
POSTOPERATIVE FIXATION AFTER REPOSITIONING OF PREMAXILLA IN A PATIENT WITH BILATERAL CLEFT LIP AND PALATE – CASE REPORT
Authors:
M. Koťová 2; M. Dušková 1; E. Leamerová 1; Wanda Urbanová 2; K. Schwarzmannová 1; K. Novotná 1; A. Sukop 1
Authors‘ workplace:
Department of Plastic Surgery and
1; Department of Stomatology, University Hospital Královské Vinohrady and 3rd Faculty of Medicine, Charles University – Centre for treatment of facial clefts, University Hospital Královské Vinohrady, Prague, Czech Republic
2
Published in:
ACTA CHIRURGIAE PLASTICAE, 59, 3-4, 2017, pp. 157-162
SUMMARY
Bilateral cleft lip and palate is often associated with unfavourable position of the premaxilla, which deteriorates further with growth of the patient. Correction of this type of cleft belongs among the most difficult. It requires basic surgical reconstructions that concern adjustment of the shape and relations of dental arches and arrangement of teeth. Premaxilla in a patient with bilateral cleft lip and palate is shifted to the front and caudally, it is fixed only to the vomer in unstable position with various extent of movements1. Location of premaxilla is attributed also to the functional and morphological insufficiency of orbicularis oris muscle2. The patient has, apart from a serious aesthetic handicap of the centrofacial area, also difficulties during the mouth closure, chewing and speech, which results in various psychosocial problems.
REPOSITIONING OF PREMAXILLA
Correction of the position of premaxilla is based on its shift cranially and backwards, in adjustment of the slope of the alveolar process, and possibly in rotation of the whole segment. The procedure is, according to the anatomical situation, either surgical or orthodontic-surgical. Correction of the position of premaxilla is possible in various developmental phases of the stomatognathic system.
In some patients with total bilateral cleft a severe deviation of premaxilla is obvious right after the birth (Fig. 1A) and primary surgical reconstruction of the lip and nose is very demanding. Therefore in the past there were also resections of the whole protruding intermaxillary segment3 or early surgical impaction of premaxilla4 performed.

In 1983, Vargervik demonstrated an unfavourable effect of early surgical procedures in the area of the premaxilla on further growth of the upper jaw5. Mainly due to his research, the age limit for surgical repositioning of the frontal segment of the maxilla was moved to higher age categories (6 years and more) and it was started to be combined with reconstruction of the alveolar process with cancellous bone at the site of the cleft defect. This operation was indicated in the phase of mixed dentition6.
Possible presurgical orthodontic (orthopaedic) repositioning of premaxilla within a moulding procedure in newborns can be problematic in bilateral cleft lip and palate patients. Such intervention is advantageous and effective in indicated cases, when it is necessary to reduce the distance of each segment of the cleft maxilla and thereby significantly reduce the tension in the area of soft tissues in primary lip reconstruction. However, the effect of moulding on the shape and further growth of maxilla was not demonstrated7, 8, 9.
As a suitable option of therapy seems the combination of surgical repositioning of premaxilla and simultaneous reconstruction of the cleft defect in alveolar process with cancellous bone between the eighth and eleventh year of age. Supplementation of bone ensures stability of the new position of repositioned premaxilla2, 10. Essential for successful healing of premaxilla in the desired position is its rigid stabilisation. Fixation of repositioned frontal segment of maxilla may be performed by a surgeon with skeletal fixation using microscrews and a surgical plate to the vomer or to the lateral maxillary segments11. The risk of this procedure is a negative impact to the growth centre of maxilla and possibility to impair teeth germs. Another option to ensure stable healing of premaxilla is usage of a Sauer splint, rigid resin bite plates and/or fixed orthodontic appliance. Until complete healing of repositioned premaxilla, it is also recommended to exclude all occlusal interferences, e.g. with bites on molar occlusion surfaces, or individual resin removable plate on the lower dental arch12, 13. Reference literature provides case reports of successful orthopaedic repositioning of premaxilla without the use of surgical procedures only with the help of an orthodontic pull14. Surgical repositioning of premaxilla in adult patients with a cleft may be a part of an orthognathic operation.
