
LASER THERAPY OF RETINAL TEARS
Authors:
P. Kristian; D. Cholevík
Authors‘ workplace:
Gemini oční klinika Ostrava
Published in:
Čes. a slov. Oftal., 79, 2023, No. 3, p. 126-133
Category:
Original Article
doi:
https://doi.org/10.31348/2023/18
Overview
Aim: To report the clinical results of treatment of patients with retinal tears or holes, including rhegmatogenous retinal detachment, who were treated primarily with laser retinopexy.
Material and methods: The effect and results of the therapy of patients with one or more retinal tears who underwent therapy with the green laser IQ 532 IRIDEX between December 2019 and August 2022 at our center with a follow-up observation period of at least 3 months were retrospectively evaluated.
Results: A total of 14 eyes of 14 patients were treated by this method during the monitored period. All the tears found were primarily successfully repaired. The overall success rate of prophylaxis of rhegmatogenous retinal detachment was 93% in our cohort. In one patient, subsequent pars plana vitrectomy was required due to the progression of retinal detachment from another biomicroscopically inaccessible hole, which was part of lattice degeneration in the peripheral part of the retina. This pathology was only verified during intraocular surgery. Postoperatively, the retina was attached with a very good anatomical and functional effect. The other patients did not require any adjuvant therapy.
Visual functions improved or remained stable in all patients in the cohort.
The follow-up observation period ranged from 3 to 36 months.
Conclusion: Laser retinopexy is a sparing, safe and effective method of retinal tear therapy. From our clinical experience, the technique is also applicable in the case of partial vitreous hemorrhage or incipient rhegmatogenous detachment.
We did not record any complications of perioperative or postoperative treatment among our patients.
Keywords:
Retinal detachment – laser – retinal tear – photocoagulation – IRIDEX – hemovitreus

INTRODUCTION
Tears (rhegma) and holes are dehiscences of the retinal neuroepithelium throughout its full thickness, enabling the infiltration of intraocular fluid subretinally, and threatening visual functions due to the onset of rhegmatogenous detachment. Holes are rounded, atrophic defects with a low risk of retinal detachment. By contrast, tears occur in the place of vitreoretinal traction, as a rule on the interface of the detached posterior surface of the vitreous body and the vitreous body that is firmly fixed to the retina, with a high risk of retinal detachment [1]. The majority of retinal tears appear during the course of acute detachment of the posterior vitreous membrane (posterior vitreous detachment – PVD – separation of the cortical vitreous from the membrana limitans interna in a posterior direction from the vitreous base); nevertheless their development may take place even after an interval of several weeks [2]. They appear more frequently in the place of malignant peripheral degenerations [1]. The predilection localization is the area between the ora serrata and the equator, most frequently the superior temporal quadrant (60%) [2]. (Fig. 1)

The prevalence of retinal tears in patients with acute PVD, most commonly manifested in suddenly appearing monocular flashes (photopsia) and floaters in front of the affected eye, varies in the literature within the range of 5.4–23% [3,4,5,6]. The most important reported symptom of the onset of retinal tear upon acute posterior vitreous detachment is subjective deterioration of visual acuity [3]. According to the results in autopsy and clinical trials, the incidence of retinal tears or holes is stated within the range of 2–9% [7].
The risk factors of onset include myopia, previous ocular surgical procedures (aphakia, pseudophakia), positive family or personal medical history of retinal detachment, and ocular traumas. Men also tend to be more frequently affected than women [4,8,9]. The development of tears and rhegmatogenous retinal detachment has been described also following various types of ophthalmological refractive procedures such as laser in situ keratomileusis (LASIK) or implantation of phakic intraocular lenses in myopic patients [10,11,12].
We divide morphological tears into horseshoe tears (U-tears), incomplete U-tears, tears with operculum, retinal dialysis and giant retinal tears (affecting more than 90 degrees of circumference of the eyeball). According to localization, we differentiate between oral, post-oral, equatorial and post-equatorial tears [2]. Some authors divide tears into symptomatic and asymptomatic on the basis of the presence or absence of simultaneous rhegmatogenous retinal detachment [13].
Tears virtually always require surgical treatment, and close spontaneously only in rare cases [14].
Therapy includes coagulation of the edges of the tear by laser barrage or cryoretinopexy, or if applicable episcleral sealing, especially in the case of incipient retinal elevation. Other options are pneumatic retinopexy or pars plana vitrectomy (PPV) [1,4,15].
