
Junctional zone thickness on magnetic resonance imaging – a non-invasive diagnostic method for adenomyosis and beyond
Authors:
Jule Eriç Horasanl 1; Fatih Akkuş 2; Pinar Diydem Yılmaz 3; Cengiz Kadıyoran 3; Ecenur Çetinkuş Polat 1
Authors‘ workplace:
Department of Obstetrics and Gynecology, Necmettin Erbakan University Faculty of Medicine, Konya, Turkey
1; Department of Obstetrics, Gynecology and Perinatology, Kütahya City Hospital, Kütahya, Turkey
2; Department of Radiology, Faculty of Medicine, Necmettin Erbakan University Faculty of Medicine, Konya, Turkey
3
Published in:
Ceska Gynekol 2026; 91(3): 173-180
Category:
Original Article
doi:
https://doi.org/10.48095/cccg2026173
Overview
Background and objectives: Adenomyosis is a prevalent gynecologic disorder involving ectopic endometrial tissue within the myometrium. Magnetic resonance imaging (MRI) enables non-invasive diagnosis, yet the role of junctional zone (JZ) thickness in predicting coexisting intrauterine pathologies remains uncertain. This study evaluated the diagnostic and predictive value of MRI-based JZ thickness in hysterectomy-confirmed adenomyosis. Materials and methods: This retrospective study included 420 patients who underwent hysterectomy with preoperative MRI between 2020 and 2025. JZ thickness was measured on sagittal T2-weighted images, and histopathological findings were recorded. Logistic regression analyses were performed to identify independent predictors of intrauterine pathologies. Diagnostic accuracy was assessed using receiver operating characteristic (ROC) curves. Results: The mean JZ thickness was 17.5 ± 3.8 mm. Histopathological evaluation confirmed adenomyosis in 97.1% of cases, with coexisting lesions including myomas (44.5%), endometrial polyps (7.9%), simple hyperplasia (6.2%), atypical hyperplasia (1.9%), and endometrial cancer (2.4%). JZ thickness demonstrated strong positive correlations with polyps (R = 0.46; P < 0.001), simple hyperplasia (R = 0.55; P < 0.001), atypical hyperplasia (R = 0.49; P < 0.001), and myomas (R = 0.38; P < 0.001). Logistic regression identified JZ thickness as the most consistent independent predictor of intrauterine lesions, with an odds ratio of 1.70 for atypical hyperplasia (95% CI 1.11–2.60; P = 0.014). ROC analysis revealed excellent discriminative ability for simple hyperplasia (AUC = 0.842), atypical hyperplasia (AUC = 0.888), and polyps (AUC = 0.840), while predictive performance for myomas was moderate (AUC = 0.661). Conclusions: MRI-based measurement of JZ thickness is a reliable, non-invasive biomarker for adenomyosis, demonstrating an additional predictive value for coexisting premalignant intrauterine pathologies. Incorporating JZ thickness thresholds into routine imaging evaluation may enhance risk stratification, reduce unnecessary invasive procedures, and inform about personalized management strategies in women with adenomyosis.
Keywords:
adenomyosis – magnetic resonance imaging – junctional zone – non-invasive diagnosis
Introduction
Defined by the presence of ectopic endometrial tissue within the uterine myometrium, adenomyosis is a common gynecologic ailment. Its clinical manifestations are varied, though dysmenorrhea (painful menstruation) and/or menorrhagia (heavy menstrual bleeding) are the predominant presenting complaints [1]. While the signs and symptoms of adenomyosis can differ, the most frequent complaints are painful periods and/or heavy menstrual bleeding. Historically, confirming this condition required a tissue sample (biopsy) or, more often, a hysterectomy. However, modern medicine allows for a non-invasive diagnosis through imaging techniques like ultrasound or magnetic resonance imaging (MRI) [2]. There are two main theories explaining how adenomyosis develops. The first suggests that when the endometrial lining is injured, the basal layer of the endometrium can grow inward into the uterine muscle (myometrium) through a damaged junctional zone, forming adenomyotic lesions. This “tissue injury and repair” idea might explain why prior uterine procedures like a cesarean delivery or D&C (dilation and curettage) increase the risk of developing adenomyosis later. The second theory proposes that adenomyotic lesions come from Müllerian remnants (embryonic cells) that change their form. When we talk about its classification, adenomyosis can be either diffuse (spreading widely) or focal (localized to a specific area) [3].
