
Treatment options for infratemporal fossa tumors – case reports
Authors:
S. Kalmanová 1; V. Čalkovský 2; P. Hanzel 2; B. Kolarovszki 3; R. Richterová 3; K. Adamicová 4; M. Janíčková 1
Authors‘ workplace:
Clinic of Stomatology and Maxillofacial Surgery, University Hospital Martin, Jessenius Faculty of Medicine in Martin, Comenius University, in Bratislava, Slovakia
1; Clinic of Otorhinolaryngology and Head and Neck Surgery, University Hospital Martin, Jessenius Faculty of Medicine in Martin, Comenius University in Bratislava, Slovakia
2; Clinic of Neurosurgery, University Hospital Martin, Jessenius Faculty of Medicine in Martin, Comenius University in Bratislava, Slovakia
3; Department of Pathological Anatomy, University Hospital Martin, Jessenius Faculty of Medicine in Martin, Comenius University in Bratislava, Slovakia
4
Published in:
ACTA CHIRURGIAE PLASTICAE, 67, 1, 2025, pp. 68-73
doi:
https://doi.org/10.48095/ccachp202568
Introduction
Tumors of the infratemporal fossa (ITF) form a heterogenous group, mostly consisting of benign tumor. Due to its specific anatomy and complicated approach, there are several factors to consider in treatment. These types of tumors represent approximately 0.5% of all head and neck tumors [1]. ITF tumors treated with radical surgical resections carry a high risk of complications, high morbidity, and mortality rate [2]. However, advancement in endoscopic endonasal surgery (EES) allowed to use this treatment option for ITF tumors and its use for management of these patients increased through the years [3].
For understanding and deciding about treatment options, the knowledge of specific anatomy of ITF is crucial because of its proximity with cranial nerves and neurovascular structures [4].
ITF lies anteriorly to the posterior wall of maxilla, posteriorly to the tympanic plate, inferiorly to zygomatic arch and laterally to the ramus of mandible and pterygoid plates. It contains masticatory muscles (masseter, temporalis, and pterygoid muscles), temporomandibular joint, maxillary artery with veins and pterygoid venous plexus and nerves – including the lingual, mandibular, and otic ganglia) [5].
Although the incidence of these type of tumors is extremely rare, they always represent a challenge for surgeons from neurosurgical, maxillofacial and otorhinolaryngology departments. Therefore, patients with ITF tumors always demands interdisciplinary approach.
In literature review by Bin-Alamer et al. containing 27 articles related to 106 patients, they described schwannomas, meningiomas and synovial chondromatosis as the most common types of ITF tumors.
There are several types of possible surgical approaches to ITF tumors. We can divide ITF approaches into lateral (traszygomatic and lateral infratemporal), anterior (transmaxillary, transfacial, transpalatal, transoral) or inferior (transmandibular and transcervical) [6].
Endoscopic endonasal approach (EEA) provides an alternative access to lesions lying both in ITF and pterygopalatinal fossa, providing less invasive method with lower morbidity rate than transcranial approaches [7]. We can further divide EEA into those treated with transpalatine, transantral and endonasal inferior turbinectomy approaches [8].
Experience of our department
As there is no agreement in literature to the therapy of ITF tumors, we would like to present a few cases of ITF tumor patients treated in cooperation with our department and different approaches to them.
Trans-mandibular approach
A 31-year-old male patient was referred to our department from an otorhinolaryngologist for pain in the temporomandibular joint area. He was complaining of pain during chewing in front of the ear lobes bilaterally, but after taking non-steroid anti-inflammatory drugs, the condition was better. During the examination, both clinically and on the orthopantomographic scan there were no signs of any pathology in the temporomandibular joint area, but there was severely poor oral hygiene, periodontitis and multiple radices. He was advised to be treated by a dentist in the first place, to rule out dental origin of symptoms, and if the difficulties persisted, he was instructed to come for a check-up.