Laser treatment of tears for prophylaxis of rhegmatogenous retinal detachment was described as early as in 1960 by Colyear et al. [16]. This is a procedure performed in outpatient care, most frequently on a slit lamp, nevertheless it is also possible with the use of an indirect ophthalmoscope or in the form of an endolaser during the course of an intraocular procedure. Photocoagulation effectively reduces the risk of progression to retinal detachment in the case of tears to under 5%, as opposed to 50% in untreated patients [16].
Complications of laser retinopexy include the development of a secondary epiretinal membrane (ERM) or proliferative vitreoretinopathy [17,18]. Lesser-known complications include transitory loss of accommodation and pupillary defects, which result from damage to the parasympathetic nerve fibers innervating the ciliary body and iris sphincter [19,20].
MATERIAL AND METHODS
We conducted a retrospective analysis of the results of therapy of patients with retinal tears or holes, including rhegmatogenous retinal detachment, who were treated primarily by laser retinopexy at our center, with a minimum follow-up observation period of 3 months. The authors reviewed the health documentation of all the patients with this diagnosis examined at our clinic during the monitored period from December 2019 to August 2022. The cohort included all patients with acute PVD who were indicated and underwent therapy with the green laser IQ 532 (IRIDEX Corporation, Mountain View, CA, USA) for one or more tears on the retinal periphery.
At the outset a detailed medical history of all the patients was recorded, and at the same time a comprehensive ophthalmological examination was conducted, including evaluation of the condition in artificial mydriasis using tropicamide gtt (Unitropic 1%, Unimed Pharma). Color photographic documentation of the finding on the posterior segment of the eye was obtained using the instrument Daytona (Optos, Marlborough, USA). At the same time, Brightness modulated (B-scan) ultrasonic imaging of the eyeball was performed using the instrument US-4000 Echoscan (NIDEK CO., LTD., Japan) (Fig. 2). In the case of favorably localized tears at an accessible distance, measurement was also conducted with the aid of Fourier-Domain optical coherence tomography (Optovue Inc., Fremont, CA, USA) (Fig. 3).


The procedures were performed by the standard method on a slit lamp, using a contact lens Mainster Wide field (Ocular Instruments, USA) in topical local anesthesia with oxybuprocaine hydrochloride (Benoxi 0.4% gtt, Unimed Pharma). All the procedures were performed by the same surgeon. The initial energy of the laser was set at 160mW and progressively titrated until the formation of a visible beam. Initially an attempt at a 360-degree bordering of the defect by confluent laser beam in 2-4 rows was performed on all the patients. In the case of tears localized too anteriorly, the convergence points were applied in an arc around the tear.
