available from: https: //pmc.ncbi.nlm.nih.gov/articles/PMC7882239/.
18. Espinosa MC., Hohman MH., Sivam S. Oral and maxillofacial surgery, facial laceration repair. [online]. Available from: https: //www.ncbi.nlm.nih.gov/books/NBK570584/.
9. Budovsky A., Yarmolinsky L., Ben-Shabat S. Effect of medicinal plants on wound healing. Wound Repair Regen. 2015, 23 (2): 171–183.
10. Carolino MV., Purnamasari L., Flores Dela Cruz J. The antibacterial properties of Psidium guajava leaf extract as a wound healing agent of laboratory animals: a review. [online]. Available from: https: //biotropika.ub.ac.id/index.php/biotropika/article/view/1313/0.
11. Buchsel PC. Polyvinylpyrrolidone-sodium hyaluronate gel (Gelclair): a bioadherent oral gel for the treatment of oral mucositis and other painful oral lesions. Expert Opin Drug Metab Toxicol. 2008, 4 (11): 1449–1454.
12. Roman R. Fibroblasts – warriors at the intersection of wound healing and immunomodulation. Biomolecules. 2023, 13 (6): 945.
13. Stunova A., Vistejnova L. Dermal fibroblasts: A heterogeneous population with regulatory functions in wound healing. Cytokine & Growth Factor Rev. 2018, 39 : 137–150.
14. Foster DS., Januszyk M., Yost KE., et al. Integrated spatial multiomics reveals fibroblast fate during tissue repair. Proc Natl Acad Sci USA. 2021, 118 (41): e2110025118.
15. Sutrisno E., Susilawati E., Herdiana GB., et al. Gel formulations of guava leaves (Psidium guajava L) ethanol extract as a wound healing of burns in rabbits. [online]. Available from: https: //journal.rescollacomm.com/index.php/ijrcs/article/view/626.
16. Dvorak HF. Reconciling VEGF with VPF: The importance of increased vascular permeability for stroma formation in tumors, healing wounds, and chronic inflammation. Front Cell Dev Biol. 2021, 9 : 660609.
17. Maigoda AR., Refdanita S., Abidin Z. Collagen synthesis in wound healing accelerated by herbal gel formulation. Int J Biol Macromol. 2022; 194 : 567–576.
18. Yang L., Zhang L., Hu J., et al. Promote anti-inflammatory and angiogenesis using a hyaluronic acid-based hydrogel with miRNA-laden nanoparticles for chronic diabetic wound treatment. Int J Biol Macromol. 2021; 166 : 166–178.
19. Ekom SE., Tamokou J-DD. Methanol leaves extract of Psidium guajava Linn. exhibited antibacterial and wound healing activities. [online]. Available from: https: //www.researchgate.net/publication/326673330_Methanol_Leaves_Extract_of_Psidium_guajava_Linn_Exhibited_Antibacterial_and_Wound_Healing_ Activities.
20. Hakim RF., Fakhrurrazi F., Zamzami FS. Comparison of the effect of guava (Psidium guajava L.) leaf extract with polyvinylpyrrolidone-sodium hyaluronate on the number of fibroblasts (study on white rats Rattus norvegicus). [online]. Available from: https: //www.researchgate.net/publication/372779522_Comparison_of_the_effect_of_guava_psidium_guajava_ l_Leaf_extract_x_withpolyvinylpyrrolidone-sodium_hyaluronate_on_the_number_fibroblasts_study_on_white_rats_rattus_norvegicus
21. Naseer S., Hussain S., Naeem N., et al. The phytochemistry and medicinal value of Psidium guajava (guava). [online]. Available from: https: //clinphytoscience.springeropen.com/articles/10.1186/s40816-018-0093-8
22. Delorino SB., Ogalesco ML., Rebadulla KR., et al. Wound healing efficacy of guava leaf extract. [online]. Available from: https: //journaljpri.com/index.php/JPRI/article/view/1882/ 3772.
23. Ahmad A., Nawaz MI. Molecular mechanism of VEGF and its role in pathological angiogenesis. J Cell Biochem. 2022, 123 (12): 1938–1965.
24. Das A., Abas M., Biswas N., et al. A modified collagen dressing induces transition of inflammatory to reparative phenotype of wound macrophages. Sci Rep. 2019, 9 : 14688.
I Gusti Ayu Agung Bella Jayaningrum
Imam Bonjol Street, Rahayu Alley
Denpasar, Bali, Indonesia
bellajayaningrumspbp@gmail.com
Submitted: 31. 3. 2025
Accepted: 31. 10. 2025
Labels
Plastic surgery Orthopaedics Burns medicine TraumatologyArticle was published in
Acta chirurgiae plasticae

2025 Issue 3
Most read in this issue
- Overall and area-specific tactile recovery following different methods of surgical reinnervation in post-mastectomy breast reconstruction – a systematic review and meta-analysis
- Brachymetacarpia – our experience with internal device for distraction osteogenesis in adolescent patients
- The importance of sentinel node biopsy and examination in malignant melanoma of the head and neck
- Case report of severe complications after gel injection breast augmentation – treatment and use of hemostatic net for effective management