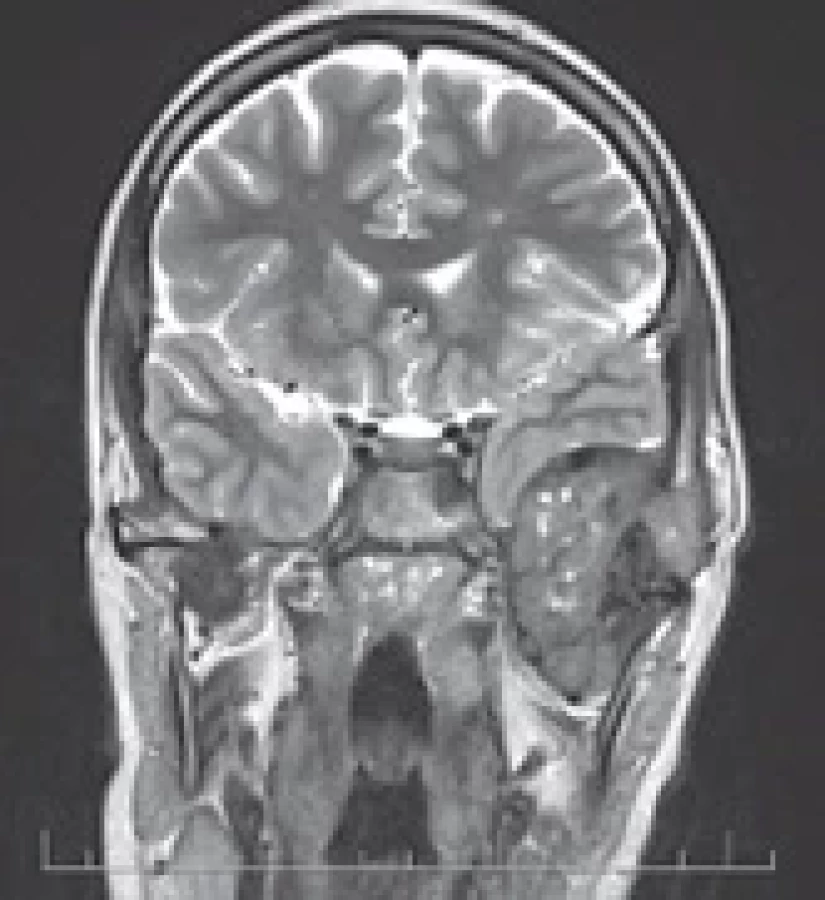
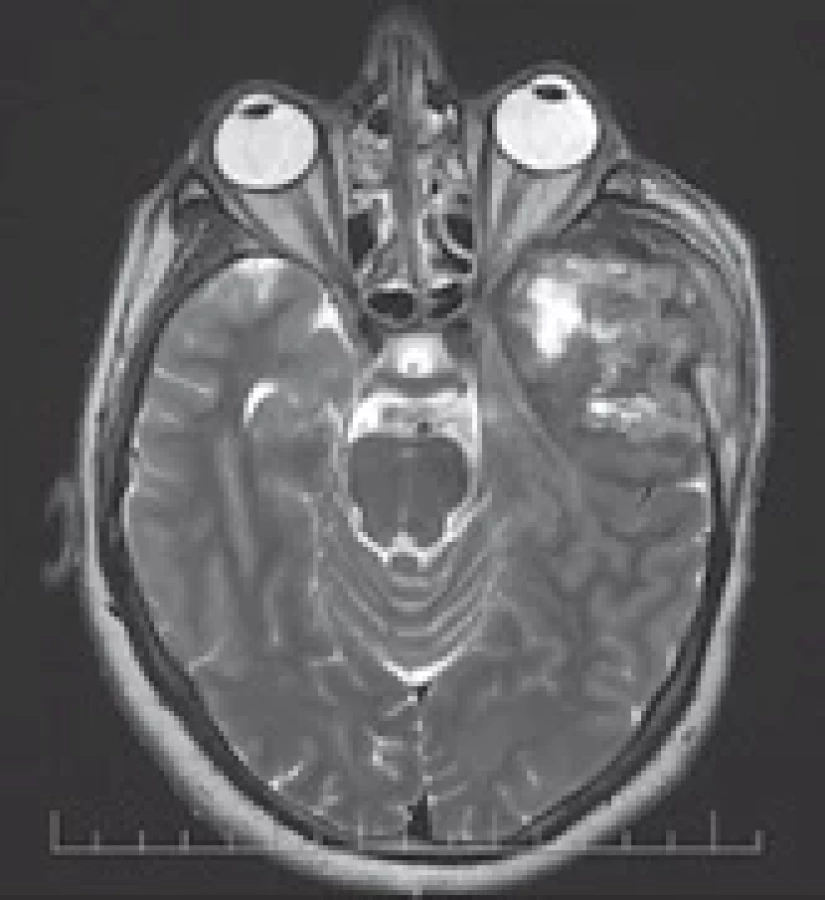
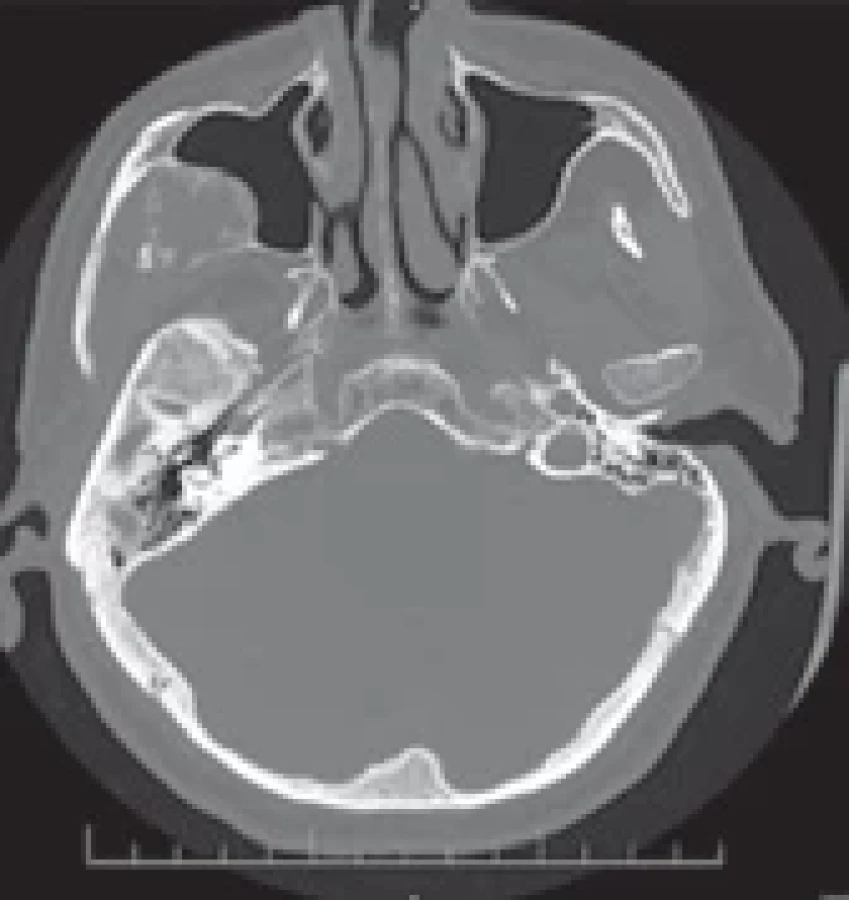
He came again after 14 months with a CT scan of the brain showing a tumorous process in the middle cranial fossa on the left side with extracranial expansion of 55 × 55 × 45 mm in size. A neurosurgical consultation and an MRI scan was done, showing a tumorous lesion extracranially, compressing the skull base with the destruction of temporal bone without intracranial invasion, with infiltration into the mastoid process and mandibular fossa on the left side (Fig. 1–3).
In that time there was an edema in preauricular area present, with facial asymmetry and limited mouth opening. Because of the contradictory results of imaging examination, based on consultations with otorhinolaryngologists, neurosurgeons and maxillofacial surgeons, a CT navigated biopsy was indicated with the result of giant cell granuloma without metaplasia present in the biopsied material.
In the next step angiography with placement of a stent graft into the internal carotid artery on the left side and embolization of the tumor were done. The removal of the tumor was done by a neurosurgeon in cooperation with a team of maxillofacial surgeons from our department. A modified Blair approach from temporal to preauricular areas was done, following separation of the temporal muscle (Fig. 4). Resection of the mandibular ramus, condylar and muscular process of the mandible was done to get approach to the tumor. The tumorous mass was growing from the temporomandibular joint. Subtotal resection of the tumor was done, without the possibility of complete removal of the tumorous lesions due to its intracranial invasion (Fig. 5, 6).
