
Pedicled pectoralis major flap in head and neck reconstruction - our experience
Authors:
Z. Dvořák 1,2,3; R. Pink 1,4; P. Michl 1,4; P. Heinz 1,4; P. Tvrdý 1,4
Authors‘ workplace:
Department of Oral and Maxillofacial Surgery, University Hospital Olomouc, Czech Republic
1; Department of Plastic and Aesthetic Surgery, St. Anne`s University Hospital, Brno, Czech Republic
2; Faculty of Medicine, Masaryk University, Brno, Czech Republic
3; Faculty of Medicine, Palacky University, Olomouc, Czech Republic
4
Published in:
ACTA CHIRURGIAE PLASTICAE, 60, 1, 2018, pp. 30-34
INTRODUCTION
The pedicled pectoralis major flap (PPM) is usually considered as a second choice flap after free flaps and the reasons for their primary use varies. The most common indications for primary use of PPM are associated comorbities, extended radical neck dissection, neck vessel depletion for microvascular anastomosis and previous various malignancies (1–5). Another preferred choice is the use of PPM in combination with a free flap (6–8). Other indications for use of PPM are a salvage reconstruction following complications (8), a salvage reconstruction following free flap failure (9) and a salvage reconstruction in prevailing or recurrent primary disease (10). The PPM used for our cases includes all these indications.
MATERIALS AND METHODS
This was a retrospective study of 18 patients operated at the Department of Oral and Maxillofacial Surgery between 1st January 2014 and 1st December 2016. 18 patients underwent reconstruction using 18 PPM flaps. All procedures were performed by two surgeons in one stage reconstruction. Patient demographic data, indications for the procedure, site and extent of primary tumor, defect itself, clinical stage of malignant disease, postoperative complications and management of these postoperative complications related to the flap were recorded and analysed.
Complications were divided into major and minor complications according to the Chepeha classification (11). Flap failures that required surgical intervention were classified as major complications. Failures, which did not require surgical intervention and were resolved conservatively by regular bandaging, incisions, excochleations, drainages, changes of compression and antibiotic therapy, were classified as minor complications. These included: partial flap necrosis, salivary gland fistula, partial flap dehiscence, wound infection, plate exposure, hematoma, seroma and other similar complications at the donor sites.
The pathological stage of the disease was based on preoperative evaluation of USG, CT and MRI results, according to current TMN classification.
Elevation of the flap was done using complete dissection of clavicular portion of pectoralis muscle from the flap and with denervation of the muscle. Photo documentation of patients (before, during and after the procedure) was taken.
RESULTS
All patients were males, average age 58.5 years (minimum 29 years, maximum 71 years and median 60.5 years). In terms of tumor type, all patients suffered from spinocellular carcinoma. In the case of patient no. 2, it was combined with chronic lymphacytic leukemia (Table 1). In terms of disease stage, there were 6 patients in stage II, 3 in stage III and 6 patients in stage IV of cancer. 15 reconstructions of oropharyngeal defects and 1 reconstruction of submandibular defect of the neck were performed using PPM. Indications for the procedure were:
- 10 cases of primary resection of polymorbid patient (all these patients were long-term smokers with a history of alcohol abuse and hepatic dysfunction).
- 5 cases in which the indication was disease recurrence after previous neck dissection and radiotherapy.
