
HETEROLOGOUS RECONSTRUCTION AND RADIOTHERAPY: THE ROLE OF LATISSIMUS DORSI FLAP AS A SALVAGE
Authors:
B. Cagli; M. J. Manzo; S. Tenna; L. Piombino; I. Poccia; P. Persichetti
Authors‘ workplace:
Campus Bio-Medico University of Rome, Plastic and Reconstructive Surgery Unit, Rome, Italy
Published in:
ACTA CHIRURGIAE PLASTICAE, 54, 2, 2012, pp. 45-51
INTRODUCTION
Immediate reconstruction with implants has many advantages due to technique’s simplicity, relatively low number of complications, duration of surgery, hospitalization time and good cosmetic result (1, 2).
Radiotherapy certainly represents an important risk factor for developing complications including alterations of the skin, ranging from simple erythema to skin necrosis, capsular contracture and peri prosthetic seroma (3).
For this reason in patients with history of previous radiotherapy or when is preoperatively known that will be required, many surgeons prefer to perform autologous or delayed reconstruction (4, 5).
Several recent studies have shown that eterologous breast reconstruction in two stages, expander-implant, represents a viable alternative to autologous reconstruction, even in selected patients undergoing radiation therapy, not affecting further eventual conversion (6, 7).
At our Department immediate reconstruction with expander is often attempted trying to replace the expander with the definitive implant after chemotherapy and before the beginning of radiation therapy (8–10).
Nevertheless some patients develop radio-induced or mechanical complications that seem to compromise the heterologous procedure.
The aim of this retrospective study was to evaluate the versatility and effectiveness of the latissimus dorsi flap as an adjunctive tool in complicated heterologous reconstruction with special regards to radiotherapy.
MATERIALS AND METHODS
The authors reviewed the files of 150 patients who underwent immediate postmastectomy reconstruction with tissue expander at the Campus Bio-Medico University Hospital of Rome from January 2000 to January 2010.
Twenty-eight patients, who developed complications of the heterologous reconstruction, and underwent heterologous reconstruction salving with latissimus dorsi flap, were included in this retrospective study and divided into three groups according to history of radiotherapy.
The first group (Group 1) included patients undergoing adjuvant radiotherapy after demolitive surgery; the second group (Group 2) included patients who had undergone salvage mastectomy after quadrantectomy and radiotherapy (QUART); the third group (Group 3) included patients with no history of pre and postoperative radiotherapy, who developed mechanical complications (control group).
Exclusion criteria were immediate breast reconstruction using the autologous flap, reconstruction of the chest wall, radiotherapy of the chest wall for other reasons than breast cancer and poor general condition due to advanced stages of the disease.
Patients were classified according to age, smoking habits, histology, stage of breast cancer, type and size of the implant, complications that required the salvage procedure (Table 1).

In Group 1 and Group 2 patients were treated with standard radiotherapy with 6MV Linear Accelerator (photons) with external beam technique against the chest wall or underarm for a total dose of 50.40 Gy with conventional fractionation (1 0.8 to 2 Gy/day). Patients undergoing cobalt therapy were excluded.
All patients had undergone previously an immediate breast reconstruction with biodimensional, textured, anatomical tissue expander with integrated valve Natrelle Style 133 MV (Allergan Inamed, Santa Barbara, Calif.). All expanders had been positioned using the same surgical technique, performed by the same surgeon, in a sub-musculofascial space created medially between the pectoralis major and the pectoralis minor, proximally and laterally in continuity with the serratus anterior muscle. The expansion was started about two weeks after surgery and continued regularly at weekly intervals. During chemotherapy, the expansion was suspended only in cases of severe neutropenia.
Group 1, including 15 patients, was affected by capsular contracture grade 3–4 in 66.5% and radiodermatitis in 40% (Table 2, Fig. 1–4).





Nine patients belong to Group 2 and presented with cutaneous fistula in 77.5% and capsular contracture in 33, 3% (Table 3, Fig. 5–7).




Heterogeneous complications were recorded in Group 3 including four patients (Table 4, Fig. 8–10).




