
Re-irradiation in high-grade gliomas – a topic still under debate
Authors:
C. C. Mirestean 1; R. I. Iancu 2,3; D. P. T. Iancu 1,2
Published in:
Cesk Slov Neurol N 2025; 88(2): 89-94
Category:
Review Article
doi:
https://doi.org/10.48095/cccsnn202589
Overview
Even after administration of a maximal standard treatment, including gross surgical resection, adjuvant radiotherapy plus concurrent and subsequently adjuvant chemotherapy with an alkylating agent, temozolomide (TMZ), a regimen validated by phase III clinical trials, the overall survival in glioblastoma (GB), which is the most frequent and malignant subtype of high-grade glioma, remains limited. With a 5-year survival rate below 10%, local recurrence is the usual cause of death. Re-operation, re-challenge with alkylating agents including TMZ or treatment of relapse with lomustine, and re-irradiation are the most frequently proposed alternatives to purely palliative treatment. Re-irradiation seems to be an option for GB in carefully selected cases, and the choice of irradiation method between standard fractionation, stereotactic hypo-fractionated radiotherapy, and stereotactic radiosurgery must take into account technical and patient-related factors and relapse pattern. The use of alkylating agents TMZ and lomustine, in combination with re-irradiation, seems to be a strategy with benefits especially after a selection of therapy based on the methylation status of the O6-methylguanine-DNA-methyltransferase promoter. Neo-adjuvant immunotherapy and identification of molecular biomarkers, more precise delineation of the target volume, based on amino-acid positron emission tomography/CT (PET-CT), but also the use of glycolytic inhibitors in association with anti-vascular endothelial growth factor agents are future research directions. Limiting the cumulative equivalent dose in 2 Gy (EQD2) received by the brain tissue to 100 Gy in the case of ultra-hypo-fractionated regimens and to < 120 Gy EQD2 in the case of other fractionation schemes could limit the risk of cerebral radio-necrosis below 10%.
Keywords:
Stereotactic radiosurgery – radiotherapy – glioblastoma – re-irradiation – temozolomide – O6-methylguanine- DNA-methyltransferase – lomustine – hypo-fractionated stereotactic radiotherapy – radio-necrosis
Introduction
Primary tumors of the CNS, including glioma, astrocytoma, embryonal tumors, meningioma, and medulloblastoma, affect 7 out of 100,000 people, with glioblastoma (GB) being the most malignant form of a high-grade glioma (HGG) [1–4].
The current standard treatment is the result of phase III trials including maximal surgical resection followed by radiotherapy in combination with temozolomide (TMZ), followed by TMZ as adjuvant treatment for another 6–12 cycles. However, the 5-year survival rate is low, currently estimated at < 10% [5,6]. This narrative review aims to evaluate the main aspects, challenges, therapeutic options, and research directions in re-irradiation of relapsed HGG.
Current standard in the GB multimodal approach
As demonstrated by the ETERNITY study, rapid progression of GB is a predictor of lower overall survival (OS). Treatment is also a prognostic factor, with biopsy without debulking resection being associated with median OS of 6.8, 4.7, and 8 months in 3 different cohorts. In the case of surgery in the same cohort of patients, the median OS was 17.2, 14.9, and 15.6 months. In the absence of any oncological treatment, the median OS was 1.8 months in a study from France, but it is generally accepted that the median OS in the absence of any active oncological treatment is 3–4 months. Regarding radiotherapy, a net advantage was if a dose of 50–60 Gy was administered during post-surgical resection, without any benefit if the dose is escalated beyond this value. However, a dose above 60 Gy was associated with a significant increase in the rate of toxicities without any differences in OS [7–11].
The use of modern radiotherapy techniques that have reduced the dose to healthy tissue in the vicinity of the target volume could limit the rate of treatment-related toxicities. Administration of treatment using the intensity modulated radiation therapy (IMRT) technique reduced the volume of a healthy brain receiving 18, 24, and 45 Gy by 10%, 14%, and 40%, respectively, compared to cases in which 3D-conformal radiation (3D-CRT) was administered. In the case of the brainstem, IMRT technique reduced the volume receiving > 45 Gy by 31%. The use of radiobiological models also demonstrated an increase in the rate of tumor control probability and a decrease in normal tissue complication probability by using IMRT. Initially, the indication of the IMRT technique was for cases where there is overlap between the target volume and critical organs in order to better spare at least part of the organ at risk. In elderly patients, short-course hypo-fractionated radiotherapy (40 Gy in 15 fractions) plus TMZ demonstrated a benefit and this has become a standard of care, both in cases with methylated O6-methylguanine–DNA methyl-transferase (MGMT) and in cases with unmethylated MGMT, although the benefit is higher in cases with methylated MGMT. For the category of patients with unmethylated MGMT, an accelerated hypo-fractionated protocol of 52.5 Gy in 15 fractions is also safe and effective [12–15].
