
Target molecules of the new generation: how molecules could change the approach to treatment of gastrointestinal stromal tumours
Authors:
S. Naizabekova 1; S. Dyikanbaeva 2; F. Djumabaeva 2; N. Dogdurbaeva 1; V. Sloeva 1
Authors‘ workplace:
Department of Chemotherapy, National Center for Oncology and Hematology, Bishkek, Kyrgyzstan
1; Department of Oncology, I. K. Akhunbaev Kyrgyz State Medical Academy, Bishkek, Kyrgyzstan
2
Published in:
Gastroent Hepatol 2026; 80(3): 239-249
Category:
Gastrointestinal Oncology: Original Article
doi:
https://doi.org/10.48095/ccgh2026239
Overview
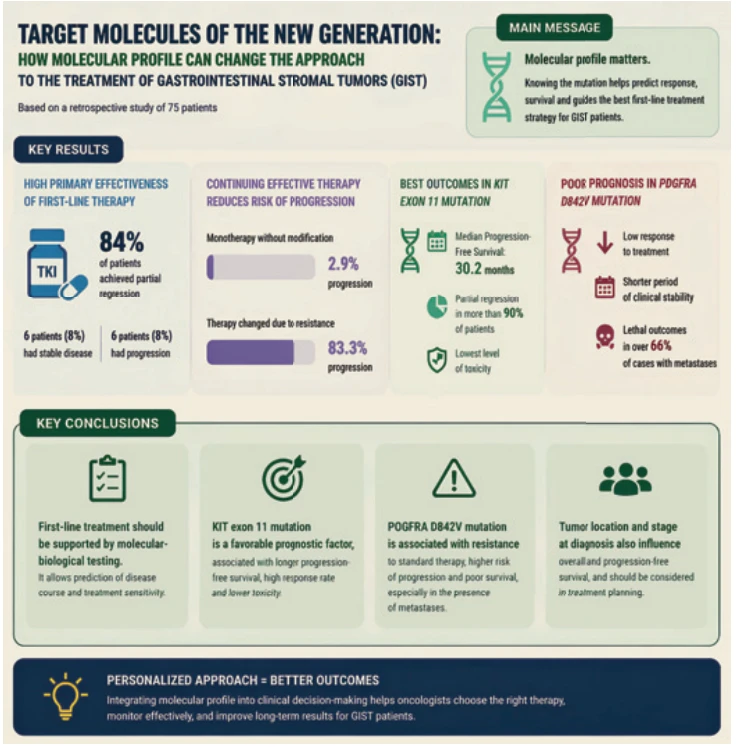
The aim of the work was to determine dependence between the molecular profile of the tumour, clinical parameters of the treatment course, and long-term treatment outcomes. The study was conducted by a retrospective analysis of data from 75 patients with a morphologically confirmed diagnosis, using comparative, frequency, and stratified statistical methods. It was revealed that 84% of patients achieved partial regression, stabilisation of the disease was recorded in 6 individuals, and the frequency of progression amounted to 8%, which allowed the identification of high primary effectiveness of the chosen drug in the first line of treatment. In the group that maintained monotherapy without modification of the protocol, disease progression was observed only in 2.9% of cases, whereas in patients whose treatment was changed due to resistance, the frequency of progression reached 83.3%. The best survival and disease control results were observed in patients with a mutation in exon 11 of the KIT gene, with median progression-free survival of 30.2 months, frequency of partial regression of over 90%, and the lowest level of toxicity. In the subgroup with mutation D842V of the PDGFRA gene, progressive course prevailed, low response to treatment was observed, shortened period of clinical stability, and lethal outcomes in over 66% of cases in the presence of metastases. Results of the stratified analysis also confirmed the influence of tumour localisation and stage at the time of diagnosis on overall and progression-free survival. The application of study results allowed substantiation of the expediency of molecular-biological support within the first line of treatment and prediction of the course of the disease. The obtained data could be used by oncologists, molecular pathomorphologists, and clinical pharmacologists in the formation of individual treatment schemes and in decision-making regarding modification of therapy on the basis of predicted sensitivity.
Keywords:
gastrointestinal stromal tumours – tyrosine kinase inhibitors – targeted cancer therapy – imatinib
Introduction
Gastrointestinal stromal tumours belong to the most common mesenchymal neoplasms of the gastrointestinal tract, at the same time being characterised by significant biological heterogeneity, which complicates the choice of therapeutic strategy. Despite the fact that the introduction of tyrosine kinase inhibitors (TKI) allowed significant improvement in survival rates, some patients exhibited primary or acquired resistance to standard treatment schemes. The presence of a clinically relevant relationship between mutational status and sensitivity to therapy determined the need to implement a personalised approach to treatment, based on molecular-biological stratification.
The problem also involved the absence of standardised models for predicting therapy outcomes, considering the combined influence of clinico-anatomical and molecular factors. Differences in treatment responses under the same TKI scheme and the presence of specific mutation variants resistant to imatinib created risks of inefficient resource use and reduced chances for long-term remission. The issue of timely identification of signs of disease progression also became relevant, which required not only clinical monitoring, but also dynamic assessment of the molecular profile. In this context, the study of the relationship between genetic characteristics, therapy response, and long--term outcomes allowed the expansion of tools of personalised oncological practice contributing to the optimisation of therapeutic decisions.
The publication of Zhong et al. [1] contained a systematised review of the results of clinical application of small-molecule inhibitors in targeted cancer therapy, with emphasis on low selectivity, development of secondary resistance, and limited control over progression. The key conclusion was the recognition of the need to increase the specificity of drug-target interaction against the background of high tumour heterogeneity. In the work of Nakamura et al. [2], multilevel analysis of biomarkers for gastric cancer and gastro-oesophageal junction cancer was carried out; it was established that the effectiveness of targeted therapy directly depended on the expression level of HER2, the presence of microsatellite instability, and programmed death-ligand 1 (PD-L1), which substantiated the introduction of molecular stratification for the choice of treatment tactics. Additionally, the authors emphasised the limitations of classical biopsies and the prospects of using circulating tumour DNA for dynamic monitoring of the therapy response.