The result of the histopathological exam was a giant cell lesion, similar to chondroblastoma, without H3F3A/B mutation. It was described as an aggressively growing giant cell tumor from the tendon sheath, probably growing from the temporomandibular joint into the surrounding skeleton.
In the early check-ups he was complaining of pain, pressure in the temporal area and paresis of the facial nerve on the left side. The check-ups were performed every 2 weeks right after the surgery. This period was extended to 1 month and later in time to 3 months. The first MRI scan was performed 1 week after the surgery, showing some residual collection and residual tumorous tissues. The residual tumorous mass was considered inoperable. In the next MRI examination, there was regression of residual collection with persisting residual tumor. It was performed 3 weeks after the surgery. Currently, the patient undergoes check-ups every 6 months in both neurosurgical and our departments and his symptoms are getting better due to chronic pain management and rehabilitations (Fig. 7, 8). In the check-ups the cone-beam CT (CBCT) scans are performed without signs of progression of the lesion into the skeletal bones and every 6 months there is an MRI examination scheduled to observe the residual tumor and its possible progression or regression.




Endoscopic approach
A 69-year-old male patient was referred to our department for a lesion found on a CT scan. The CT scan was done due to a collapse and the ITF tumor was an accidental finding on the scans. He did not have any previous signs or complaints connected to the tumor. He was treated for arterial hypertension without any other previously treated diseases.
On the CT scan, it was described as circumscribed contrast-induced hyperdense lesions located dorsally from the lateral maxillary sinus wall on the right side. A potential diagnosis based on these scans was an osteoblastoma or a chondrosarcoma.
On MRI, enhancing tumor of right ITF with a calcified border destroying lateral wall of the maxillary sinus was described, with 23 × 36 × 31 cm in size. It was slightly protruding into the maxillary sinus (Fig. 9–11).
After the consultation with neurosurgical and otorhinolaryngology department, we decided for endoscopic endonasal approach after embolization of the branches of maxillary artery – blood supply of the tumor.
At the beginning of the surgery approach for functional endoscopic sinus, functional endoscopic sinus surgery (FESS) was done with supraturbinal antrostomy on the right side. Visualization of tumor verified by CT navigation was done, without other pathological finding in the maxillary sinus (Fig. 12). Part of the tumor obtained after removing the bone in the lateral wall of maxillary sinus was send to frozen section with the result of mesenchymal lesion with unclear dignity. Because the tumor was not possible to reach from the supraturbinal antrostomy, intraoral approach through the anterior wall of the maxilla was chosen. The tumor was then mobilized into the maxillary sinus and removed through the anterior wall of the maxillary sinus (Fig. 13). It was growing into the ITF with its size of 40 × 25 × 25 mm. The defect was reconstructed with an autologous fat pad graft from the left thigh, covered with oxidized regenerated cellulose and the fascia lata. Through supraturbinal antrostomy an epistat (nasal catheter) was inserted into the maxillary sinus to hold the graft in place.
The definitive histopathological examination described the tumor as a benign fibro-osseal lesion growing from the cranio-facial skeleton. The patient was complaining of mild pain 1 month after the procedure without any alterations of sight.





Observation
A 71-year-old female patient was referred to our department by an otorhinolaryngologist with a lesion found on MRI. The patient was previously treated for migraines without any other complaints with possible connection to the tumor. An accidental finding was described on MRI – a tumor of 2 cm (in the largest diameter) in the skull base behind the left maxillary sinus. Due to its characteristics, it was suspected to be a congenital cholesteatoma or an epidermoid tumor (Fig. 14).
The patient was referred to our otorhinolaryngology and neurosurgical departments. Based on the MRI scan, it was an incidental lesion with benign characteristic and the localization was hardly achievable, therefore we decided consensually for observing the patient with follow-up MRI scan after 1 year.


Discussion
There is a certain discrepancy in literature between authors about exact borders of ITF [4], as well as its approaches. Before 1960s, ITF was considered surgically inaccessible [9].
