
Role of clinical, histopathological, and immunohistochemical findings in the diagnosis of gastrointestinal stromal tumors: a single-center experience
Authors:
G. Erkilinc 1; T. Devrim 1; S. S. Tuncer 2; E. Ayhan 2; A. Demirel 1
Authors‘ workplace:
Department of Medical Pathology, Izmir Bakircay University, Çiğli Training and Research Hospital, Izmir, Turkey
1; Department of Medical Pathology, Ministry of Health, Çiğli Training and Research Hospital, Izmir, Turkey
2
Published in:
Gastroent Hepatol 2026; 80(3): 225-233
Category:
Gastrointestinal Oncology: Original Article
doi:
https://doi.org/10.48095/ccgh2026225
Overview
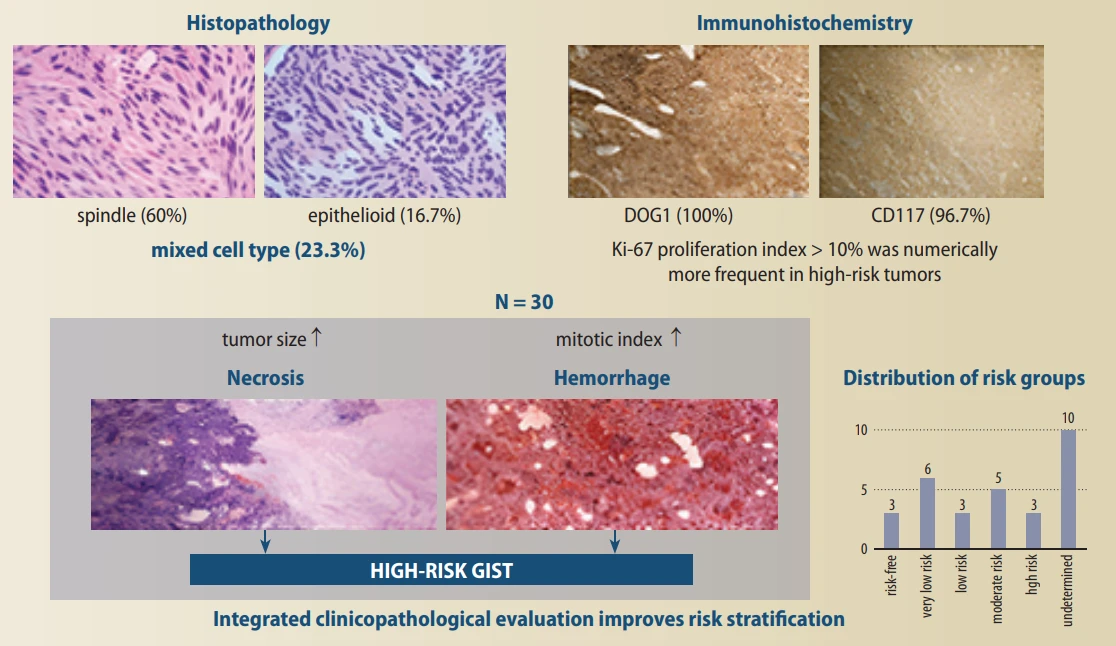
Background: Accurate risk stratification in gastrointestinal stromal tumors (GISTs) is critical for predicting aggressive behavior and guiding clinical management. Although tumor size and mitotic activity are established prognostic parameters, the combined contribution of histopathological features and immunohistochemical markers to risk assessment remains incompletely defined in routine practice. Materials and methods: We retrospectively analyzed 30 GIST cases diagnosed at a single tertiary center between 2012 and 2025. Clinicopathological parameters, including tumor size, location, histological subtype, mitotic index, necrosis, hemorrhage, and ulceration, were systematically re-evaluated. Immunohistochemical expression of CD117, CD34, DOG1, and Ki-67 was assessed, and risk stratification was performed according to AFIP criteria. Results: Tumors were most frequently located in the stomach (66.7%). Larger tumor size and increased mitotic activity were strongly associated with higher risk categories (P = 0.005 and P = 0.049, respectively). Histopathological features reflecting aggressive biological behavior, namely necrosis and hemorrhage, were more frequently observed in high-risk tumors. Immunohistochemically, CD117 (96.7%) and DOG1 (100%) demonstrated consistently high diagnostic sensitivity. While immunostaining patterns did not correlate with risk category, a Ki-67 proliferation index ≥ 10% was numerically more frequent in high-risk tumors; however, this difference did not reach statistical significance (P = 0.503). Conclusion: Beyond tumor size and mitotic activity, the presence of necrosis and hemorrhage provides additional histopathological evidence of aggressive behavior in GISTs. Immunohistochemical markers, particularly CD117 and DOG1, ensure diagnostic accuracy, while Ki-67 showed a tendency toward higher expression in high-risk tumors; however, its prognostic relevance requires further investigation. These findings underscore the value of an integrated clinicopathological and immunohistochemical approach to refine risk assessment and optimize patient management in GISTs.
