
SURGICAL CORRECTION OF LABIA MINORA HYPERTROPHY, A PERSONAL TECHNIQUE
Authors:
S. Di Lorenzo; B. Corradino; M. Cillino; M. Hubova; A. Cordova
Authors‘ workplace:
Dip. Discipline Chirurgiche, Oncologiche e Stomatologiche, sez. Chirurgia Plastica, Università di Palermo, Italy
Published in:
ACTA CHIRURGIAE PLASTICAE, 59, 2, 2017, pp. 60-64
INTRODUCTION
The labia minora are two muco-cutaneous folds situated between labia majora. The hypertrophy of labia minora, originally described as protuberant tissue projecting beyond the labia majora, is a congenital or acquired pathological condition whose aetiology is not well known and in some cases may be due to chronic inflammation, exposure to exogenous androgens, use of urinary catheters in patients with spinal paralysis, specific sexual activities or continuous manual stretching in some primitive cultures 1,2. This alteration of the anatomical shape of labia minora often causes discomfort for patients. The reasons why these women come to the doctor may be different. The protrusion of hypertrophied labia minora outside the vulvar vestibule, perceived as disgraceful by the patients, represent the most frequently reported motivation for consultation. There seems to be a correlation between the degree of hypertrophy and the incidence of resulting discomfort 3. Young girls usually describe a discomfort with perception of a “bulge” in the underwear or bathing suite. They need to fold up and push the labia into vagina, in order to reduce the bulge 3. Usually both labia minora are hypertrophic. More rarely hypertrophy is unilateral.
It is difficult to determine when a labium requires surgical correction. Friedrich 4 considers normal a labium that is less than 5 cm in width when pulled anteriorly. Other authors suggest that the normal width of labia minora should be less than 3–4 cm. The labia minora hypertrophy was classified by Franco 5 into grade 1 through 4 depending on the protrusion of the labia minora through the labia majora: grade 1, <2cm; grade 2, from 2 to 4 cm; grade 3, from 4 to 6 cm; and grade 4. Some patients associate the normally darker, corrugated appearance of the labial edge with an “aged” appearance and prefer to have it removed, regardless of its length or width. Chang et al described in 2013 a new classification system with four classes of labia protrusion based on size and location. 6 The labia minora should be fully extended and measured from midline to the lateral free edge during the physical examination. If the labia measure more than 4–5 cm, surgical correction can be planed but in the majority of cases the symptoms described by the patients are more important than measurements alone. In literature different techniques of labia minora reduction are described 7–15. The most popular are:
- The edge excision technique as described by Capraro 16 and Felicio 17, which simply involves amputation of protuberant tissue, thus removing the dark, corrugated labial edge.
- The deepithelialization of the central portion of the medial and lateral surface of each hypertrophic labium and the direct suture of the margins with an absorbable monofilament suture 4/0, introduced by Choi and Kim 18.
- The wedge resection of the central portion of hypertrophic labia.
- The longitudinal amputation of the hypertrophic segment through double w-shaped interdigitated complementary incisions. It is indicated in cases of severe hypertrophy. The interdigitated suture avoids the problem of scar retraction of a linear suture 19.
- The superior pedicle technique with inferior wedge resection as described by Alter (20) and modified by Rouzier et al 21.
- Laser labioplasty with ablative lasers (Nd Yag). 22
The authors present their experience with labioplasty described by Alter and Rouzier plus lipofilling of the labia majora.
The association of labioplasty and lipofilling is described here for the first time.
MATERIALS AND METHODS
Between 2005 and 2014, 27 patients underwent surgical reduction of the labia minora in our institute (Table 1). Surgical treatment was requested by 6 patients in order to correct the hypertrophy with related functional problems and to improve labia minora appearance. The reasons for surgical treatment varied and were as follows: interference with sexual intercourse; poor hygiene; difficulty wearing tight-fitting pants; difficulty performing sporting activities such as cycling; aesthetic complaints.