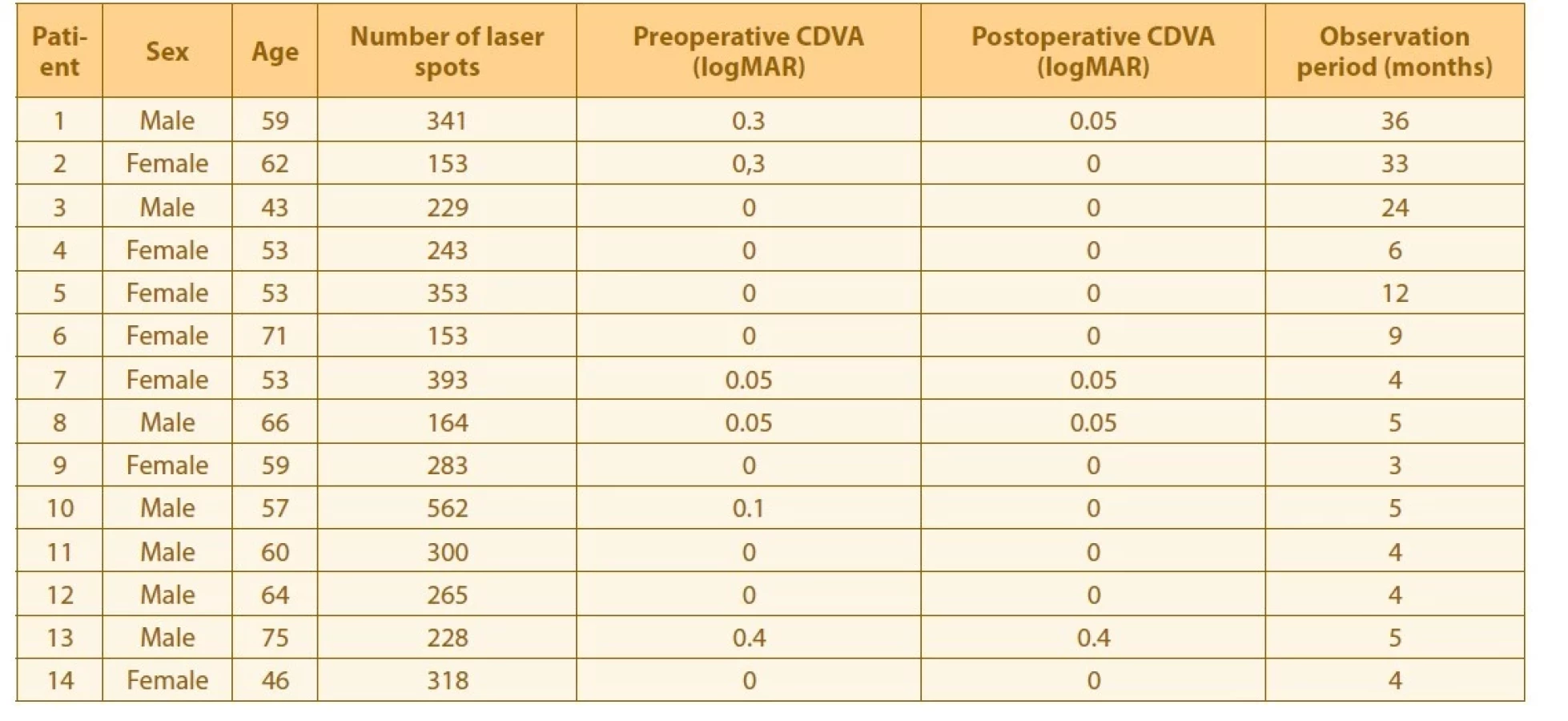
During the monitored period, a total of 14 patients with a mean age of 59 years (median 59) were treated. Men and women were represented equally. We observed a slight predominance of affliction of the left eye (8 : 6).
The most common present risk factor in our cohort was myopia in ten of the patients, followed by previous cataract surgery (six patients). Two eyes had also previously undergone YAG capsulotomy, and two patients had undergone laser refractive surgery on the cornea.
In the majority of the patients (11 cases) only 1 tear was found, in the remaining three patients two tears were verified. Morphologically this concerned 11 horseshoe tears and six operculated tears with a cap. The most common localization was the superior temporal quadrant (8 eyes), followed by the inferior temporal quadrant (5 eyes). Nine patients simultaneously had accompanying hemorrhage into the vitreous (hemovitreus), in three eyes subretinal fluid was present at the time of examination, with incipient detachment of the peripheral retina.
The summary demographic and clinical characteristics of our cohort are presented in Table 1.

All the procedures were performed by the same surgeon. The energy used was within the range of 160–260 mW. The width of the beam was 200 μm as standard, the time 0.2 seconds in all cases. The average number of applied beams was 285 points (median 274).
Postoperatively the influence on visual acuity was evaluated, as well as the success rate of therapy (progression of rhegmatogenous retinal detachment, if applicable presence of new tears) and objective appearance on color photography of the fundus. The observation period following the procedure was within the range of 3 months to 3 years.
RESULTS
All the tears we found were successfully repaired, and none of the procedures was affected by perioperative complications (Fig. 4, 5, 6).



The overall success rate of prophylaxis of rhegmatogenous detachment following primary laser treatment was 93% in our cohort. We did not record the necessity to repeat laser therapy or supplement it with cryoretinopexy in any of our patients. One of our patients subsequently underwent an intraocular operation in the form of PPV due to progression of retinal detachment from another biomicroscopically inaccessible hole, which was part of lattice degeneration in the peripheral part of the retina. This pathology was only verified during the performance of PPV with gas tamponade by sulfur hexafluoride (SF6). Postoperatively the retina was reattached with very good anatomical and functional effect. The other patients did not require any adjuvant therapy.
Visual functions remained stable or improved throughout the course of the follow-up observation period in all the patients of the cohort (see Table 2).