Currently, because of the possibilities connected with innovations in microsurgery and endoprostheses, it should be a standard to do the reconstruction after resection of large benign tumors to improve patient’s quality of life. However, in the first described case, we have not done the reconstruction yet because of incomplete removal of the lesion. The remaining lesion was described as inoperable by neurosurgeons, an otorhinolaryngologist and a maxillofacial surgeon due to its localization and proximity to brain structures without clear borders of the lesion.
Another important thing to consider is performing condylectomy for ITF tumor removal. An alternative to this kind of resection can be the anterior displacement of the mandible in order to get an acceptable field of view. Some authors prefer resection because of the pain and temporomandibular joint disorders that can result from lateral movement of mandible [10]. On the other hand, there is a deviation of the mandible and pain resulting from the resection of the condyle [11]. We believe that after careful analysis of possible complications, appropriate approach should be chosen to get a sufficiently large surgical field for safe performance of the resection.
In the second case, we decided to use the transoral endoscopic approach with electromagnetic navigation to decrease possible complications from open surgery. There is a limitation in the exposure and instrumentation of the lateral part of ITF through endoscopic endonasal surgery [12]. At the beginning of the identification of the tumor through the endonasal approach, we did not have enough space to reach the ITF, so the access by modified Caldwell-Luc was done through the anterior maxillary wall. The possible limitations included mobilization of the tumor and incomplete resection of the lesion endoscopically. Due to the localization of the tumor, we were trying to avoid disruption of the orbital floor, which would be then reconstructed by a titanium plate. The most important limitation of endoscopic approaches to consider is a restricted possibility to repair severe vascular injuries, so in-depth anatomical knowledge is necessary to choose this type of approach. After the surgery, there was a dispensation of the patient – every 7 days in the first month after the surgery, then every 14 days for another month and currently the patient is attending regular check-ups every month. Three months after the surgery a CBCT scan was done – with presentation of clear paranasal sinuses and afterwards 4 months post-surgery MRI examination was performed without showing any residual tumor or relapse. The next MRI examination is planned in 1 year from the surgery.
The third case represents a non-surgical treatment of ITF tumor. The decision of observing the tumor was based on the age and overall health of the patient, regarding the placement and characteristics on MRI.
The pre-operative biopsy was only performed in the first case. The tumor was considered almost inoperable, so the outcome of the biopsy was crucial for choosing the treatment option. Furthermore, the localization of tumor made it reachable for performing the biopsy. If the tumor is malignant, palliative treatment would be a better option for the patient, because of the size and placement of the tumor. In the second case, based on the localization and appearance on MRI (pre-operatively), it was assumed, that the tumor had benign characteristic. It was approachable and complete removal was presumed. In the third case, the localization of the tumor made it inapproachable for probatory biopsy. The possible risk factors and damage of associated structures resulting from biopsy of the tumor would not bring such benefit for the patient, as it was clearly evaluated in the MRI scans – the tumor has the characteristics of congenital cholesteatoma or epidermoid tumor. This type of lesions would not be considered as life threatening for the patient, so the decision was made to observe the patient during regular check-ups – the first one was performed 6 months from the diagnosis. Based on the interdisciplinary consultation, another MRI examination will be performed after 1 year (and every year) from the first examination. The benefit of the preoperative biopsy both for the patient and for the outcome of the possible surgical procedure should be considered, especially if the tumor is not easily approachable, and the result of preoperative biopsy would not change the decision process of the treatment.
Conclusion
The ITF tumors are rare but rather complicated lesions for surgical approach. Removal of this type of tumor is associated with a high morbidity and mortality rate due to its usual proximity to crucial neurovascular structures, and often due to their invasion of the intracranial space. They present a challenge in every patient, they usually grow asymptomatically and when the symptoms occur, the lesions tend to be large and sometimes they cannot be removed completely. As for the surgical (or even non-surgical) treatment, there is not one universal solution for every ITF tumor. We need to analyze every case individually and we can also combine approaches yet described in the literature. In presented cases, the trans-mandibular and endoscopic approaches were performed. Observation of the tumor was chosen in the third case of ITF tumor considering the possible risk factors resulting from surgery due to its localization. Anatomical knowledge is essential together with cooperation between other specialties – maxillofacial surgery, neurosurgery, otorhinolaryngology, vascular surgery and radiology – for the best outcome with minimal complication rate and successful rehabilitation of the patient.