The objective of the GRIPS study, a multicenter trial that includes 326 cases, is to compare the IMRT technique in the standard arm with the Proton beam therapy experimental arm. The study also includes data on the standard or hypo-fractionated regimen and the target volume inclusion of the sub-ventricular zone and on the administration of concurrent chemotherapy. The standard regimens include 30 fractions of 2 Gy or 33 fractions of 1.8 Gy, while the hypo-fractionated regimen consists of 15 fractions of 2.67 Gy. This trial is still ongoing and results will likely be available at the end of 2027. The primary objective of the study is the cumulative toxicity rate in the first 4 months after therapy and secondary objectives are OS, progression-free survival (PFS), quality of life (QoL), and neurocognition [16].
Glioblastoma – options beyond disease progression
At the time of disease progression, therapeutic options are limited. There are several factors that could be considered in the decision to perform surgical re-intervention, including Karnofsky Performance Score (KPS) > 70 and more than 6 months interval between surgeries being prognostic factors for survival, where data are already being confirmed by meta-analyses. Recurrence volume < 50 cm3 and KPS ≥80 were also correlated with survival. In the article “Recurrent glioblastoma multiforme, when should we reoperate?” Barbagallo et al. mentioned an age ≤ 50 years, but also KPS as factors associated with a survival benefit if surgical re-intervention was performed; this also delays relapse, with a reduction in the need for corticosteroids and with an improved QoL. While there is no consensus regarding the decision to re-operate for recurrence in GB, there is a consensus that the possibility of performing a total gross resection and the initial subtotal operation should be deciding factors for reoperation. Franceschi et al. noted a minimal benefit of the second operation, with MGMT methylation status and PFS being identified as prognostic factors [8,17,18].
The Food and Drug Administration (FDA) approved an anti-angiogenic agent, bevacizumab, in the treatment of relapsed GB in 2009. The validation studies were phase II trials, where initially bevacizumab was being associated with a topoisomerase inhibitor (irinotecan). With a 6-month PFS rate of 42.6% and 50.3% in the bevacizumab arm as a single agent or in combination with irinotecan, the BRAIN study also identified higher rates of adverse events, 46% and 66% in the monotherapy arm and the dual combination arm including irinotecan, respectively. The phase II trial conducted in 14 hospitals in the Netherlands called BELOB identified a benefit only when bevacizumab was associated with the alkylating nitrosourea compound administered orally named lomustine, which also mentioned the futility of launching trials investigating the benefit of bevacizumab alone. Although the EORTC 26101 trial identified a 2.7-month benefit in PFS (4.2 months vs 1.5 months) in favor of the combination of bevacizumab and lomustine, the EORTC 26101 trial did not report a benefit in OS by adding bevacizumab to lomustine, but reported a 63.6% rate of grade 3–5 toxicities in the case of treatment with both agents. In this study, MGMT methylation was identified as a prognostic factor. Also, the generation of a hypoxic environment by suppressing angiogenesis may lead to an activation of glycolysis and tumor proliferation, possibly requiring the association of a glycolytic inhibitor in the study protocols [1,19–22].
Temozolomide, the most widely used alkylating agent in GB, has proven benefits especially in cases where the O6-MGMT protein promoter is methylated; these cases are being associated with an increased sensitivity to chemotherapy compared to GB cases with un-methylated MGMT status. Re-challenge with TMZ at the time of progression was the subject of a study proposed by Franceschi et al. The trial included 106 cases that had at least 8 weeks between the completion of radio-chemotherapy and adjuvant chemotherapy with TMZ, and cases without progressive disease at the first imaging follow-up [23].
The randomized phase III placebo-controlled, partially blinded REGAL trial was evaluating another inhibitor of vascular endothelial growth factor (VEGF), Cediranib alone or in combination with lomustine in recurrent GB. The primary endpoint of the study was PFS, and the secondary endpoint was OS. The study objectives were not met, but the group that combined lomustine with cediranib reported 80% of grade 3 or higher toxicities compared to 60% in the arm treated with lomustine alone or cediranib alone. However, this trial also has some positive aspects. Anti-VEGF therapy could lead to a reduction in the need for corticosteroids and a delay in neurological decline, identifying subgroups that will benefit from anti-VEGF therapy at recurrence remains the subject of future research. The AGILE translational trial aims to identify possible biomarkers for stratifying therapy in recurrent GB [24,25].