The following case report demonstrates repositioning of premaxilla in an eight-year-old boy as one of the phases of a complex interdisciplinary treatment of the patient with bilateral cleft lip and palate.
CASE REPORT
A boy with a total bilateral cleft of the maxilla was born as a twin from a 1st risky pregnancy, the second child – sister – is healthy; family history is negative with regards to the patient‘s impairment. Labour with Caesarean section was accomplished without complications, as well as the postpartum adaptation.
The first examination of the boy at Orthodontic department of the Centre for treatment of congenital head and neck disorders, Centre for treatment of facial clefts, University Hospital Královské Vinohrady in Prague took place within the preoperative examination on admission for planned primary reconstruction of the lip at the age of 5 months (see Figure 1A). At this examination, there was already obvious significant protrusion of premaxilla frontally and caudally and transversal collapse of lateral maxillary segments. At the age of 22 months was performed reconstruction of the palate (Fig. 1B). The boy suffered from persisting significant transverse narrowing of the maxilla, insufficient lip closure, sucking in of the lower lip at the age of three years. We therefore attempted to improve the anatomical relations with the application of a palate plate with a transversal expansion screw (Fig. 2 A, B, C) on which the patient got surprisingly well adapted. After four months of appliance usage, the boy learned how to open mouth better; the lip closure improved and the mother reported also improved speech. Transversal expansion of lateral segments demonstrated significant tendency to recurrence, long-term usage of expansion appliance was therefore needed. Exchange of teeth started at the age of seven years with the eruption of permanent molars, eruption of incisives was delayed.

Within interdisciplinary treatment plan was indicated repositioning of premaxilla after eruption of upper permanent incisors. This occurred at the age of eight years of the patient, when a band fixed appliance was applied on the upper dental arch (Fig. 3 A, B). The upper dental model was rebuilt and thick postsurgical wires were prepared in accordance with the required position of premaxilla and an operation plate. Bands as a part of fixed appliance were placed on the permanent central incisors, temporary canines and first permanent molars.
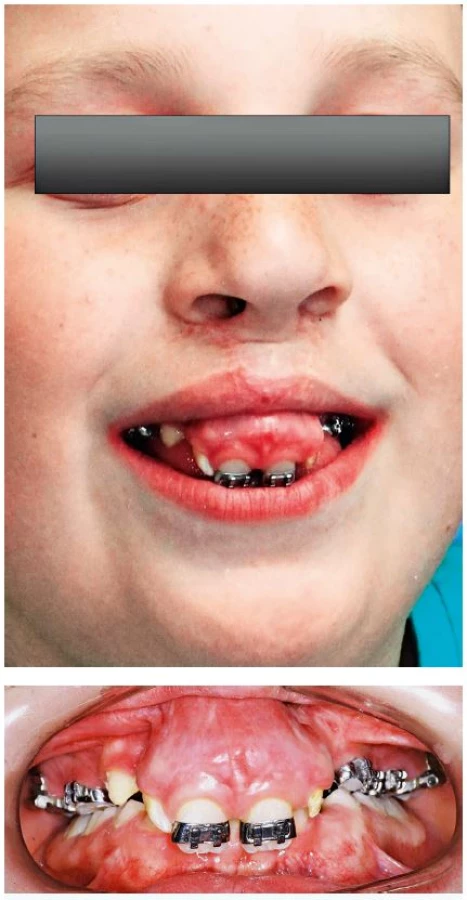
During the operation was performed osteotomy of the neck of the premaxilla and its shortening by 6 mm as planned, insertion of premaxilla to the optimal horizontal and vertical position. Simultaneously was performed bilateral closure of vestibulo-oronasal communication together with bilateral reconstruction of the alveolar process with cancellous grafts from the crest of the ilium bone in a total volume of 6 cc. There were also dysplastic afunctional upper lateral incisors removed from premaxilla. External fixation of maxillary segments was performed with fixed band orthodontic appliance with two intraoral arches (Fig. 4). The whole operated area was subsequently covered with semielastic surgical splint with plastic dressing. Postoperative course and subsequent healing was accomplished without any complications. The option to keep the fixed appliance for the whole mixed dentition period was not accepted by the patient and the appliance was removed after an agreement with the parents after six months and the patient still uses removable appliance (Fig. 5 A, B). Currently continues very slow second phase of teeth exchange; occlusion plane of the maxilla is satisfactory; bite significantly raised and the next phase of therapy with a fixed appliance again is planned after the eruption of upper permanent canines.