Precise data on adenomyosis demographics and prevalence remain elusive, largely due to historical underreporting and under-diagnosis. Current prevalence estimates typically fall between 20% and 35%, a narrower range than earlier figures (5% to 70%). The classic portrayal of adenomyosis as a condition primarily affecting pre-menopausal, multiparous women in their 30s and 40s was likely biased by the need for hysterectomy for diagnosis. Advancements in ultrasound and MRI diagnostics have significantly improved our understanding of the affected population [4–6].
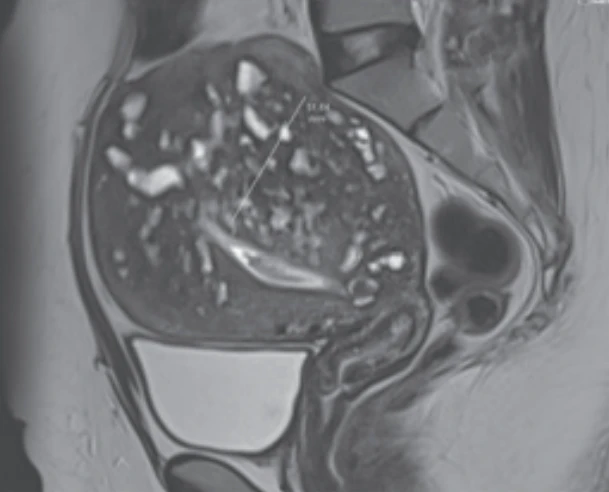
Hyperintense myometrial foci, a direct MRI finding of adenomyosis, provide imaging evidence that corresponds to histopathological features and represent heterotopic endometrial glands within the myometrium. On MRI, they appear as abnormally located T2-bright foci within the myometrium, typically ranging in size from 2 to 7 mm (Fig. 1) [7]. Adenomyosis diagnosis via MRI most commonly relies on an indirect finding: either focal or diffuse thickening of the junctional zone (JZ). Normally, the JZ is situated directly beneath the endometrium and corresponds to the inner dense layer of the myometrium. On T2-weighted images, it appears as a well-defined low-signal intensity band, distinguishable from the adjacent high-signal endometrium and the intermediate-signal outer myometrium. In cases of adenomyosis, this zone may exhibit either localized or widespread thickening (Fig. 2). A JZ thickness of 12 mm or more is widely accepted as a diagnostic threshold, while measurements under 8 mm are strongly predictive of the absence of the disease [8].

Although JZ thickness is a typical finding in adenomyosis, it can also be associated with other gynecologic pathologies. Therefore, we designed this retrospective study to evaluate the relationship between JZ thickness measured by MRI and subsequent histopathologic findings and to determine whether JZ thickness could be used as a predictive marker for concurrent uterine and endometrial pathologies.
Materials and methods
Study type and patient selection
This was a retrospective study conducted at a medical faculty hospital between 2020 and 2025. The medical records of patients who underwent hysterectomy with a diagnosis of adenomyosis and had pre-operative MRI were included in the study. Data were obtained from the hospital’s information management system and patient files. A total of 420 patients were included. The study protocol was reviewed and approved by the Non-Interventional Research Ethics Committee of Necmettin Erbakan University, Meram Faculty of Medicine (Meeting no: 122, Decision No: 2020/2955, Date: December 18, 2020).
Data collection
The clinical, demographic, and pathological data of the patients were collected in detail. The collected data included age, height, weight, body mass index (BMI), parity, gravidity, number of abortions, number of cesarean sections (C/S count), duration of breastfeeding, and infertility status.