To identify patients with recurrent GB after TMZ concurrent with radiotherapy and subsequent adjuvant which might benefit from re-challenge with TMZ at the time of disease progression, the study compared TMZ-based chemotherapy and nitrosourea-based chemotherapy in cases with a treatment-free interval of ≥ 5 months, with the median OS being 17.7 vs 11.6 months in favor of TMZ. In conclusion, the authors note that a treatment-free interval of ≥ 5 months is a predictor of response to re-challenge with TMZ. Continuous daily treatment with TMZ at 50 g/m2 at the time of progression appears to be a feasible option with an acceptable toxicity profile including lymphopenia. Wick et al. noted a benefit in re-challenge with TMZ whether re-challenge was proposed after initial failure of TMZ therapy or there was a progression-free interval and an initial response [26,27].
Alternating electric fields of intermediate frequencies, also called tumor treating fields (TTFields or TTF), are based on action at the cell cycle level by interfering with the metaphase-anaphase transition, resulting in mitotic catastrophe or cell death by aberrant exit from mitosis. Alteration of cytokinetic cleavage induces immunogenic cell death, which could enhance the antitumor response of the host. The combination of TTF with TMZ in the adjuvant setting was beneficial compared to the administration of TMZ as a single treatment. With a net benefit (11.8 vs 9.2 months) for patients who were treated with TMZ plus TTF or TMZ alone and received 2nd line chemotherapy + TTF after progression, the EF-14 trial (NCT00916409) demonstrates the role of TTF in association with systemic treatment after recurrence [28,29].
Epidermal growth factor receptor (EGFR) amplification expresses mutant receptor EGFRvIII identified in approximately 40% of GB cases which justifies the evaluation in clinical trials of EGFR inhibitors such as erlotinib and gefitib, but also third-generation agents such as osimetrinib. Neither the EGFR inhibitors of generation I nor the bevacizumab/osimetrinib association generated notable results, where the blockade of the PI3K/AKT/mTOR pathway was a new research direction due to the potential effect of increasing TMZ cytotoxicity and decreasing resistance to alkylating agents [30,31].
Regarding immunotherapy, the results are mainly summarized in terms of tolerance and toxicity profile without specific data regarding survival benefit. For the programmed death 1 (PD-1) inhibitor nivolumab, a possible benefit is outlined for patients who associate the methylated status of MGMT with the association of pembrolizumab, another PD-1 inhibitor with bevzicumab that seems to increase the disease control rate. A favorable safety profile was reported by associating radiotherapy with a dual angiogenic and immune checkpoint blockade. However, neoadjuvant administration of immunotherapy seems promising, with evidence of a benefit in the immune-mediated tumor response and possibly in OS. The programmed death ligand 1 (PD-L1) inhibitors atezolizumab, durvalumab, and avelumab have been evaluated from the point of view of safety profile, but to date there are no conclusive data on OS benefit. avelumab, which was tested in association with another VEGF inhibitor (axitinb) demonstrated a benefit, but without statistical significance, in the development of new brain metastases. The anti-CTLA4 antibody, ipilimumab, combined with the PD-1 inhibitor nivolumab administered intratumorally has demonstrated safety and a favorable outcome even in OS, opening horizons for intratumoral administration of immunotherapy [32,33].
Re-irradiation of recurrent GB – between controversies and challenges
The number of studies reporting data on the option of re-irradiation with a potentially curative goal provides a solid basis for establishing the safety and feasibility of re-irradiation. Both conventional and hypo-fractionated radiation regimens have been proposed, with doses generally ranging from 15 to 36 Gy. Median survival generally ranges from 7 to 13 months, and the risk of radio-necrosis is considered low, generally < 10% [34].
Analyzing seventy published articles, which included 3302 patients that were all initially irradiated with a curative intent for a total dose of 60 Gy in 30 fractions, a correlation was identified between median OS and irradiation technique after adjustment for age, re-irradiation dose, and equivalent biological dose in standard fractionation (EQD2). The interval between irradiation and re-irradiation sessions was also a factor involved in prognosis. Superior results in OS were identified in the case of using single fraction stereotactic radiosurgery (SRS), (12.2 months), followed by hypo-fractionated stereotactic radiotherapy (10.1 months). In the case of using conventional fractionation in the re-irradiation regimen, the median OS was only 8.9 months. Even though the study argues for a benefit of single fraction radiosurgery in recurrent GB re-irradiation, the authors mention that there could be a selection bias and it cannot be stated with certainty whether there is superiority of the SRS technique in this case. The study validates the option of re-irradiation by any of the 3 techniques mentioned above, where the results and toxicity profile are favorable. Using SRS and fractionated stereotactic radiotherapy (fSRT) for salvage therapy of recurrent GB, Gigliotti et al. reported a median OS of 9 months and a 29% OS rate at 1 year, with re-irradiation being delivered with a linear accelerator (LINAC) for a total dose of 25 Gy in 5 fractions. This study also reports low toxicity rates and advocates the use of these techniques in re-irradiation of recurrent GB [35,36].