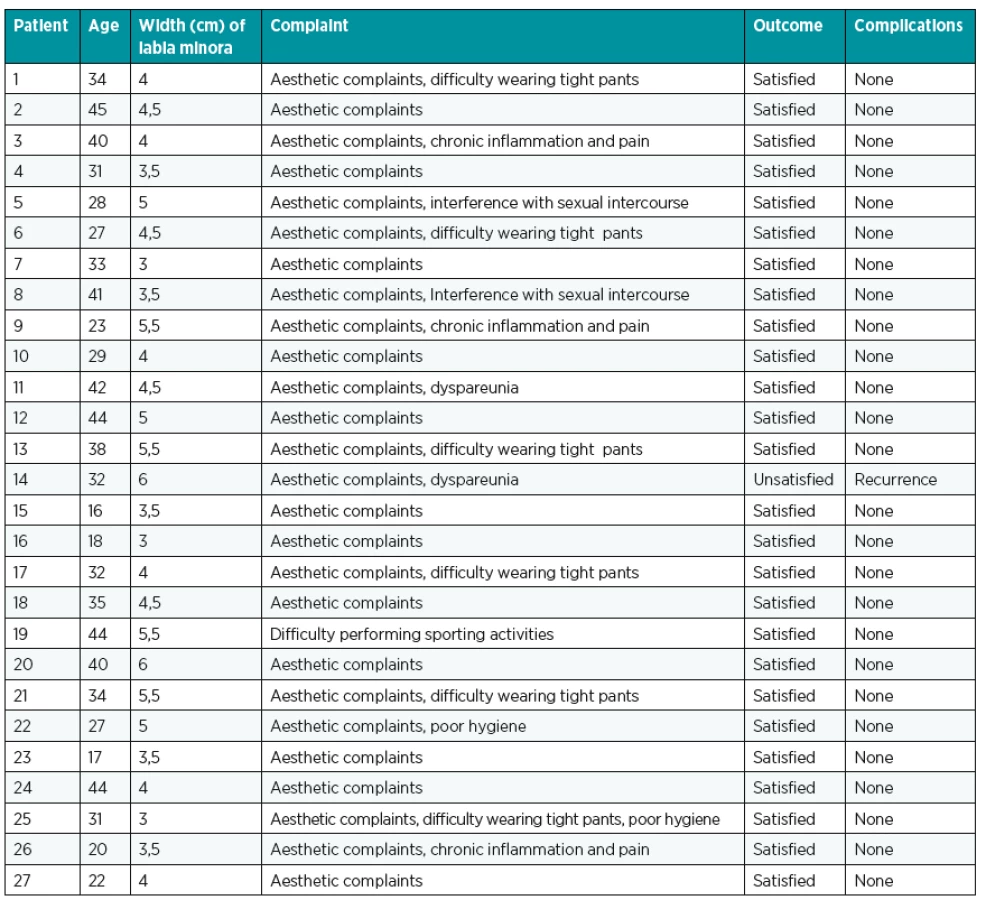
Regarding aetiology, all patients had congenital labia minora hypertrophy. All patients reported worsening of hypertrophy over the years and complained of the aged appearance of their external genitalia. The surgical procedure was bilateral in 26 patients and unilateral in one patient. The average age of the patients was about 32 years (from 16 to 45).
The labia minora of all patients measured 4 to 6 cm in width and thus were grade 3–4 according to the classification of Franco. In all patients the wedge resection of labia minora was associated with lipofilling of labia majora. The aim of the surgery was to achieve coverage of the labia minora with labia majora.
All procedures were performed with sedation and small amount of local anaesthesia, in order to avoid modification of the shape of labia minora before incision and to minimize the discomfort of the patients. In the operating room, patients were placed in lithotomic position. The labia were fully extended and measured. The inferior wedge was marked. The angle and the extent of the wedge vary, depending on the tissue excision and the cutaneous-mucosal laxity. After the infiltration with local anaesthetic plus adrenaline, the inferior wedge resection was performed leaving a superior pedicle flap with a rich blood supply, as described by Altier and Rouzier. Haemostasis is easily achieved; the superior pedicle labial flap is gently spread and sutured inferiorly without tension with absorbable interrupted stitches. Furthermore, care must be taken to avoid wide undermining and haemostasis near the base of the superior flap because the vascular supply comes from this region. Surgery does not require the placement of a urinary catheter (two cases only) or vaginal packing, or the administration of systemic antibiotic therapy. Patients were discharged home the same day of the surgery; they were seen after a week to change the dressing. Postoperative care include perineal hygiene and analgesic. Postoperative pain was reported by 8 patients. It is usually treated with NSAID (nonsteroidal anti-inflammatory drugs) at least for one week. Most of the patients complained of burning sensation for about ten days. Frequent washing with antiseptic solution and cold water relieved this symptom. Wound dehiscence was observed in 3 patients. Only one patient required surgical correction under local anaesthesia. No infection was observed. All patients reported post-operative dyspareunia (the pain lasted for up to 5 weeks).
