
Mitral valve rheumatoid nodule complicated by infective endocarditis
Authors:
Monika Manethová; Václav Stejskal; Ivo Šteiner; Jiří Soukup
Authors‘ workplace:
The Fingerland Department of Pathology, Charles University, Faculty of Medicine And University Hospital Hradec Kralove
Published in:
Čes.-slov. Patol., 59, 2023, No. 3, p. 129-131
Category:
Overview
We report a case of a 73-year-old male with rheumatoid arthritis presenting with acute abdominal and back pain and rapidly developing multiorgan failure. A positive blood culture (Staphylococcus aureus, Candida species) followed by transoesophageal sonography established a diagnosis of mitral valve infective endocarditis.
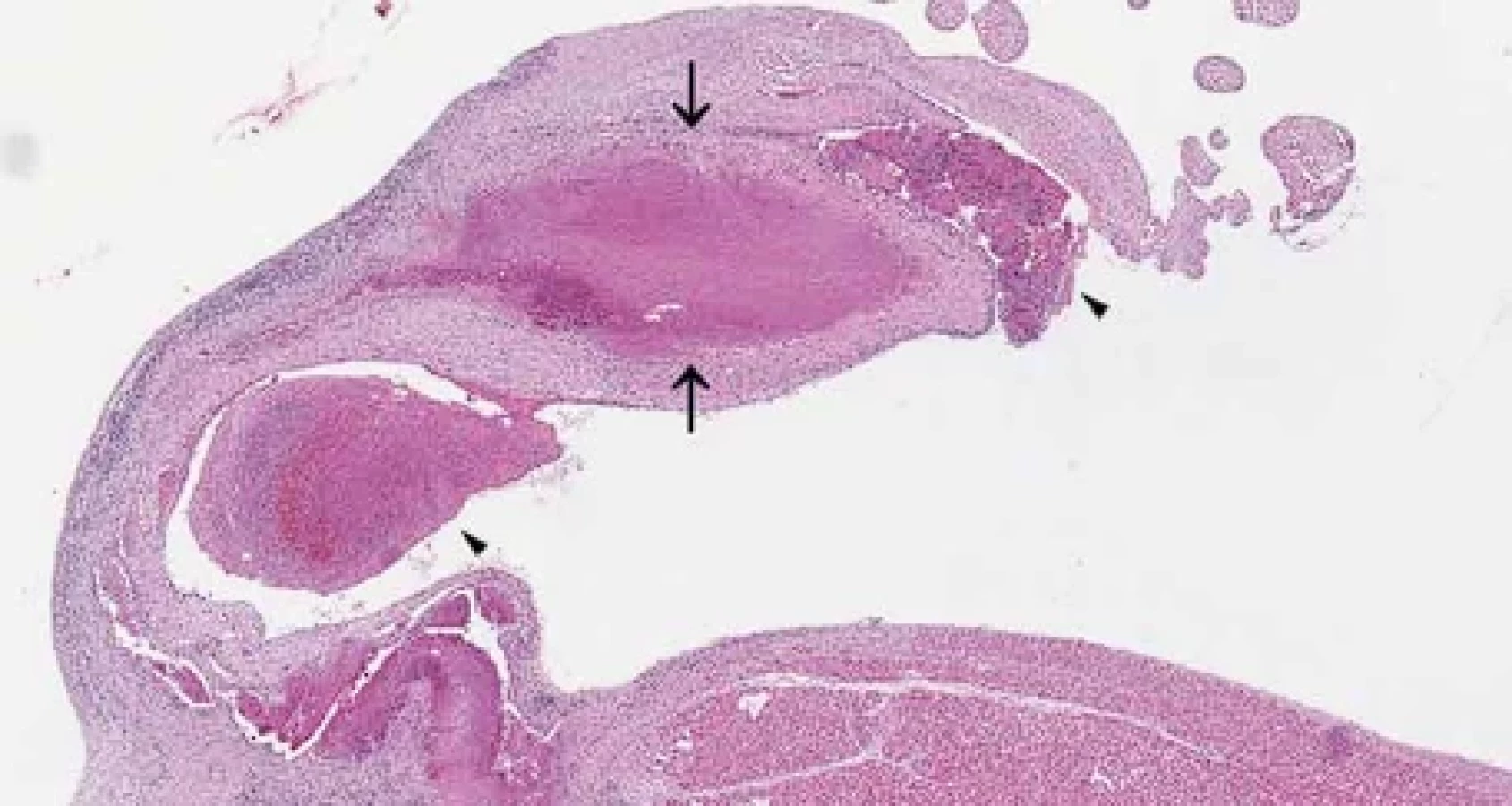
At the autopsy, the heart examination revealed fibrinous pericarditis and multiple small vegetations on the mitral valve. The mitral valve itself showed no significant damage. Surprisingly, the histological examination of the mitral valve showed granulomatous inflammation with central fibrinoid necrosis and peripheral palisade of histiocytes, with occasional giant cells and lymphocytic inflammatory infiltrate - findings consistent with a rheumatoid nodule. Infective vegetations were overlying the nodule.