Introduction
Gastrointestinal stromal tumors (GISTs) represent the predominant mesenchymal tumors within the gastrointestinal tract (GI). GISTs have different clinical features, localization, histopathology, and prognosis. They are observed at a rate of 1–2 per 100,000 in the population and constitute 1–2% of all gastrointestinal tumors [1]. GISTs can be localized anywhere along the GI tract, and more than half are observed in the stomach, followed by the small intestines, colon, and esophagus. About 1% of all GISTs are localized in extra-GI tract foci such as subcutaneous tissue, peritoneum, and pancreas, and these cases are defined as extra-GIST (EGIST). It has a higher probability of being malignant and constitutes 10% [2,3].
Symptoms of GIST can vary depending on tumor size. They may be detected incidentally during surgery performed for another tumor or asymptomatically during endoscopy when the tumor is small. Contrast-enhanced computed tomography (CT) is often used for follow-up after diagnosis [4].
The factors that determine the risk of recurrence are the tumor’s size, location, and symptoms. As the tumor size increases, the likelihood of symptomatic disease increases. The most common known symptoms are low hemoglobin, obstruction, and compression symptoms [4].
The gold standard for diagnosis is histopathological examination. Histopathologically, in hematoxylin & eosin (H&E) stained sections, it can consist of spindle (70%), epithelioid (20%), and mixed (10%) types of cells. Depending on the tumor’s risk, it may acquire features such as increased mitotic count, necrosis, and atypia. Immunohistochemical staining reveals CD117 and DOG1 expression, which are among the most valuable known markers for confirming the diagnosis in the vast majority of GISTs [5]. Approximately 20–30% are smooth muscle actin (SMA) positive, 10% are S100 protein positive, and less than 5% are desmin positive. CD34 and SMA expression are generally correlated. GISTs and Cajals, have phenotypic similarities with interstitial cells, and therefore, a histogenetic origin from these cells has been suggested. An alternative possibility, the origin of pluripotential stem cells, is also possible; this is supported by the common origin of Cajal cells and smooth muscle along with common SMA expression [6].
Leiomyosarcomas, which are extremely uncommon in the GI tract, and leiomyomas are clinically and pathogenetically different from GISTs. Leiomyomas are found in the GI tract, primarily in the colon, rectum (muscularis mucosa tumors), and esophagus (intramural tumors) [7]. They are also distinct from schwannomas, which are benign S100-positive spindle cell tumors that typically develop in the stomach. GISTs are likely a subset of GI autonomic nerve tumors (GIN). Dedifferentiated liposarcoma, angiosarcomas, desmoid, and myofibroblastic tumors are other types of mesenchymal tumors that must be distinguished from GISTs. Additionally, metastatic tumors, which are usually KIT-positive, should not be confused [8].
Surgery is the gold standard for treatment. Tyrosine kinase inhibitors (KIT) are very useful [9]. The combined use of surgery and KIT treatment has been confirmed to provide effective treatment, and transarterial chemotherapy and tumor ablation with silver nanoparticles can be listed among the new treatment regimens [10,11].
The National Institutes of Health (NIH) published a consensus statement proposing risk stratification criteria for GISTs based on tumor size and mitotic activity [12]. Following this statement, the Armed Forces Institute of Pathology (AFIP) conducted extensive studies on GISTs and developed a modified risk classification scheme incorporating tumor location in addition to tumor size and mitotic rate [13,14].
The aim of this study is to examine GISTs with their clinical, histopathological, and immunohistochemical findings, to distinguish them from lesions included in the differential diagnosis, and to evaluate tumor risk groups.
Patients and methods
Study population, design, and ethical approval
Hematoxylin-eosin and immunohistochemical stained preparations were evaluated, if any, of the materials belonging to 30 patients diagnosed with GIST between January 2012 and December 2025 in our pathology department. This retrospective study was approved by the ethics committee of our institution on 10/09/2025 with decision number: 2431 and research number: 2419.