The wedge resection of labia minora was associated with lipofilling of labia majora in order to protect and cover the labia minora (Fig. 1). Lipofilling of the labia majora is a technique of external genitalia rejuvenation. The adipose tissue was harvested from the abdominal region by means of liposuction technique. The surgeon chose abdominal region because of the quantity of fat and the simplicity of the technique. Donor sites were infiltrated with tumescent solution, and fat was harvested using a 3-mm Luer-lock cannula under low pressure in 20 ml syringes. Fat was then collected in 10 ml syringes, and oil and serum were decanted before centrifugation. The harvested fat samples were centrifuged at 3000 rpm for 2–4 minutes. The goal was to obtain a homogeneous “paste” that could be easily and predictably injected. Oil and serum were again fractionated and decanted. Viable fat cells were placed in 10 ml syringes in preparation for injection. Less fibrous fat has better flow characteristics, permitting smoother infiltration.

It is important to be aware of the flow characteristics of the fat, which is injected to prevent irregularities, and to ensure that specimens of similar quality are used symmetrically. About 35-50 ml of adipose tissue are injected on the free edge of every labium major through a single skin incision located in the vulva.
The labia majora increase in volume and firmness, cover and protect the labia minora, which are surgically reduced (Fig. 2–5).




RESULTS
The mean follow up was 1 year. All patients reported an improvement in comfort aesthetically, when wearing close-fitting clothes and improvement in their sexuality. In one case we recorded a “recurrence” with an increase of labia minora width, still lower than the preoperative situation but greater than the immediate postoperative status (Fig. 6). Probably this is due to the manual stretching of the patient during the days following the operation, which led to a dehiscence of the sutures and a secondary wound healing.

DISCUSSION
The high degree of satisfaction reported by the patients support the use of this procedure. The surgery is short-lived, can be performed under sedation and local anaesthesia as outpatient surgery, does not require urinary catheterization or vaginal packing and helps to improve the quality of patients’ life.
Careful haemostasis and personal postoperative hygiene reduce the incidence of immediate complications such as a hematoma, wound dehiscence and infections.
Late complications described in literature are the retraction of the scar, neuroma-like hypersensitivity and relapse. The scarring and retraction with consequent advancement of the rear fork and vaginal narrowing of the introitus is a rare complication. In most cases it happens due to a technical error of re-approximation of the skin flaps to the rear fork. In our series of patients, scarring was not significant or symptomatic and did not alter the final appearance of the labia minora. The risk of flap necrosis is minimal with this technique, considering the labia vascularization 23.
The recurrence rate is very low and occurs practically only in patients who continue to perform mechanical stretching of the resected lip (1 patient in our series). The wedge resection preserves the free edge of labia minora, so its natural appearance and sensitivity. In cases of large hypertrophies, which extend posteriorly, resection should be limited and should not extend too far posteriorly to avoid that the scars alter the vaginal introitus causing persistent discomfort and post-operative pain. In our cases, associated with the wedge resection of labia minora, the lipofilling of the labia majora helps to protect the labia operated but still hypertrophic in its posterior part. The increase in volume of the labia majora not only protects and covers the labia, but also greatly improves the aesthetic appearance of the vulvar region, giving a greater firmness and a more youthful appearance.
CONCLUSIONS
Reduction of the labia minora hypertrophy with conservative techniques that preserve the colour and the natural contour of the labia minora allow achieving excellent results in terms of aesthetics and functionality. Despite there was no technique described in literature to be superior to the others with regards to the outcomes and complication rate, labioplasty with inferior wedge resection and superior pedicle flap in our experience provides a better aesthetic result by preserving the pigmented free edge of the labium, its sensibility and vascularization with a low rate of complications and the simple lipofilling of labia majora allows to preserve and protect the labia minora through a volumetric increase of the labia majora. The surgical procedures in almost all cases yielded results, that were satisfactory from the aesthetic point of view and exceptional from the functional point of view, allowing the patients to perform normal physical and sexual activity.
Acknowledgment: The authors declare that they have no conflicts of interest to disclose.
Corresponding author:
Sara Di Lorenzo, M. D., PhD.
via del Vespro 129
90127 Palermo, Italy
E-mail: dilsister@libero.it
Sources
1. Hailparn TR. What is a girl to do?: the problem of adolescent labial hypertrophy. Obstet Gynecol. 2014 May;123 Suppl1 : 124S - 5S.
2. Heller DS, Kuye OO. Recurrent hypertrophy of the labia minora: a hormonally related lesion possibly related to fibroepithelial stromal polyps of the vulva. J Low Genit Tract Dis. 2011 Jan;15(1):69-70.