Almost 20 years ago, Grosu et al. proposed the first clinical trial including re-irradiation using fSRT and TMZ, where image--guided radiotherapy was used in all cases. Target volumes were delineated using (11) C-methionine positron emission tomography (MET-PET) or 123I-alpha-methyl-tyrosine (IMT) single-photon computed emission tomography (SPECT) /CT fused with simulation CT. Radiotherapy was administered for a total dose of 30 Gy in 6 fractions of 5 Gy for 6 consecutive days, preceded by 2 cycles of TMZ 200 mg/m2. Even though the median OS was 8 months in the study, significant differences (9 months vs. 5 months) were observed in OS between cases for which treatment planning was performed based on PET-CT/SPECT fusion with CT planning compared to cases in which radiotherapy planning was based on MRI-CT fusion, respectively. Longer interval between first treatment and recurrence, and interval to retreatment and TMZ were identified as prognostic factors. Amino-acid PET (AA-PET) and the concept of biological dose painting for delineation of the target volume of re-irradiation was exploited in a phase II trial (NOA 10/ARO 2013-1). The study has multiple endpoints, from the evaluation of the re-irradiation benefit in term of OS, in the toxicity profile, to comparative evaluation of QoL using the EORTC QLQ-C15 PAL questionnaire and to the comparison of the of re-irradiation target volume delineated on AA-PET versus MRI [37–39].
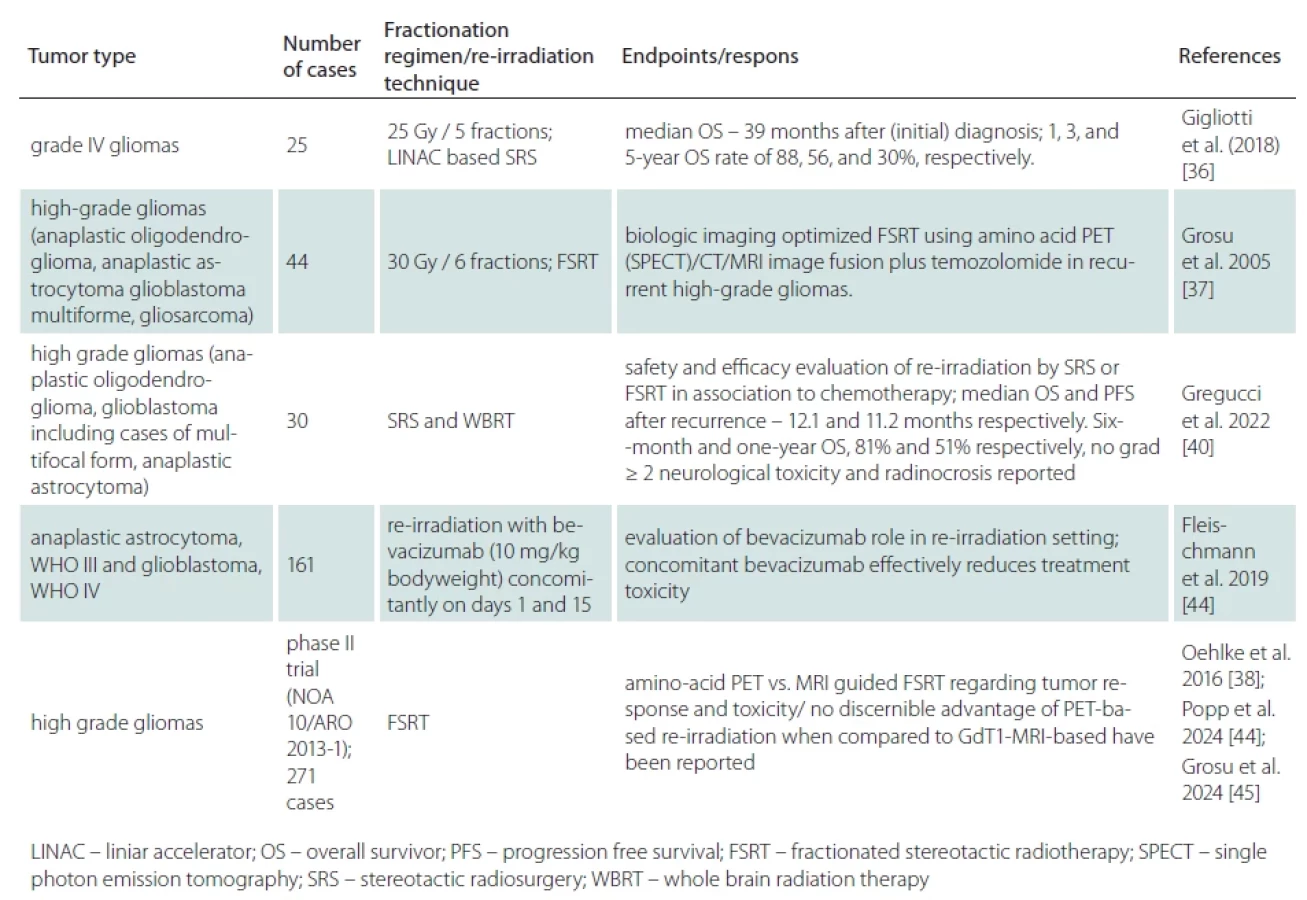
Analyzing the tolerance of treatment with re-radiation fSRT or SRS treated with second-line chemotherapy, Gregucci et al. analyzed the outcomes of patients with HGG. It is important to note the heterogeneity of tumor types, but also of the treatment for relapse, including multifocal form of GB. At 13 months after relapse, 33% of patients were alive, and of the deaths, 75% were due to disease progression. Even if the toxicity profile regarding radio-necrosis was favorable, the authors mentioned hematological toxicity, septic or thromboembolism-associated deaths and even wound dehiscence in a case treated with regorafenib. However, the study advocated for the possibility of using second-line chemotherapy after relapse in association with local treatment [40].
Limiting the cumulative dose around the EQD2 value of 120 Gy is considered a dosimetric endpoint that reduces the risk of cerebral radio-necrosis to < 10%, but an increase in the cumulative EQD2 dose to 132 Gy increases the risk of toxicity to 24%. Taking this into account, most cases were treated with a total dose in the first therapeutic sequence of 60 Gy in a standard fractionation regimen, so we could consider as a recommendation to limiting EQD2 to a maximum of 60 Gy in the second treatment sequence. Limiting the