- 3 cases of secondary reconstruction due to osteonecrosis or absence of the mandible in irradiated area
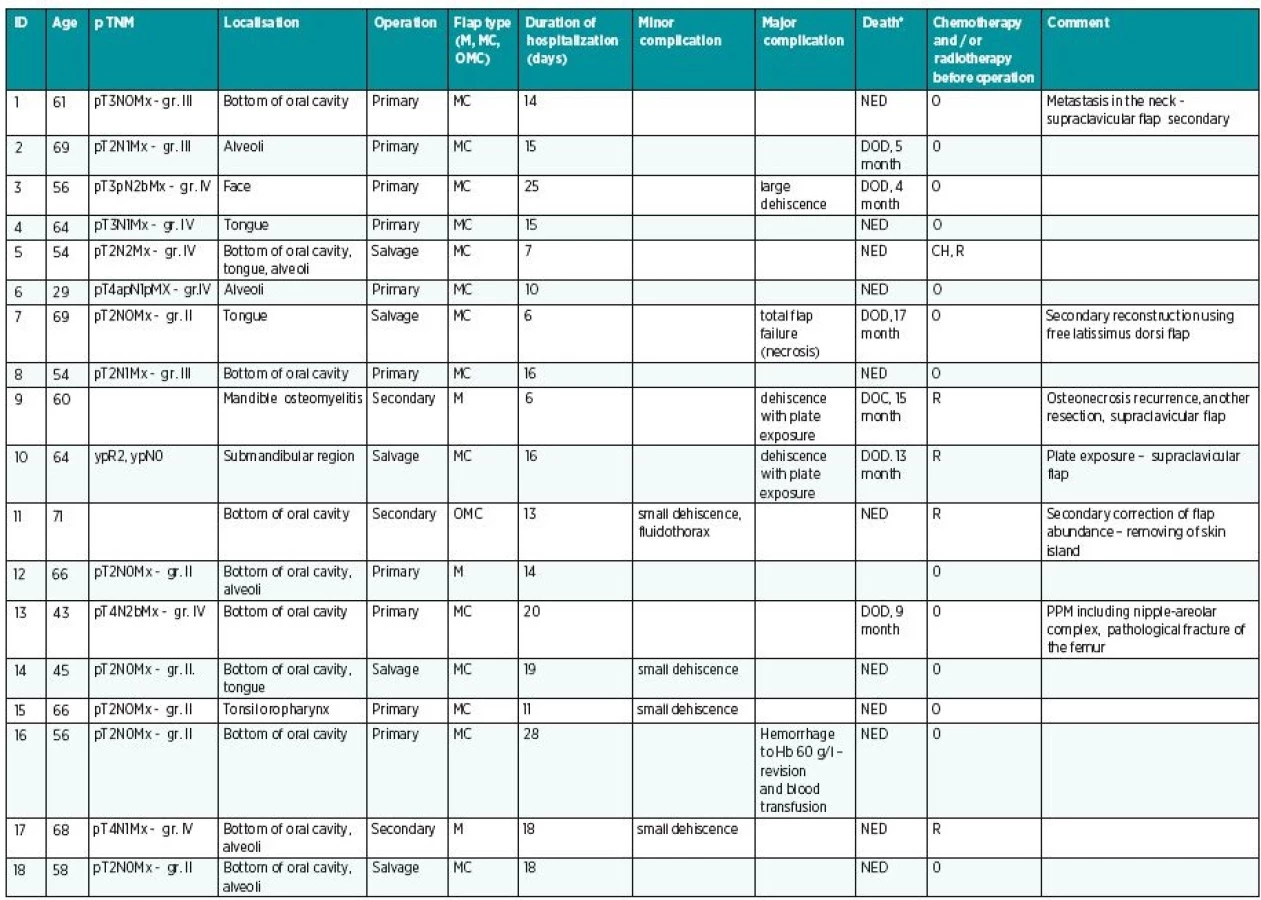
* Legend to „Death“ values NED (no evidence of disease), DOD (died of disease), DOC (died of other of causes)
Denervated PPM in all cases, 14 PPM with skin island, 3 PPM without skin island and 1 PPM with skin island and rib bone (osteomyocutaneous flap).
Surgeries were used for the reconstruction of the floor of the oral cavity, oropharynx, lateral side of the neck and in one case was PPM used for the treatment of osteomyelitis after complete radionecrosis of the mandible (see Table 1).
Complications occurred in 9 out of 18 patients (50.0 %). There were 5 major (27.8 %) and 4 minor complications (22.2 %).
Major complications included:
- 1 case of total flap failure (necrosis) due to technical error (5.5 %). This submandibular defect was successfully treated afterwards using the LDM flap transfer - free tissue transfer of latissimus dorsi myocutaneous flap).