All patients underwent latissimus dorsi salvage pedicled flap that has been harvested according to the clinical characteristics of the patients in different manner: musculo-cutaneous or muscular only, without a skin paddle, both in combination with the tissue expander, previously positioned.
Suction drains were applied to all the patients, both in the donating area of the flap and in correspondence of the recipient mammary area.
Upon completion of the expansion, the patients were subject expander replacement with a cohesive textured, anatomic, silicon based prosthetic implant, Natrelle Style 410 variants MM, MX, MF, LX and LF (Allergan Inamed, Santa Barbara, Calif.); the second reconstructive stage has required a radial capsulotomy and the reconstruction of the inframammary fold.
All patients followed the same medication protocol and medical adjuvant therapy according to international protocols and had a follow up of one year at least.
After the salvage surgery with the latissimus dorsi flap the following parameters were evaluated: surgery duration, hospitalization duration, complications, contralateral breast treatment, ancillary procedures, quality and stability of the aesthetic result.
The complication related to latissimus dorsi flap were classified according to the donor site complications, with seroma and phatological scars, and recipient site complications, with capsular contracture, partial necrosis of the flap, periprothetic infection, cutaneous fistula and periprothetic seroma.
The stability and quality were evaluated by the same plastic surgeon on the base of the pictures post-operative, following the photographic standards at 6 months and 1 year and, where be able, at maximum 5 years, using a valuation score from 1 to 4. (1= poor result, 2= sufficient result, 3= good, 4= excellent). For the final valuation was considered the average score from all the different evaluation.
Statistical analysis
We conducted a statistical analysis with χ2 test (chi square) to evaluate the significance of complications from heterologous reconstruction, evaluating them as discrete variables.
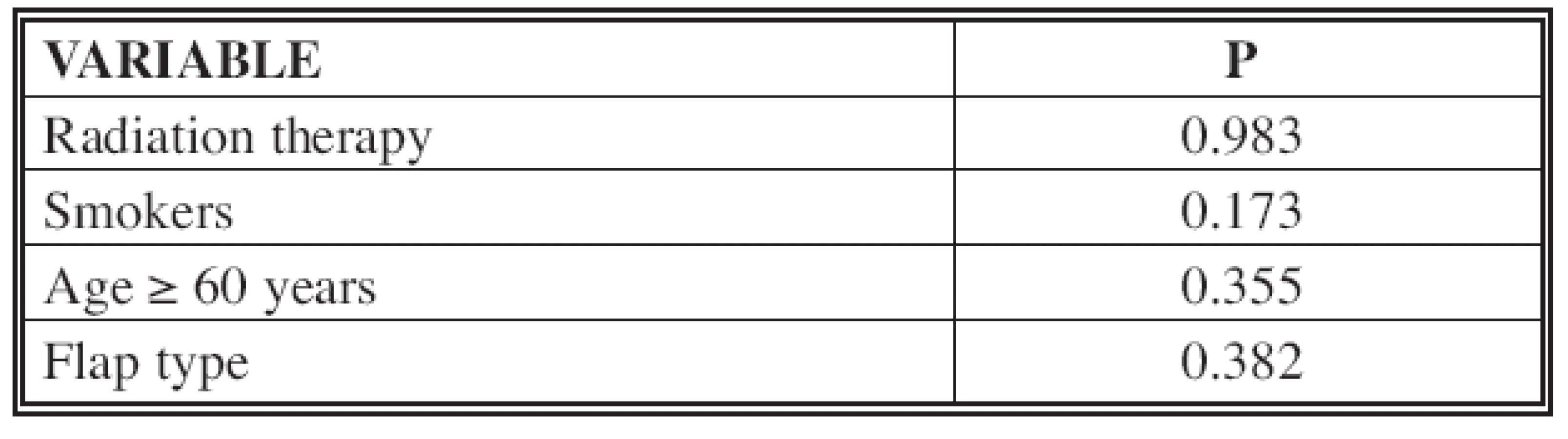
A uni-variated Log-rank analysis has been done to evaluate after flap reconstruction the correlation between the complications and the following prognostic factors: radiotherapy, smoking habit, flaps type, age.
A multivariate analysis with logistic Cox regression was also performed to evaluate the significance of prognostic factors such as radiotherapy, smoking, age and type of border for the development of complications after the salvage procedure.
All analyses were carried out using SPSS Statistics.
RESULTS
All flaps were viable and no necrosis or major complications related to the flap were registered.
In Group 1, musculo-cutaneous flap with tissue expander was performed in 11 patients (73.3%), the muscle variant in four patients (26.7%), with tissue expander in one case and permanent prosthesis in three cases. In Group 2, musculo-cutaneous flap was performed in five patients (55.5%), the muscle flap in four patients (45.5%), always with tissue expander. In Group 3, musculo-cutaneous flap was performed in one patient (25%), muscle flap in the remaining three cases (75%), always in association with a tissue expander.
The duration of surgery was between one and a half and three hours, with an average duration of 2 hours and 30 minutes.
The hospitalization time for the salvage surgery was 4 days for 17 patients (60.8%), 3 days for four patients (14.2%) and 2 days for seven patients (25 %), with an average time of hospitalization of 3.3 days.
Donor and recipient site complications were recorded as show in Table 5. These complications occurred in six patients with musculocutaneous flap (85.7%) and in one patient with muscular flap (14.3%). Considering both the complications on the donor and recipient site, eight patients (28.5%) developed complications after the flap reconstruction, with six of these patients complication (75%) belonged to Group 1 and Group 2. Five (62.5%) of the patients who developed complications were smokers.