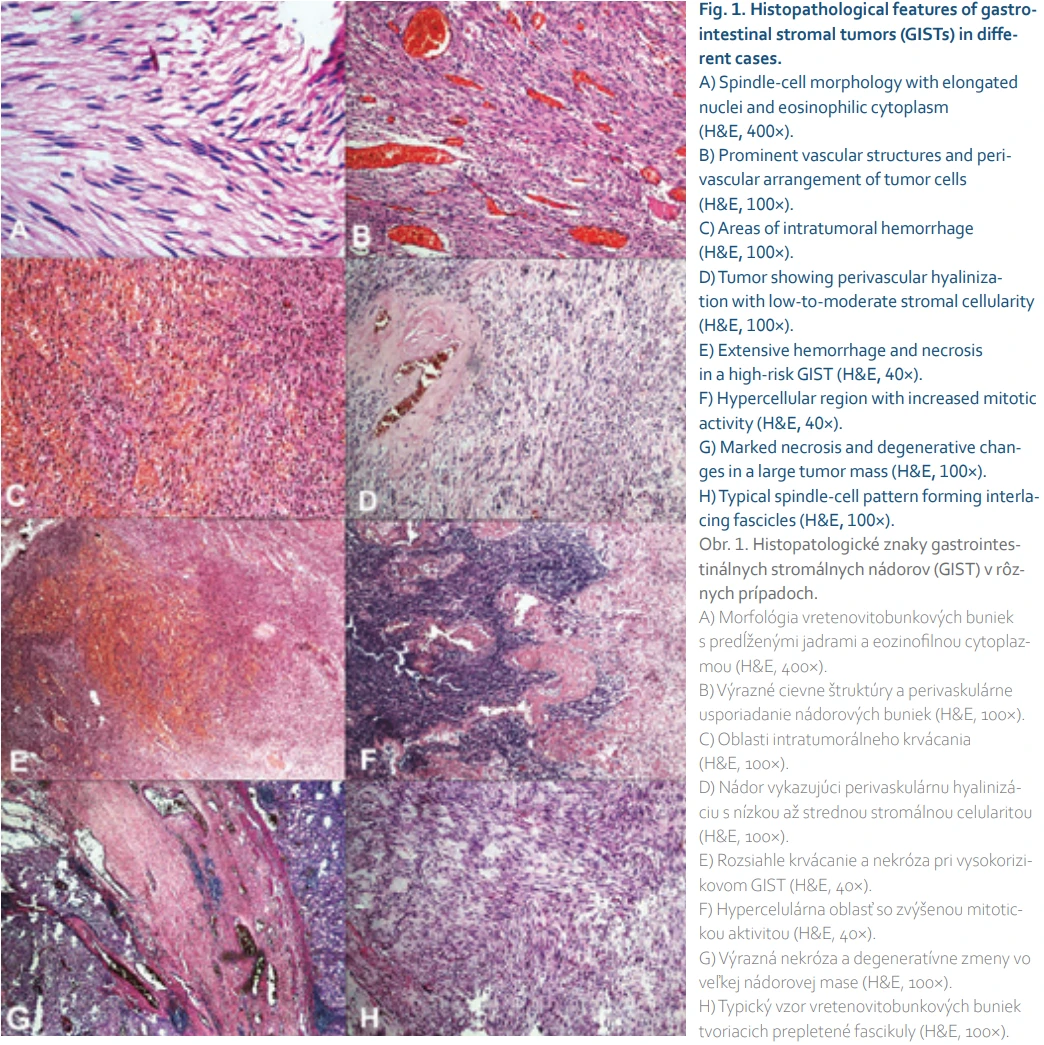
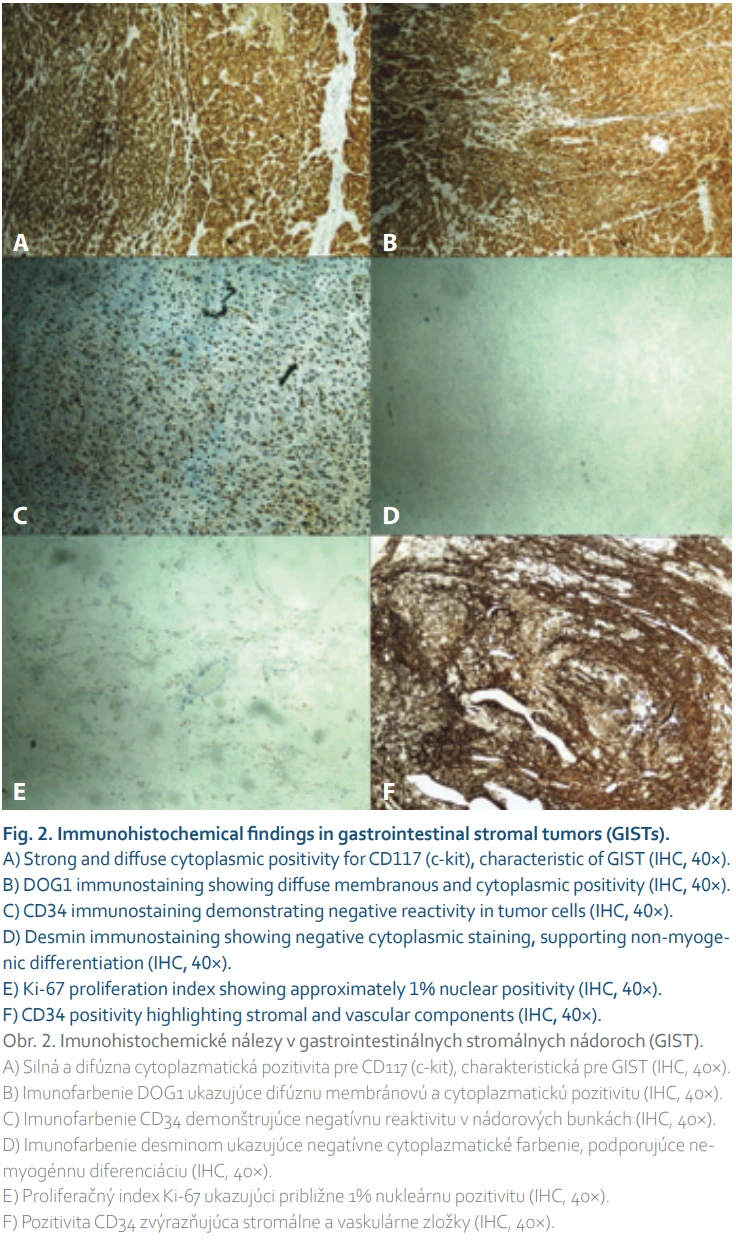
The number of patients included in the study was obtained by scanning patients diagnosed with GIST in the hospital automation system. Age, sex, tumor location, and tumor size were recorded from the patient’s pathology reports. H&E-stained sections and available immunohistochemically stained preparations were retrospectively re-evaluated (Fig. 1, 2).
