
Stable osteosynthesis of pathological fracture of long bones in patients with multiple myeloma; retrospective evaluation of the therapy
Authors:
Milan Krtička 1; Martin Chovanec 1; Pavel Smékal 1; Martin Štork 2; Luděk Pour 2
Authors‘ workplace:
Klinika úrazové chirurgie FN Brno a Lékařské fakulty Masarykovy univerzity
1; Interní hematologická a onkologická klinika FN Brno a Lékařské fakulty Masarykovy univerzity
2
Published in:
Úraz chir. 27., 2020, č.1
Overview
Objective: Retrospective evaluation of the results of operating treatment in patients with multiple myeloma (MM) with pathological fracture of the long bone treated by the stable osteosynthesis (OS) at the Trauma Clinic of the University Hospital Brno in the period from January 2013 to December 2018.
Material and methods: Retrospective evaluation of the set of 410 patients treated with MM at the University Hospital Brno in the period of 2013–2018. Both inclusion and exclusion criteria were determined. The method of the performed osteosynthesis of a pathological fracture of the long bone depended on its localisation. It was either a nailing or plating osteosynthesis with stabilisation using the Prevotʼs rods. The following was evaluated on the acquired set of patients. Epidemiology data, fracture occurrence mechanism and type of fracture, intensity of pain, Mirels´ score, type of the osteosynthesis used, time section from determination of the MM diagnosis to occurrence of the fracture and also from the performed osteosynthesis to the healing of the fracture, and any treatment complications, if appropriate.
Results: Following the satisfaction of the inclusion and exclusion criteria, a set was formed of 24 patients with MM, who suffered a total of 32 pathological fractures of long bones in the myeloma deposits and were treated using the osteosynthesis method. 11 men and 13 women were represented in the set. The average age of the monitored patients was 71 years. Fractures were localized in 20 cases into the region of diaphysis and proximal humerus, once into the radial area, and in 11 cases into the femoral area. Nailing osteosynthesis was used in 26 fractures (82 %), plating osteosynthesis was used in 5 fractures (15 %), and Prevotʼs rods were used in 1 case (3 %). In correlation with the used osteosynthesis method, we reported the healing of the fracture with a bony callus in 29 cases (91 %), in 2 cases (6 %) the direct healing, and 1 fracture did not heal and a false joint was formed (3 %). The following complications occurred during the treatment in 23 patients: periimplant fracture (N=2), and proximalisation of humeral nail with interference into subacromial space (N=1).
Conclusion: MM represents a serious hematologic disease. Unlike in metastatic affection of bones with solid tumours, performance of stable osteosynthesis is indicated in respect of myeloma bone disease in the case of a pathological fracture of long bones, which does not exclude simultaneous systemic treatment of MM or radiotherapy.