- 2 cases of large dehiscence with plate exposure. These two cases were treated by secondary surgery with plate coverage using an ipsilateral supraclavicular flap (11.1 %).
- 1 case of large dehiscence was treated with secondary surgery (5.5 %).
- 1 case of large hemorrhage mainly to donor area in the thorax, accompanied by blood loss of about 600 ml with drop of hemoglobin level to 60 g/l. This case was a polymorbid patient with systemic morbidities and impaired coagulation cascade due to previous toxonutritive hepatopathy. During the successful surgical revision was diffuse bleeding stopped with QuikClot® devices impregnated with kaolin that were removed the next day after compensation of the blood loss.
Minor complications were only small dehiscences. These occurred in 4 cases (22,2 %), one of them was associated with fluidothorax after the rib harvesting (5,5 %). Repeated needle aspiration of pleural effusion was used to resolve this complication.
No case of muscle abundance on the neck or supraclavicular bulge was observed; the overall morbidity of donor site was very low and no orocutaneous fistula occurred.
The median duration of hospitalization was 15 days (minimum 6 days, maximum 28 days).
The rate of complications on the sample of 5 patients, who underwent radiotherapy before the surgery, was 80 %. There were 2 cases of small dehiscences and 2 cases of large dehiscence that required secondary surgical intervention as a transposition of a supraclavicular flap.
Postoperative folow up was 5 to 36 months. There were 6 deaths observed during the postoperative period (38%), none of them related to the surgery. Five were caused by recurrence and overall progression of the cancer and one pacient died due to heart failure.
In one case, metastasis was found after a period from the surgery, which was resolved by excision and coverage of the defect using a supraclavicular flap.
DISCUSSION
The overall incidence of complications in our small sample of patients was 50%, which can be considered as the mid-range of values referred from other groups of patients - Wilson et al. 16% (12), Milenovic et al. 33% (13), Liu et al. 35% (6), Vartanian 36.1% (14), Pinto et al 43.1% (15), Ijsselstein et al. 53% (16), Rudes et al. 59.3% (17), Kroll et al. 63% (18), and Shah et al. 63% (19). Total flap necrosis occurred in 6% of cases although the literature reports a flap failure from 2% to 3% (13,18,19). This fact may be due to the small sample. The microvascular free tissue transfer (free flap reconstruction) was used as a salvage operation as Tang et al. 2012 (20).
The rate of minor and major complications contrasts with the literature (5,6,9,13,19,21,22) but like Vanni Salles Ribeiro et al., (23) and Pinto et al. (15) probably due to the small sample size. Previous radiotherapy increased the incidence of postoperative complications as observed in other studies (24,25) and also deterioration in perception of quality of life (26).
All patients were males. The supraclavicular flap is the preferred option for women patients due to a higher risk of skin paddlefailure and subsequent deformity of the breast (27). The mean duration of hospitalisation time was 14.7 as in other authors (4,21,28). During the elevation of the flap, we did not use surgical sparing of the field of elevation of deltopectoral flap. However, this can be used after harvesting of pedicled pectoral major flap (13,17,29). We used the supraclavicular flap instead, to achieve a better aesthetic result for the contours of the soft tissues on the head and neck (30–32).
Our team has always performed nerve transection (13) and we have never observed development of bulges or contracting folds in place of the vascular pedicle as it is often reported in the literature. Another factor that is fundamentally involved in any supraclavicular bulge is strict disconnection of the transferred muscle flap and rotation around the clavicle only on the vascular bundle (33,34). There was no neck deformity in our patients probably owing to the above.
In our sample, we did not use the dominance of the lateral thoracic artery. Kanno et al. reported (35) that preservation of the lateral thoracic artery and use of the subclavian route are alternatives to ensure sufficient blood supply and an increased rotation arc of PPM. In our sample, we did not use the subclavian route.
There was no complaint of ipsilateral shoulder movement restriction or reduced functional capability. PPM flap reconstruction has a small but significant negative effect on upper extremity dysfunction and also neck ROM limitations (36–38). In general, we can say that patients who undergo primary reconstruction using PPM, often have significantly reduced working capacity, mainly due to preoperative polymorbidity.