Localization of the patients’ tumors (gastrointestinal origin, extra-gastrointestinal), tumor size, ulcer (present/absent), bleeding (present/absent), necrosis (present/absent), adjacent organ invasion (present/absent), and lymph node involvement (present/absent) were evaluated. Tumor size (≤ 2 cm; > 2 to ≤ 5 cm; > 5 to ≤ 10 cm; >10 cm) and mitotic activity (≤ 5/5 mm2 and > 5/5 mm2) were classified as very low, low, moderate, and high according to AFIP criteria and tumor location (gastric, small intestines, rectum) [13,14].
The present findings were correlated with recurrence and survival. Furthermore, in cases with available immunohistochemical stains, CD34 and CD117 were scored in three groups based on the extent of staining in tumor cells: < 10%; 10–50%; and > 50%, and staining intensity: mild (+), moderate (++), and severe (+++) [15,16]. Ki-67 antibody was evaluated in the foci with the highest mitotic index, and the percentage of nuclear positivity per 1,000 cells was determined. The agreement between diagnosis and score was compared.
Statistical analysis
Statistical analyses were performed using SPSS version 21.0 (IBM, Chicago, USA). Categorical variables were summarized as frequencies and percentages, and continuous variables as mean ± SD and median values. Normality of distribution was assessed using the Shapiro-Wilk test. Since continuous variables did not meet normal distribution criteria, comparisons between low - and high-risk groups were performed using the Mann-Whitney U test. Categorical variables were compared using the Chi--square or Fisher’s exact test. Correlations between quantitative parameters were evaluated using Spearman’s rank correlation. A P-value < 0.05 was considered statistically significant.
Results
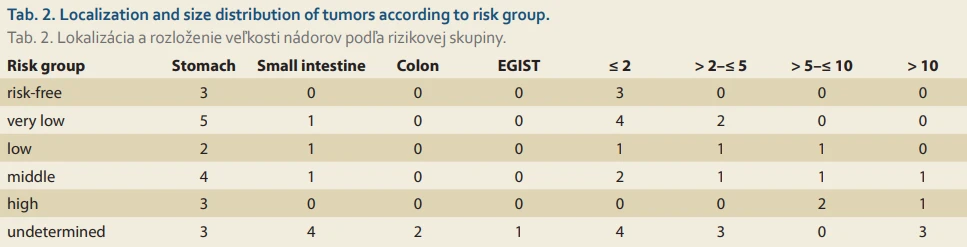
The patients’ ages ranged from 29 to90 years, with a mean age of 66.7±±14.0 years and a median age of 65 years. The most common tumor location was the stomach (66.7%), followed by the small intestines (23.3%), colon (6.7%), and EGIST (3.3%). Tumor sizes ranged from 0.5 to 15 cm, with a mean tumor size of 4.4 ± 4.2 cm (median 3.75 cm) (Tab. 1). No significant correlation was observed between tumor size and tumor localization (P = 0.188) (Tab. 2).
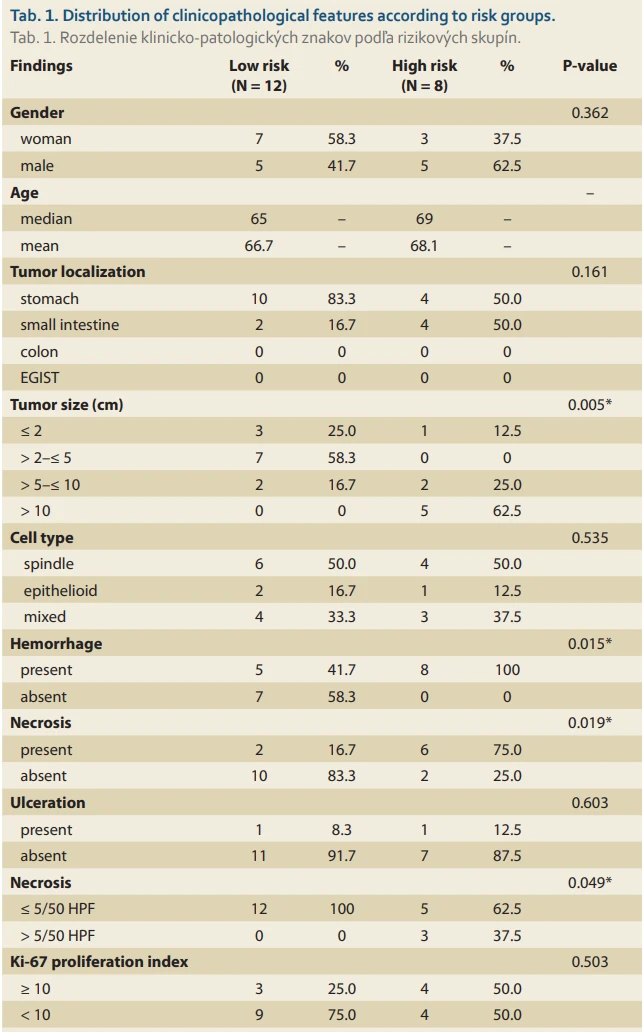
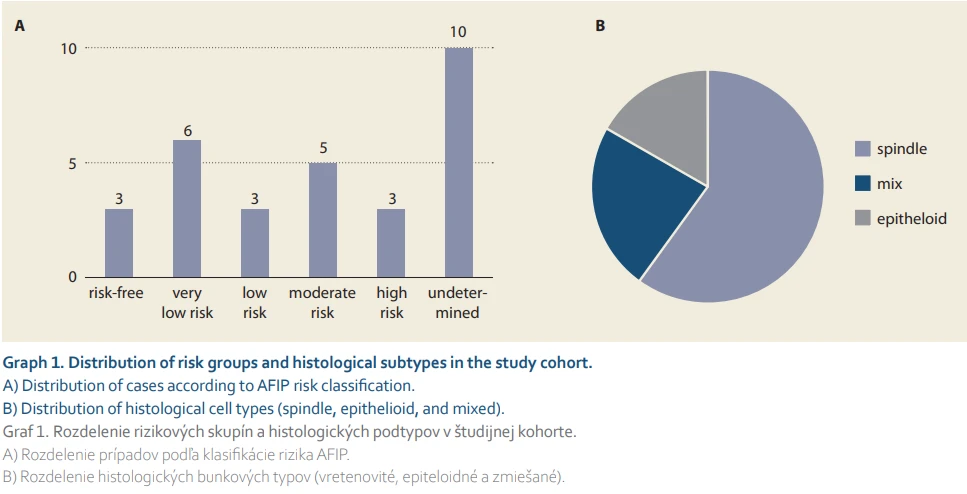
According to risk classification, 10% of cases were categorized as no risk, 20% as very low risk, 10% as low risk, 16.7% as moderate risk, and 10% as high risk, while the risk category could not be determined for 33.3% of cases, mainly due to limited biopsy material and incomplete pathological parameters required for AFIP classification. When the low-risk (0–2) and high-risk (3–4) groups were compared in the analysis, tumor sizes were significantly larger in the high-risk group (P = 0.005). Frequency of necrosis was significantly higher in the high--risk group (75.0%) than in the low-risk group (16.7%) (P = 0.019). Similarly, hemorrhage was present in all cases in the high-risk group, while it was seen in only 41.7% of cases in the low-risk group (P = 0.015) (Tab. 1, Graph 1).