Magnetic resonance imaging
All MRI examinations were performed using a Siemens Magnetom Essenza 1.5 Tesla system (Siemens Healthineers, Erlangen, Germany). Patients were scanned in the supine position with a 16-channel phased-array body coil. T2-weighted sequences were obtained, as they provide excellent visualization of uterine anatomy and pathology and are particularly important for the diagnosis of adenomyosis. Additionally, measurements of the endometrial JZ thickness from pre-operative MR images were recorded. The thickness of the JZ was measured on T2-weighted images captured in the midsagittal plane.
Histopathology
Histopathological data, including pathologies found in the uterus, cervix, and ovaries after hysterectomy (such as adenomyosis, endometrial cancer, hyperplasia, polyps, myomas, chronic cervicitis, endometriomas, and cysts), were also examined and recorded.
Patient selection
Inclusion criteria
Patients with a JZ thickness of 12 mm or more on MRI were classified as the “thick JZ” group and included in the study. Additional inclusion criteria were having undergone a hysterectomy and having available histopathological data.
Exclusion criteria
Patients with a JZ thickness of less than 12 mm on MRI were classified as the “normal JZ” group and were excluded from the study. Patients with available MRI data who had undergone hysterectomy at another center and lacked accessible histopathological data were also excluded.
Ethics approval
This study received the necessary approval from the relevant institutional ethics committee. (NEÜ 18. 12. 2020 / 2955) Patient data confidentiality was protected throughout the conduct of the study.
Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, NY, USA) and JASP software, Version 0.19.3 (JASP Team, Amsterdam, The Netherlands). Continuous variables were expressed as mean ± standard deviation (SD) and median (Min.–Max.), whereas categorical variables were presented as frequencies and percentages. The normality of data distribution was assessed using the Kolmogorov-Smirnov test. Correlation analyses between demographic, clinical, and histopathological parameters were conducted using Pearson’s correlation coefficient for normally distributed variables and Spearman’s rank correlation coefficient for non-normally distributed variables. Independent predictors of intrauterine pathologies (endometrial polyp, myoma, simple endometrial hyperplasia, and atypical hyperplasia) were identified through binary logistic regression models. Results were reported as odds ratios (OR) with corresponding 95% confidence intervals (CI). The diagnostic performance of JZ thickness was evaluated by constructing receiver operating characteristic (ROC) curves. The area under the curve (AUC) with 95% CI was calculated, and optimal cutoff values were determined using the Youden index. Sensitivity and specificity values were also reported. A two-tailed P-value of < 0.05 was considered statistically significant.
Results
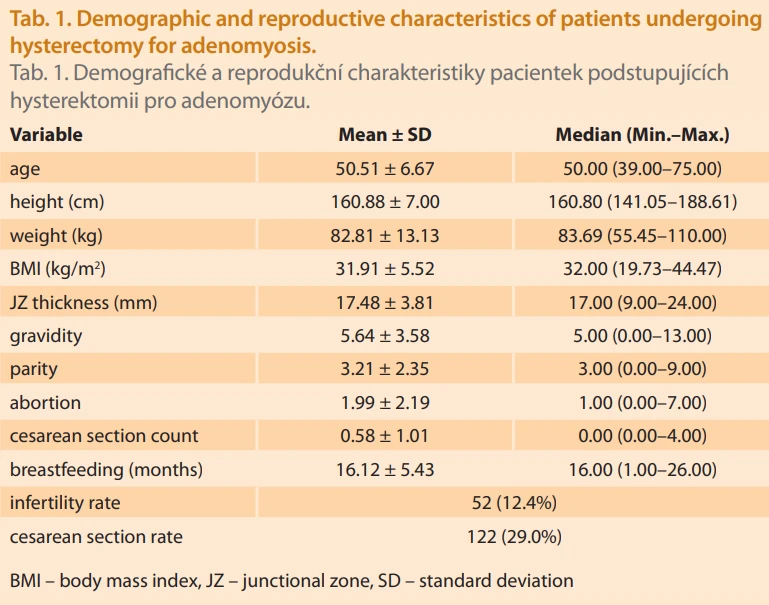
A total of 420 patients who underwent hysterectomy for adenomyosis were included in the study. The demographic and reproductive characteristics of the study population are presented in Tab. 1. The mean age was 50.5 ± 6.7 years (median 50.0; range 39–75). The mean BMI was 31.9 ± 5.5 kg/m², with a mean weight of 82.8 ± 13.1 kg and height of 160.9 ± 7.0 cm. The average JZ thickness was 17.5 ± 3.8 mm (median 17.0; range 9.0–24.0). Reproductive history revealed a mean gravidity of 5.6 ± 3.6, parity of 3.2 ± 2.4, and abortion number of 2.0 ± 2.2. The mean number of cesarean sections was 0.6 ± 1.0, and mean breastfeeding duration was 16.1 ± 5.4 months. The infertility rate was 12.4% (N = 52), and the overall cesarean section rate was 29.0% (N = 122).
