
Treatment of Rockwood type III acromioclavicular joint dislocation
Authors:
Kateřina Gajdošíková; Radek Veselý
Authors‘ workplace:
Klinika traumatologie, Lékařská fakulta, Masarykova univerzita, Brno, Úrazová nemocnice
Published in:
Úraz chir. 27., 2020, č.1
Overview
The authors in their work present the results of a group of patients, in which the Rockwood type III acromioclavicular joint dislocation was treated conservatively as compared with a group, which was treated by introduction of K-wires with their tension transfixation using tension wire cerclage or Orthocord loop with suture of acromioclavicular (AC) and coracoclavicular (CC) ligaments.
OBJECTIVE: Retrospective evaluation and comparison of the result of the management of Rockwood type III acromioclavicular joint dislocation treated conservatively and using a surgery technique.
MATERIAL AND METHODOLOGY: Retrospective evaluation of pain, scope of movement and normal daily activity according to Constant-Murley Shoulder Outcome Score system after one year from the injury. Also evaluation of the length of total therapy, necessary rehabilitation, cosmetic impact of the treatment and their complications.
RESULTS: From January 2017 to October 2018, 72 Rockwood type III acromioclavicular dislocations were treated in the Trauma Hospital in Brno. 58 of these patients were treated by Ki-wire transfixation and Orthocord loop or tension cerclage with the suture of ligaments; 14 patients were treated conservatively. 82.8 % of the patients treated invasively achieved excellent results (more than 60 points) in the modified Constant-Murley Shoulder Outcome Score system; in the group treated conservatively, 85.7 % of the patients achieved this level.
CONCLUSION: No significant difference between conservative and surgical therapy of the Rockwood type III acromioclavicular joint dislocation has been proved.
Keywords:
Rockwood type III – acromioclavicular joint dislocation
INTRODUCTION
Acromioclavicular joint (AAC) is a joint connection of the lateral end of clavicle with the blade acromion, between which a ligament disk is inserted. The joint capsule is reinforced from the upper side by the acromioclavicular (AC) ligament and the whole joint is stabilised by means of the coracoclavicular (CC) ligament, which connects the coracoid process of the blade with clavicle. This slightly movable joint (amphiarthrosis) participates in movement in the shoulder, particularly in lifting the arm above the horizontal line [4].
Incidence of AAC dislocation is 1.8 per 10,000 inhabitants [5, 17], representing 9–12 % of all shoulder injuries; it is most frequently caused by direct fall over oneʼs shoulder in young people doing sports or by fall on oneʼs stretched limb (indirect mechanism). Men are predominantly affected (8 : 1) [5, 17, 18].
The most globally used classification in clinical practice describing acromioclavicular dislocations is the classification according to Rockwood. In type I there is distension and microruptures of the joint capsule or ligaments, but the continuity of ligaments remains intact, without abnormalities on the X-ray image. Type II is characterised by joint capsule disruption together with AC ligament; CC ligament remains intact. This is manifested on the X-ray image as a vertical subluxation of distal part of clavicle by approx. a half of the bone width. In type III, apart from the joint capsule, both ligaments (AC and CC) are disrupted as well, which is manifested on the X-ray image as a dislocation of clavicle from acromion by more than width of the bone. Besides pain and functional limitation present in all types, this type is clinically accompanied by the Delbetʼs sign. ISAKOS company further suggested subdivision of type III into two subtypes - stable type IIIA, when no dislocation occurs in AAC on the cross-arm in AP projection (Basamani-Alexander) and scapular dyskinesis is not significant, and unstable type IIIB, which is characterised by a shift in AAC on Basamani projection with a therapy-resistant scapular dyskinesis [1].
Scapular dyskinesis is a term including blade function and position disorders where the scapular support of AC and CC ligaments is disrupted. On X-ray image in Basamaniʼs projection it is necessary to look for the asymmetry of medial edge of the blade because any prominence indicated internal scapular rotation and/or anteflection of the blade, which may result in shoulder function disorder [9]. Type IV includes type III with dislocation of clavicle dorsally between the trapezius muscle fascicles, which is shows best on an axial image. Rockwood type V includes type III with separation of the deltoid and trapezius muscle from the distal end of clavicle. X-ray shows an image of significantly extended width of the joint fissure (2 to 3-times the width of bone) with dislocation of the blade in caudal direction. Rockwood type VI includes type V with dislocation of clavicle underneath the coracoid process or acromion, which is manifested by a “negative” CC space on the X-ray image.