Due to poor quality of rib bone, we refrain from mandible reconstruction using osteomyocutaneous PPM flap (39). Another aspect that needs to be considered is the necessity of donor site closure using mesh, need for chest tube drainage due to distortion of pleural cavity and long term patient recovery (40). Given these facts, we refrain from bone reconstruction and rarely use a reconstructive plate in the case of severely polymorbid patients (3). If possible, we prefer the reconstruction using fibular free flap even for “borderline” indicated patients whenever the condition of blood vessels that supply lower limb permits (2).
CONCLUSION
Even today, usage the PPM in head and neck reconstruction surgery cannot be considered as a historical reconstructive procedure that has been completely replaced by a free microvascular flap. Innovations of flap harvesting techniques and high rate of flap survival are the main reasons why PPM can still be primarily indicated for high-risk patients, non-cooperative patients and also for patients with extensive neck dissection. A combination of PPM and free flap can be advantageous for reconstruction of large complex defects. PPM has been the first choice in salvage surgery, in cases of a complication or free flap failure or a recurrence of a primary disease. In these cases, PPM morbidity remains comparable to morbidity in patients undergoing reconstruction using a free flap.
Acknowledgements: This research received no funding from public agencies, commercial, or not-for-profit sectors.
Conflict of interest statement: The authors state that there are no conflicts of interest regarding the publication of this article.
Corresponding author:
Richard Pink M.D., Ph.D.
Department of Oral and Maxillofacial Surgery, University Hospital
I. P. Pavlova 6, 779 00, Olomouc, Czech Republic
E-mail: richard.pink@seznam.cz
Sources
1. Kroll SS, Evans GR, Goldberg D, et al. A comparison of resource costs for head and neck reconstruction with free and pectoralis major flaps. Plast Reconstr Surg. 1997 Apr;99(5):1282–6.
2. Talesnik A, Markowitz B, Calcaterra T, Ahn C, Shaw W. Cost and outcome of osteocutaneous free-tissue transfer versus pedicled soft-tissue reconstruction for composite mandibular defects. Plast Reconstr Surg. 1996 May;97(6):1167-78.
3. Singh B, Cordeiro PG, Santamaria E, Shaha AR, Pfister DG, Shah JP. Factors associated with complications in microvascular reconstruction of head and neck defects. Plast Reconstr Surg. 1999 Feb;103(2):403-11.
4. Schusterman MA, Horndeski G. Analysis of the morbidity associated with immediate microvascular reconstruction in head and neck cancer patients. Head Neck. 1991 Jan-Feb;13(1):51-5.
5. O’Neill JP, Shine N, Eadie PA, Beausang E, Timon C. Free tissue transfer versus pedicled flap reconstruction of head and neck malignancy defects. Ir J Med Sci. 2010 Sep;179(3):337–43.
6. Liu R, Gullane P, Brown D, Irish J. Pectoralis major myocutaneous pedicled flap in head and neck reconstruction: retrospective review of indications and results in 244 consecutive cases at the Toronto General Hospital. J Otolaryngol. 2001 Feb;30(1):34-40.
7. Mehta S, Sarkar S, Kavarana N, Bhathena H, Mehta A. Complications of the pectoralis major myocutaneous flap in the oral cavity: a prospective evaluation of 220 cases. Plast Reconstr Surg. 1996 Jul;98(1):31–7.
8. Schneider DS, Wu V, Wax MK. Indications for pedicled pectoralis major flap in a free tissue transfer practice. Head Neck. 2012 Aug;34(8):1106-10.
9. Avery CM, Gandhi N, Peel D, Neal CP. Indications and outcomes for 100 patients managed with a pectoralis major flap within a UK maxillofacial unit. Int J Oral Maxillofac Surg. 2014 May;43(5):546-54.
10. Liu HL, Chan JY, Wei WI. The changing role of pectoralis major flap in head and neck reconstruction. Eur Arch Otorhinolaryngol. 2010 Nov;267(11):1759-63.
