
Elevation of vitamin B12 levels attributed to biopolymer implants – a case report
Authors:
J. A. Avila Rueda 1; A. Hurtado-Ortiz 2; M. Licht-Ardila 2; G. Camelo-Pardo 3; A. Mendoza-Monsalve 2; E. F. Manrique-Hernández 2
Authors‘ workplace:
Oncology institute, Fundación Cardiovascular de Colombia, Santander, Colombia
1; Department of Epidemiology, Fundación Cardiovascular de Colombia, Santander, Colombia
2; Servicio de Urgencias, Fundación Cardiovascular de Colombia, Santander, Colombia
3
Published in:
ACTA CHIRURGIAE PLASTICAE, 67, 1, 2025, pp. 64-67
doi:
https://doi.org/10.48095/ccachp202564
Introduction
Biopolymers are inert compounds frequently utilized to enhance the volume of specific body areas, such as the buttocks and breasts. Some of these biopolymers are synthetic, often derived from silicone [1]. However, their use can be associated with various complications, including granuloma formation and migration of the material to different parts of the body, which can potentially compromise vital organs [2]. Complications may manifest both locally and systemically [2,3]. Systemic manifestations may include polyarthralgia, myalgia, and cognitive and sleep disorders [3]. Additionally, serum vitamin B12 levels can be altered in association with chronic inflammatory processes, with documented levels exceeding 950 pg/mL [4].
Case presentation
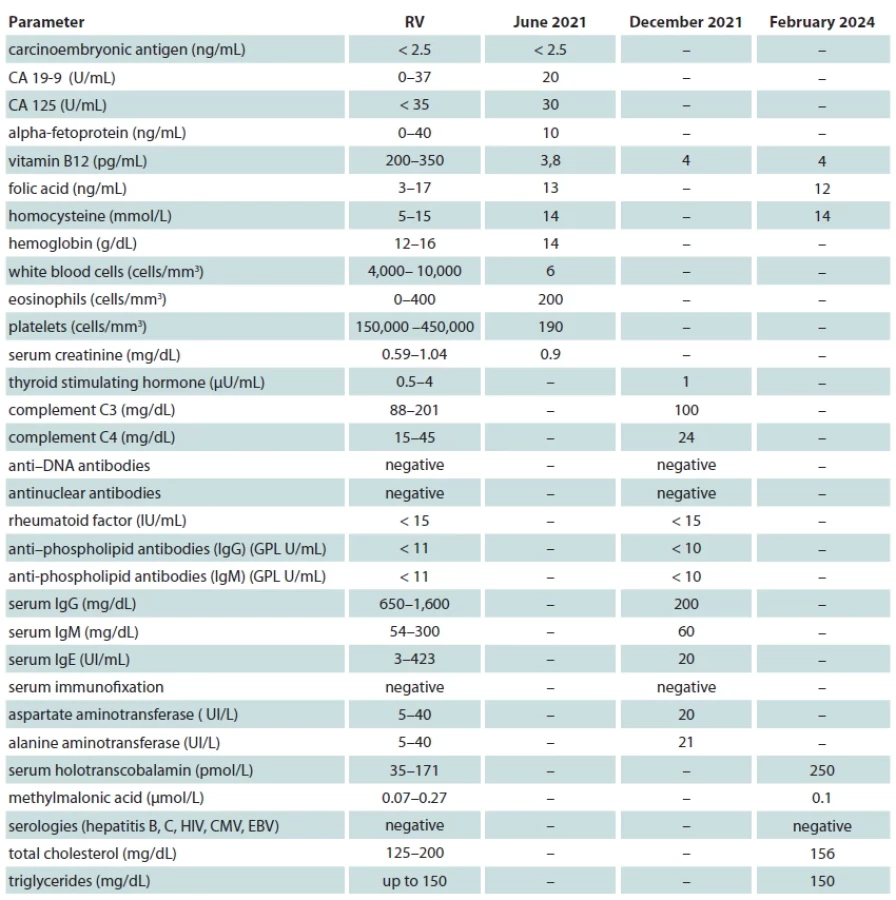
A 62-year-old female patient with no relevant medical history has been reviewed intermittently in hematology since June 2021. The consultation was prompted by an incidental finding of elevated serum vitamin B12 levels during a routine examination performed in the context of musculoskeletal pain, which resolved spontaneously. Upon inquiry, the patient denied taking any supplements or medications containing vitamin B12 and has remained asymptomatic to date. However, the patient reported complaints of pain, edema, and erythema, which were most pronounced between 4 and 12 months following biopolymer infiltration. Currently, pain in the infiltration areas persists, though it is sporadic and occurs primarily when acupressure is applied to these regions. The following studies were conducted, as detailed in Tab. 1.