volume treated in SRS to 10 ml for doses of 15 Gy is associated as an acceptable risk of brain necrosis to approximately 8%. Also, limiting the margin from the clinical target volume to the planning target volume to 2 mm is acceptable to reduce the risk of cerebral necrosis. However, if SRS or ultra-hypo-fractionated regimens are administered, a cumulative EQD2 dose of a maximum of 100 Gy is recommended; this finding is based on the concept that the linear quadratic model cannot provide an accurate dose equivalence at fractions > 10 Gy, and using the 120 Gy EQD2 threshold value in this situation could underestimate the risk of late toxic effects [41–44].
Rahman et al. identified several factors for and against re-irradiation, among those advocating for re-irradiation, a long interval between recurrence and the first treatment, a limited recurrence in volume, a favorable performance status, and good tolerance to the first treatment. Anatomical location of target volume related to severe risk of toxicity after re-irradiation is also a decisive factor. Multifocal recurrences, frail patients and poor performance status, the patient‘s desire to receive other active treatment or palliative treatment, and alternative options with a lower risk of side effects are also factors against re-irradiation [34]. Studies that include different approaches to radiation in recurrent HGG have been summarized in Tab. 1.
Re-irradiation in GBs – steps towards standardization
Recently, the European Association for Neuro-Oncology/European Society for Radiotherapy and Oncology (ESTRO/EANO) recommendations regarding re-irradiation of GB were published. The main proposed directions are based on expert consensus and statistical data analysis and are discussed in 9 questions. KPS is considered a major factor in the decision to initiate re-irradiation, a minimum interval of 6 months since the last irradiation is recommended. T1-weighted MRI is the recommended imaging, being complemented by other protocols including MR perfusion, MRI spectroscopy, and PET-CT imaging with amino acids. The use of 3–5 mm margins from the gross tumor volume to the clinical target volume and a fractionation of 35 Gy in 10 fractions is also proposed. For small tumor recurrences, the authors recommend hypofractionated regimens of 30 Gy in 5–6 fractions and even stereotactic irradiation [47]. Dose summation using EQD2 and a/b values = 3 are proposed for dose summation to risk organs, and the use of alkylating agents such as lomustine and temodolomide, but also antiangiogenics such as bevacizumab is accepted. Regarding follow-up, it is recommended to use the initial plan to differentiate radionecrosis from progression and avoid declaring a progression on MRI performed at 6 weeks [48].