A mitotic count of > 5/50 HPF was detected only in the high-risk group, and this difference was significant (P = 0.049). No significant differences were observed between the risk groups in terms of gender, localization, cell type, ulceration, and Ki-67 proliferation index (P > 0.05 for all) (Tab. 1, 2).
When cell types were examined, 60.0% of the cases were spindle-shaped, 16.7% were epithelioid, and 23.3% were mixed. Necrosis was present in 26.7% of the cases, and hemorrhage was present in 50% (Tab. 1). In additional univariate analyses, necrosis was associated with tumor size (P = 0.026) and mitotic index (P = 0.019), while hemorrhage was associated with tumor size (P = 0.0078) but not mitotic index (P = 0.223).
Immunohistochemically, CD117 positivity was 96.7%, and diffuse and strong staining was observed in 70.0% of cases. CD34 positivity was 93.3%, and DOG1 positivity was found in all cases (100%). Diffuse and strong cytoplasmic expression was observed in 83.3% of DOG1 staining. Immunoreaction: No significant relationship was found between patterns and risk classification (P > 0.05 for all) (Tab. 3).
Discussion
In this study, the clinical, histopathological, and immunohistochemical features of GIST cases diagnosed in our center were evaluated.
GISTs are mostly seen in individuals over 50 years of age, with a slight male predominance [17,18]. In our study, patients had a wide age range, with 86.6% of cases over 50 years of age and 53.3% male, which is consistent with the literature.
GISTs are often detected incidentally. Most symptomatic cases present with symptoms such as gastrointestinal bleeding and associated fatigue caused by the tumor [19,20]. Less commonly, they may present with symptoms of obstruction or compression. In our study, necrosis and hemorrhage were more frequently observed in tumors classified within the high-risk group. In additional analyses evaluating their relationship with established prognostic parameters, necrosis was more commonly identified in larger tumors and in cases with higher mitotic activity, whereas hemorrhage appeared to be primarily associated with tumor size. These findings suggest that necrosis and hemorrhage may reflect overall tumor burden rather than functioning as independent prognostic determinants. Therefore, their association with risk classification in our cohort should be interpreted with caution.
Scores defined by AFIP, based on tumor size, tumor location, and mitotic status, are widely used to predict the risk of recurrence [19]. Tumor sizes vary widely, and in our study, a spectrum ranging from small lesions (< 2 cm) to giant tumors (> 10 cm) was observed. The expected linear relationship between size and risk group was observed; mitotic rate and risk category were significantly increased in larger tumors.
In GISTs, tumor size and mitotic count are the strongest prognostic parameters determining the risk of metastasis and recurrence. It is known that tumors smaller than 2 cm are considered low-risk, while tumors larger than 10 cm in the stomach and 5 cm in the small intestines are associated with a poor prognosis [21]. When tumor size and mitotic count are evaluated together, a mitotic count greater than 10 in 50 HPF is associated with an increased risk of recurrence and metastasis [22]. In our study, tumor size ranged from 0.5 to 15 cm, with a mean of 4.4 cm, and the largest tumor was measured at 15 cm.