In the study of Klug et al. [3], generalisation of the effectiveness of the newest tyrosine kinase inhibitors in the treatment of advanced forms of a gastrointestinal stromal tumour (GIST) was presented, with the finding that mutations in exon 11 of the KIT gene were associated with the highest level of clinical response; whereas the PDGFRA D842V variant had an unfavourable prognosis. Matsuoka and Yashiro [4] focused on the problems of implementing personalised therapy in gastrointestinal oncology, emphasising the dependence of treatment effectiveness on the availability of validated molecular markers.
According to the results of Bai et al. [5], the use of molecular-functional imaging allowed non-invasive determination of tumour biological activity and effectiveness of targeted intervention at the early stages of treatment.
Min and Lee [6] summarised data on molecular drugs of a wide spectrum of action, focusing on the need to form a toxicity profile before treatment prescription to optimise safety and therapy effectiveness. At the same time, the results of El Fil et al. [7] demonstrated the growing role of immunotherapy in the treatment of gastrointestinal tumours, with the combination of TKI and immunomodulators providing higher clinical response in patients with resistant forms.
In the work of Muto et al. [8], regional clinical experience of treating gastrointestinal tumours in Asia and the Middle East was summarised. In the article of Kaur et al. [9], a historical-functional analysis of cancer treatment methods was conducted, where the conclusion was made that only a comprehensive approach considering the genomic profile could ensure clinically relevant effectiveness in targeted therapy.
Within the analysed sources, the key role of a tumour mutational profile in predicting TKI effectiveness was established, but there were no generalisations regarding the prognostic significance of different genetic variants in combination with clinical parameters (presence of metastases, tumour localisation). Most works focused on general mechanisms of drug action or were limited to certain forms of cancer without considering the specifics of GIST. However, in real practice, an insufficient level of integration of genetic predictors into clinical algorithms was observed, which reduced the effectiveness of therapeutic intervention in patients with an aggressive disease course. Regional differences in access to molecular diagnostics were also insufficiently characterised, which was critical for countries with limited resources, including Uzbekistan. Not enough attention was paid to the analysis of side effects in the context of mutational status, which complicated the formation of personalised therapy schemes.
The aim of the conducted study was identification of the relationship between the biomolecular profile of the tumour, therapy response, and clinical prognosis of patients with gastrointestinal stromal tumours who received tyrosine kinase inhibitors. Within the study, quantitative assessment of therapy effectiveness was carried out considering the mutational status of the tumour, the frequency of side effects, and the impact on treatment tolerability was analysed; typical clinical reactions depending on mutation variants in KIT and PDGFRA genes were determined, as well as stratification profiles formed considering the presence of metastases and genetic characteristics of the tumour with the purpose of predicting survival and disease course.
Materials and methods
Within the conducted study, a retrospective design was applied with the inclusion of patients who received therapy in specialised oncological institutions of Kyrgyzstan between 2009 and 2025. The analysis was based on already established medical registries and patients’ medical records, without interference in the course of treatment, which corresponded to the methodology of retrospective observation. The sample included cases of morphologically confirmed gastrointestinal stromal tumours with verified results of molecular-genetic testing, which allowed the assessment of mutational status. All patients underwent treatment with tyrosine kinase inhibitors according to current clinical protocols, with the duration of observation ranging from 12 to 36 months for each patient, depending on the availability of complete clinico-molecular data. The sample was determined by the presence of a unified system of observation, completeness of clinico-molecular documentation, and the possibility of conducting a stratified analysis in conditions with limited resources. The exclusion criteria were: absence of confirmation of the GIST diagnosis at morphological and immunohistochemical levels; absence of molecular-genetic testing results; incomplete medical documentation; observation period of less than 12 months; and treatment conducted outside the national oncological system. For validation and international comparison, data were used from countries with established oncological surveillance systems, in particular Germany, USA, Japan, and South Korea, allowing a valid assessment of GIST detection frequency, diagnostic staging, and effectiveness of therapeutic strategies in a comparative aspect.
The collection of clinical and molecular data was carried out on the basis of primary documentation of patients who were treated at the National Centre of Oncology and Haematology (NCOH) of Kyrgyzstan between 2021 and 2025. To form the initial dataset, the clinical monitoring database of NCOH, reports from the Department of Molecular Diagnostics of the Scientific Centre for Biomedical Research at I.K. Akhunbaev Kyrgyz State Medical Academy [10], results of KIT and PDGFRA gene sequencing, as well as therapeutic management protocols were used. Data were obtained from annual reports in this centre, which accumulated the results of molecular-genetic studies of patients with GIST conducted within the framework of the university laboratory. Additional sources included international statistical databases and registries, which were used for comparative analysis.
The assessment of therapeutic effectiveness was carried out with the use of frequency methods, in particular the calculation of the proportion of cases of partial response (PR), stable disease (SD), and progressive disease (PD) among 75 analysed patients. The results were evaluated taking into account the localisation of the primary lesion, stage according to the tumour-node--metastasis (TNM) classification (stages I and III), type of therapy, and presence of its correction. The choice of imatinib as the basic first-line drug was determined by its status as the only agent approved by national clinical guidelines for the treatment of GIST in Kyrgyzstan at the time of the study, as well as its effectiveness confirmed by international recommendations for KIT mutations and certain variants of PDGFRA. Comparative statistics between stratified subgroups (by mutational status: KIT, PDGFRA, SDH-negative (succinate dehydrogenase), NF1-associated; and by the presence of metastases) were performed using the c² criterion and the Mann-Whitney U test in the IBM SPSS Statistics software environment (version 26.0) and with additional verification of results in the R package (version 4.3.1). Mean durations of treatment were calculated with consideration of missing values in the database, applying descriptive statistical methods and listwise deletion procedures to avoid distortion of the results.