Conclusions
Re-irradiation is an option for GB in carefully selected cases, and the choice of technique between standard fractionation, hipofractionated stereotactic radiation therapy, and SRS should take into account technical and patient disease-related factors. The use of alkylating agents TMZ and lomustine in combination with re-irradiation seems to be a beneficial strategy especially after a selection of therapy based on MGMT methylation. Neo-adjuvant immunotherapy and the identification of molecular biomarkers as well as more precise delineation of the target volume based on amino-acid PET-CT, but also the use of glycolytic inhibitors in combination with anti-VEGF agents are future research directions.
Conflict of interest
The authors declare they have no potential conflicts of interest concerning drugs, products, or services used in the study.
Sources
1. Birk HS, Han SJ, Butowski NA. Treatment options for recurrent high-grade gliomas. CNS Oncol 2017; 6 (1): 61–70. doi: 10.2217/cns-2016-0013.
2. Apuzzo MLJ. Malignant cerebral glioma. American Association of Neurological Surgeons; Park Ridge, USA: 1990. pp. 79–89.
3. Pranckeviciene A, Bunevicius A. Depression screening in patients with brain tumors: a review. CNS Oncol 2015; 4 (2): 71–78. doi: 10.2217/cns.14.60.
4. Salari N, Ghasemi H, Fatahian R et al. The global prevalence of primary central nervous system tumors: a systematic review and meta-analysis. Eur J Med Res 2023; 28 (1): 39. doi: 10.1186/s40001-023-01011-y.
5. Stupp R, Mason WP, van den Bent MJ et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 2005; 352 (10): 987–996. doi: 10.1056/NEJMoa043330.
6. Stupp R, Hegi ME, Mason WP et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol 2009; 10 (5): 459–466. doi: 10.1016/S1470-2045 (09) 70025-7.
7. Fabbro-Peray P, Zouaoui S, Darlix A et al. Association of patterns of care, prognostic factors, and use of radiotherapy-temozolomide therapy with survival in patients with newly diagnosed glioblastoma: a French national population-based study. J Neurooncol 2019; 142 (1): 91–101. doi: 10.1007/s11060-018-03065-z.
8. Weller M, Cloughesy T, Perry JR et al. Standards of care for treatment of recurrent glioblastoma – are we there yet? Neuro Oncol 2013; 15 (1): 4–27. doi: 10.1093/neuonc/nos273.
9. Weller M, Reifenberger G, Le Rhun E et al. Molecular genetic, host-derived and clinical determinants of long-term survival in glioblastoma: First results from the ETERNITY study (EORTC 1419). J Clin Oncol 2019; 37 (suppl 15) 2056–2056. doi: 10.1200/JCO.2019.37.15_suppl. 2056.
10. Barani IJ, Larson DA. Radiation therapy of glioblastoma. Cancer Treat Res 2015; 163 : 49–73. doi: 10.1007/978-3-319-12048-5_4.
11. Pöhlmann J, Weller M, Marcellusi A et al. High costs, low quality of life, reduced survival, and room for improving treatment: an analysis of burden and unmet needs in glioma. Front Oncol 2024; 14 : 1368606. doi: 10.3389/fonc.2024.1368606.
12. Perlow HK, Prasad RN, Yang M et al. Accelerated hypofractionated radiation for elderly or frail patients with a newly diagnosed glioblastoma: a pooled analysis of patient-level data from 4 prospective trials. Cancer 2022; 128 (12): 2367–2374. doi: 10.1002/cncr.34192.
13. MacDonald SM, Ahmad S, Kachris S, Vogds BJ et al. Intensity modulated radiation therapy versus three-dimensional conformal radiation therapy for the treatment of high-grade glioma: a dosimetric comparison. J Appl Clin Med Phys 2007; 8 (2): 47–60. doi: 10.1120/jacmp.v8i2.2423.
14. Perry JR, Laperriere N, O‘Callaghan CJ et al. Short-course radiation plus temozolomide in elderly patients with glioblastoma. N Engl J Med 2017; 376 (11): 1027–1037. doi: 10.1056/NEJMoa1611977.
15. Minniti G, Scaringi C, Lanzetta G et al. Standard (60 Gy) or short-course (40 Gy) irradiation plus concomitant and adjuvant temozolomide for elderly patients with glioblastoma: a propensity-matched analysis. Int J Radiat Oncol Biol Phys 2015; 91 (1): 109–115. doi: 10.1016/j.ijrobp.2014.09.013.
16. König L, Jäkel C, von Knebel Doeberitz N. Glioblastoma radiotherapy using intensity modulated Radiotherapy (IMRT) or proton radiotherapy – GRIPS Trial (Glioblastoma Radiotherapy via IMRT or Proton BeamS): a study protocol for a multicenter, prospective, open-label, randomized, two-arm, phase III study. Radiat Oncol 2021; 16 : 240. doi: 10.1186/s13014-021-01962-8.