In July 2022, the patient underwent several examinations, including a mammogram, which showed no pathological findings (BIRADS 1): a contrast-enhanced CT scan of the neck, chest, and abdomen, which also revealed no pathological findings, a complete blood count with no abnormalities, and both a total colonoscopy and upper gastrointestinal endoscopy, which showed no morphological alterations. Additionally, her vitamin B12 levels were found to be 4,000 pg/mL. In December 2023, a bone marrow biopsy demonstrated normal cellularity for her age, with appropriate maturation of erythroid, granulocytic, and platelet lineages, and no evidence of dysplasia, blasts, or pathological plasma cells. The bone marrow karyotype was normal (46, XX), and the electrocardiogram showed a sinus rhythm with no alterations in the QRS complex.
Furthermore, repeated levels of carcinoembryonic antigen and alpha-fetoprotein remained within expected values. To date, oncohematological disorders, liver diseases, pulmonary conditions, viral infections, autoimmune disorders, and cardiovascular causes, as well as a potential paradoxical increase in vitamin B12 levels associated with a deficiency in its active form, have been excluded. It was hypothesized that the elevated vitamin B12 levels were related to an exacerbated chronic inflammatory process. Consequently, the patient was queried about any procedures involving the placement of prosthetic materials or the presence of retained foreign bodies. The patient reported receiving polymethylsiloxane implants in 2009 for cosmetic purposes in the buttocks and ankles. An MRI of the pelvic and gluteal regions and a soft tissue ultrasound of both ankles were performed, revealing the following findings. Biopsies were not performed due to the high risk of complications, including soft tissue infection and potential inflammatory response triggered by the disruption of encapsulated biopolymer content in the absence of clinical signs or symptoms warranting invasive intervention.
The MRI of the pelvis (Fig. 1a, b) showed multiple nodular lesions in the subcutaneous tissue of the gluteal region (diameters up to 10 mm), hyperintense lesions on short tau inversion recovery (STIR) sequences, and silicone, suppressed on silicone suppression sequences as well as diffuse alteration with hyperintense signals on the STIR sequence in the subcutaneous tissue and the superficial fibers of the gluteus maximus muscle. Diagnosis: changes of alogenosis with focal nodular involvement and diffuse infiltration of the subcutaneous tissue and superficial fibers of the gluteus maximus bilaterally and symmetrically.
The ankle ultrasound (Fig. 1c, d) showed the presence of mixed echogenic material with marked attenuation in deep planes as well as cystic images with thin walls (average diameter of 0.3 cm) in the subcutaneous tissue of the distal third of the leg, neck, and dorsum of the foot. Diagnosis: Presence of modulating material (pure silicone and silicone oil) widely distributed in the subcutaneous tissue of the distal third of the legs, neck, and dorsum of both feet.
Although initially and according to what was stated by the patient herself, she presented obvious clinical signs of inflammation (within the period between 4 and 12 months after the infiltration procedure with biopolymers, the same external signs of inflammation such as pain and erythema subsided over time spontaneously); however, according to the recent images taken in our department, image changes compatible with chronic inflammation still persist (in this case being mild edema of the surrounding fatty tissue, signs of pericapsular hyperintensity in the nodular lesions) beyond the fact that currently there is no pain, limitation or redness.
Given these findings, it was assumed that the elevation of vitamin B12 was related to a chronic inflammatory process exacerbated by polymethylsiloxane implants. Currently, since the patient is asymptomatic and, aside from her age, does not present high cardiovascular risk factors, the risk and benefit of attempting to remove the multiple foreign bodies lodged in the buttocks and ankles were evaluated. It was decided to maintain semi-annual clinical monitoring, including laboratory tests and imaging studies, with extraction surgery to be considered only if the patient presents clinical abnormalities or significant changes in imaging.

Discussion
The infiltration of substances into the buttocks for esthetic purposes is sometimes associated with complications, such as the migration of the material to different parts of the body and the development of inflammatory processes (sometimes leading to foreign body granulomas), potentially resulting in local or systemic damage [3]. In our case, a persistent elevation of vitamin B12 without a clear explanation was noteworthy, ruling out its origin from the considered hematological, hepatic, and autoimmune pathologies. Metabolic disorders and even “paradoxical elevation” of non-functional vitamin B12 were also ruled out. Given that medical literature reports have associated cases of hypervitaminosis B12 with local or systemic inflammatory processes, our medical team proposed a viable interpretation of increased vitamin B12 levels associated with the presence of biopolymers in the subcutaneous tissues. Biopolymers have been described as adjuvants in the development of a systemic inflammatory response mediated by B and T lymphocytes. The chronic inflammatory reaction induced by these foreign materials, characterized by granuloma formation and infiltration of inflammatory cells, could have triggered this situation, leading to elevated vitamin B12 levels [5].
Previous studies have described associations between chronic inflammation and alterations in the metabolism of various vitamins and minerals [6]. Similarly, chronic diseases and some types of cancer can affect vitamin B12 metabolism [7]. In this case, the presence of biopolymers and the chronic inflammatory response revealed in imaging studies showing the presence of foreign material and changes in subcutaneous tissue suggest a persistent associated inflammatory reaction, which could have altered the mechanisms of transport and metabolism of vitamin B12, leading to its chronic accumulation in the serum.