Log-rank analysis results are showed in Table 6.

Multivariate analysis with logistic Cox regression led to the results showed in Table 7.
Of 25 patients with a tissue expander, 24 (96%) have replaced it with a permanent prosthesis, between 365 and 625grams, while, only one patient has not concluded the reconstruction, representing the only failure in the therapeutic process.
The contralateral breast surgery adjustment was performed in ten patients (35%): a breast reduction was performed in three patients (30%); a mastopexy was performed in six patients (60%), of which four (66.6%) required the aid of a prosthesis implant; breast augmentation was performed in one patient (10%). The nipple-areola complex reconstruction has been performed in 8 patients (28.5%). Eleven patients (39%) underwent ancillary procedures: in Group 1, seven patients (46.6%) underwent adipose transplantation with Coleman technique, and two patients (13.3%) had scar revision; in Group 2, four patients (44.4%) underwent adipose transplantation with Coleman technique; in Group 3, there has not been any ancillary procedure.
The evaluation of the cosmetic result and the stability of outcome over time has led to an assessment with a score of 3 in 17 patients (60.7%), score 4 in eight patients (28.6%), score 2 in two patients (7%) and a score of 1 in one patient (3.6%), distributed as follows: in Group 1, two patients (13.3%) had a score of 2, ten patients (66.6%) had a score of 3, three patients (20%) had a score of 4; in Group 2, one patient (11.1%) had a score of 1, five patients (55.5%) a score of 3, three patients (33.3%) had a score 4; in Group 3, two patients (50%) had a score of 3, two patients (50%) had a score of 4.
DISCUSSION
Radiotherapy certainly represents an important risk factor for developing complications following heterologous reconstructions and this relationship is undoubtedly stronger in patients that received adjuvant radiotherapy compared to those who have had previous radiotherapy (3).
The versatility and effectiveness of the latissimus dorsi flap in combination with implants is certainly well known and documented. Spear et al. in 2007 and Disa et al. in 2008 analyzed the results from a series of 28 and 57 patients respectively, who underwent latissimus dorsi flap reconstruction, with tissue expander or permanent prosthesis, demonstrating that this technique has cosmetically optimal results with manageable risks and complications (11, 12).
Other series also showed the autologous variant (“extended” latissimus dorsi) as a valid alternative to the abdominal flaps which remains the gold standard in autologous reconstruction (13–15).
Usually, in case of complications such as cutaneous fistula, implant exposure and severe capsular contracture, related or not to radiotherapy, autologous reconstruction is commonly recommended. Our experience adds a further indication introducing the use of latissimus dorsi flap combined with implant like a “life vest” in problematic heterologous reconstruction.
In selected patients, with previous multiple surgeries and psychological distress, this choice may be advisable due to limited scars and reduced operating time.
Our data also confirmed that patients with heterologous immediate reconstruction, requiring adjuvant radiotherapy, are burdened by a greater number of complications. Some studies have already proposed the replacement of the definitive implant before radiotherapy in order to decrease the risk of autologous reconstruction conversion (16, 17).
Analyzing the results appears that complications from heterologous reconstruction have a different distribution in the three groups.
Capsular contracture was more frequent in Group 1, followed by radiodermitis, demonstrating a direct relationship between radiotherapy and fibrosis.
Cutaneous fistula was more frequent in Group 2, confirming the chronic damage of radiation therapy.
In Group 3 the few and heterogeneous complications were all mechanical, outlighting the negative effect of radiation therapy on tissues.
In our review the results obtained with the univariate log-rank analysis for the recipient site complications have not proved to be statistically significant, we believe because of the small sample size recruited.
However the analysis of data shows how the prognostic factors studied were crucial in the development of these complications.
In particular, adjuvant radiation therapy was found to be the prognostic factor with the worst outcome, followed by the musculocutaneous variant of the flap and the smoking habit.