17. Barbagallo GM, Jenkinson MD, Brodbelt AR. Recurrent‘ glioblastoma multiforme, when should we reoperate? Br J Neurosurg 2008; 22 (3): 452–455. doi: 10.1080/02688690802182256.
18. Franceschi E, Bartolotti M, Tosoni A et al. The effect of re-operation on survival in patients with recurrent glioblastoma. Anticancer Res 2015; 35 (3): 1743–1748.
19. Taal W, Oosterkamp HM, Walenkamp AM et al. Single-agent bevacizumab or lomustine versus a combination of bevacizumab plus lomustine in patients with recurrent glioblastoma (BELOB trial): a randomised controlled phase 2 trial. Lancet Oncol 2014; 15 (9): 943–953. doi: 10.1016/S1470-2045 (14) 70314-6.
20. Friedman HS, Prados MD, Wen PY et al. Bevacizumab alone and in combination with irinotecan in recurrent glioblastoma. J Clin Oncol 2009; 27 (28): 4733–4740. doi: 10.1200/JCO.2008.19.8721.
21. Wick W, Gorlia T, Bendszus M et al. Lomustine and bevacizumab in progressive glioblastoma. N Engl J Med 2017; 377 (20): 1954–1963. doi: 10.1056/NEJMoa1707358.
22. Mireștean CC, Iancu RI, Iancu DPT. New horizons in modulating the radio-sensitivity of head and neck cancer – 100 years after Warburg‘ effect discovery. Front Oncol 2022; 12 : 908695. doi: 10.3389/fonc.2022.908695.
23. Franceschi E, Lamberti G, Visani M et al. Temozolomide rechallenge in recurrent glioblastoma: when is it useful? Future Oncol 2018; 14 (11): 1063–1069. doi: 10.2217/fon-2017-0681.
24. Batchelor TT, Mulholland P, Neyns B et al. Phase III randomized trial comparing the efficacy of cediranib as monotherapy, and in combination with lomustine, versus lomustine alone in patients with recurrent glioblastoma. J Clin Oncol 2013; 31 (26): 3212–3218. doi: 10.1200/JCO.2012.47.2464.
25. Alexander BM, Ba S, Berger MS et al. Adaptive global innovative learning environment for glioblastoma: GBM AGILE. Clin Cancer Res 2018; 24 (4): 737–743. doi: 10.1158/1078-0432.CCR-17-0764.
26. Perry JR, Rizek P, Cashman R et al. Temozolomide rechallenge in recurrent malignant glioma by using a continuous temozolomide schedule: the “rescue” approach. Cancer 2008; 113 (8): 2152–2157. doi: 10.1002/cncr. 23813.
27. Wick A, Pascher C, Wick W et al. Rechallenge with temozolomide in patients with recurrent gliomas. J Neurol 2009; 256 (5): 734–741. doi: 10.1007/s00415-009 - 5006-9.
28. Wong ET, Lok E, Swanson KD. Alternating electric fields therapy for malignant gliomas: from bench Observation to clinical reality. Prog Neurol Surg 2018; 32 : 180–195. doi: 10.1159/000469690.
29. Kesari S, Ram Z; EF-14 Trial Investigators. Tumor-treating fields plus chemotherapy versus chemotherapy alone for glioblastoma at first recurrence: a post hoc analysis of the EF-14 trial. CNS Oncol 2017; 6 (3): 185–193. doi: 10.2217/cns-2016-0049.
30. Chen L, Han L, Shi Z et al. LY294002 enhances cytotoxicity of temozolomide in glioma by down-regulation of the PI3K/Akt pathway. Mol Med Rep 2012; 5 (2): 575–579. doi: 10.3892/mmr.2011.674.
31. Cardona AF, Jaramillo-Velásquez D, Ruiz-Patiño A et al. Efficacy of osimertinib plus bevacizumab in glioblastoma patients with simultaneous EGFR amplification and EGFRvIII mutation. J Neurooncol 2021; 154 (3): 353–364. doi: 10.1007/s11060-021-03834-3.
32. Awada G, Ben Salama L, De Cremer J et al. Axitinib plus avelumab in the treatment of recurrent glioblastoma: a stratified, open-label, single-center phase 2 clinical trial (GliAvAx). J Immunother Cancer 2020; 8 (2): e001146. doi: 10.1136/jitc-2020-001146.
33. Olivet MM, Brown MC, Reitman ZJ et al. Clinical applications of immunotherapy for recurrent glioblastoma in adults. Cancers (Basel) 2023; 15 (15): 3901. doi: 10.3390/cancers15153901.