11. Chepeha DB, Annich G, Pynnonen MA, et al. Pectoralis major myocutaneous flap vs revascularized free tissue transfer: complications, gastrostomy tube dependence, and hospitalization. Arch Otolaryngol Head Neck Surg. 2004 Feb;130(2):181-6.
12. Wilson JS, Yiacoumettis AM, O’Neill T. Some observations on 112 pectoralis major myocutaneous flaps. Am J Surg. 1984 Feb;147(2):273–9.
13. Milenović A, Virag M, Uglesić V, Aljinović-Ratković N. The pectoralis major flap in head and neck reconstruction: first 500 patients. J Craniomaxillofac Surg. 2006 Sep;34(6):340-3.
14. Vartanian JG, Carvalho AL, Carvalho SM, Mizobe L, Magrin J, Kowalski LP. Pectoralis major and other myofascial/myocutaneous flaps in head and neck cancer reconstruction: experience with 437 cases at a single institution. Head Neck. 2004 Dec;26(12):1018-23.
15. Pinto FR, Malena CR, Vanni CM, Capelli Fde A, Matos LL, Kanda JL. Pectoralis major myocutaneous flaps for head and neck reconstruction: factors influencing occurrences of complications and the final outcome. Sao Paulo Med J. 2010 Dec;128(6):336-41.
16. IJsselstein CB, Hovius SE, ten Have BL, Wijthoff SJ, Sonneveld GJ, Meeuwis CA, et al. Is the pectoralis myocutaneous flap in intraoral and oropharyngeal reconstruction outdated? Am J Surg. 1996 Sep;172(3):259–62.
17. Rudes M, Bilić M, Jurlina M, Prgomet D. Pectoralis major myocutaneous flap in the reconstructive surgery of the head and neck--our experience. Coll Antropol. 2012 Nov;36 Suppl 2 : 137-42.
18. Kroll SS, Goepfert H, Jones M, Guillamondegui O, Schusterman M. Analysis of complications in 168 pectoralis major myocutaneous flaps used for head and neck reconstruction. Ann Plast Surg. 1990 Aug;25(2):93–7.
19. Shah JP, Haribhakti V, Loree TR, Sutaria P. Complications of the pectoralis major myocutaneous flap in head and neck reconstruction. Am J Surg. 1990 Oct;160(4):352–5.
20. Tang CL, Wu YC, Lai CH, et al. Salvage for pectoralis major myocutaneous flap failure in head and neck reconstruction by microvascular flap. J Plast Surg Hand Surg. 2012 Oct;46(5):335–8.
21. Kekatpure VD, Trivedi NP, Manjula BV, Mathan Mohan A, Shetkar G, Kuriakose MA. Pectoralis major flap for head and neck reconstruction in era of free flaps. Int J Oral Maxillofac Surg. 2012 Apr;41(4):453-7.
22. McLean JN, Carlson GW, Losken A. The pectoralis major myocutaneous flap revisited: a reliable technique for head and neck reconstruction. Ann Plast Surg. 2010 May;64(5):570–3.
23.Ribeiro Salles Vanni CM, de Matos LL, Faro Junior MP, et al. Enhanced morbidity of pectoralis major myocutaneous flap used for salvage after previously failed oncological treatment and unsuccessful reconstructive head and neck surgery. ScientificWorld Journal. 2012;2012 : 384179.
24. Tabah RJ, Flynn MB, Acland RD, Banis JC. Microvascular free tissue transfer in head and neck and esophageal surgery. Am J Surg. 1984 Oct;148(4):498–504.
25. Zhang C, Sun J, Zhu H, et al. Microsurgical free flap reconstructions of the head and neck region: Shanghai experience of 34 years and 4640 flaps. Int J Oral Maxillofac Surg. 2015 Jun;44(6):675-84.
26. Herce-Lopez J, Rollon-Mayordomo A, Lozano-Rosado R, Infante-Cossio P, Salazar-Fernandez CI. Assessment of quality of life of oral cancer survivors compared with Spanish population norms. Int J Oral Maxillofac Surg. 2013 Apr;42(4):446–52.