For the assessment of progression--free survival (PFS) and overall survival (OS), the Kaplan-Meier method [11] was applied. Determination of statistical significance of intergroup differences was carried out with the log-rank test. Determination of observation status (alive, dead, lost to follow-up) was conducted on the basis of clinical monitoring data of NCOH over 36 months. Particular attention was paid to the interpretation of not reached medians of PFS and OS, which were denoted as “> 42 months”.
The stratified analysis envisaged the construction of multidimensional cross--tables, in which clinico-genetic variables – type of mutation (KIT ex11, PDGFRA D842V, other/negative variants), tumour localisation (stomach, small intestines, others), and metastatic status – were combined. On the basis of such combinations, patterns with the highest risk of progression, short PFS, and probability of developing toxic reactions of grade 3-4 according to the Common Terminology Criteria for Adverse Events (CTCAE) [12] were identified. Additionally, the analysis of therapeutic responses was conducted considering the type of prescribed inhibitor and the frequency of transition to the second line of treatment. Within the conducted study, the term “combined therapy” was used to denote the combination of imatinib with other methods of treatment (surgical intervention, radiotherapy) in cases when monotherapy did not provide adequate control of the disease. The principle of prescribing combined therapy was based on clinical indications, in particular the development of secondary resistance or local progression under a systemically controlled process.
Interpretation of results was based on comprehensive alignment of clinical, morphological, and molecular characteristics. Frequencies of PR, SD, and PD within each stratified subgroup were taken into account. Indicators of therapeutic responses were correlated with survival levels (PFS, OS) and frequency of lethal outcomes, allowing the formation of empirical prognostic models for the justification of personalised therapy. All clinical and molecular data were preliminarily anonymised in accordance with the principles of Good Clinical Practice (GCP) [13] and the ethical provisions of the World Medical Association’s Declaration of Helsinki [14].
Results
Clinical and epidemiological characteristics of patients with GIST in Kyrgyzstan
For the purpose of systematising baseline characteristics, demographic and clinical parameters of 75 patients were presented in a generalised graphical model. This format allowed clear visualisation of key variables and served as a basis for further multivariate analyses. Considering the single-centre study design, aggregation of population characteristics increased the reliability of stratified comparisons within therapeutic subgroups.
Graph 1 shows the distribution of patients by age, sex, tumour localisation, presence of metastases, and clinical stage. This graphical overview summarises baseline cohort characteristics and supports interpretation of treatment effectiveness depending on clinical-biological variables.
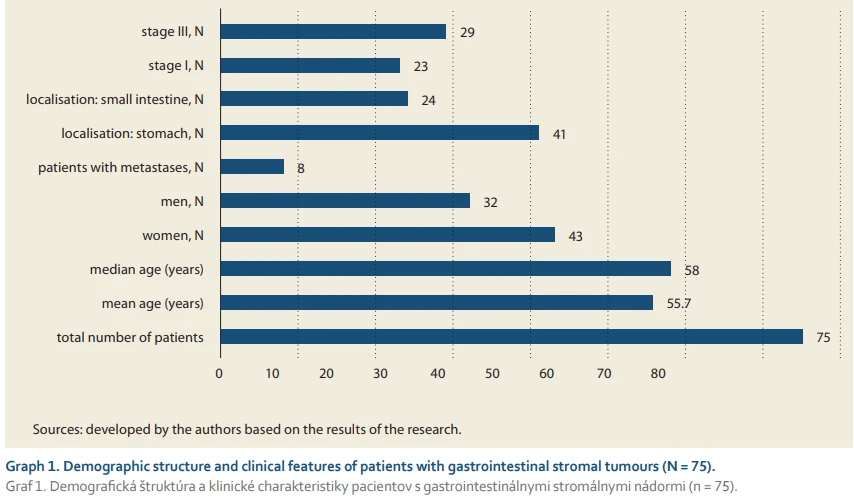
Analysis revealed predominance of women (N = 43) over men (N = 32). The mean age was 55.7 years, median = 58 years, which was consistent with typical GIST presentation. Gastric tumours were most frequent (N = 41), followed by small intestine involvement (N = 24). Distant metastases were present in 8 patients at diagnosis. Stage III predominated (N = 29), while stage I was observed in 23 patients, reflecting variability in clinical debut and the need for flexible therapeutic planning.
Comparison with international registries highlighted peculiarities of GIST detection in Kyrgyzstan. Graph 2 shows GIST incidence per 1 million population and the proportion of early-stage diagnoses (I–II) compared with other countries.