Due to its relative frequency, a possibility of cardiac involvement by rheumatoid arthritis and its potential infective complications should be considered in patients with appropriate history and clinical symptoms.
Keywords:
infective endocarditis – rheumatoid arthritis – rheumatoid nodule – mitral valve
Rheumatoid arthritis (RA) is a multifactorial chronic systemic autoimmune disease predominantly affecting joints and causing progressive disability, premature death and socioeconomic burden (1). Global prevalence of RA is 460 : 100 000, but varies according to geographical location, and it is increasing, especially in industrialized countries (2, 3). RA arises more frequently in women than men and it can affect patients of any age (4).
Rheumatoid arthritis is characterized by synovial inflammation and synovial hyperplasia, cartilage and bone destruction and autoantibody production (i.e. ACPA – anti-citrullinated protein antibody) (5). RA affects small and large joints of extremities, spine and axial joints. In a poorly controlled or severe disease, there is a risk of extraarticular manifestations, even though its incidence is decreasing due to new and effective treatment possibilities with disease-modifying anti-rheumatic drugs (DMARDS) (5,6).
Heart involvement in RA is relatively common, mostly in form of fibrinous pericarditis. Formation of heart rheumatic nodules is however only rarely reported in the literature and their complication by infectious endocarditis as described in this report is exceptional (7).
CASE DESCRIPTION
We report an autopsy case of a 73-year-old male with second type diabetes mellitus, diagnosed with seropositive rheumatoid arthritis two years prior to his death and treated with corticosteroids. The patient further developed a pulmonary rheumatoid nodule which was biopsied seven months before his death. No cutaneous rheumatoid nodules were described. The patient presented with acute abdominal and back pain at the current admission, with a rapid development of a multiorgan failure. Following positive blood culture (Staphylococcus aureus and Candida species), the transoesophageal sonography was performed, establishing the diagnosis of mitral valve infective endocarditis. A conservative approach was chosen due to the clinical condition of the patient. Acute ischemia of distal ileum and proximal colon developed later, requiring surgical removal of the affected intestine. The patient died 12 days after the admission due to refractory septic shock with multiorgan failure.
After patient’s death, a standard autopsy was performed at our department. The main findings consisted of severe atherosclerosis of the aorta and changes after previous proctocolectomy, right lung lower lobe resection and partial resection of the diaphragm with pleural adhesions. Small infarcts in the spleen and right kidney were also present. The heart showed fibrinous pericarditis and multiple small vegetations on the mitral valve at the autopsy, while the mitral valve itself showed no significant damage.
The histological examination identified granulomatous valve inflammation with central fibrinoid necrosis and peripheral palisade of histiocytes, with occasional giant cells and lymphocytic inflammatory infiltrate – findings consistent with rheumatoid nodule in rheumatoid arthritis. Infective vegetations were overlying the nodule (Fig.1, Fig.2). Special stains (Gram, Grocott, Ziehl-Neelsen) were negative. Another rheumatoid nodule with identical morphology was further identified in pleural adhesions of the right lung.