In the literature, tumor necrosis and perforation are also reported. It has been reported that these are independent factors that negatively affect the outcome [20,23]. The presence of necrosis and hemorrhage is an indicator of aggressive biological behavior, and in our study, these parameters were observed more frequently, especially in the high--risk group. This finding suggests that poor prognostic features cluster in a mutually supportive manner.
Because it is often impossible to determine prognosis based on a single parameter in GIST cases, research on different genetic and molecular pathways is ongoing. KIT mutations are detected in approximately 85% of GIST cases, and this mutation plays an important targetable role in treatment [24]. PDGFRa mutations have been identified in approximately 5–7% of cases without KIT mutations [18].
Although tumors can be observed in different localizations, the most common location is the stomach; EGISTs constitute less than 5% of all GISTs [25,26]. In our study, tumors were most frequently located in the stomach (66.7%), followed by the small intestines (23.3%), colon (6.7%), and EGIST (3.3%). The observed EGIST rate in our cohort is consistent with previously reported data.
GISTs can exhibit different cellular patterns, including spindle, epithelioid, and mixed. The higher prevalence of the spindle type is consistent with the known natural distribution of GISTs. Some studies have reported that mixed and epithelioid tumors may be associated with more aggressive histological features [27]. In our study, 63.3% of the cases were spindle, 26.6% were epithelioid, and 10% were mixed. This distribution is consistent with the literature reporting a higher prevalence of the spindle type.
CD117, CD34, and DOG1 immunohistochemical markers are widely used in the diagnosis of GIST due to their high sensitivity and specificity [17,28]. In our study, almost all cases showed a positive immunoreaction with CD117. This finding is consistent with the literature reporting that KIT protein expression is positive in approximately 95% of GISTs. CD117 prevalence, as well as staining intensity, was mostly moderate to strong. Although limited/focal staining was observed in some low-risk cases, this condition was not found to be statistically significantly associated with risk classification. CD34 positivity was detected in 93.3% of the cases in our cohort. Although this rate appears higher than that reported in some large series (60–70%), variations in tumor localization and sample composition may contribute to this difference. In our study, no significant association between CD34 and risk classification was found.
DOG1 staining is one of the most striking immunohistochemical findings of our study. Diffuse and strong DOG1 positivity was detected in the majority of cases. This result is consistent with studies demonstrating high sensitivity of DOG1, particularly in CD117-negative GIST cases. Although a slight decrease in DOG1 prevalence was observed as the risk category increased, this was not statistically significant.
When the relationship between the number of mitoses and CD117 staining pattern was examined, the mean number of mitoses was found to be significantly higher in cases with focal or weak CD117 positivity. This relationship has been evaluated by only a few studies [29], and it is noteworthy because the effect of KIT expression on biological behavior is controversial. Our finding suggests that low KIT expression is associated with more aggressive disease. This suggests that it may reflect proliferative activity; however, this relationship needs to be confirmed in a larger series. The relationship between the Ki-67 proliferation index and risk group showed a numerical trend toward higher values in the high-risk group, with Ki-67 ≥ 10% observed in 60% of high-risk cases; however, this difference did not reach statistical significance. Although previous studies have suggested that Ki-67 may serve as a complementary prognostic marker in GISTs, our findings indicate that its role requires further investigation. Elevated Ki-67 expression tended to be more common in tumors with a mitotic rate of > 5/50 HPF and in larger tumors.
Prognostic parameters such as tumor size, mitotic count, and tumor localization have a strong relationship with risk classification. We comprehensively evaluated the clinical, histopathological, and immunohistochemical features of GIST cases followed at our center. The data showed that GISTs were most commonly diagnosed in patients over 50 years of age, with a slight male predominance, were most frequently located in the stomach, and spindle-cell morphology was the dominant histological pattern.
In the immunohistochemical analysis, CD117 (96.7%), CD34 (93.3%), and DOG1 (100%) positivity rates in our cohort were consistent with the literature, further emphasizing the importance of these markers in terms of diagnostic accuracy. Furthermore, the association of focal or weak CD117 expression with high mitotic count is a noteworthy finding, suggesting that it may play a complementary role in determining biological behavior. A Ki-67 proliferation index of 10% or higher was more frequently observed in the high-risk group; however, this association did not reach statistical significance. These findings suggest that Ki-67 may warrant further investigation as a complementary parameter in prognostic assessment.
Adjuvant treatment approaches tailored to the risk group are among the most important factors determining the overall prognosis of patients. Our study supports that risk stratification informs clinical management, immunohistochemical markers provide high diagnostic reliability, and high-risk cases require close follow-up.
These findings emphasize the importance of careful histopathological evaluation in routine practice and may help identify patients who require closer clinical follow-up.