DISCUSSION
Retinal tears are the most common urgent vitreoretinal condition in ophthalmology [21]. A frequent complication is detachment of the posterior vitreous membrane, which is classified among degenerative age-related conditions. Whereas the majority of patients remain asymptomatic, some manifest typical symptoms of floaters in front of the eye caused by opacities of the liquefied vitreous. We observe the progression of tears in 6–18% of patients with symptomatic PVD, which is manifested in symptoms of retinal traction such as photopsia or flashes [7,22,23]. In the case of a sudden increase in the number of floaters with or without flashes, a prompt examination by an ophthalmologist is recommended [23].
The main risk factors of the onset of retinal tears and rhegmatogenous detachment have been identified as myopia and previous cataract surgery [24,25]. In accordance with these publications, we confirmed at least one of these factors in all our patients.
Diagnostically it is most beneficial to conduct a thorough biomicroscopic examination in artificial mydriasis, supplemented with instrument imaging. At our center we routinely perform color wide-angle photographic documentation of the posterior segment of the eye and examination by ultrasound. For verification of subretinal fluid and the effect of therapy we also make effective use of imaging by means of optical coherence tomography (OCT) (Fig. 7).

Historically various different types of therapy have been used in prophylaxis of rhegmatogenous retinal detachment. The first of these were cauterization and diathermy, then subsequently in the 1950s photocoagulation with xenon arc was widely applied. The next most widely used technique was retinal cryopexy. Later, in the 1960s, the effect of photocoagulation of retinal tears with an argon laser was described [26]. Laser retinopexy then became the primary treatment for retinal tears [27].
A further described option for treatment is pars plana vitrectomy (PPV) with the use of an endolaser, and without the need for a gas tamponade at the end of the operation [28,29]. Studies are available which describe the results of early vitrectomy in cases of vitreous hemorrhage, probably in connection with retinal tears. In a cohort of 40 treated eyes, the authors identified as many as 46.3% of tears only during the course of the operation. These defects were undetectable preoperatively, which indicates a certain danger of a conservative approach to hemovitreus [30]. Among our own patients we also discovered one hidden hole in the retinal periphery only during the subsequent intraocular procedure.
The success rate of laser therapy varies in the literature. The experience of the operating surgeon appears to be an important parameter in some of the publications. Acutely occurring tears often require prompt treatment in emergency care. Ghosh et al. published a retrospective analysis of the results of urgent photocoagulation by argon laser performed by young doctors. The outcome of this study was the necessity of subsequent therapy in 24% of patients [31]. Petrou et al. also evaluated the effectiveness of the procedure on 100 eyes when performed by junior doctors. The outcome was that 58% of patients required subsequent vitreoretinal care [32]. A large retrospective study (307 eyes) comparing the results of treatment by resident doctors and by specialists was presented by Lankry et al. They observed progression to rhegmatogenous retinal detachment in 6.9% of cases treated by resident doctors, and 5.5% treated by specialists. The authors thus did not find a significant difference between the two groups [33].
Garoon et al. presented the results of treatment of retinal tears by laser retinopexy in 401 eyes, in which repeated therapy was required in 18.7% of cases, and a vitreoretinal operation due to rhegmatogenous retinal detachment was required in 5.7% [34]. A similarly large cohort was published by Kovacević et al. The authors found primary therapy to be successful in 94% of the total of 430 eyes, with rhegmatogenous retinal detachment occurring in the remaining 6% of patients [18]. We attained similar results (7%) also in our own patients. A number of studies report a relatively low success rate following primary laser therapy. Khan et al. observed complete success in only 53.5% of 45 patients, whereas in the remainder repeated laser barrage or cryotherapy was required. The authors stated progression to rhegmatogenous detachment and the surgical solution thereof in 7% of treated patients, more commonly in the case of defects with bridging vessels or vitreous hemorrhages [27]. Lankry et al. also defined the presence of vitreous hemorrhages and subretinal fluid as a statistically significant risk factor for the progression of retinal detachment [33]. In our only patient who underwent PPV due to the progression of the finding, preoperative partial hemovitreus and localized retinal detachment was also confirmed, which was in accordance with these publications.
The cited studies and our long-term results are analogous in terms of the frequency of failure of primary laser therapy and progression to rhegmatogenous retinal detachment with the need for vitreoretinal surgery. As regards complications of treatment, the literature describes proliferative vitreoretinopathy, transitory loss of accommodation or pupillary defects. We did not record these or any other complications in our own patients.
CONCLUSION
Laser retinopexy is a sparing, safe and effective method of treating retinal tears. All the tears we found were successfully repaired by primary treatment. From our clinical experience, the technique is also applicable in the case of partial vitreous hemorrhage or incipient rhegmatogenous retinal detachment.