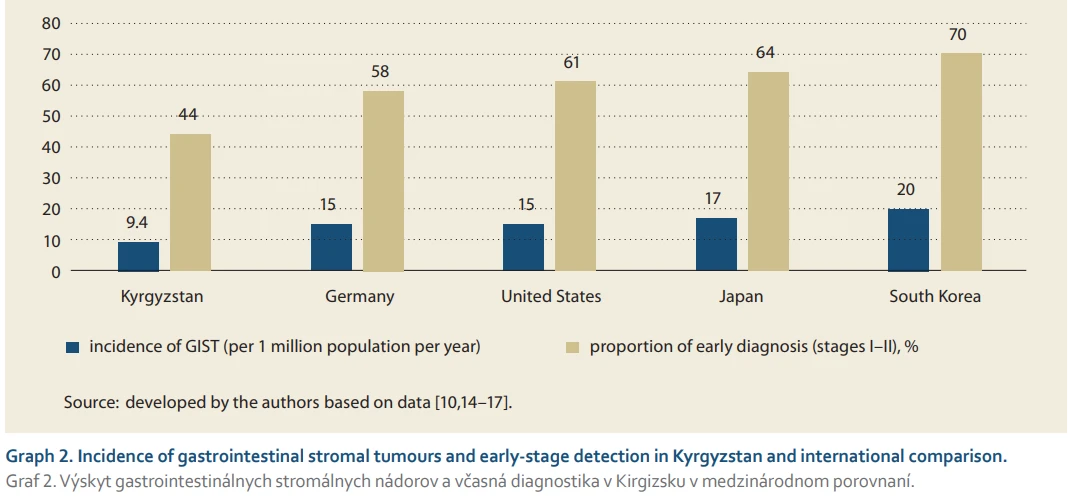
The incidence of GIST in Kyrgyzstan was 9.4 cases per 1 million per year, which was lower than in South Korea (20), Japan (17), USA (15), and Germany (15). Only 44% of patients were diagnosed at stages I–II, lagging behind international benchmarks (South Korea 70%, Japan 64%, USA 61%, Germany 58%). This may reflect limited screening coverage, low awareness of early symptoms, and fragmented use of standard diagnostic protocols. Adapting effective international early-diagnosis models to national conditions is necessary to strengthen clinical outcomes in GIST treatment.
Clinical effectiveness of new generation targeted therapy in patients
All patients (N = 75) received targeted therapy with imatinib, the only available first-line drug for GIST in Kyrgyzstan at the time of observation. Uniformity of treatment was guided by national clinical guidelines and limited access to alternative targeted agents. Within imatinib therapy, differences were noted in therapy duration, dosage individualisation, dose modification, and monitoring frequency.
Graph 3 summarises main treatment parameters, including therapy lines, average duration, dosing regimen (initial or modified), management features, and spectrum of toxic effects. The standard initial dose was 400 mg, modified in about one-third of patients due to adverse reactions or decreased effectiveness. Most common toxicities were peripheral oedema and gastrointestinal symptoms, mainly grade I–II. Prolonged imatinib use without dose modification was associated with better tumour control and lower severe toxicity, whereas patients at high risk of progression required regimen adjustment. These findings highlight the importance of flexible dosing based on clinical-molecular monitoring.
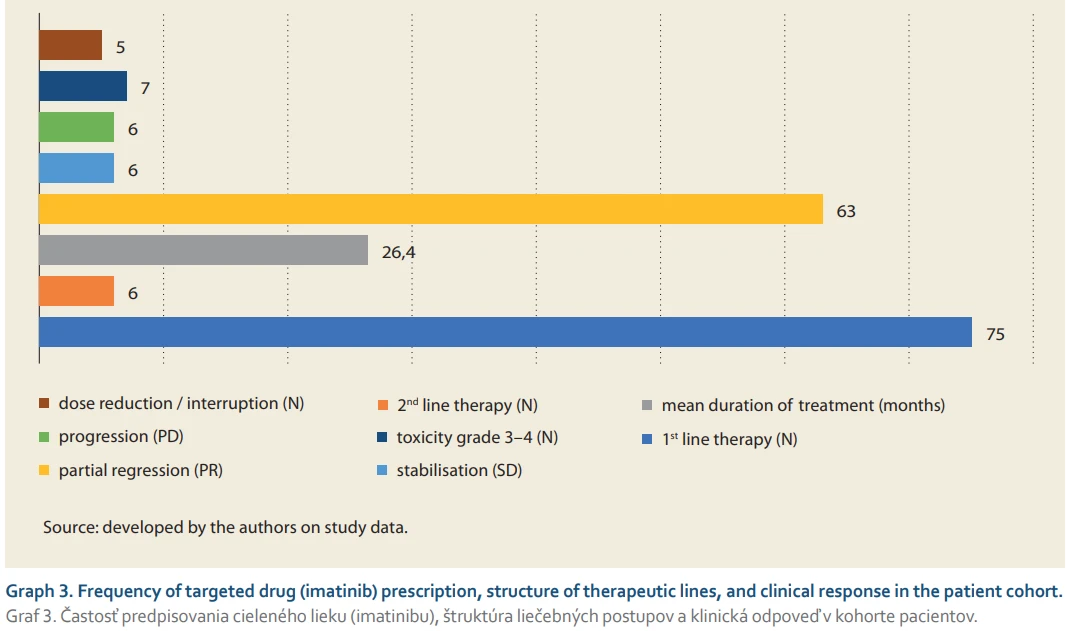
Evaluation according to RECIST criteria showed partial regression (PR) in 63 patients, disease stabilisation (SD) in 6, and progression (PD) in 6. Transfer to second-line therapy was recorded in 6 patients (8%) due to progression, confirming high initial effectiveness of imatinib.
A comparative analysis of progression frequency between monotherapy and modified therapy groups revealed a significant difference. In the monotherapy group (N = 69), progression occurred in 2.9%, while in patients with modified therapy (N = 6), progression reached 83.3% (Tab. 1). This contrast reflected both therapy type and baseline tumour aggressiveness, including primary resistance or unfavourable mutational profiles.
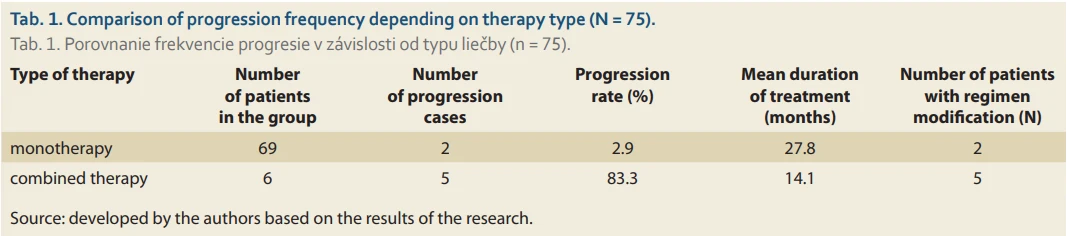
Patients who persisted on imatinib without alterations to the protocol sustained disease control for a minimum of 24 months, thereby validating the enduring treatment efficacy in the context of heightened tumour sensitivity. Advancement in several originally responding patients underscored the threat of acquired resistance, emphasising the necessity for dynamic molecular surveillance and prompt therapy modifications.