Patients age not seem to be a significant prognostic factor. In multivariate analysis, however, smoking became the most significant prognostic factor.
The aesthetic results were rated as good or excellent in most patients, with few cases of sufficient evaluation only in Group 1 and 2 with a single case of insufficient evaluation due to complete failure of the reconstructing process supporting the cosmetic outcome of this salvage technique.
CONCLUSION
Although the abdominal flaps remains the standard in reconstructing the mastectomy defect in the irradiated patient, there are occasions where a favorable, cosmetically satisfactory reconstruction can be achieved when combining an implant with a latissimus flap allowing the salvage of the complicated heterologous reconstruction.
Speed of execution, short hospitalization and recovery times observed, have shown the versatility of latissimus dorsi demonstrating the validity of this technique offering long-term stability and acceptable cosmetic results.
Address for correspondence:
Stefania Tenna, MD, Ph D
Via Alvaro del Portillo 200
Rome, Italy
E-mail s.tenna@unicampus.it
Sources
1. Cordeiro PG., McCarthy CM. A single surgeon’s 12-year experience with tissue expander/implant reconstruction: Part I. A prospective analysis of early complications. Plast. Reconstr. Surg., 118, 2006, p. 825–831.
2. Strock LL. Two-stage expander implant reconstruction: recent experience. Plast Reconstr Surg., 124(5), 2009, p. 1429–1436.
3. Krueger EA., Wilkins EG., Strawderman M. et al. Complications and patient satisfaction following expander/implant breast reconstruction with and without radiotherapy. Int. J. Radiat. Oncol. Biol. Phys., 49, 2001, p. 713–721.
4. Kronowitz SJ., Robb GL. Breast reconstruction with postmastectomy radiation therapy: Current Issues. Plast. Reconstr. Surg., 114(4), 2004, p. 950–60.
5. Kronowitz SJ., Robb GL. Radiation therapy and breast reconstruction: A critical review of the literature. Plast. Reconstr. Surg., 124(2), 2009, p. 395–408.
6. Ascherman JA., Hanasono MM., Newman MI. et al. Implant reconstruction in breast cancer patients treated with radiation therapy. Plast. Reconstr. Surg., 117(2), 2006, p. 359–365.
7. Persichetti P., Cagli B., Simone P. et al. Implant breast reconstruction following salvage mastectomy in previously irradiated patients. Ann. Plast. Surg., 62(4), 2009, p. 350-354.
8. Mc Carthy CM., Pusic AL., Disa JJ. et al. Unilateral postoperative chest wall radiotherapy in bilateral tissue expander/implant reconstruction patients: a prospective outcomes analysis. Plast. Reconstr. Surg., 116(6), 2005, p. 1642–1647.
9. Cordeiro PG., Pusic AL., Disa JJ. et al. Irradiation after immediate tissue expander/implant breast reconstruction: outcomes, complications, aesthetic results, and satisfaction among 156 patients. Plast .Reconstr. Surg., 113(3), 2004, 877–881.
10. Nava MB., Pennati AE., Lozza L. et al. Outcome of different timings of radiotherapy in implant-based breast reconstructions. Plast. Reconstr. Surg., 128(2), 2011, p. 353–359.
11. Spear SL, Boehmler JH, Taylor NS et al. Plast Reconstr Surg. 2007 Jan;119(1):1-9; discussion 10-1.
12. Disa JJ., McCarthy CM., Mehrara BJ. et al. Immediate latissimus dorsi/prosthetic breast reconstruction following salvage mastectomy after failed lumpectomy/irradiation. Plast. Reconstr. Surg., 121(4), 2008, p. 159e–164e;
13. Chang DW., Youssef A., Cha S. et al. Autologous breast reconstruction with the extended latissimus dorsi flap. Plast. Reconstr. Surg.,110(3), 2002, p. 751-759; discussion 760-761.
14. Heitmann C., Pelzer M., Kuentscher M. et al. The extended latissimus dorsi flap revisited. Plast. Reconstr .Surg., 111(5), 2003, p. 1697–1701.
15. Rifaat MA., Amin AA., Bassiouny M. et al. The extended latissimus dorsi flap option in autologous breast reconstruction: A report of 14 cases and review of the literature. Indian J. Plast. Surg., 41(1), 2008, p. 24–33.
16. Cordeiro PG., Pusic AL., Disa JJ. et al. Plast. Reconstr. Surg., 113(3), 2004, p. 877–881.
17. Nava MB., Pennati AE., Lozza L. et al. Outcome of different timings of radiotherapy in implant-based breast reconstructions. Plast. Reconstr. Surg., 128(2), 2011, p. 353–359.
Labels
Plastic surgery Orthopaedics Burns medicine TraumatologyArticle was published in
Acta chirurgiae plasticae

2012 Issue 2
Most read in this issue
- GIANT MALIGNANT MELANOMA: A CASE REPORT
- HETEROLOGOUS RECONSTRUCTION AND RADIOTHERAPY: THE ROLE OF LATISSIMUS DORSI FLAP AS A SALVAGE
- CLINICAL TRIAL OF THE TEMPORARY BIOSYNTHETIC DERMAL SKIN SUBSTITUTE BASED ON A COLLAGEN AND HYALURONIC ACID NAMED COLADERM H/HM, FIRST PART
- EXTENSION OF OROFACIAL CLEFT SIZE AND GESTATIONAL BLEEDING IN EARLY PREGNANCY