In this country, classification according to Tossy is widespread in clinical practice due to its simplicity. Rockwood type I-II is adequate to the Tossy type I-II, Tossy type III includes both types IIIA and IIIB according to Rockwood.
Injuries of AAC type I and II are treated conservatively. The therapy includes relieving of the affected limb in a cravat or fixation with an orthosis for 1–2 weeks, cooling, analgetics, and early rehabilitation. Types IV–VI, on the other hand, are indications for surgery. However, Tossy/Rockwood type III continues to be controversial.
Constant-Murley Shoulder Outcome Score System (CMSOS) is often used to evaluate the results of treatment. This score system with the maximum of 100 points evaluated pain (15 points), normal daily activity (20 points), mobility (40 points) and limb strength (25 points) [3].
The aim of this study retrospective evaluation of clinical results of the set of patients treated in our hospital.
MATERIAL AND METHOD
Method of this observation consisted in retrospective evaluation of patients with acromioclavicular joint dislocation, treated either as outpatients or hospitalized in our hospital during the period of almost two years. Those who had mobility of sensitivity disorder of the injured limb before the injury already, those who did not appear for regular check-ups or visited other facilities, and patients who reported low compliance during the treatment, were excluded from the set.
X-ray images in AP projections were evaluated in individual periods after the injury, but the standard follow-up was 1 year, when the patients were invited for a targeted check-up. Shift in the area of acromioclavicular joint was measured by means of the ruler function of the PACS software used in our hospital to display X-ray images. On these X-ray images, we also observed the presence of calcification/ossification of the CC or AC ligament, osteolysis or ACC osteoarthritis.
Clinical evaluation consisted in objective evaluation of the mobility range of the affected limb and subjective perception of the patient upon completion of the treatment after one year from the injury during the outpatient visit using the Constant score system modified by us. By default, in our set we did not evaluate the strength of the affected limb; therefore, we had to modify the resulting evaluation scale accordingly. With regard to the absence of muscle strength evaluation, full number of points was determined to be 75. Excellent results were achieved when the score from 60 to 75 points was achieved; good results were achieved with 48 to 59 points, satisfactory with 38–47 points and unsatisfactory where less than 37 points were achieved.
With regard to the custom practice at our site, most dislocations were managed invasively, i.e. using the open access with introduction of Ki-wires and their tension cerclage transfixation or with the Orthocord loop with suture of AC and CC ligaments. Selection of method depended on preferences of the operating surgeon only - After the surgery, the operated limb was fixed with a cravat suspension for 2 weeks. After 2 weeks the patients started exercising the affected limb up to full mobility depending on pain. The metal material was extracted 10–24 weeks from fixation (11 weeks being the median of extraction) in all patients managed by surgery. The patients started exercising the injured limb after extraction of the metal. Where the patients were not able to do this alone or this therapy had no effect, targeted professional rehabilitation was indicated. Patients were treated conservatively rather on their own request, when they refused the surgery, than on the surgeonʼs recommendation. Fixing with orthosis was for 1–2 weeks individually, with subsequent gradual exercising or targeted professional rehabilitation, as appropriate.
The need of professional rehabilitation, total duration of the treatment and cosmetic impact of the therapy were evaluated as well.
RESULTS
From January 2017 to October 2018, 72 Rockwood type III acromioclavicular joint dislocations were treated in the Trauma Hospital in Brno (n=72). Vast majority of the patients were men (61 men and 11 women). The age average of this set was 39 years (18–65 years). The most frequent mechanism of injury was a fall on the shoulder during sports activity.