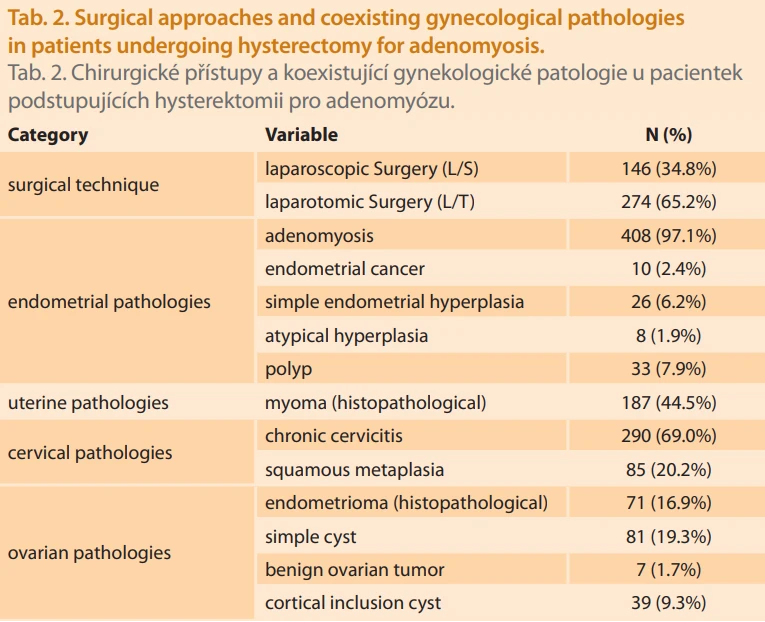
The surgical approaches and concomitant gynecological pathologies are summarized in Tab. 2. Laparoscopic hysterectomy was performed in 34.8% of cases (N = 146), whereas laparotomic hysterectomy accounted for 65.2% (N = 274). Histopathological evaluation confirmed adenomyosis in 97.1% of patients (N = 408). Additional endometrial pathologies included endometrial cancer in 2.4% (N = 10), simple endometrial hyperplasia in 6.2% (N = 26), atypical hyperplasia in 1.9% (N = 8), and endometrial polyps in 7.9% (N = 33). Myomas were identified in 44.5% of patients (N = 187). Cervical pathologies included chronic cervicitis in 69.0% (N = 290) and squamous metaplasia in 20.2% (N = 85). Ovarian findings were also common, including endometriomas in 16.9% (N = 71), simple cysts in 19.3% (N = 81), benign ovarian tumors in 1.7% (N = 7), and cortical inclusion cysts in 9.3% (N = 39).