Keywords:
pathological fracture – Multiple myeloma – osteolytic deposit – stable osteosynthesis – Mirels´ score
INTRODUCTION
Multiple myeloma (Kahlerʼs disease) is a malignant tumour disease the aetiology of which is not quite clear yet. Incidence of the disease in the Czech Republic is quantified to be 4.8 patients per 100,000 inhabitants while men are affected more frequently; the age median of newly diagnosed patients is 69 years and the incidence of the disease increases with the increasing age [15]. The disease develops by clonal proliferation of plasmocytes, which are responsible for immunoglobulin secretion in the immunity system. If malignant transformation occurs, a subpopulation of one clone of plasmocytes develops, grows uncontrollably and their cumulation in the bone marrow occurs [1]. Myeloma cells form deposits, often bulky ones, in the bone marrow, or they infilter the marrow diffusively [23]. One of the features of the pathologically transformed plasmocytes is the stimulation of osteoclasts by the way of cytokine signalling and suppression of osteoblasts at one time. This humoral activity results in the disturbance of dynamic balance of the bone metabolism in favour of the osteolysis [17]. In early stages, the osteolytic deposit weakens particularly the trabecular bone and as the disease progresses, affection of cortical layer of the bone and microfractures develop. It results in disturbed strength of the bone and its mechanical instability in the place of osteolytic lesion. Cumulation of plasmocytes results in increased intraosseal pressure and perifocal edema with irritation of nerve endings. This process is accompanied by increasing pain in the place affected by osteolysis [1]. Pathologically changed plasmocytes are predilectionally accumulated particularly in places with persisting hematopoiesis in the adult age (lumbar and thoracic spine, skull, pelvis, and long bone diaphysis). MM is clinically manifested by a broad scale of symptoms, the most frequent of them being hypercalcemia, renal insufficiency, anemia and myeloma bone disease, which affects 80 % of the patients with MM (group). Osteolytic affection of the skeleton in terms of a bone disease is present in up to 70 % of the patients and pathological fractures affect up to 50 % of the above-mentioned patients [6]. Myeloma bone disease is typically accompanied by the night back pain in consequence of vertebral osteolysis or subsequent compressive fracture [5]. Additional less frequent, but the more intensive symptoms of the disease are represented by limb pains resulting from osteolytic affection of long bone diaphyses, which often result in development of a pathological fracture in the place of deposit in consequence of dynamic-static demands on the limbs. These pathological fractures may be burdened with not only an increased blood loss but also the risk of development of compartment syndrome or affection of nerves and vessels in the given locality. Preventive osteosynthesis, which can be performed as early as before development of a pathological fracture, is being offered as an ideal solution to the affection of long bones in limbs. Unfortunately, the myeloma-specific indication criteria for its performance have not been determined up to the present moment.
An MM and monoclonal gammapathy work group has established at the Internal Hematooncology Clinic (IHOK) of the University Hospital (FN) in Brno since 1996. IHOK FN Brno is the biggest centre providing comprehensive care of the patients with MM across the Czech Republic. About 100 new patients are annually diagnosed here with MM. The objective of our work was the retrospective evaluation of the result of treatment of the patients with MM treated at the Trauma Surgery Clinic of the University Hospital in Brno due to pathological fracture of long bones in 2013-2018.
MATERIAL AND METHODOLOGY
Retrospective evaluation of a set of 410 patients with MM treated at the University Hospital in Brno in the interval from January 2013 to December 2018. The following inclusion criteria were determined: MM in medical history, presence of long bone osteolytic deposits, pathological fracture in myeloma deposit in the long bone of limbs, minimal length of monitoring of the patient 12 months from the performed osteosynthesis. Exclusion criteria were as follows: pathological fracture in the area of thoracic and lumbar spine, conservative therapy of the pathological fracture of a long bone in the place of myeloma deposit, associated long bone fracture without pathological correlate. The AmisH hospital information system, the MariaWeb radiologic documentation web browser, and the monoclonal gammapathy register (RMG) administered by the Czech Myeloma Group (CMG) were used to collect the data.
A definite set of patients for the following evaluation was formed based on the satisfaction of inclusion and exclusion criteria. In the set formed we evaluated the basic epidemiologic data (age, sex, laterality, locality affected), level of pain reported before development of the fracture evaluated by means of Visual Analog Scale [2], fracture development mechanism, time interval from MM diagnose to development of the fracture and also from the OS procedure to the healing of the fracture. Type of fracture according to AO classification, osteosynthesis method used and complications during the treatment, if any, were monitored as well.
Evaluation of the type of fracture was performed from the x-ray images captured in two mutually perpendicular projections. Location and size of the deposit, level of erosion of the cortical layer of the bone were always described. From the last x-ray, where no fracture in the pathological deposit was obvious yet, we calculated the Mirels´ score [20] for all patients; this score can predict the risk of fracture in pathological bone lesions; for details see Table 1. If the Mirels´ score ranges from 1 to 7 points, the risk of pathological fractures is 4 %; at 8 points it grows up to 15 %, at 9 point and more it grows to more than 33 %. In the given case, preventive osteosynthesis of the long bone with pathological deposit should be indicated.