Comparison of the result of cephalometric analyses of lateral skull views six months after the operation demonstrated increased SNA angle (Point Sella-Point Nasion-Point A) due to the movement of point A due to cranial shift of a large premaxilla and increased ANB (Point A-Point Nasion-Point B) angle, which we attributed at the age of eight years mainly to the adaptation of the mandible to the new occlusion relations (Fig. 6 A, B; Table 1). The slope of upper central incisors with regards to the skull base and interincisival angle corrected.


DISCUSSION
In the aforementioned patient, it was already obvious in the first years of life that it will be necessary to adjust the position of the deviated premaxilla. Its caudal and ventral position caused that the patient was not able to close the mouth and while smiling and talking, there was gingiva and mucosa of the alveolar process of the frontal segment of maxilla visible. Orthopaedic impaction of premaxilla using orthodontic appliances in the early phases of development was not successful, therefore surgical revision was indicated.
It is obvious from the available literature that it is optimal to associate surgical repositioning of premaxilla with reconstruction of cleft defects of alveolar process of maxilla between the eighth and eleventh year of life of the patient2. Timing of repositioning of maxilla was, with regards to the choice of postoperative fixation, in our case dependent also on the condition of dentition in the upper arch.
Healing of bone graft depends on the condition of bony walls of the cleft defect and patency of fistula closure. Bone connection of maxillary segments provides fixation of premaxilla in an optimal position. If there was no surgical repositioning of premaxilla achieved during reconstruction of alveolar process with bone grafts, the result would be fixation of unfavourable position of frontal segment of maxilla.
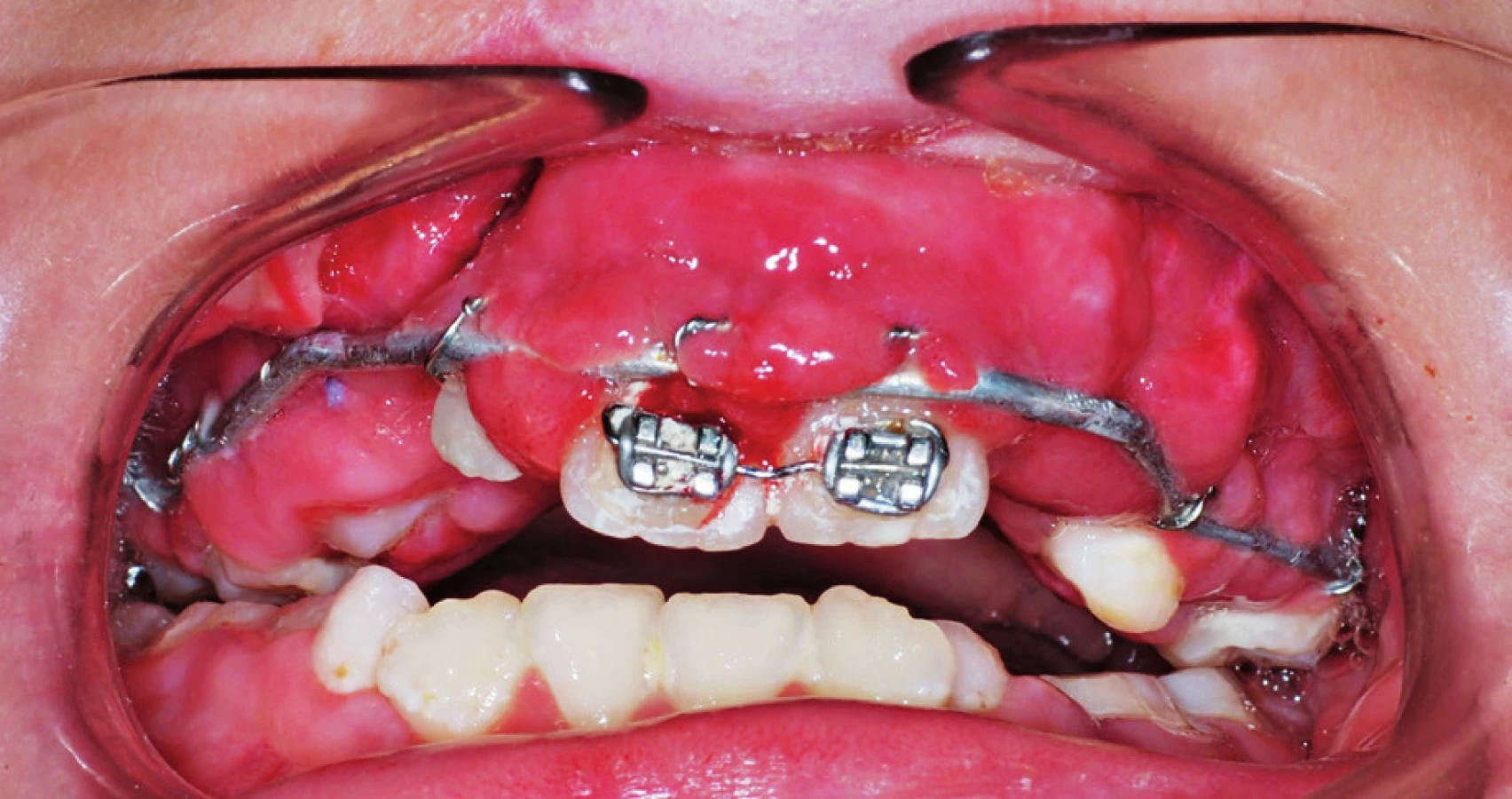