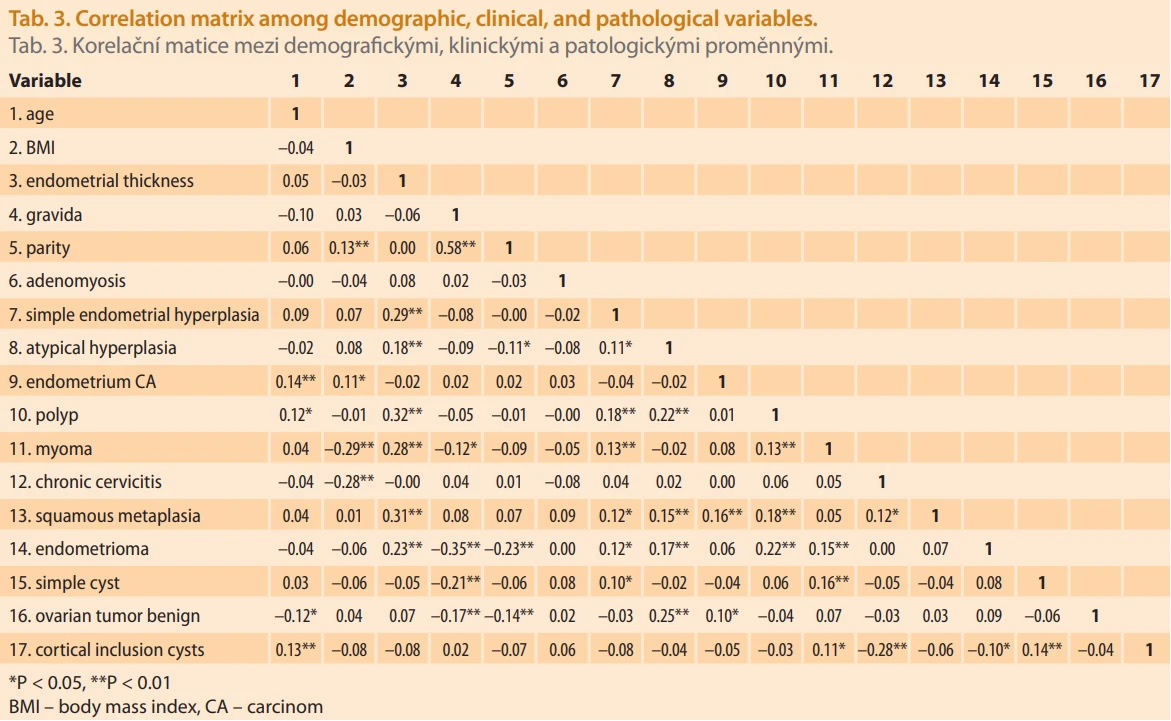
The correlation matrix of clinical, demographic, and histopathological variables is presented in Tab. 3. JZ thickness demonstrated the strongest positive correlations with intrauterine lesions, including polyps (R ≈ 0.46; P < 0.001), simple endometrial hyperplasia (R ≈ 0.55; P < 0.001), atypical hyperplasia (R ≈ 0.49; P < 0. 001), and myomas (R ≈ 0.38; P < 0.001). Age was positively correlated with polyps (R ≈ 0.32; P < 0.05) and atypical hyperplasia (R ≈ 0.28; P < 0.05), while BMI showed a negative correlation with myomas (R ≈ –0.41; P < 0.01). In contrast, gravidity, parity, abortion history, and breastfeeding duration demonstrated no significant associations with intrauterine pathologies.