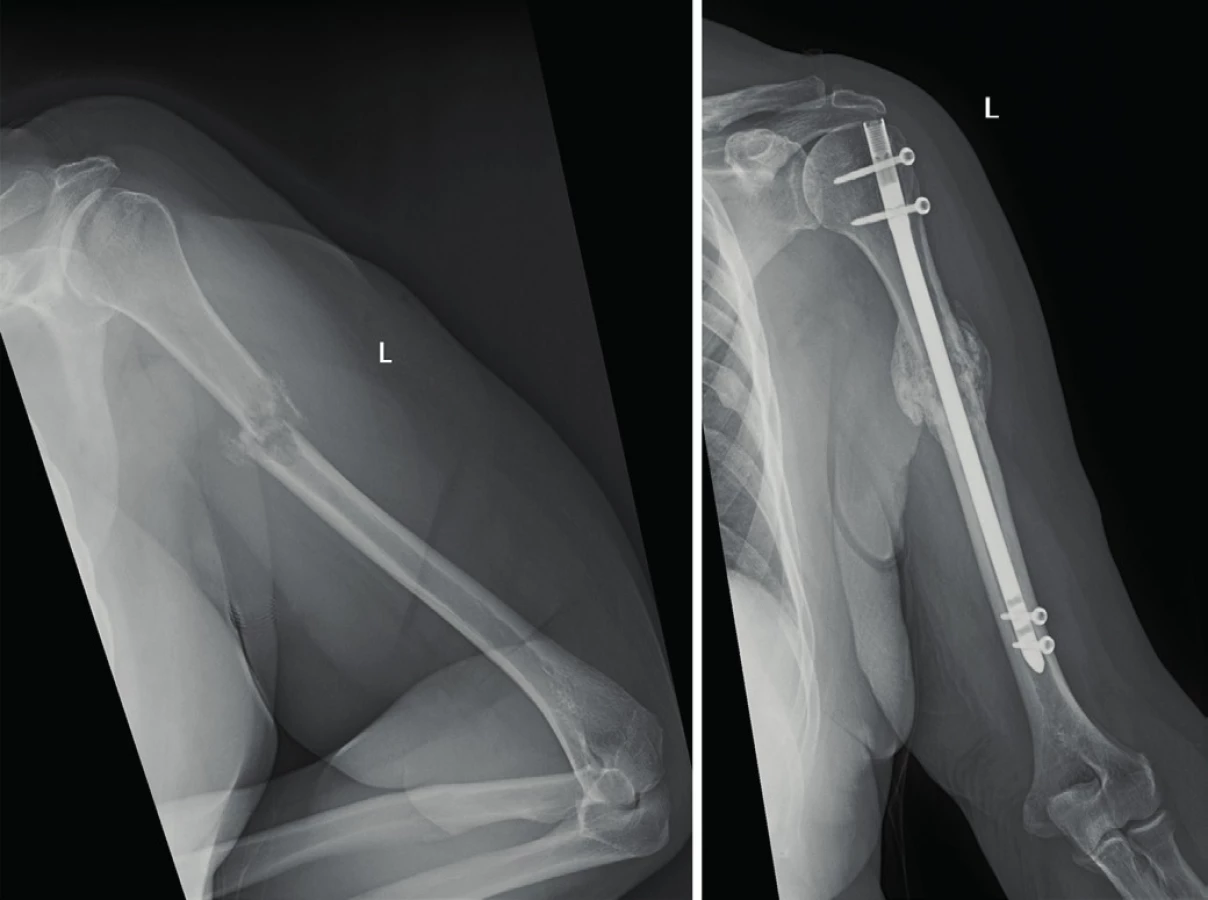
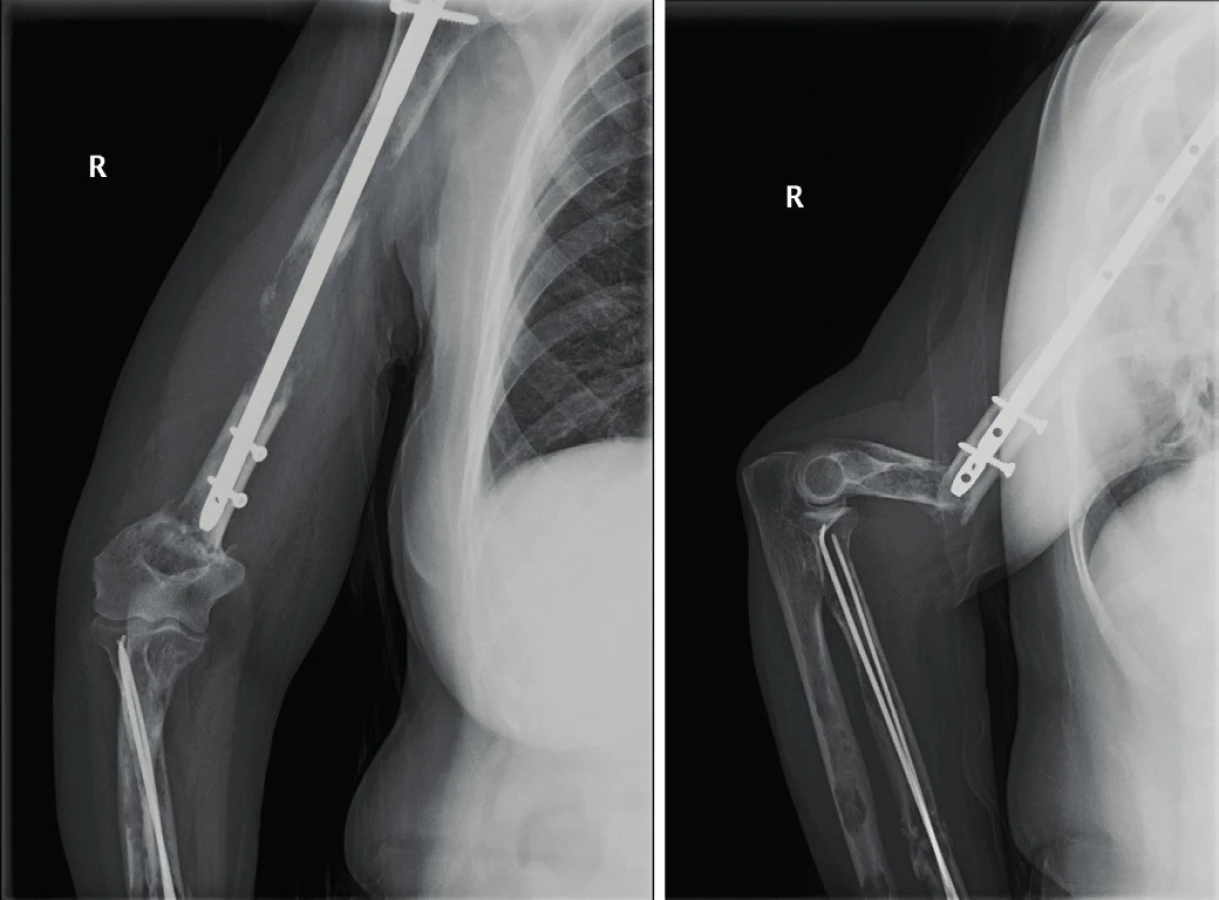
Osteosynthesis with a reconstruction nail (Targon PFT; B-Braun) was performed in proximal femoral fractures. In diaphyseal fractures, on the other hand, we chose OS using a statically locked femoral nail (LFN, Synthes). In the event of localisation of the fracture in the distal femoral area, the osteosynthesis method using a 5.0 mm, under-pulled, pre-formed distal femoral plate (Synthes). Forearm fractures were treated either by plating osteosynthesis (3.5mm direct plate with stable angle, Synthes) or using the intra-marrow osteosynthesis with Prevotʼs rods (Synthes), see Fig. 2. The surgical technique we chose depended on the type and localisation of the fracture. Proximal humeral fractures and fractures in the area of diaphysis were managed by nailing osteosynthesis (OS) with a straight or angular humeral nail (Targon PH, H; B-Braun), see Fig. 1.