3. Trichot C, Thubert T, Faivre E, Fernandez H, Deffieux X. Surgical Reduction of Hypertrophy of labia minora. Int J Gynaecol Obstet. 2011 Oct;115(1): 40-3.
4. Freidrich EG. Vulvar Disease, 2nd ed, WB Saunders, Philadelphia 1983.
5. Franco T, Franco D. Hipertrofia de Ninfas. J Bras Ginecol. 1993;103 : 163–165.
6. Chang P, Salisbury MA, Narsete T, Buckspan R, Derrick D, Ersek RA. Vaginal labiaplasty: defense of the simple “clip and snip” and a new classification system. Aesthetic Plast Surg. 2013 Oct;37(5):887-91.
7. Ellsworth WA, Rizvi M, Lypka M, et al. Technique for labia minora reduction: an algorithmic approach. Aesth Plast Surg. 2010;34 : 105-110.
8. Triana L, Robledo AM. Refreshing labioplasty techniques for plastic surgeon. Aesth Plast Surg. 2012;36 : 1078-1086.
9. Kelishadi SS, Elston JB, Rao AJ, et al. Posterior wedge resection: a more aesthetic labiaplasty. Aesthet Surg J. 2013 Aug 1;33(6).847-53.
10. Gress S. Composite Reduction Labiaplasty. Aesth Plast Surg. 2013;37;674-683.
11. Munhoz AM, Filassi JR, Ricci MD, et al. Aesthetic labia minora reduction with inferior wedge resection and superior pedicle flap reconstruction. Plast Reconstr Surg. 2006;118 : 1237.
12. Reddy J, Laufer MR. Hypertrophic labia minora. J Pediatr Adolesc Gynecol. 2010;23 : 3.
13. Jothilakshmi PK, Salvi NR, Hayden BE, Bose-Haider B. Labial reduction in adolescent population-a case series study. J Pediatr Adolesc Gynecol. 2009 Feb;22(1):53-5.
14. Hodgkinson DJ, Hait G. Aesthetic vaginal labioplasty. Plast Reconstr Surg. 1984;74 : 414.
15. Laufer MR, Galvin WJ. Labia hypertrophy: a new surgical approach. Adolesc Pediatr Gynecol. 1995;8 : 39-41.
16. Capraro VJ. Congenital anomalies. Clin Obstet Gynecol 1971;14 : 988-1012.
17. Felicio Y. Chirurgie Intime. La Ver Chir Esth Lang Franc. 1992;XVII(67):37-43.
18. Choi HY, Kim KT. A new method for aesthetic reduction of labia minora (the deepithelialized reduction of labioplasty). Plast Reconstr Surg. 2000 Jan;105(1):419-22.
19. Maas SM, Hage JJ. Functional and aesthetic labia minora reduction. Plast Reconstr Surg. 2000;105(4):1453-1456.
20. Alter GJ. A new technique for aesthetic labia minora reduction. Ann Plast Surg. 1998 Mar. 40(3):287-90.
21. Rouzier R, Sylvestre CL, Paniel BJ, Haddad B. Hypertrophy of labia minora: experience with 163 reductions. Am J Obstet Gynaecol. 2000 Jan;182 : 35-40.
22. Pardo J, Solà V, Ricci P, Guilloff E. Laser labioplasty of labia minora. Int J Gynaecol Obstet. 2006;93 : 38.
23. Georgiou CA, Benatar M, Dumas P, et al. A Cadaveric Study of the Arterial Blood Supply of the Labia Minora. Plast Reconstr Surg. 2015 Jul;136(1):167-178.
Labels
Plastic surgery Orthopaedics Burns medicine TraumatologyArticle was published in
Acta chirurgiae plasticae

2017 Issue 2
Most read in this issue
- SURGICAL CORRECTION OF LABIA MINORA HYPERTROPHY, A PERSONAL TECHNIQUE
- INTRAOPERATIVE FAT GRAFTING INTO THE PECTORALIS AND LATISSIMUS DORSI MUSCLES-NOVEL MODIFICATION OF AUTOLOGOUS BREAST RECONSTRUCTION WITH EXTENDED LATISSIMUS DORSI FLAP
- COMPLICATIONS OF LOWER EXTREMITY HEMATOMAS IN PATIENTS WITH PRE-INJURY WARFARINE USE
- HAS A GLOMUS TUMOR ALWAYS A QUICK DIAGNOSIS?