This study has some limitations. Its retrospective and single-center design may modestly limit the generalizability of the findings. In addition, the relatively small sample size may have constrained statistical power in certain subgroup analyses. Variability in biopsy specimen types over the study period limited the consistent assessment of some pathological parameters, including the precise tumor location within tissue layers (mucosa, submucosa, muscularis mucosa, muscularis propria, and serosa), surgical margin status, and growth pattern (expansive vs. infiltrative). As a result, risk classification could not be performed in all cases.
Despite these limitations, the study also has important strengths. All cases were evaluated within a single institution by an experienced pathology team, ensuring uniformity in histopathological and immunohistochemical assessment and minimizing interobserver variability. The study includes a comprehensive panel of routinely used immunohistochemical markers (CD117, DOG1, CD34, desmin, Ki-67), allowing for a robust evaluation of diagnostic features across different GIST presentations. Additionally, the dataset reflects a real-world clinical spectrum encountered in routine practice, including small biopsies and heterogeneous specimen types, which enhances the practical relevance of the findings. Together, these strengths support the reliability of the observed histopathological patterns contributing valuable data to the literature on the diagnostic features of GISTs.
In conclusion, tumor size and mitotic activity remain the most robust and widely accepted predictors of aggressive behavior in GISTs. In our cohort, necrosis and hemorrhage were more frequently observed in high-risk tumors and may represent additional histopathological features associated with tumor burden. Although Ki-67 showed a numerical increase in high-risk tumors, its prognostic value was not statistically confirmed in our cohort warranting further investigation. Given the heterogeneous biological behavior of GISTs, an integrated evaluation combining classical prognostic parameters with histopathological and immunohistochemical findings may provide a more comprehensive framework for risk assessment and clinical decision-making.
Author contributions
GE: Conceptualization, study design, data acquisition, histopathological evaluation, writing – original draft, supervision.
TD: Data collection, methodology, immunohistochemical evaluation, writing – review &editing.
SST: Statistical analysis, interpretation of results, critical revision of the manuscript.
EA: Data acquisition, literature review, preparation of tables and figures.
AE: Data analysis, technical support, manuscript editing.
All authors read and approved the final version of the manuscript.
ORCID of authors
G. Erkilinc 0000-0003-4704-7415,
T. Devrim 0000-0002-5321-2002,
S. S. Tuncer 0000-0003-0872-7493,
E. Ayhan 0000-0003-0524-9254,
A. Demirel 0009-0000-6415-2490.
Submitted/Doručené: 1. 2. 2026
Accepted/Prijaté: 16. 3. 2026
Corresponding author
Prof. Gamze Erkilinc, MD
Department of Medical Pathology
Izmir Bakircay University, Çiğli Training and Research Hospital
8780/1 Sk 18
35620 Çiğli/Izmir Turkey
gamze.erkilinc@bakircay.edu.tr
Sources
1. Lopes DD, Pereira R, Couto E et al. Cerebral metastasis of a gastrointestinal stromal tumor: a case report and literature review. Cureus 2025; 17 (6): e85857. doi: 10.7759/cureus.85857.
2. Kurokawa Y, Honma Y, Sawaki A et al. Pimitespib in patients with advanced gastrointestinal stromal tumor (CHAPTER-GIST-301): a randomized, double-blind, placebo-controlled phase III trial. Ann Oncol 2022; 33 (9): 959–967. doi: 10.1016/j.annonc.2022.05.518.
3. Napolitano A, Vincenzi B. Secondary KIT mutations: the GIST of drug resistance and sensitivity. Br J Cancer 2019; 120 (6): 577–578. doi: 10.1038/s41416-019-0388-7.
4. Aregawi AB, Fenta BD, Worku MA et al. Gastrointestinal stromal tumors with atypical features and presentations: a case series. Int J Surg Case Rep 2025; 133 : 111569. doi: 10.1016/j.ijscr.2025.111569.
5. Miettinen M, Lasota J. Gastrointestinal stromal tumors: definition, clinical, histological, immunohistochemical, and molecular genetic features and differential diagnosis. Virchows Arch 2001; 438 (1): 1–12. doi: 10.1007/s004280000338.
6. Kurt F, Ozlu O, Basaran A. Surgical and histopathologic outcomes of gastrointestinal stromal tumors. Ann Ital Chir 2021; 92 : 604–608.
7. Coskun SK. Clinicopathological features of gastrointestinal stromal tumors and review of the literature: a single institution experience. Konuralp Med J 2022; 14 (2): 373–379. doi: 10.18521/ktd.1094503.
8. Gök MA, Yeğen SF, Kafadar MT et al. The role of immunohistochemical markers and tumor size on prognosis in gastrointestinal stromal tumors. Kocaeli Med J 2022; 11 (1): 101–106. doi: 10.5505/ktd.2022.97769.
9. Ngow HA, Nowalid WM, Kharina W. Gastrointestinal stromal tumour: cause of obscure gastrointestinal bleeding case report. Ces Slov Gastroent Hepatol 2010; 64 (5): 22–25.
10. Nishida T, Blay JY, Hirota S et al. The standard diagnosis, treatment, and follow-up of gastrointestinal stromal tumors based on guidelines. Gastric Cancer 2016; 19 (1): 3–14. doi: 10.1007/s10120-015-0526-8.
11. Rîmbu MC, Popescu L, Mihăilă M et al. Synergistic effects of green nanoparticles on antitumor drug efficacy in hepatocellular cancer. Biomedicines 2025; 13 (3): 641. doi: 10.3390/biomedicines13030641.