Disclosure
The authors have no conflicts of interest to disclose. The authors declare that this study has received no financial support. All procedures performed in this study involving human participants were in accordance with ethical standards of the institutional and/or national research committee and with the Helsinki declaration and its later amendments or comparable ethical standards.
Roles of authors
Sarah Kalmanová – article writing, data processing, surgery; Vadimír Čalkovský, Pavel Hanzel, Branislav Kolarovszki, Romana Richterová – surgeries, part of diagnostic process, interdisciplinary consultations; Katarína Adamicová – histopathological examination; Mária Janíčková – performing surgery, supervision, text editing, corresponding author.
Sources
1. Bin-Alamer O., Bhenderu LS., Palmisciano P., et al. Tumors involving the infratemporal fossa: a systematic review of clinical characteristics and treatment outcomes. Cancers (Basel). 2022, 14 (21): 5420.
2. Zhou B., Huang Q., Shen PH., et al. The intranasal endoscopic removal of schwannoma of the pterygopalatine and infratemporal fossae via the prelacrimal recess approach. J Neurosurg. 2016, 124 (4): 1068–1073.
3. Kassam AB., Gardner P., Snyderman C., et al. Expanded endonasal approach: fully endoscopic, completely transnasal approach to the middle third of the clivus, petrous bone, middle cranial fossa, and infratemporal fossa. Neurosurg Focus. 2005, 19 (1): E6.
4. Isolan GR., Rowe R., Al-Mefty O. Microanatomy and surgical approaches to the infratemporal fossa: an anaglyphic three-dimensional stereoscopic printing study. Skull Base. 2007, 17 (5): 285–302.
5. Kim SM., Paek SH., Lee JH. Infratemporal fossa approach: the modified zygomatico-transmandibular approach. Maxillofac Plast Reconstr Surg. 2019, 41 (1): 3.
6. Tiwari R., Quak J., Egeler S., et al. Tumors of the infratemporal fossa. Skull Base Surg. 2000, 10 (1): 1–9.
7. Prevedello DM., Ditzel Filho LF., Solari D., et al. Expanded endonasal approaches to middle cranial fossa and posterior fossa tumors. Neurosurg Clin N Am. 2010, 21 (4): 621–vi.
8. Theodosopoulos PV., Guthikonda B., Brescia A., et al. Endoscopic approach to the infratemporal fossa: anatomic study. Neurosurgery. 2010, 66 (1): 196–203.
9. Schramm VL., Jr. In: Sekhar LN., Schramm VL., eds. Tumors of the Cranial Base: Diagnosis and Treatment. Mount Kisco, NY: Futura Publishing Co; 1987. Infratemporal fossa surgery; pp. 421–437.
10. Donald PJ. In: Donald PJ. (ed). Surgery of the Skull Base. Philadelphia: Lippincott-Raven Publishers; 1998. Infratemporal fossa: middle cranial fossa approach, pp. 309–339.
11. Bejjani GK., Sullivan B., Salas-Lopez E., et al. Surgical anatomy of the infratemporal fossa: the styloid diaphragm revisited. Neurosurgery. 1998, 43 : 842–852.
12. Yacoub A., Anschuetz L., Schneider D., et al. Minimally invasive lateral endoscopic multiport approach to the infratemporal fossa: a cadaveric study. World Neurosurg. 2018, 112: e489–e496.
Assoc. Prof. Mária Janíčková, MD, PhD, MPH
Klinika stomatológie a maxilofaciálnej chirurgie
Jesseniova lekárska fakulta v Martine Univerzity
Komenského v Bratislave a Univerzitná nemocnica Martin
Kollárova 2
036 01 Martin
Slovensko
maria.janickova@uniba.sk
Submitted: 14. 11. 2024
Accepted: 19. 1. 2025
Labels
Plastic surgery Orthopaedics Burns medicine TraumatologyArticle was published in
Acta chirurgiae plasticae

Most read in this issue
- Comparison of lymphovenous anastomosis and vascularized lymph node transfer in lymphedema treatment – a literature review
- Possibilities of intranasal reconstruction in complex nasal defects
- Elevation of vitamin B12 levels attributed to biopolymer implants – a case report
- Landmarks in facial reanimation – a bibliometric analysis of the 50 most cited papers in dynamic facial reconstruction