The trial validated the clinical efficacy of imatinib as the primary treatment for GIST. Elevated partial regression rates, minimal progression in monotherapy, and extended disease control substantiate imatinib as an appropriate standard treatment. Additional research integrating clinical and molecular-genetic attributes holds promise for individualised treatment methods and optimisation of the following therapeutic regimens.
Molecular-biological support of therapy and biomarkers of sensitivity and resistance
Molecular heterogeneity of GIST necessitates patient stratification based on genetic markers with proven prognostic and predictive significance. The main targets are mutations in KIT and PDGFRA genes, which encode receptor tyrosine kinases and determine TKI sensitivity. Rare cases included SDH-deficient and NF1-associated forms, characterised by atypical courses and poor response to standard therapy. Molecular profiling is thus a mandatory step in personalised treatment planning and therapy prediction.
Analysis of mutation distribution considered exon localisation, mutation type, and GIST morphological variant, linking molecular profile to clinical parameters (Tab. 2).
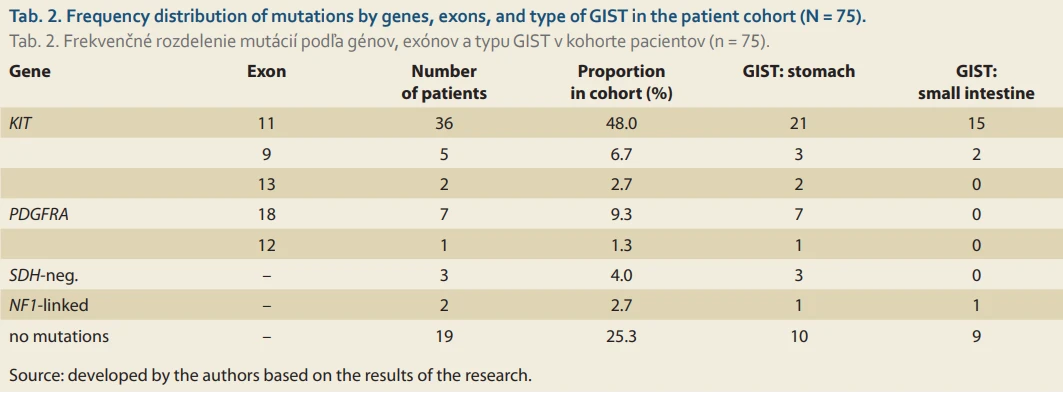
The majority of detected mutations were KIT alterations, predominantly exon 11 (48%), confirming its key role in GIST pathogenesis. PDGFRA D842V mutations were mainly gastric and were associated with variable TKI sensitivity, while rare SDH-deficient and NF1-associated forms required alternative strategies. About 25.3% of patients had no detectable KIT or PDGFRA mutations, highlighting the need for extended sequencing to identify less-studied targets.
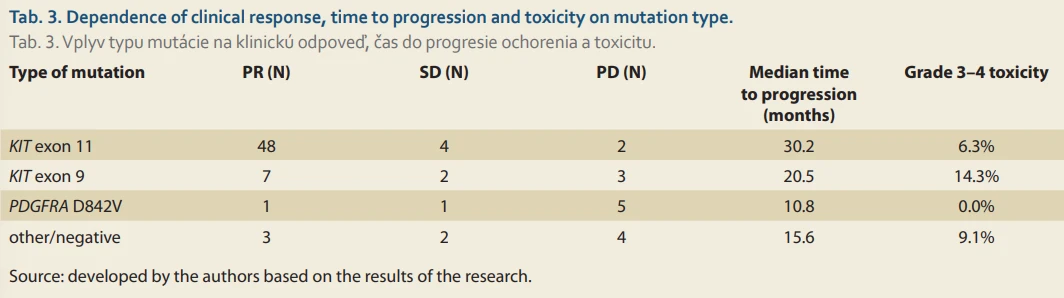
Clinical response strongly correlated with mutation type (Tab. 3). The most favourable profile was in KIT exon 11, with high partial regression, prolonged median progression-free survival (30.2 months), and low severe toxicity. PDGFRA D842V showed predominantly progressive disease and low response, confirming resistance to first-line therapy. KIT exon 9 mutations had intermediate response but highest grade 3–4 toxicity, requiring closer monitoring.
Predictive models combining mutation type, tumour location, and initial stage enabled accurate estimation of clinical effect and timely protocol adjustments, optimising therapeutic strategy and resource use.
The results confirm that molecular-biological support is essential in GIST management, linking genetic profile, disease course, and therapy toxicity, and forming the basis for personalised oncological care adaptable to current protocols and new targeted agents.
Survival and prognosis in the use of targeted drugs in GIST
Long-term effectiveness of GIST therapy was assessed using progression-free survival (PFS) and overall survival (OS). Kaplan-Meier curves [11] accounted for censored observations, and patients were stratified by age, sex, tumour localisation, metastatic status, therapy regimen, and mutation type.
Analysis revealed that mutation type, tumour localisation, and metastatic status at diagnosis were significant prognostic factors, allowing identification of subgroups with differentiated outcomes (Tab. 4).