The decision to opt for semi-annual clinical monitoring instead of surgical intervention was based on the absence of symptoms and significant cardiovascular risk factors, as well as the absence of similar reports in the medical literature at the time of this case publication documenting experiences in management strategies for this situation. Besides, taking into account that the patient has not been presenting clinical signs, or limitation, pain or secretion, the risk/benefit of performing some type of invasive intervention was evaluated. Given the location (areas of biopolymer infiltration), a high risk of soft tissue infection, and spillage of already encapsulated content within the area with subsequent initiation of an inflammatory response of unknown intensity, it was decided not to perform invasive procedures on the patient who has not presented any clinical recurrence to date. This conservative strategy allows for the monitoring of potential complications without exposing the patient to the risks of extraction surgery, which will only be considered if clinical abnormalities or significant changes in imaging arise, taking into account that there has been no clinical recurrence to date.
Conclusions
Considering this case where biopolymer implants can be a potential source of unexplained systemic symptoms and laboratory anomalies, regular monitoring and a comprehensive approach are essential for managing patients with these implants and preventing complications. Future guidelines should emphasize surveillance and consideration of complications related to biopolymers in differential diagnoses.
This study followed the principles of the Declaration of Helsinki. The patient provided written informed consent for the publication of this case report and the use of her clinical data. The identity of the patient has been protected to ensure confidentiality and privacy. The research was conducted in accordance with ethical standards, ensuring that all patient interactions prioritized well-being, respect, and autonomy.
Roles of the authors
Jhon Alexander Avila Rueda – conceptualization of the case report, clinical data collection, and primary manuscript drafting; Edgar Fabián Manrique-Hernández – analysis and interpretation of laboratory results, as well as critical revisions of the manuscript; Alexandra Hurtado-Ortiz – coordination of patient management, imaging studies, and drafting of clinical discussion; Maricel Licht-Ardila – supervision of the ethical considerations and patient consent process, ensuring compliance with the Declaration of Helsinki; Gianmarco Camelo-Pardo – statistical analysis and review of differential diagnoses, essential input on diagnostic processes; Alejandra Mendoza-Monsalve – final manuscript revision for intellectual content and assistance with journal submission.
Disclosure
The authors have no conflicts of interest to disclose. The authors declare that this study has received no financial support. All procedures performed in this study involving human participants were in accordance with ethical standards of the institutional and/or national research committee and with the Helsinki declaration and its later amendments or comparable ethical standards.
Sources
1. Duarte y Sanchez A., Hamid Hedo-Toledo A., Pradel-Mora J., et al. Complicación tardía tras infiltración de biopolímeros en glúteos. [online]. Available from: https: //scielo.isciii.es/scielo.php?script=sci_arttext&pid=S0376-7892201 6000400011.
2. Seeger JB., Ahmed GA., Basad E., et al. Gluteal silicone injections and total hip arthroplasty: a case report. J Med Case Rep. 2014, 8 : 140.
3. Ramos-Gallardo G., Cuenca-Pardo J., Cárdenas-Camarena L., et al. Morbidity induced by the infiltration of foreign substances into the buttocks: a systematic review. J Plast Reconstr Aesthet Surg. 2024, 91 : 135–153.
4. Andrès E., Serraj K., Zhu J., et al. The pathophysiology of elevated vitamin B12 in clinical practice. QJM 2013, 106 (6): 505–515.
5. Watad A., Bragazzi NL., Shoenfeld Y. (eds). Autoimmune disorders: adjuvants and other risk factors in pathogenesis. [online]. Available from: https: //books.google.com/books/about/Autoimmune_Disorders.html?id=kbwDEQAA QBAJ.
6. Zulfiqar A-A., Andres E., Villalba NL. Hipervitaminosis B12: nuestra experiencia y una revisión. Medicina 2019, 79 (5): 391–396.
7. Arendt JF., Sørensen HT., Horsfall LJ., et al. Elevated vitamin B12 levels and cancer risk in UK primary care: a THIN database cohort study. Cancer Epidemiol Biomarkers Prev. 2019, 28 (4): 814–821.
Jhon Alexander Avila Rueda
Oncology institute, Fundación Cardiovascular de Colombia
681012, Piedecuesta, Santander, Colombia
jhonavila@fcv.org
Submitted: 16. 10. 2024
Accepted: 26. 1. 2025
Labels
Plastic surgery Orthopaedics Burns medicine TraumatologyArticle was published in
Acta chirurgiae plasticae

Most read in this issue
- Comparison of lymphovenous anastomosis and vascularized lymph node transfer in lymphedema treatment – a literature review
- Possibilities of intranasal reconstruction in complex nasal defects
- Elevation of vitamin B12 levels attributed to biopolymer implants – a case report
- Landmarks in facial reanimation – a bibliometric analysis of the 50 most cited papers in dynamic facial reconstruction