DISCUSSION
The involvement of the cardiovascular system in rheumatoid arthritis is relatively common, and it is associated with increased mortality. The involvement includes fibrinous pericarditis (most commonly), cardiomyopathy, myocarditis, cardiac amyloidosis, coronary vasculitis, arrhythmias and valve disease, but also congestive heart failure and ischemic heart disease (8). Furthermore, chronic inflammation or the influence of some chronic therapies can promote and accelerate atherosclerotic plaque development or additionally increase vascular vulnerability (9). Patients with rheumatoid arthritis can present with both infective (7) and non-infective (sterile, non-bacterial thrombotic) endocarditis (10), with treatment-related immunosuppression being a possible contributing factor. The symptomatic manifestation of cardiac rheumatoid nodules is rare, although 30 – 50 % of patients with systemic rheumatoid arthritis do have some other kind of cardiovascular involvement (11). There are few well documented cases of rheumatoid nodules of the cardiac valves in the literature, some of them causing acute coronary syndrome or cerebral stroke in case of embolization (11) or causing valvular insufficiency (12). Complication in form of infective endocarditis developing on the background of such a damaged valve is however exceedingly rare (7) and can be potentially fatal, like in our case.
Other extraarticular organ manifestations of RA include keratitis, pulmonary involvement: granulomas (rheumatoid nodules), interstitial lung disease, constrictive or follicular bronchiolitis, bronchiectasis (13); serositis (pleuritis, pericarditis), small vessel vasculitis, cutaneous manifestations, such as classic cutaneous nodules, but also pyoderma gangrenosum, interstitial granulomatous dermatitis, Felty syndrome (14); and neurologic manifestations (15). Central and peripheral nervous system is usually affected due to small vessel vasculitis, joint damage or drug toxicity. Microvascular cerebral damage is associated with the development of the Azheimer´s disease and vascular dementia (15).
The exact etiology of rheumatoid nodules is not known (16). Classic rheumatoid nodules commonly occur in genetically predisposed patients with severe, seropositive arthritis (16). Homozygosity for HLA-DRB1*0401 makes RA patients susceptible to involvement of major organs (17). Studies of cytokine composition suggest that the nodule is probably due to a Th-1-mediated inflammatory mechanism (18). Subcutaneous nodules could be also associated with previous trauma (19). Methotrexate therapy or other systemic therapies can paradoxically induce or exacerbate nodule formation (20). Cardiac valvular nodules may arise on any cusp or valvular ring, but are most commonly described on the mitral and aortic valve (21).
Incidence of infective endocarditis is annually estimated between 15 to 80 cases per million persons in population-based studies and it is markedly increased in patients with valve prostheses or with prior infective endocarditis. Impaired valvular endothelium is a predisposing factor for vegetation formation
(22) and apparently played a role in our case as well. Affected patients are older and the most frequent responsible microorganism is Staphylococcus sp. (23). Infective endocarditis as a complication of intracardiac rheumatoid nodule is only exceptionally reported (7).
According to a study of Meune et al. RA is associated with 60 % increase in risk of cardiovascular death in comparison to general population and the standardized mortality ratio has remained unchanged over the past decades (9, 24). RA patients also have twice the risk of myocardial infarction compared to general population (15). Compared to the healthy population, the mortality rate is higher in patients with rheumatoid arthritis and cardiovascular and other systemic complications remain a major challenge (25). Thus, reduction of cardiovascular mortality should be considered one of the main targets in RA management (9, 24). Suspicion of rheumatoid nodules and their potential infective complications should be also considered in patients with rheumatoid arthritis and cardiac or systemic symptoms.
Funding
This study was supported by Ministry of Health, Czech Republic, project No. NV19-01-00435 and by the project BBMRI-CZ LM2023033.
Conflict of interest
The authors declare that there is no conflict of interest regarding the publication of this paper.
Correspondence address:
MUDr. Monika Manethová
The Fingerland Department of Pathology
Charles University, Faculty of Medicine and University Hospital Hradec Kralove
Sokolská 581, 500 05 Hradec Králové, Czech republic e-mail: manethom@lfhk.cuni.cz
tel: +420 495 832 896
Sources
- Guo Q, Wang Y, Xu D, et al. Rheumatoid arthritis: pathological mechanisms and modern pharmacologic therapies. Bone Res 2018; 6 : 15.
- Finckh A, Gilbert B, Hodkinson B, et al. Global epidemiology of rheumatoid arthritis. Nat Rev Rheumatol 2022; 18 : 591-602.
- Almutairi K, Nossent J, Preen D, et al. The global prevalence of rheumatoid arthritis: a meta-analysis based on a systematic review. Rheumatol Int 2021; 41 : 863-877.
- Radu AF, Bungau SG. Management of Rheumatoid Arthritis: An Overview. Cells 2021; 10.