12. Abera SA, Tadesse AK, Abera KA et al. Duodenal gastrointestinal stromal tumor presenting with life‑threatening upper GI bleeding in a young patient. Clin Case Rep 2024; 12 (4): e8796. doi: 10.1002/ccr3.8796.
13. Miettinen M, Sobin LH, Lasota J. Gastrointestinal stromal tumors of the stomach. Am J Surg Pathol 2005; 29 (1): 52–68. doi: 10.1097/01.pas.0000146010.92933.de.
14. Miettinen M, Makhlouf H, Sobin LH et al. Gastrointestinal stromal tumors of the jejunum and ileum. Am J Surg Pathol 2006; 30 (4): 477–489. doi: 10.1097/00000478-200604000-00008.
15. Liegl-Atzwanger B, Fletcher JA, Fletcher CD. Gastrointestinal stromal tumors. Virchows Arch 2010; 456 (2): 111–127. doi: 10.1007/s00428-010-0891-y.
16. Nishida T, Hirota S. Biological and clinical review of stromal tumors in the gastrointestinal tract. Histol Histopathol 2000; 15 (4): 1293–1302. doi: 10.14670/HH-15.1293.
17. Corless CL. Gastrointestinal stromal tumors: what do we know now? Mod Pathol 2014; 27 (Suppl 1): S1–S16. doi: 10.1038/modpathol. 2013.173.
18. Heinrich MC, Corless CL, Duensing A et al. PDGFRA activating mutations in gastrointestinal stromal tumors. Science 2003; 299 (5607): 708–710. doi: 10.1126/science.1079666.
19. Chen T, Qiou H, Feng X et al. Comparison of modified NIH and AFIP risk-stratification criteria for gastrointestinal stromal tumors. Zhonghua Wei Chang Wai Ke Za Zhi 2017; 20 (9): 1020–1024.
20. Zheng J, Li R, Qiu H et al. Tumor necrosis and >20 mitoses per 50 high-power fields can distinguish “very high‑risk” and “highest-risk” within “high-risk” gastric gastrointestinal stromal tumor. Future Oncol 2018; 14 (7): 621–629. doi: 10.2217/fon-2017-0509.
21. Miettinen M, El‑Rifai WE, Sobin LH et al. Evaluation of malignancy and prognosis of gastrointestinal stromal tumors. Hum Pathol 2002; 33 (5): 478–483. doi: 10.1053/hupa.2002.124123.
22. Fletcher CD, Berman JJ, Corless C et al. Diagnosis of gastrointestinal stromal tumors: a consensus approach. Int J Surg Pathol 2002; 10 (2): 81–89. doi: 10.1177/106689690201000201.
23. Supsamutchai C, Wilasrusmee C, Hiranyatheb P et al. A cohort study of prognostic factors associated with recurrence or metastasis of gastrointestinal stromal tumor (GIST) of stomach. Ann Med Surg 2018; 35 : 1–5. doi: 10.1016/j.amsu.2018.08.010.
24. Jang NR, Choi JH, Gu MJ. Expression of p16 predicts poor outcome for patients with gastrointestinal stromal tumors. Int J Clin Exp Pathol 2017; 10 (6): 6912–6917.
25. Sui XL, Wang H, Sun XW et al. Expression of DOG1, CD117 and PDGFRA in gastrointestinal stromal tumors and correlations with clinicopathology. Asian Pac J Cancer Prev 2012; 13 (4): 1389–1393. doi: 10.7314/apjcp.2012.13.4.1389.
26. Kara T, Serinsoz E, Arpaci RB et al. Contribution of DOG1 expression to the diagnosis of gastrointestinal stromal tumors. Pathol Res Pract 2013; 209 (7): 413–417. doi: 10.1016/j.prp.2013.04.005.
27. Hirota S, Ohashi A, Nishida T et al. Gain-of-function mutations of platelet-derived growth factor receptor alpha gene in gastrointestinal stromal tumors. Gastroenterology 2003; 125 (3): 660–667. doi: 10.1016/s0016-5085 (03) 01046-1.
28. Güler B, Özyılmaz F, Tokuç B et al. Histopathological features of gastrointestinal stromal tumors and the contribution of DOG1 expression to the diagnosis. Balkan Med J 2015; 32 (4): 388–396. doi: 10.5152/balkanmedj.2015.15912.
29. Kaymaz E, Taşdöven İ, Barut F. The relationship of clinicopathological findings and PDGFR‑b expression with tumor recurrence in gastrointestinal stromal tumors. Turk J Gastroenterol 2021; 32 (12): 1038–1048. doi: 10.5152/tjg.2021.21148.
Labels
Paediatric gastroenterology Gastroenterology and hepatology SurgeryArticle was published in
Gastroenterology and Hepatology

2026 Issue 3
Most read in this issue
- Current options for drug therapy in perianal Crohn’s disease
- Role of home parenteral nutrition in gastroenterology
- Oral sulfate solution as a modern approach to bowel preparation for colonoscopy: evidence and clinical data
- Extracorporeal shock wave lithotripsy in patients with the algic obstructive form of chronic pancreatitis