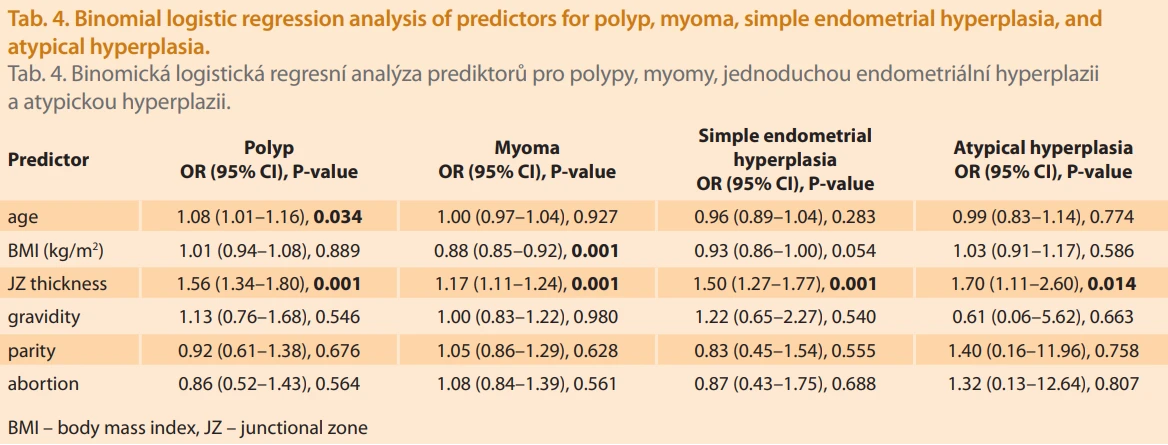
Binomial logistic regression analysis of predictors for polyps, myomas, simple endometrial hyperplasia, and atypical hyperplasia is shown in Tab. 4. JZ thickness was the most consistent independent predictor: polyps (OR 1.56; 95% CI 1.34–1.80; P = 0.001), myomas (OR 1.17; 95% CI 1.11–1.24; P = 0.001), simple endometrial hyperplasia (OR 1.50; 95% CI 1.27–1.77; P = 0.001), and atypical hyperplasia (OR 1.70; 95% CI 1.11–2.60; P = 0.014). Age was an additional predictor for polyps (OR 1.08; 95% CI 1.01–1.16; P = 0.034). Conversely, BMI was inversely associated with myomas (OR 0.88; 95% CI 0.85–0.92; P = 0.001). Gravidity, parity, and abortion history were not significant predictors in multivariable analysis.
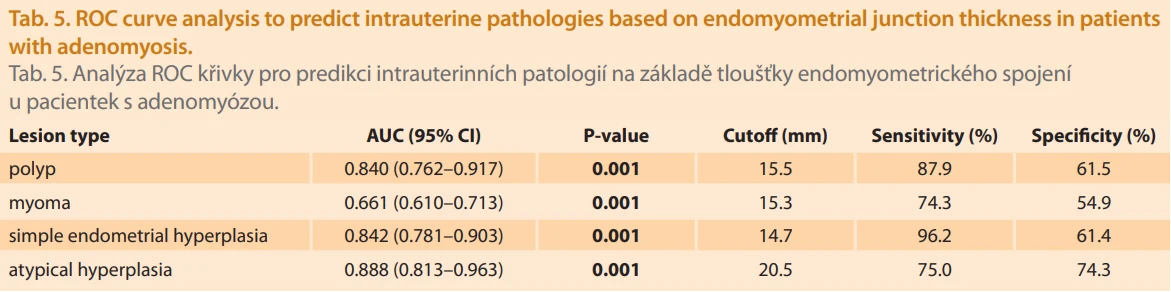
The diagnostic performance of JZ thickness for predicting intrauterine lesions is illustrated in Fig. 3 (is available on the journal’s website) and detailed in Tab. 5. JZ thickness showed excellent discriminative power for simple endometrial hyperplasia (AUC 0.842; 95% CI 0.781–0.903; P = 0.001; cutoff 14.7 mm, sensitivity 96.2%; specificity 61.4%) and atypical hyperplasia (AUC 0.888; 95% CI 0.813–0.963; P = 0.001; cutoff 20.5 mm; sensitivity 75.0%; specificity 74.3%). For polyps, the AUC was 0.840 (95% CI 0.762–0.917; P = 0.001; cutoff 15.5 mm; sensitivity 87.9%; specificity 61.5%). In contrast, the predictive ability for myomas was moderate (AUC 0.661; 95% CI 0.610–0.713; P = 0.001; cutoff 15.3 mm; sensitivity 74.3%; specificity 54.9%).

Discussion
This retrospective study investigates the diagnostic value of junctional zone (JZ) thickness measured on MRI in predicting adenomyosis and its associated intrauterine pathologies. Among 420 patients diagnosed with adenomyosis and who underwent hysterectomy, the mean JZ thickness was found to be 17.5 ± 3.8 mm. Notably, adenomyosis was diagnosed in 97% of patients with a JZ thickness greater than 12 mm.