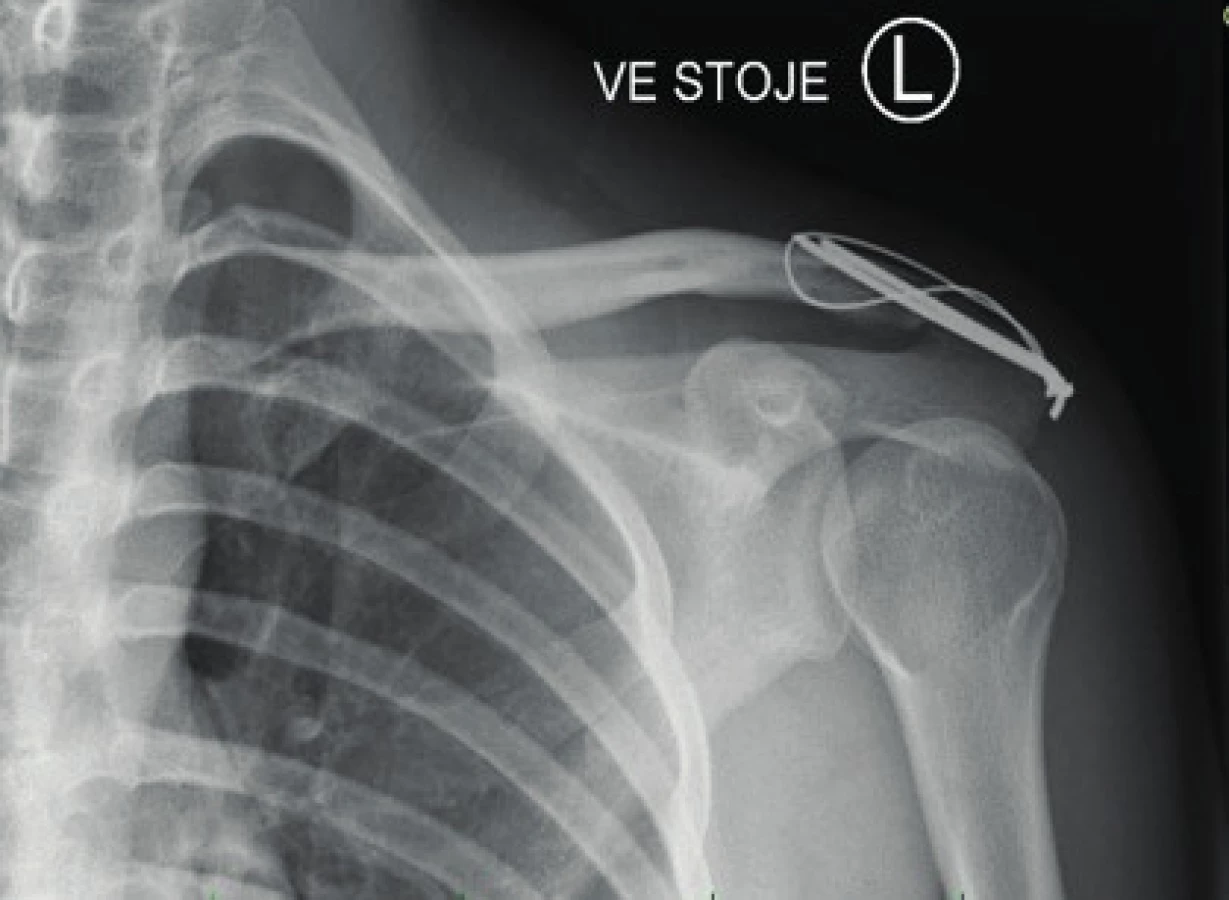
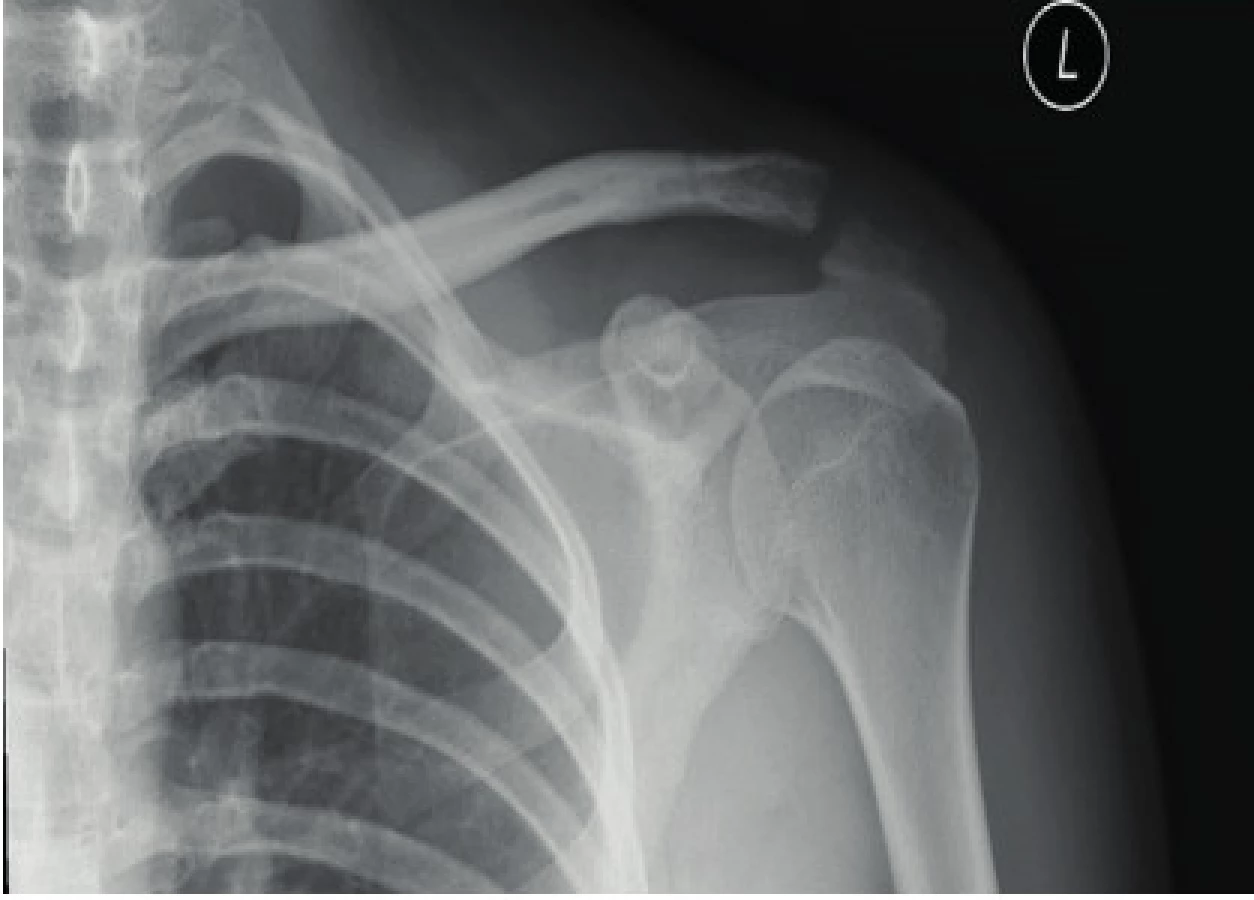
58 out of the total of 72 of AC dislocations were treated by surgery. Orthocord loop for transfixation of Ki-wires was used in 24 cases; tension cerclage transfixation was used in 34 cases. 14 patients were treated conservatively (Fig. 4 and 5).



In the group of patients managed by Orthocord loop transfixation, 14 patients (58.3 %) were satisfied with the treatment upon completion of the treatment already, i.e. before extraction of the metal material - subjectively they did not feel any limitation of mobility or pain limiting them in their normal daily activities. In three of these patients, mild deterioration of the X-ray image in AP projection occurred in the sense of shift of the clavicle by several millimetres in respect of the acromion. However, these changes resulted in no clinical response. The remaining 10 patients (41.6 %) shortly before extraction of the metal experienced pain or reduced mobility as compared with condition before the injury. 3 of these patients (12.5 %) experienced improvement of mobility after extraction of the metal material. Rehabilitation therapy was indicated for the remaining 7 patients (29 %) who did not experience improvement even after extraction. Considerable improvement to full satisfaction and improvement of mobility up to the maximum occurred in 4 patients (rehabilitation effect in 57.1% patients) at the end of 1–2 rehabilitation cycles. 3 patients (12.5 %) subjectively experienced difficulties even one year from the injury.