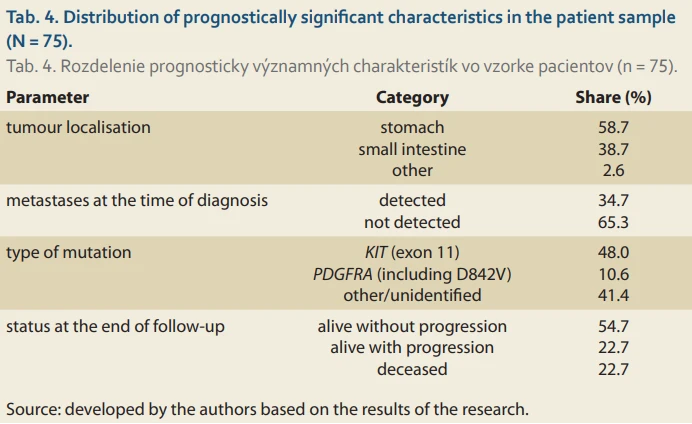
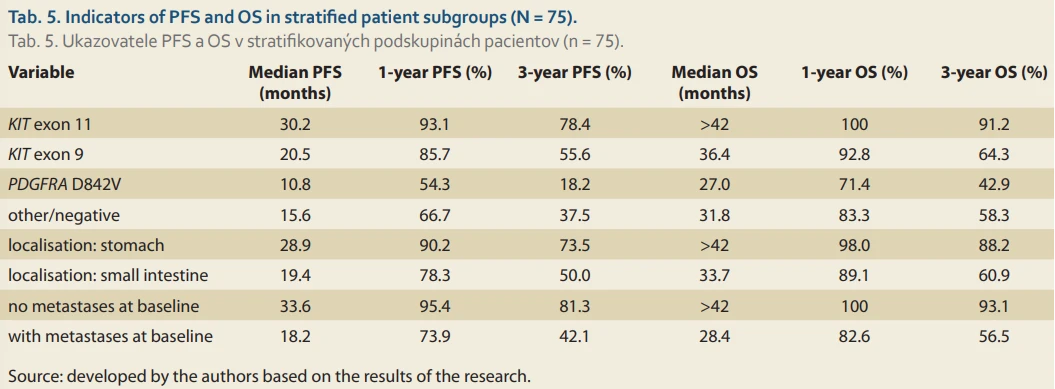
Gastric localisation and KIT exon 11 mutations were linked to the best progression-free survival (PFS) and overall survival (OS), while PDGFRA D842V mutations and metastatic disease were connected with worst outcomes. Fatalities (22.7%) were predominantly observed in subgroups characterised by severe illness and resistant mutations. Stratified analysis yielded median progression-free survival (PFS), overall survival (OS), and one - and three-year survival rates (Tab. 5).
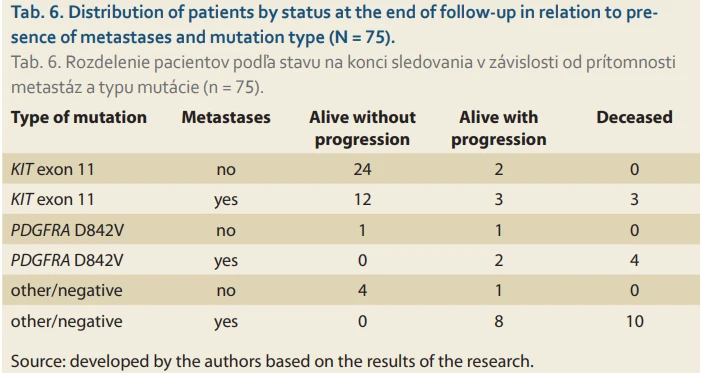
Tab. 6 summarises patient status at follow-up in relation to mutation and metastases. KIT exon 11 without metastases showed the most favourable prognosis, while PDGFRA D842V with metastases had the highest lethality (> 66%).
The data substantiate a robust correlation among tumour molecular profile, disease stage, and survival outcomes. The presence of KIT exon 11, stomach location, and absence of metastases were associated with favourable outcomes, while PDGFRA D842V and the presence of metastases signified a poor prognosis. These findings endorse a tiered therapeutic approach that takes into account both genetic modifications and tumour stage.
Discussion
The analysis showed that the clinical effectiveness of imatinib in GIST depends on the interplay of tumour molecular-genetic characteristics, disease stage, and therapeutic regimen. The highest PFS and OS were observed in patients with KIT exon 11 mutations and no metastases, indicating a long-term stable disease course. Conversely, patients with PDGFRA D842V mutations and advanced disease had unfavourable outcomes, with high progression rates and frequent deaths. Toxicity correlated with mutational status, emphasising the need for stratification via both efficacy and safety. These findings support molecular-biological monitoring during clinical decision-making, particularly where access to new-generation TKIs is limited.
A clear correlation between mutation type and therapy response was found, especially in subgroups with KIT exons 11 and 17 mutations, justifying precise molecular typing prior to treatment [15]. Immunohistochemical and molecular-genetic methods were critical for diagnosis verification, particularly with ambiguous morphological signs. Analysis of PR, SD, and PD according to mutational burden revealed variable responses depending on genetic subtype, consistent with Cicala et al. [16], confirming the need for personalised therapy in rare variants.
Stratified approaches improved prognostic accuracy. Lowest lethality occurred in patients with mutations highly sensitive to imatinib. This aligns with Incorvaia et al. [17], where variant allele frequency of KIT/PDGFRA predicted survival and treatment adherence. Between 2021 and 2024, rare genotypes associated with atypical GIST forms increased, confirming the need for protocol updates [10].
Treatment duration and therapy modifications correlated with initial molecular characteristics. Timely adaptation improved efficacy and reduced progression, which was consistent with Schaefer et al. [18]. Combining morphological and molecular indicators enhanced prediction of disease course and identified high-risk subgroups, as in line with Blay et al. [19].