Progression of retinal detachment with the necessity of PPV operation occurred in only one case, due to a further biomicroscopically originally undetectable hole in the retinal periphery. After the intraocular procedure, the retina was reattached without the requirement for further intervention.
The visual functions of all our patients improved or remained stable.
However, the predicative value of our results is limited due to the small size of the cohort.
The authors of the study declare that no conflict of interests exists in the compilation, theme and subsequent publication of this professional article, and that it is not supported by any pharmaceuticals company. The study has not been submitted to in any other journal or published elsewhere, with the exception of congress abstracts.
Received: February 3, 2023
Accepted: March 9, 2023
Available on-line: June 20, 2023
MUDr. Petr Kristian
Gemini oční klinika Ostrava
Zdeňka Chalabaly 3041/2
Bělský Les
700 30 Ostrava
E-mail: kristian.petr@gmail.com
Sources
1. Kuchynka P. Oční lékařství. Praha: Grada; 2007. 768.
2. Kanski JJ, Bowling B. Clinical Ophthalmology: a systematic approach. 7th ed. Edinburgh: Elsevier Saunders; 2003. 909.
3. Hollands H, Johnson D, Brox AC, Almeida D, Simel DL, Sharma S. Acute-onset floaters and flashes: is this patient at risk for retinal detachment? JAMA. 2009 Nov 25;302(20):2243-2249.
4. Blindbaek S, Grauslund J. Prophylactic treatment of retinal breaks - -a systematic review. Acta Ophthalmol. 2015 Feb;93(1):3-8.
5. Seider MI, Conell C, Melles RB. Complications of Acute Posterior Vitreous Detachment. Ophthalmology. 2022 Jan;129(1):67-72.
6. Verhoekx JSN, van Overdam KA, Gishti O, van Leeuwen R, Crama N. Plotse toename van mouches volantes is een alarmsymptoom, ook zónder lichtflitsen [Acute onset of floaters, even without flashes, is an urgent ophthalmic warning sign]. Ned Tijdschr Geneeskd. 2021 Oct 21;165:D5850. Dutch.
7. Blindbaek S, Grauslund J. Prophylactic treatment of retinal breaks - -a systematic review. Acta Ophthalmol. 2015 Feb;93(1):3-8.
8. McCullagh D, Higham A, Best R. The BElfast Retinal Tear and detachment Score (BERT Score). Eye (Lond). 2021 May;35(5):1427-1430.
9. Gergelyová K. Obrovské trhliny sítnice [Giant retinal tears]. Cesk Slov Oftalmol. 1999 Nov;55(6):384-394. Czech.
10. Arevalo JF, Ramirez E, Suarez E, et al. Rhegmatogenous retinal detachment in myopic eyes after laser in situ keratomileusis. Frequency, characteristics, and mechanism. J Cataract Refract Surg. 2001 May;27(5):674-680.
11. Reviglio VE, Kuo IC, Gramajo L, Olmedo MA, Falco M, Juarez CP. Acute rhegmatogenous retinal detachment immediately following laser in situ keratomileusis. J Cataract Refract Surg. 2007 Mar;33(3):536-539.
12. Martínez-Castillo V, Boixadera A, Verdugo A, Elíes D, Coret A, García - Arumí J. Rhegmatogenous retinal detachment in phakic eyes after posterior chamber phakic intraocular lens implantation for severe myopia. Ophthalmology. 2005 Apr;112(4):580-585.
13. Rozsíval P, et al. Oční lékařství. Praha: Galén; 2006. 373.
14. Heissigerová J a kol. Oftalmologie. 1. vyd. Praha: Maxdorf; 2021. 392.
15. Hejsek L, Dusová J, Stepanov A, Rozsíval P. Operace rhegmatogenního odchlípení sítnice zevním postupem [Scleral buckling for rhegmatogenous retinal detachment]. Cesk Slov Oftalmol. 2014 Feb;70(1):36-39. Czech.
16. Somoskeoy T, Shah P. Safety and efficacy of the use of navigated retinal laser as a method of laser retinopexy in the treatment of symptomatic retinal tears. Eye (Lond). 2021 Apr;35(4):1256-1260.
17. Israilevich R, Salabati M, Mahmoudzadeh R, et al. Secondary epiretinal membrane after laser retinopexy for retinal tear or localized retinal detachment: Surgical Outcomes and Optical Coherence Tomography Structural Analysis. Retina. 2022 Jan 1;42(1):38-45.