27. Ou KL, Chen TM, Dai NT, et al. Treatment of breast deformity with free deep inferior epigastric perforator flap secondary to pectoralis major flap harvesting. Formos J Surg. 2014;47(1):32-35.
28. Tsue TT, Desyatnikova SS, Deleyiannis FW, et al. Comparison of cost and function in reconstruction of the posterior oral cavity and oropharynx. Free vs pedicled soft tissue transfer. Arch Otolaryngol Head Neck Surg. 1997 Jul;123(7):731-7.
29. Nayak BB, Nilamani M. Single stage reconstructions in head and neck surgery using deltopectoral and pectoralis major myocutaneous flaps. Indian J Plast Surg. 2012 Jan;45(1):151-3.
30. Granzow JW, Suliman A, Roostaeian J, Perry A, Boyd JB. Supraclavicular artery island flap (SCAIF) vs free fasciocutaneous flaps for head and neck reconstruction. Otolaryngol Head Neck Surg. 2013 Jun;148(6):941-8.
31. Pallua N, Wolter TP. Moving forwards: the anterior supraclavicular artery perforator (a-SAP) flap: a new pedicled or free perforator flap based on the anterior supraclavicular vessels. J Plast Reconstr Aesthet Surg. 2013 Apr;66(4):489-96.
32. Pallua N, Machens HG, Rennekampff O, Becker M, Berger A. The fasciocutaneous supraclavicular artery island flap for releasing postburn mentosternal contractures. Plast Reconstr Surg. 1997 Jun;99(7):1878-84; discussion 1885-6.
33. Ariyan S. Further experiences with the pectoralis major myocutaneous flap for the immediate repair of defects from excisions of head and neck cancers. Plast Reconstr Surg. 1979 Nov;64(5):605-12.
34. Temiz G, Şirinoğlu H, Yeşiloğlu N, et al. A salvage maneuver for the caudal part of the pectoralis major muscle in the reconstruction of superior thoracic wall defects: The pectoralis kite flap. J Plast Reconstr Aesthet Surg. 2015 May;68(5):698-704.
35. Kanno T, Nariai Y, Tatsumi H, Karino M, Yoshino A, Sekine J. A modified pectoralis major myocutaneous flap technique with improved vascular supply and an extended rotation arc for oral defects: A case report. Oncol Lett. 2015 Nov;10(5):2739–42.
36. Sun Q, Guo S, Wang D, Xu N, Jin SF, Wang CC. Does pectoralis major flap harvesting induce upper extremity dysfunction? J Int Med Res. 2015 Aug;43(4):555-9.
37. Moukarbel RV, Fung K, Franklin JH, et al. Neck and shoulder disability following reconstruction with the pectoralis major pedicled flap. Laryngoscope. 2010 Jun;120(6):1129-34.
38. Refos JW, Witte BI, de Goede CJ, de Bree R. Shoulder morbidity after pectoralis major flap reconstruction. Head Neck. 2016 Aug;38(8):1221-8.
39. Shunyu NB, Medhi J, Laskar HA, Lyngdoh N, Syiemlieh J, Goyal A. 5th Rib Osteo-pectoralis Major Myocutaneous Flap-Still a Viable Option for Mandibular Defect Reconstruction. Indian J Otolaryngol Head Neck Surg. 2014 Dec;66(4):414-7.
40. Ord RA. The pectoralis major myocutaneous flap in oral and maxillofacial reconstruction: a retrospective analysis of 50 cases. J Oral Maxillofac Surg. 1996 Nov;54(11):1292-5; discussion 1295-6.
Labels
Plastic surgery Orthopaedics Burns medicine TraumatologyArticle was published in
Acta chirurgiae plasticae

2018 Issue 1
Most read in this issue
- Pedicled pectoralis major flap in head and neck reconstruction - technique and overview
- Use of licap and ltap flaps for breast reconstruction
- Editorial
- Intraosseous haemangioma od the zygoma - case report and literature review