According to the Constant-Murley Shoulder Outcome Score system completed after one year from the injury, 21 patients (87.5%) achieved excellent results. After completion of the therapy, 3 patients complained about intermittent pain under load or mobility limitation – 2 of them achieved good results (CMSOS 57) and one achieved satisfactory results (CMSOS 45). Satisfactory result was achieved by a young patient pursuing the climbing. He was able to do everyday activities without problems, but he was limited by pain when he was climbing. Total duration of the treatment was14.8 weeks, in this fixation took 3 weeks as a standard. On X-ray in AP projection, Ki-wire migration was reported in two case and subluxation at ACC in two cases (change in the CC space by + 6 mm on the average). Operation wound infection complications occurred in 1 patient (4.2 %), where dissolution of the wound, therapy with antiseptic covers, and subsequent resuture were needed. The other operation wounds healed per primam. Hypertrophic scar occurred in one case. 4 patients were not satisfied with the shape of the scar (including the patient with the hypertrophic scar).

34 patients were operated using the tension cerclage. 18 (52.9 %) were subjectively without mobility limitations or pain before extraction of the osteosynthetic material already. Out of the 16 patients who experienced limited mobility before extraction, mobility regained its maximum after the extraction in 10 patients (29.4 %); the 2 out of the remaining 6 patients (5.9 %) were positively influenced by subsequent rehabilitation. Thus, 4 patients (11.8 %) in total had subjectively permanently reduced mobility of the affected limb or experienced intermittent pains, particularly under strain. After one year from the injury using the clinical evaluation with Constant-Murley Shoulder Outcome Score system, excellent results (CMSOS 73) were achieved by 27 patients (79.4 %). Good results (CMSOS 55) were achieved by 4 patients (11.8 %), satisfactory results (CMSOS 44) by 2 patients (5.9 %), and unsatisfactory results (CMSOS 35) by 1 patient (2.9 %). Total length of therapy was 16.7 weeks on the average, fixation period was 3 weeks as a standard. On X-ray in AP projection, Ki-wire migration was observed in 3 cases at the time just before extraction, subluxation at the ACC in one patient (change of the CC space by + 8mm) after one year from the injury. Wound infection was reported in 3 cases (8.8 %); 5 patients were not satisfied with the shape of the scar – however, hypertrophic scar was not present in any of these cases, it was a subjective evaluation only.
Therefore, in the group of patients who were operated using any method (58 in total), 48 patients (82.8 %) achieved excellent results, 6 patients (10.3 %) achieved good results, 3 patients (5.2 %) achieved satisfactory results, and 1 patient was not satisfied (1.7 %) according to scoring system upon full completion of the therapy including the extraction of osteosynthetic material and rehabilitation therapy. Targeted rehabilitation outpatient therapy was indicated in 21.9 % of patients. The average length of therapy was 15.8 weeks with fixation for 3 weeks. Infection in wound occurred in 4 cases and 9 patients were subjectively dissatisfied with the shape of the scar.
On the other hand, in the group of patients with conservative treatment, 12 patients out of 12 (85.7 %) achieved the excellent level (CMSOS 69). Targeted rehabilitation therapy was necessary for full healing and mobility improvement in 4 of these patients (28.6 %). Rehabilitation therapy was also indication in the remaining 2 patients (14.3 %) - 1 patient achieved a good result (CMSOS 48) and one patient achieved a satisfactory result (CMSOS 63). In total, rehabilitation was necessary in 6 patients (42.9 %). Total average duration of duration was 11.6 weeks, duration of fixation was 1–2 weeks, individually depending on the pain experienced by the patient. 8 patients reported that they mind the cosmetic impact of the therapy - disfiguration in the area of AC joint.
DISCUSSION
The therapy of Rockwood AAC-type III dislocation is amply discussed in the literature and continues to be controversial.