RESULTS
A total of 410 patients with MM were treated at the University Hospital in Brno in the monitored period from January 2013 to December 2018. Inclusion criteria were met by 98 patients. Additionally, 5 patients were excluded from the set due to conservative therapy of the fracture, 1 patient was excluded due to associated distal radial fracture in the field not affected by a myeloma deposit, and 68 patients with associated compressive fractures of lumbar and thoracic spine. In total, we evaluated a set of 24 patients with MM with 32 pathological fractures of long bones in the myeloma deposits.
11 men (46 %) and 13 women (54 %) were represented in the set. The average age of all the monitored patients was 71 years (52–100 years), the median being 69 years. Out of the total number of 32 pathological fractures, 15 fractures were on the left and 17 fractures were on the right. The period between determination of the MM diagnosis and development of the fracture ranged within the interval from 0 months (pathological fracture was the first symptom of the MM and its development resulted in diagnosing the MM) to 11 years (132 months). On the average it was 51 months, i.e. 4 years and 3 months from the diagnosing and development of a pathological fractures, for details see Table 2. Low-energy mechanism of the injury (fall from the body height on the limb) was described in 18 patients with 21 fractures. In 6 patients with 11 fractures, on the other hand, the pathological fracture developed spontaneously in the myeloma deposit, i.e. without any injury event.

In 18 patients we performed 24 osteosyntheses of upper limb long bones and in 8 patients we performed 8 osteosyntheses of femoral fractures. Crural fracture was not represented in our set. Osteosynthesis of both the upper and lower limbs simultaneously was necessary in two patients. Humeral fracture in proximal third part was represented in 1 patient, in the middle third part in 19 cases; distal third part was not affected by fracture. Femoral fractures were most frequently localised on distal third part (N=5), subsequently in the area of diaphysis (N=4), and least frequently in the peritrochanteric area (N=2).
Nailing osteosynthesis dominated in fracture stabilisation; it was used in 26 cases (82 %) mainly in diaphyseal fractures. LCP osteosynthesis was performed in 5 fractures (15 %), with localisation in proximal humeral region. Prevotʼs rods were used for stabilisation of 3 pathological radial fractures (3 %). LCP plate was used on lower limb to treat the distal femoral fracture. Table 3 shows application of the type of osteosynthesis depending on localisation of the fracture.

The measured intensity of pain in the affected limb at the time before development of the pathological fracture in most cases ranged from moderate to strong pain. Stronger pains dominated in lower limbs. Table 4 provides a clearly arranged evaluation.

In correlation with the used osteosynthesis method, we reported the healing of the fracture with a bony callus in 29 cases (91 %), in 2 cases (6 %) the direct healing, and 1 fracture did not heal and a false joint was formed (3 %).
The following complications occurred in the monitored set: periprosthetic fracture below the nail (Fig. 3) and above the plating osteosynthesis; proximalisation of humeral nail in the field of extreme osteoporosis occurred in one patient. Conservative approach was used in patients with periprosthetic fractures with regard to unfavourable internal condition of the patients, which was a contraindication of subsequent surgical procedures.