The condition of good healing is rigid fixation of premaxilla in a new position. In the Centre for treatment of congenital head and neck disorders at the University Hospital Královské Vinohrady in Prague, Czech Republic was previously, during these operations, standardly used immobilisation of maxillary segments with Sauer splints and screws. Fixation of wires in the area of the teeth necks however results in irritation and swelling of gingiva (Fig. 7). Problematic is also adequate oral hygiene of the whole splint in the postoperative period. Inflammation could subsequently impair the conditions for satisfactory healing. Therefore, it is not possible to keep this type of fixation in the mouth of the patient for a long time and within interdisciplinary consultations was searched for a solution to fix premaxilla for the whole period of healing. This may be ensured in patients with adequate teeth with a fixed appliance and supplementary rigid vestibular wire (see Fig. 4), which is fixed to supplementary slots of orthodontic bands on first permanent molars and frontally to the block of central upper incisors. The advantage of a fixed appliance is its additional possibility of orthodontic use to restore the shape of the upper teeth arch and to manage overbite of upper incisives.
CONCLUSION
Repositioning of premaxilla at the time of teeth exchange significantly improves anatomical relationships of the dental arches and thereby enables better results of orthodontic therapy; it also contributes to create a more favourable relationship of the lips and to improve lip closure. Important is also a significant change of the aesthetics of centrofacial area, which significantly affects the socialisation of an adolescent patient. In the aforementioned case was only a fixed appliance used for postoperative fixation; osteosynthesis of repositioned premaxilla was not needed. The prerequisite to use this method is the condition of teeth that enables placement of a fixed appliance. Usage of dental fixation in permanent as well as solid temporary teeth is not causing any interference to bone healing; it does not influence the germs of developing permanent teeth. Furthermore, the aforementioned method of fixation for the patient is much more convenient and gentle than Sauer splint.
Corresponding author:
Magdalena Koťová, M.D., PhD.