- Li N, Wang JC, Liang TH, et al. Pathologic finding of increased expression of interleukin-17 in the synovial tissue of rheumatoid arthritis patients. Int J Clin Exp Pathol 2013; 6 : 1375-1379.
- Conforti A, Di Cola I, Pavlych V, et al. Beyond the joints, the extra-articular manifestations in rheumatoid arthritis. Autoimmun Rev 2021; 20 : 102735.
- Giladi H, Sukenik S, Flusser D, et al. A rare case of enterobacter endocarditis superimposed on a mitral valve rheumatoid nodule. J Clin Rheumatol 2008; 14 : 97-100.
- Voskuyl AE. The heart and cardiovascular manifestations in rheumatoid arthritis. Rheumatology (Oxford) 2006; 45 Suppl 4: iv4-7.
- Meune C, Touze E, Trinquart L, et al. Trends in cardiovascular mortality in patients with rheumatoid arthritis over 50 years: a systematic review and meta-analysis of cohort studies. Rheumatology (Oxford) 2009; 48 : 1309-1313.
- Choi JH, Park JE, Kim JY, et al. Non-Bacterial Thrombotic Endocarditis in a Patient with Rheumatoid Arthritis. Korean Circ J 2016; 46 : 425-428.
- Tennyson C, Kler A, Chaturvedi A, et al. Rheumatoid nodule on the anterior mitral valve leaflet. J Card Surg 2018; 33 : 643-645.
- Chand EM, Freant LJ, Rubin JW. Aortic valve rheumatoid nodules producing clinical aortic regurgitation and a review of the literature. Cardiovasc Pathol 1999; 8 : 333-338.
- Kadura S, Raghu G. Rheumatoid arthritis-interstitial lung disease: manifestations and current concepts in pathogenesis and management. Eur Respir Rev 2021; 30.
- Sayah A, English JC, 3rd. Rheumatoid arthritis: a review of the cutaneous manifestations. J Am Acad Dermatol 2005; 53 : 191-209; quiz 210-192.
- Figus FA, Piga M, Azzolin I, et al. Rheumatoid arthritis: Extra-articular manifestations and comorbidities. Autoimmun Rev 2021; 20 : 102776.
- Garcia-Patos V. Rheumatoid nodule. Semin Cutan Med Surg 2007; 26 : 100-107.
- Weyand CM, Xie C, Goronzy JJ. Homozygosity for the HLA-DRB1 allele selects for extraarticular manifestations in rheumatoid arthritis. J Clin Invest 1992; 89 : 2033-2039.
- Hessian PA, Highton J, Kean A, et al. Cytokine profile of the rheumatoid nodule suggests that it is a Th1 granuloma. Arthritis Rheum 2003; 48 : 334-338.
- Brawer AE, Goel N. The onset of rheumatoid arthritis following trauma. Open Access Rheumatol 2016; 8 : 77-80.
- Tilstra JS, Lienesch DW. Rheumatoid Nodules. Dermatol Clin 2015; 33 : 361-371.
- Bonfiglio T, Atwater EC. Heart disease in patients with seropositive rheumatoid arthritis; a controlled autopsy study and review. Arch Intern Med 1969; 124 : 714-719.
- Iung B, Duval X. Infective endocarditis: innovations in the management of an old disease. Nat Rev Cardiol 2019; 16 : 623-635.
- Iung B. Infective endocarditis. Epidemiology, pathophysiology and histopathology. Presse Med 2019; 48 : 513-521.
- van den Hoek J, Roorda LD, Boshuizen HC, et al. Trend in and predictors for cardiovascular mortality in patients with rheumatoid arthritis over a period of 15 years: a prospective cohort study. Clin Exp Rheumatol 2016; 34 : 813-819.
- McInnes IB, Schett G. The pathogenesis of rheumatoid arthritis. N Engl J Med 2011; 365 : 2205-2219.
Labels
Anatomical pathology Forensic medical examiner ToxicologyArticle was published in
Czecho-Slovak Pathology

2023 Issue 3
Most read in this issue
- Stevens-Johnson syndrome and toxic epidermal necrolysis from pathologist’s point of view
- Clinical and histopathological aspects of the most common inflammatory non-infectious skin diseases
- Tall cell carcinoma of the breast with reversed polarity - a report of three cases with a review of the literature
- Diagnostic Pitfalls in Dermatopathology