According to the x-rays evaluated, erosion of the cortical bone layer was obvious in 14 cases, ranging from 34 to 99 %. The calculated Mirels´ score from the time of the last x-ray, where the fracture was not apparent yet, achieved the value of 8.5 points for the upper limbs and 9.7 points from the lower limbs. The average score not distinguishing the limbs equalled 8.8 points. In 20 cases (63 %), the score was bigger than or equalled 9, i.e. it was over the limit. A pathological fracture subsequently developed in all the monitored patients.
DISCUSSION
Myeloma bone disease occurs in 70 % of the patients with MM and in 50 % it is complicated by a pathological fracture, which usually develops within the first two years after being diagnosed with the MM and it substantially affects the patients´ quality of life [18]. Pathological fracture and its surgical treatment are also the most frequent reason for delaying or necessary reducing of the anti-tumour treatment. No less negligible fact is the significant impairment of the patients´ pain [5].
In our set we evaluated patients with pathological fracture of long bones of the upper and lower limb. Before the fracture, the patients suffered from considerable pain of the affected limbs. It is this pain that causes significant morbidity and affects the quality of life of the patients with MM [22].
At present, indication criteria for the performance of preventive nailing osteosynthesis of lytic lesions of long bones in patients with MM are not explicitly determined. Screening whole-body x-ray examinations or whole-body low-dose CT can be used in the given case. Bone lesions are evaluated according to the Mirels´ score [20]. This is however a universal indicator for a metastatic bone disease; it is not MM-specific and it evaluates the level of subjectively perceived painful perception, i.e. its reproducibility by other evaluators is reduced [8].
With regard to mechanical function of the long bones, the identified predictors of an imminent pathological fracture in the osteolytic field particularly include: size of deposit, erosion of the cortical layer of bone, and chronic pain in the place of deposit, particularly where it progresses when the limb is loaded [6, 7]. A retrospective study of ninety-six patients. The size of osteolytic deposit exceeding two thirds of the bone diameter results in a pathological fracture in up to 81% of the patients, being accompanied by heavy pain with impaired function of the limb [14] this information corresponds with our results of the VAS measured.
Development of a pathological fracture, i.e. complete interruption of both cortical layers of the bone, causes a sharp pain in the place of fracture. According to findings of Melton et al. 75 % of pathological fractures in patients with myeloma bone disease develop spontaneously during their daily activities [18]. This information is in contrast with our finding where spontaneous fracture in our set developed in 25% of the patients only. The remaining patients reported low-energy mechanisms of the injury. Correctly set bisphosphonate therapy in combination with systemic therapy could be the explanation [26].
In our retrospectively evaluated set, 63 % of the patients achieved the Mirels´ score of 9 and more, i.e. they met the criteria for preventive surgical treatments of the affected long bone which, if it was performed, would mean that no pathological fracture would develop. With regard to primary care of patients taken by hemato-oncology specialists and to sub-optimally adjusted co-operation with a bone surgeon, the fractures described above did develop. Since 2018, a bone surgeon is a valid part of the myeloma team at the University Hospital in Brno and preventive osteosynthesis of the affected long bones is indicated based on the Mirels´ score achieving 9 or more.
If a pathological fracture develops in a patient, therapeutic method needs to be determined. A fact that vertebroplasty or kyphoplasty is a safe therapeutic method, which is fully indicated in the given case, has been confirmed in respect of compressive vertebral fractures with subsequent neurological symptomatology [12]. No such explicit recommendation has been determined for the fractures of long bones yet. Most authors agree on the fact that the surgical treatment of such lesions brings significant relief from pain as well as restored function of the affected limb [7, 18, 22]. A retrospective study of ninety-six patients [11, 21]. However, no uniform surgical procedure has been established. Some authors recommend resection or curretage of the deposit and its filling with bone cement and subsequent performance of stable osteosynthesis of the fracture using the intra-marrow nail or plate [3, 19]. On the other hand, some authors indicate that plain stabilisation of the pathological fracture of the long bone in myeloma deposit using a stable osteosynthesis supplemented with systemic therapy leads to the healing of the fracture [9, 27].