Mutation profiling was essential for individualised regimens, particularly for rare or negative variants [20]. Morphological parameters – tumour size, localisation, and metastatic status – significantly influenced prognosis, which was consistent with Cannella et al. [21]. Topographic and pathophysiological markers guided personalised therapy, reflecting the findings by Moga et al. [22]. Early evaluation via imaging enabled timely adjustments, improving PFS, as noted by Weeda et al. [23] and Ceausu et al. [24]. Radiological-genetic correlations helped predict molecular status, confirming the results of Palatresi et al. [25].
The study’s therapeutic approaches aligned with GEIS [26] and British Sarcoma Group [27] recommendations, focusing on stratification by genetic and clinical parameters, and reflected morphological-genetic differentiation concepts. Survival analysis confirmed benchmark-level clinical effectiveness, supporting timely therapy correction, particularly for PDGFRA D842V subgroups [28,29]. Surgery combined with TKIs improved prognosis in limited metastases, as shown by Rahimi-Ardabily et al. [30].
PDGFRA D842V as a resistance predictor aligned with von Mehren et al. [31]. Data-driven stratification models enhanced decision-making. Adherence prediction via machine learning [32] and AI-assisted diagnostics complemented molecular profiling [33].
Effectiveness of imatinib was highest in KIT exon 11, confirming the need for pre-treatment mutation assessment and protocol adaptation [34]. Combined clinical and molecular evaluation supports digital twin models and Bayesian network predictions [35]. Imaging and AI facilitated timely therapy adjustment, consistent with clinical-molecular monitoring, and pharmacogenomics-radiomics integration informed comprehensive patient stratification.
In conclusion, the study confirms the necessity of clinical-molecular stratification in GIST, integrating genetic, morphological, and imaging data to personalise therapy. Multidisciplinary and digital approaches provide a solid basis for adapting treatment protocols and improving clinical effectiveness.
Author contributions
SN, SD, FD, ND and VS contributed to conceptualization, methodology, data curation, and writing – original draft preparation.
SN was responsible for visualization, investigation, and supervision.
SD, FD, ND and VS contributed to software, validation, and writing – review & editing.
All authors have read and approved the final manuscript.
Submitted/Doručeno: 15. 1. 2026
Accepted/Přijato: 10. 4. 2026
Corresponding author
Svetlana Naizabekova, MD, PhD
Department of Chemotherapy
National Center for Oncology and Hematology
92 Akhunbaev Str.
720020 Bishkek
Kyrgyzstan
svetlananaizabekova5@gmail.com
Sources
1. Zhong L, Li Y, Xiong L et al. Small molecules in targeted cancer therapy: advances, challenges, and future perspectives. Signal Transduct Target Ther 2021; 6 (1): 201. doi: 10.1038/s41392-021-00572-w.
2. Nakamura Y, Kawazoe A, Lordick F et al. Biomarker-targeted therapies for advanced-stage gastric and gastro-oesophageal junction cancers: an emerging paradigm. Nat Rev Clin Oncol 2021; 18 (8): 473–487. doi: 10.1038/s41571-021-00492-2.
3. Klug LR, Khosroyani HM, Kent JD et al. New treatment strategies for advanced-stage gastrointestinal stromal tumours. Nat Rev Clin Oncol 2022; 19 (5): 328–341. doi: 10.1038/s41571-022-00606-4.
4. Matsuoka T, Yashiro M. Molecular-targeted therapy toward precision medicine for gastrointestinal caner: current progress and challenges. World J Gastrointest Oncol 2021; 13 (5): 366–390. doi: 10.4251/wjgo.v13.i5.366.
5. Bai JW, Qiu SQ, Zhang GJ. Molecular and functional imaging in cancer-targeted therapy: current applications and future directions. Signal Transduct Target Ther 2023; 8 (1): 89. doi: 10.1038/s41392-023-01366-y.
6. Min HY, Lee HY. Molecular targeted therapy for anticancer treatment. Exp Mol Med 2022; 54 (10): 1670–1694. doi: 10.1038/s12276-022-00864-3.
7. El Fil S, Uwishema O, Ahmed AR et al. Immunotherapy in gastrointestinal cancers: current strategies and future directions-a literature review. Ann Med Surg 2025; 87 (1): 151–160. doi: 10.1097/MS9.0000000000002757.
8. Muto M, Sunakawa Y, Sandhir N et al. Real-world genomic landscape of gastrointestinal cancers in Asia and the Middle East using comprehensive circulating tumor DNA next-generation sequencing. Oncol Res Treat 2025; 48 (12): 1–17. doi: 10.1159/000545560.
9. Kaur R, Bhardwaj A, Gupta S. Cancer treatment therapies: traditional to modern approaches to combat cancers. Mol Biol Rep 2023; 50 (11): 9663–9676. doi: 10.1007/s11033-023-08809-3.
10. Brčić I, Argyropoulos A, Liegl-Atzwanger B. Update on molecular genetics of gastrointestinal stromal tumors. Diagnostics 2021; 11 (2): 194. doi: 10.3390/diagnostics11020194.
11. Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc 1958; 53 (282): 457–481. doi: 10.2307/2281868.
12. NCI. Common Terminology Criteria for Adverse Events (CTCAE) v5.0. 2021 [online]. Available from: https: //ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm.
13. ICH Harmonised Guideline. Integrated addendum to ICH E6 (R1): guideline for good clinical practice E6 (R2). 2016 [online]. Available from: https: //database.ich.org/sites/default/files/E6_R2_Addendum.pdf.
14. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA 2013; 310 (20): 2191–2194. doi: 10.1001/jama.2013.281053.
15. Unk M, Jezeršek Novaković B, Novaković S. Molecular mechanisms of gastrointestinal stromal tumors and their impact on systemic therapy decision. Cancers 2023; 15 (5): 1498. doi: 10.3390/cancers15051498.