The definite advantage of conservative therapy is represented by the absence of even two invasive procedures (primary stabilisation with necessary extraction of the metal in the interval of approx. 8–10 weeks from primary stabilisation) and the possibility of early rehabilitation with overall reduction of the healing time. Disadvantage is represented by the inability to achieve the anatomic position with persisting deformity in the AAC area, which may result in potential pain, arthritis, instability and weakness of the limb [18] together with negative cosmetic impact. Operation treatment entails the risks of infectious complications during the healing of the operation wound, osteolysis, ossification of CC and AC ligaments and ACC osteoarthritis, pain, limited function or development of hypertrophic scar [17, 18].
Numerous studies deal with evaluation of individual operating techniques with tendency to mini-invasiveness; considerable number of studies however deals with conservative therapy. It is a trend of most of the European sites to operate these injuries; in America, on the other hand, rather the conservative procedure is preferred [11]. Inconsistent consensus is obvious in a broad range of evaluation methods - randomised prospective or retrospective studies or theoretical questionnaire examinations. According to Tang [23], there is no significant difference between the operation and conservative therapy in respect of the pain, weakness, post-traumatic arthritis or unsatisfactory strength. Korsten [11] compared patients from several already published studies by various authors dealing with this issue. On several scientific portals he searched all studies that compared the operating and conservative therapy for the Rockwood ACC III type dislocation; he excluded duplicate articles, publications in other than English or German language, articles in which original data of patients were not presented or where veterinary studies were included, where it was not about Rockwood type only, or the article was not available in a full-text version. Out of the original 5,815 published articles from 5 scientific resources, only 8 met these criteria. The author thus evaluated a total of 142 patients treated operatively and 105 patients treated conservatively. Limitation of this study was the inability to perform summary statistic evaluation of the obtained data because each of the individual authors used a differed scoring system. However, most of these studies did not prove any significant difference between the individual groups. Only Gstettner proved a significant difference in favour of the operated group (excellent results) as compared with the conservative therapy (good results). Domos [6] dealt with this issue too; he distributed a targeted one-page web questionnaire to all consultants of the British Elbow and Shoulder Society. The questionnaire contained the level of experience, preferred therapy for this injury, indications for operation and preferred method for symptomatic patients in various subgroups (top-level athletes, active people, or depending on age or sex). In total, the questionnaire was completed by 137 specialists. All of them, i.e. 100 % reported that they would treat type III conservatively using the cravat suspension fixation for up to 4 months or a bit less in patients over 65. 86 % of the respondents started a targeted rehabilitation. The respondents were also asked to indicate the time elapsed from the injury after which they would operate this injury in the event of persisting symptomatology. Functional damage of limb, condition of limb before injury, pain and the patients´ request showed to be the factor influencing the decision regarding the intervention. Individual subgroups or sex, on the other hand, have no impact on this decision. The average duration of surgical intervention, with persisting symptomatology, was 3.8 months from the injury. It also became apparent that more experienced specialists (with more than 10 years of experience in this discipline) are more reserved than their younger colleague who tend to operate earlier.
Also, 69 % of team doctors of the American baseball players would initiate conservative therapy first; however, 31% would suggest immediate operation [16]. 80 % of top-level athletes, who experienced this injury in their dominant limb and received conservative treatment, achieved normal function of the limb and they were without pain. 90 % had full mobility range. On the other hand, 92 % of the operated baseball players did not perceive any limitation of function or pains and had full mobility range [16].
We decided, based on these studies, to evaluate the set of our patients, because our site tends to operate these injuries. Even in our set, in correlation with the above-mentioned studies, we did not prove after one year from the injury any significant difference between the group receiving the operation technique treatment and the group receiving the conservative treatment. Evaluation of a group of patients using the Constant score system modified by us is incomplete, but with regard to inclusion of the subjective part sufficient for clinical evaluation of the therapy. Subjective perception contributes to the patients´ satisfaction more than objectively verified mobility orange or absence of pain. Incomplete mobility during normal daily activity does not have to be a problem; on the other hand, difficulties of a patient, in who full mobility and absence of pain in daily activities were measured, may manifest under stress only, thus considerably worsening the overall results.