At our site, we share the same opinion in accordance with the Czech Myeloma Group. In the case of pathological fractures of long bones in diagnosed patients with MM we do not perform resection of deposits and replacement with bone cement and we do not perform the biopsy of the bone deposits either. A long bone fracture localised in the area of metadiaphysis is primarily stabilised using the intra marrow nail. In the event of epiphyseal position we choose stabilisation using an angle stable plate. In respect of type 31 B and C proximal femoral fractures we indicate total endoprosthetic implant or cervicocapital prostheses in patients with expected survival shorter than 2 years. The surgical procedure performed by us does not exclude simultaneous administration of systemic MM therapy or radiotherapy of the osteolytic deposits. With the said procedure, we achieved the healing of the fracture in 97 % of the patients. We can attribute this to significant progress in the MM pharmacotherapy as well.
New targeted drugs such as proteasom inhibitors, immunomodulation therapy or monoclonal antibodies are highly effective and their spectre of adverse effects differs from that of conventional cytostatics that interfere non-selectively with the cellular proliferation [24, 25]. The above-mentioned procedure cannot be applied in patients with solid tumours and metastatic affection of long bones because healing of the pathological fracture cannot be expected during the chemotherapy [16, 19]. Complications within the meaning of occurrence of periimplant fractures did not exceed their usual occurrence in the population of patients who had an implant or osteosynthetic procedure [4].
CONCLUSION
Multiple myeloma is a serious hematologic disease, which is very often accompanied by the myeloma bone disease associated with the pain of the affected skeleton and the risk of development of a pathological fracture (it affects up to 50 % of these patients). In patients with MM and pathological fracture of long bones, maintenance of the bones using the stable osteosynthetic or endoprosthetic method is indicated. Myeloma deposit does not have to be resected. The surgical procedure performed does not exclude administration of systemic MM therapy or radiotherapy. The question of myeloma-specific indication criteria after completion of preventive osteosynthesis in the place of the growing deposit with the risk of development of a pathological fracture remains unresolved. This issue requires additional detailed processing.
MUDr. Martin Chovanec
chovanec.martin@fnbrno.cz
Sources
- ADAM, Z., HÁJEK, R., MAJER, J. et al. Mnohočetný myelom a další monoklonální gamapatie. Brno : Masaryk University Press, 1999.
- AITKEN, RCB. Measurement of feelings using visual analogue scales. Proceedings of the Royal Society of Medicine. 1969, Sv. 62, stránky 989–993.
- BARKER, J., BARKER, M., KOTWAL, SY et al. Surgical management of metastatic disease of the proximal part of the femur. J Bone Joint Surg Am. 2014, 96, 2091–2098.
- CAPONE, A., CONGIA, S., CIVININI, R., et al. Periprosthetic fractures: epidemiology and current treatment. Clin Cases Miner Bone Metab. 2017, 14, 189–196.
- DURR, HR, KUHNE, JH, HAGENA, FW et al. Surgical treatement for myeloma of the bone. Arch Ortop Traum Surg. 1997, 116, 463–469.
- FIDLER, M. Incidence of fracture through metastases in long bones. Acta orthop scand. 1981, 52, 623–627.
- FIDLER, M. Surgical treatment for secondary neoplastic fractures. A retrospective study of ninety-six patients. The Journal of Bone & Joint Surgery. 1970, 52, 665–686.
- HOWARD, EL, SHEPHERD, KL, CRIBB, G. et al. The Validity of the Mirels score for predicting impending pathological fractures of the lower limb. Bone Joint J. 2018, 100-B, 1100–1105.
- CHNG, WJ, DISPENZIERI, A., CHIM, CS. et al. International Myeloma Working Group. IMWG consensus on risk stratification in maultiple myeloma. Leukemia. 2014, 28, 269–277.