16. Cicala CM, Olivares-Rivas I, Aguirre-Carrillo JA et al. KIT/PDGFRA inhibitors for the treatment of gastrointestinal stromal tumors: getting to the gist of the problem. Expert Opin Investig Drugs 2024; 33 (3): 159–170. doi: 10.1080/13543784.2024.2318317.
17. Incorvaia L, De Biase D, Nannini M et al. KIT/PDGFRA variant allele frequency as prognostic factor in gastrointestinal stromal tumors (GISTs): results from a multi-institutional cohort study. Oncologist 2024; 29 (1): e141–e151. doi: 10.1093/oncolo/oyad206.
18. Schaefer IM, DeMatteo RP, Serrano C. The GIST of advances in treatment of advanced gastrointestinal stromal tumor. Am Soc Clin Oncol Educ Book 2022; 42 : 1–15. doi: 10.1200/EDBK_351231.
19. Blay JY, Kang YK, Nishida T et al. Gastrointestinal stromal tumours. Nat Rev Dis Primers 2021; 7 (1): 22. doi: 10.1038/s41572-021-00254-5.
20. Calderillo-Ruíz G, Pérez-Yepez EA, García-Gámez MA et al. Genomic profiling in GIST: implications in clinical outcome and future challenges. Neoplasia 2024; 48 : 100959. doi: 10.1016/j.neo.2023.100959.
21. Cannella R, Tabone E, Porrello G et al. Assessment of morphological CT imaging features for the prediction of risk stratification, mutations, and prognosis of gastrointestinal stromal tumors. Eur Radiol 2021; 31 (11): 8554–8564. doi: 10.1007/s00330-021-07961-3.
22. Moga DFC, Vlădoiu G, Frățilă AM et al. Understanding gastric GIST: from pathophysiology to personalized treatment. J Clin Med 2024; 13 (14): 3997. doi: 10.3390/jcm13143997.
23. Weeda YA, Kalisvaart GM, van Velden FH et al. Early prediction and monitoring of treatment response in gastrointestinal stromal tumors by means of imaging: a systematic review. Diagnostics 2022; 12 (11): 2722. doi: 10.3390/diagnostics12112722.
24. Ceausu M, Socea B, Ciobotaru VP et al. A multidisciplinary approach in the diagnostic challenge of GIST. Exp Ther Med 2021; 22 (4): 1063. doi: 10.3892/etm.2021.10497.
25. Palatresi D, Fedeli F, Danti G et al. Correlation of CT radiomic features for GISTs with pathological classification and molecular subtypes: preliminary and monocentric experience. Radiol Med 2022; 127 (2): 117–128. doi: 10.1007/s11547-021-01446-5.
26. Serrano C, Martín-Broto J, Asencio-Pascual JM et al. 2023 GEIS Guidelines for gastrointestinal stromal tumors. Ther Adv Med Oncol 2023; 15 : 17588359231192388. doi: 10.1177/175883592 31192388.
27. Judson I, Jones RL, Wong NA et al. Gastrointestinal stromal tumour (GIST): British Sarcoma Group clinical practice guidelines. Br J Cancer 2025; 132 (1): 1–10. doi: 10.1038/s41416-024-02672-0.
28. Li J, Huang Z, Zhou H et al. Survival outcomes and prognostic factors of advanced gastrointestinal stromal tumors: in the era of multiple tyrosine kinase inhibitors. J Gastrointest Oncol 2024; 15 (3): 931–945. doi: 10.21037/jgo-24-63.
29. Haller V, Reiff C, Hamacher R et al. Overall survival of patients with KIT-mutant metastatic GIST in the era of multiple kinase inhibitor availability. J Cancer Res Clin Oncol 2024; 150 (11): 489. doi: 10.1007/s00432-024-05965-2.
30. Rahimi-Ardabily A, Murdande S, Dong M et al. Liver resection for metastatic GIST tumor improves survival in the era of tyrosine kinase inhibitors: a systematic review and meta-analysis. Langenbecks Arch Surg 2023; 408 (1): 373. doi: 10.1007/s00423-023-03052-7.
31. von Mehren M, Heinrich MC, Shi H et al. Clinical efficacy comparison of avapritinib with other tyrosine kinase inhibitors in gastrointestinal stromal tumors with PDGFRA D842V mutation: a retrospective analysis of clinical trial and real-world data. BMC Cancer 2021; 21 (1): 291. doi: 10.1186/s12885-021-08013-1.
32. Liu L, Yu Z, Chen H et al. Imatinib adherence prediction using machine learning approach in patients with gastrointestinal stromal tumor. Cancer 2025; 131 (1): e35548. doi: 10.1002/cncr.35548.
33. Stefanou IK, Dovrolis N, Gazouli M et al. miRNAs expression pattern and machine learning models elucidate risk for gastric GIST. Cancer Biomark 2022; 33 (2): 237–247. doi: 10.3233/CBM-210173.
34. Beecroft JR, Brar S, Feng X et al. Pan-Canadian consensus recommendations for GIST management in high-and low-throughput centres across Canada. Ther Adv Med Oncol 2024; 16 : 17588359241266179. doi: 10.1177/17588359 241266179.
35. Renne SL, Cammelli M, Santori I et al. True mitotic count prediction in gastrointestinal stromal tumors: bayesian network model and PROMETheus (Preoperative Mitosis Estimator Tool) application development. J Med Internet Res 2024; 26: e50023. doi: 10.2196/50023.
Labels
Paediatric gastroenterology Gastroenterology and hepatology SurgeryArticle was published in
Gastroenterology and Hepatology

2026 Issue 3
Most read in this issue
- Current options for drug therapy in perianal Crohn’s disease
- Role of home parenteral nutrition in gastroenterology
- Oral sulfate solution as a modern approach to bowel preparation for colonoscopy: evidence and clinical data
- Extracorporeal shock wave lithotripsy in patients with the algic obstructive form of chronic pancreatitis