Limitation of this study is a small set of conservatively treated patients because the trend of our site is to treat the Rockwood type III invasively. Low capture of calcification/ossification of the CC or AC ligament, ACC osteolysis and osteoarthritis is given by the absence of long-term results (the last X-ray image was made upon the entrance check-up one year after the injury). These results could have been in some degree biased also by the absence of distinguishing between the stable and unstable type IIIA and IIIB according to ISAKOS [1].
Rehabilitation therapy was indicated in a smaller number of patients than indicated in respect of this injury in the published studies. Our site does not indicate this treatment across the board; it is indicated only in patients who are not able to work their limb out by themselves. Increased targeted rehabilitation therapy could therefore result in even better functional results.
Total duration of the treatment is shorter for the conservative treatment method (11.6 weeks) - the fixation time is shorter (1–2 weeks) with early workout depending on pain as compared with the operation management (15.8 weeks), when the limb remains fixed for 3 weeks, with subsequent fixation for a few days after the extraction.
Probably the biggest difference is in the degree of cosmetic impact of the treatment - in the conservative therapy, disfiguration in the ACC area remains in all cases and 71.4 % of the patients classified it as obtrusive. The scar is present in all cases of the operating treatment; however, only 15.5 % of the patients classified it as obtrusive. Cosmetic impact of the operating method is generally perceived as the “necessary evil” and therefore its perception is not so negative.
Our site is currently changing the therapeutic strategy - we therefore start the treatment of predominant majority of patients with Rockwood type III injury in a conservative manner. If the pains and limited mobility of the shoulder persist even after 4 weeks, we will offer the operation to young patients.
CONCLUSION
In our study we did not prove any significant difference between the conservative and operating treatment of the Rockwood type III dislocation of acromioclavicular joint – 82.8 % of the patients treated by some of the invasive techniques and 85.7 % of all the conservatively treated patients achieved more than 60 points in the Constant score system modified by us, which means the excellent stage.
In conservative therapy, the need of targeted professional rehabilitation is up to twice as frequent in order to achieve good functional results.
Total length of the treatment is shorter by approx. 4 weeks with the conservative therapy - the patients return faster to their normal everyday life with all social and economic consequences.
Conservative therapy has a worse cosmetic impact - disfiguration in the area of acromioclavicular joint is subjectively taken worse than post-operation wound.
Doc. MUDr. Radek Veselý, Ph.D.
E-mail: ves.radek@seznam.cz
Sources
- BEITZEL, K., MAZZOCCA, AD, BAK, K. et al. Upper extremity committee consensus statement on the need for diversification of the Rockwood classification for acromioclavicular joint injuries. Arthroscopy. 2014, 30, 271.
- CALVO, E., LOPEZ-FRANCO, M., ARRIBAS, IM. Clinical and radiologic outcomes of surgical and conservative treatment of type III acromioclavicular jointinjury. J Shouder Elbow Surg. 2006, 15, 300–305.
- CONSTANT, CR, MURLEY, AHG. A clinical method of functional assessment of the shoulder. Clin Orthop. 1987, 214, 160–164.
- ČIHÁK, R. Anatomie. Třetí, upravené a doplněné vydání. Praha: Grada, 2016. 552 s. ISBN 978-80-247-3817-8
- CHILLEMI, C., FRANCESCHINI, V., DEI GIUDICI, L., et al. Epidemiology of isolated acromioclavicular joint dislocation. Emerg Med Int. 2013, doi:10.1155/2013/171609
- DOMOS, P., SIM, F., DUNNE M., White A. Current practice in the management of Rockwood type III acromioclavicular joint dislocations-National survey. J Orthop Surg. 2017, 25, 1–6.
- FRASER-MOODIE, JA, SHORTT, NL, ROBINSON, CM. Injuries to the acromioclavicular joint. J Bone Joint Surg Br. 2008, 90, 697–707.
- HORST, K., GARVING, C., THOMETZKI, T. Comparative study on the treatment of Rockwood type III acute acromioclavicular dislocation: Clinical results from the TightRope® technique vs. K-wire fixation. Orthop Traumatol Surg Res. 2017, 103, 171–176. doi: 10.1016/j.otsr.2016.