- International myeloma working group. Myeloma. [Online] [Citace: prosinec. 12 2019.] https://www.myeloma.org/bone-disease.
- ISSACK, PS, BARKER, J., BARKER, M. et al. Surgical management of metastatic disease of the proximal part of the femur. J Bone Joint Surg Am. 2014, 96, 2091–2098.
- KALLMES, DF, COMSTOCK, BA, HAEGERTY, PJ. et al. A randomized trial of vertebroplasty for osteoporotic spinal fractures. N Engl J Med. 2009, 361, 569–579.
- KIVIOJA, AH, KARAHARJU, EO, ELOMAA, I. et al. Surgical treatment of myeloma of bone. Eur J Cancer. 1992, 28, 1865–1869.
- KYLE, RA, Gertz, MA, Witzig, TE et al. Review of 1027 Patients With Newly Diagnosed Multiple Myeloma. Mayo Clin Proc. 2003, 78, 21–33.
- MALUSKOVÁ, D., SVOBODOVÁ, I., KUCEROVA, M. et al. Epidemiology of Multiple Myeloma in the Czech Republic. Klin Onkol. 2017. 30, 35–42.
- MÄRDIAN, S., SCHASER, KD, RUPPERT, M. et al. Metastázová choroba femuru: výsledky ošetření nitrodřeňovým hřebem. Acta Chirurgiae Orthopaedicae et Traumatologiae Čechosl. 2015, 82, 192–197.
- MATĚJOVSKÝ, M., KOFRÁNEK, I., KRYSTLÍK, Z. et al. Riziko zlomenin při osteopatiích nádorů dlouhých kostí. Ortopedie. 2010, 4, 143–149.
- MELTON LJ, KYLE R., ACHENBACH, S. et al. Fracture risk with Multiple Myeloma: A population Based Study. J Bone Miner Res. 2004, 20, 487–493.
- MILLER, BJ, SONI, EE, GIBBS, CP et al. Intramedullary nails for long bone metastases: why do they fail? Orthopedics. 2011, 34, 274.
- MIRELS, H. Metastatic disease in long bones. Clin orthop. 1989, 249, 256–264.
- PAPAGELOPOULOS, PJ, GALANIS, EC, GREIPP, PR et al. Prosthetic hip replacement for pathologic or impending fractures in myeloma. Clin Orthop Relat res. 1997, 341, 192–205.
- PALUMBO, A., ANDERSON, K. Multiple myeloma. N Engl J Med. 2011, 364, 1046–1060.
- POVÝŠIL, C., ŠTEINER, I. et al. Speciální patologie. Praha : Galén Karolinum, 2007.
- ŠTORK, M., KREJČÍ, M., SANDECKÁ, V. et al. Využití nových léků v primoterapii mnohočetného myelomu. Vnitř Lék. 2016, 62, 413–422.
- ŠTORK, M., POUR, L., SANDECKÁ, V. et al. Využití monoklonální protilátky daratumumab v léčbě mnohočetného myelomu. Transfuze hematol dnes. 2016, 22, 230–237.
- TERPOS, E., NTANASIS-STATHOPOULOS, I., DIMOPOULOS, MA. Myeloma bone disease: from biology findings to treatment approaches. Blood. 2019, 133, 1534–1539.
- VAISHYA, R., VIJAY, V., AGARWAL, AK. Healing of pathological fracture in case of multiple myeloma. BMJ Case Rep. 2017, Published online. doi:10.1136/bcr-2016-218672.
Labels
Surgery Traumatology Trauma surgeryArticle was published in
Trauma Surgery

2020 Issue 1
Most read in this issue
- Treatment of Rockwood type III acromioclavicular joint dislocation
- Nailing osteosynthesis of proximal humeral fractures
- Odontoid fracture in the elderly, our therapeutic approach
- Stable osteosynthesis of pathological fracture of long bones in patients with multiple myeloma; retrospective evaluation of the therapy