Department of Stomatology
University Hospital Královské Vinohrady
Šrobárova 50, 100 34 Prague 10, Czech Republic
E-mail: magdalenakotova@seznam.cz
Sources
1. Fára M, Hrivnáková J. The problem of protruding premaxilla in bilateral total clefts. Acta Chir Plast. 1965;7(4):281-96.
2. Bitterman G, Ruiter A, Janssen N, Bittermenn A, van de Molen A, van Es R, Rosenberg A, Koole R. Management of the premaxilla in the treatment of bilateral cleft of the lip and palate: what can literature tell us? Clin Oral Invest. 2016; 20 : 207-217.
3. Cosman B. Premaxillary excision: reasons and effects. Plast Reconstr Surg. 1984 Feb;73(2):195-206.
4. Bishara SE, Olin WH. Surgical repositioning of the premaxilla in complete bilateral cleft lip and palate. Angle Orthod. 1972 Apr;42(2):139-47.
5. Vargervik K. Growth characteristics of the premaxilla and orthodontic treatment principles in bilateral cleft lip and palate. Cleft Palate J. 1983 Oct;20(4):289-302.
6. Lino M, Sasaki T, Kochi S, Fukuda M, Takahashi T, Yamaguchi T. Surgical repositioning of the premaxilla in combination with two-stage alveolar bone grafting in bilateral cleft lip and palate. Cleft Palate Craniofac J. 1998 Jul;35(4):304-9.
7. Urbanová W, Koťová M. Ortodontická léčba před primární rekonstrukcí rtu u pacientů s rozštěpem. Ortodoncie. 2008, 17(1):26-35.
8. Li W, Liao L, Dai J, Zhong Y, Ren L, Liu Y. Effective retropulsion and centralization of the severely malpositioned premaxilla in patients with bilateral cleft lip and palate: a novel modified presurgical nasoalveolar molding device with retraction screw. J Craniomaxillofac Surg. 2014 Dec;42(8):1903-8.
9. Mahmood R, Flood T, Robinson S, Al-Gholmy M. Early Orthopedic Retraction of the Premaxilla in Bilateral Complete Cleft Lip and Palate: An Innovative Approach to a Difficult Problem. Cleft Palate Craniofac J. 2016 May;53(3):363-7.
10. Akita S, Hirano A. Usefulness of simultaneous pre-maxillary osteotomy and bone grafting in the bilateral clefts. J Craniofac Surg. 2006 Mar;17(2):291-6.
11. Carlini JL, Biron C, Gomes KU, Da Silva RM. Surgical repositioning of the premaxilla with bone graft in 50 bilateral cleft lip and palate patients. J Oral Maxillofac Surg. 2009 Apr;67(4):760-6.
12. Behnia H, Mesgarzadeh A, Tehranchi A, Morad G, Samieerad S, Younessian F. Stabilization of premaxilla repositioned during secondary bone grafting in complete bilateral cleft lip and palate patients. J Craniofac Surg. 2014 Jul;25(4):1554-7.
13. Oyama T, Yoshimura Y, Onoda M, Hosokawa K, Kanomi R. Stabilization of a mobile premaxilla by cementing a bite splint with 1-stage bilateral alveolar bone grafting. J Craniofac Surg. 2008 Nov;19(6):1705-7.
14. Kecik D, Enacar A. Repositioning of premaxilla in bilateral cleft lip and palate using a “J-hook headgear”. J Craniofac Surg. 2006 Nov;17(6):1198-207.
Labels
Plastic surgery Orthopaedics Burns medicine TraumatologyArticle was published in
Acta chirurgiae plasticae

2017 Issue 3-4
Most read in this issue
- THE NASOLABIAL FLAP: THE MOST VERSATILE METHOD IN FACIAL RECONSTRUCTION
- CURRENT TREATMENT OPTIONS OF DUPUYTREN´S DISEASE
- PATIENT SATISFACTION AFTER BREAST RECONSTRUCTION: IMPLANTS VS. AUTOLOGOUS TISSUES
- OLEOGEL-S10 TO ACCELERATE HEALING OF DONOR SITES: MONOCENTRIC RESULTS OF PHASE III CLINICAL TRIAL