- KIBLER, WB, SCIASCIA, A. Current concepts: Scapular dyskinesis. Br J Sports Med. 2010, 44, 300–305.
- KIM, S., Blank, A., Strauss, E. Management of type 3 acromioclavicular joit dislocations: current controversies. Bull Hosp Jt Dis. 2014, 72, 53–60.
- KORSTEN, K., GUNNING, AC, LEENEN LPH. Operative or conservative treatment in patients with Rockwood type III acromioclavicular dislocation: a systematic review and update of current literature. Int Orthopaedics. 2014, 35, 697–703. ISSN 0341-2695
- LI, X., MA, R. BEDI, A., DINES, D., et al. Management of Acromioclavicular Joint Injuries. J Bone Joint Surg. 2014, 96, 71–84.
- LIU, JN., GARCIA, GH, WEEKS, KD, ET AL. Treatment of Grade III Acromioclavicular Separations in Professional Baseball Pitchers: A Survey of Major League Baseball Team Physicians. Am J Orthop. 2018, 47, 7.
- LONGO, UG, CIUFFREDA, M., RIZZELLO, G. et al. Surgical versus conservtive management of Type III acromioclaviulalr dislocation: a systematic review. Br Med Bull. 2017, 122, 31–49.
- MAZZOCCA, AD, ARCIERO, RA, BICOS J. Evaluation and treatment of acromioclavicular joint injuries. Am J Sports Med. 2007, 35, 316–329.
- MCFARLAND, EG, BLIVIN, SJ, DOEHRING, CB. et al. Treatment of Grade III acromioclavicular separations in professional throwing athletes: results of survey. Am J Orthop (Belle Mead NJ). 1997, 26, 771–774.
- RIAND, N., SANDOWSKI, C., HOFFEMEYER, P. Acute acromioclavicular dislocations. Acta Orthop Belg. 1999, 65, 393–403.
- SEONG-HUNG, K., KYOUNG-HWAN, K. Treatment of Rockwood Type III Aomioclavicular Joint Dislocation. Clin Shoulder Elbow. 2018, 21, 48–55. ISSN 2383-8337
- SIMOVITCH, R., SANDERS, B., OZBAYDAR, M. et al. Acromioclavicular joint inuries: diagnosis and management. J Am Acad Orthop Surg. 2009, 17, 207–219.
- SMITH, TO, CHESTER, R., PEARSE, EO et al. Operativev versus non-operative management following Rockwood grade III acromioclavicular separation: A meta-analysis of the current evidence base. J Orthop traumatol. 2011, 12, 19–27. doi: 10.1007/s10195-011-0127-1.
- SPENCER, EE, JR. Treatment of grade III acromioclavicular joint injuries: a systematic review. Clin Orthop Relat Res. 2007, 455, 38-44.
- TAMAOKI, MJ, BELLOTI, JC, LENZA, M. et al. Surgical versus conservative interventions for treating acromioclavicular dislocation of the shoulder in adults. Cochrane Database Syst. Rev. 2010, 8.
- TANG, G., ZHANG, Y., LIU, Y. et al. Comparison of surgical and conservative treatment of Rockwood type-III acromioclaviculr dislocation: A meta-analysis. Medicine. 2018, 97, 4.
- WENDSCHE, P., VESELÝ, R. Traumatologie. Praha: Galén, 2015. 344 s. ISBN 987-80-7492-211-4.
- ŽVÁK, I. Traumatologie ve schématech a RTG obrazech. Praha: Grada Publishing, 2006. 207 s. ISBN 80-247-1347-0.
Labels
Surgery Traumatology Trauma surgeryArticle was published in
Trauma Surgery

2020 Issue 1
Most read in this issue
- Treatment of Rockwood type III acromioclavicular joint dislocation
- Nailing osteosynthesis of proximal humeral fractures
- Odontoid fracture in the elderly, our therapeutic approach
- Stable osteosynthesis of pathological fracture of long bones in patients with multiple myeloma; retrospective evaluation of the therapy