18. Kovacević D, Loncarek K. Dugorocni rezultati argonske laserske fotokoagulacije mreznice zbog ruptura [Long-term results of argon laser retinal photocoagulation for retinal ruptures]. Acta Med Croatica. 2006;60(2):149-52. Croatian.
19. Polizzi S, Fujikado T. Transient Deficit of Accommodation After Laser Barrage for Retinal Tear. Optom Vis Sci. 2016 Feb;93(2):218-219.
20. Lifshitz T, Yassur Y. Accommodative weakness and mydriasis following laser treatment at the peripheral retina. Ophthalmologica. 1988;197(2):65-68.
21. Moussa G, Samia-Aly E, Ch’ng S, et al. Vitreoretinal specialists compared with residents on outcomes of primary laser retinopexy in preventing retinal detachment in 958 eyes. BMJ Open Ophthalmol. 2022 Feb 4;7(1):e000859.
22. Uhr JH, Obeid A, Wibbelsman TD, et al. Delayed Retinal Breaks and Detachments after Acute Posterior Vitreous Detachment. Ophthalmology. 2020 Apr;127(4):516-522.
23. Gishti O, van den Nieuwenhof R, Verhoekx J, van Overdam K. Symptoms related to posterior vitreous detachment and the risk of developing retinal tears: a systematic review. Acta Ophthalmol. 2019 Jun;97(4):347-352.
24. Feltgen N, Walter P. Rhegmatogenous retinal detachment-an ophthalmologic emergency. Dtsch Arztebl Int. 2014 Jan 6;111(1 - 2):12-21; quiz 22. doi: 10.3238/arztebl.2014.0012
25. Schick T, Heimann H, Schaub F. Netzhautablösung – Teil 1 [Retinal Detachment Part 1 - Epidemiology, Risk Factors, Clinical Characteristics, Diagnostic Approach]. Klin Monbl Augenheilkd. 2020 Dec;237(12):1479-1491. German.
26. Pollak A, Oliver M. Argon laser photocoagulation of symptomatic flap tears and retinal breaks of fellow eyes. Br J Ophthalmol. 1981 Jul;65(7):469-472.
27. Khan AA, Gupta A, Bennett H. Risk stratifying retinal breaks. Can J Ophthalmol. 2013 Dec;48(6):546-548.
28. Lee KH, Chung YR, Yeo S, Lee K. Is gas/air tamponade essential for eyes with small peripheral retinal breaks without detachment during vitrectomy? BMC Ophthalmol. 2022 Apr 22;22(1):186.
29. Martínez-Castillo V, Zapata MA, Boixadera A, Fonollosa A, García-Arumí J. Pars plana vitrectomy, laser retinopexy, and aqueous tamponade for pseudophakic rhegmatogenous retinal detachment. Ophthalmology. 2007 Feb;114(2):297-302.
30. Tan HS, Mura M, Bijl HM. Early vitrectomy for vitreous hemorrhage associated with retinal tears. Am J Ophthalmol. 2010 Oct;150(4):529-533.
31. Ghosh YK, Banerjee S, Tyagi AK. Effectiveness of emergency argon laser retinopexy performed by trainee doctors. Eye (Lond). 2005 Jan;19(1):52-54.
32. Petrou P, Lett KS. Effectiveness of emergency argon laser retinopexy performed by trainee physicians: 10 years later. Ophthalmic Surg Lasers Imaging Retina. 2014 May-Jun;45(3):194-196.
33. Lankry P, Loewenstein A, Moisseiev E. Outcomes following Laser Retinopexy for Retinal Tears: A Comparative Study between Trainees and Specialists. Ophthalmologica. 2020;243(5):355-359.
34. Garoon RB, Smiddy WE, Flynn HW Jr. Treated retinal breaks: clinical course and outcomes. Graefes Arch Clin Exp Ophthalmol. 2018 Jun;256(6):1053-1057.
Labels
OphthalmologyArticle was published in
Czech and Slovak Ophthalmology

2023 Issue 3
Most read in this issue
- LASER THERAPY OF RETINAL TEARS
- CHANGES IN THE VISION OF ADULT AMBLYOPIC PATIENTS FOLLOWING CLEAR LENS EXTRACTION
- GIANT PROLACTINOMA. A CASE REPORT
- PATHOGENESIS AND CURRENT METHODS OF TREATMENT OF SECONDARY UVEITIC GLAUCOMA. A REVIEW