34. Rahman R, Preusser M, Tsien C et al. The role of reirradiation in recurrent glioblastoma. Neuro-Oncology 2024: noae209. doi: 10.1093/neuonc/noae209.
35. Shanker M, Chua B, Bettington C et al. Re-irradiation for recurrent high-grade gliomas: a systematic review and analysis of treatment technique with respect to survival and risk of radionecrosis. Neurooncol Pract 2019; 6 (2): 144–155. doi: 10.1093/nop/npy019.
36. Gigliotti MJ, Hasan S, Karlovits SM et al. Re-irradiation with stereotactic radiosurgery/radiotherapy for recurrent high-grade gliomas: improved survival in the modern era. Stereotact Funct Neurosurg 2018; 96 (5): 289–295. doi: 10.1159/000493545.
37. Grosu AL, Weber WA, Franz M et al. Reirradiation of recurrent high-grade gliomas using amino acid PET (SPECT) /CT/MRI image fusion to determine gross tumor volume for stereotactic fractionated radiotherapy. Int J Radiat Oncol Biol Phys 2005; 63 (2): 511–519. doi: 10.1016/j.ijrobp.2005.01.056.
38. Oehlke O, Mix M, Graf E et al. Amino-acid PET versus MRI guided re-irradiation in patients with recurrent glioblastoma multiforme (GLIAA) – protocol of a randomized phase II trial (NOA 10/ARO 2013-1). BMC Cancer 2016; 16 (1): 769. doi: 10.1186/s12885-016-2806-z.
39. Amino-acid PET versus MRI guided re-irradiation in patients with recurrent glioblastoma multiforme (GLIAA). [online]. Available from: https: //clinicaltrials.gov/study/NCT01252459?cond=NCT01252459&rank=1.
40. Gregucci F, Surgo A, Carbonara R et al. Radiosurgery and stereotactic brain radiotherapy with systemic therapy in recurrent high-grade gliomas: is it feasible? Therapeutic strategies in recurrent high-grade gliomas. J Pers Med 2022; 12 (8): 1336. doi: 10.3390/jpm12081336.
41. Mireștean CC, Iancu RI, Iancu DPT. Micro-RNAs, the cornerstones of the future of radiobiology in head and neck cancers? Curr Oncol 2022; 29 (2): 816–833. doi: 10.3390/curroncol29020069.
42. Minniti G, Niyazi M, Alongi F et al. Current status and recent advances in reirradiation of glioblastoma. Radiat Oncol 2021; 16 (1): 36. doi: 10.1186/s13014-021 - 01767-9.
43. Buzea CG, Mirestean C, Butuc I et al. Radiation-induced biological changes of neural structures in the base of the skull tumours. J Radiother Prac 2017; 16 (2): 183–198. doi: 10.1017/S1460396916000601.
44. Fleischmann DF, Jenn J, Corradini S et al. Bevacizumab reduces toxicity of reirradiation in recurrent high-grade glioma. Radiother Oncol 2019; 138 : 99–105. doi: 10.1016/j.radonc.2019.06.009.
45. Popp I, Weber A, Graf E et al. Re-irradiation in recurrent glioblastoma: PET - or MRI-based? Results of a prospective randomized clinical trial. J Clin Oncol 2024; 42 : 2021–2021. doi: 10.1200/JCO.2024.42.16_suppl.2021.
46. Grosu A, Weber A, Graf E et al. GLIAA: FET-PET - vs. MRI-based re-irradiation in recurrent glioblastoma. A prospective randomized trial. J Nucl Med 2024; 65 (suppl 2): 242119.
47. Andratschke N, Heusel A, Albert NL et al. ESTRO/EANO recommendation on reirradiation of glioblastoma. Radiother Oncol 2025; 204 : 110696. doi: 10.1016/j.radonc.2024.110696.
48. Preusser M, Kazda T, Le Rhun E et al. Lomustine with or without reirradiation for first progression of glioblastoma, LEGATO, EORTC-2227-BTG: study protocol for a randomized phase III study. Trials 2024; 25 (1): 366. doi: 10.1186/s13063-024-08213-7.
Labels
Paediatric neurology Neurosurgery NeurologyArticle was published in
Czech and Slovak Neurology and Neurosurgery

Most read in this issue
- Recommended standard of discharge report for stroke patients
- Paraneoplastic neurologic syndromes and autoimmune encephalitis – 10-year monocentric observational study
- Efficacy and safety of emergent microsurgery in acute ischaemic stroke patients after intravenous thrombolysis and mechanical thrombectomy failures – a systematic review
- An artistic portrayal of frontotemporal dementia – “děd Vševěd”: a character from the stage play “Dlouhý, Široký a Krátkozraký” by the theatrical company Divadlo Járy Cimrmana