When evaluating the sociodemographic characteristics and MRI findings of our sample, the mean JZ thickness was found to be 17.5 ± 3.8 mm. The average number of pregnancies was 5.6 ± 3.6, the mean parity was 3.2 ± 2.4, and the average number of miscarriages was 2.0 ± 2.2. The rate of infertility was 12.4% (N = 52), and the overall cesarean section rate was 29.0% (N = 122). The study also observed a 12.4% infertility rate, supporting existing literature that links adenomyosis with impaired implantation and adverse reproductive outcomes. In our study, the prevalence of adenomyosis was higher among women with a history of multiple pregnancies and deliveries, a finding that has also been reported in other studies.
Among the coexisting uterine pathologies, myomas were the most frequently observed (44.5%), followed by chronic cervicitis (69%), endometrial polyps (7.9%), and endometrial hyperplasia (6.2% for simple; 1.9% for atypical). While JZ thickness demonstrated moderate diagnostic value for myomas (AUC: 0.661), its predictive ability was significantly higher for endometrial polyps (AUC: 0.840), simple hyperplasia (AUC: 0.842), and atypical hyperplasia (AUC: 0.888). An increase of 1 mm in the JZ thickness was found to be linked to a 70% higher likelihood of developing atypical hyperplasia (OR: 1.70; 95% CI 1.11–2.60; P = 0.014) [9,10].
These findings imply that JZ thickening may reflect not only myometrial involvement but also alterations within the endometrial architecture, particularly in hyperplastic and premalignant conditions.
Endometrial polyps, hyperplasia with or without atypia, and adenocarcinoma are more frequently observed among women with adenomyosis. Bergholt and colleagues reported a significant association between adenomyosis and endometrial hyperplasia [11]. The relationship between high estrogen concentrations and adenomyosis, as well as elevated estrogen levels in the menstrual blood of women with adenomyosis, has been previously reported [12]. Additionally, relatively high estrogen biosynthesis due to aromatase activity in human adenomyotic tissue has been described, and it has been suggested that elevated estrogen levels may contribute to the growth of adenomyosis. Tekikkurt and colleagues conducted a retrospective analysis of resected uterine specimens from 319 patients and evaluated endometrial and myometrial lesions associated with adenomyosis. Lesions such as polyps, disordered proliferative endometrium, or hyperplasia were found to be associated with hyperestrogenemia in approximately one-third of the patients [13]. JZ thickness also showed strong predictive ability for the presence of endometrial polyps (AUC: 0.840; sensitivity: 87.9%). Threshold values such as 14.7 mm for simple hyperplasia and 20.5 mm for atypical hyperplasia may serve as useful clinical cutoffs, helping to identify high-risk patients non-invasively and potentially reducing the need for unnecessary invasive procedures.
Interestingly, age was an additional predictor of polyp formation, while BMI was negatively associated with myoma presence, diverging from classical assumptions. The lack of association between gravidity, parity, and abortion history with intrauterine lesions contrasts with older views linking reproductive history to adenomyosis, suggesting a shift in disease patterns and detection due to improved imaging modalities.
The increased mRNA and protein expression of estrogen receptor-a and receptor-b in the myometrium appears to be a risk factor for the development of leiomyoma, along with early menarche, nulliparity, and obesity. Additionally, the levels of growth factors and their receptors are elevated in fibroids. Adenomyosis is commonly found in hysterectomy specimens of patients with concurrent fibroids. The reported incidence of coexisting fibroids ranges from 19% to 57% [14]. In a study conducted on 150 patients, adenomyosis without fibroids was observed in 52%, both adenomyosis and fibroids in 18%, and fibroids alone in 30% of the cases [15].
In our current study, fibroids were the most common coexisting uterine pathology, seen in 44.5% of patients. However, the predictive value of JZ thickness for fibroids was lower (AUC: 0.661). Consistent with recent studies, both conditions often coexist and negatively impact fertility.
While the retrospective and single--center design are limitations, the large sample size and histopathological correlation strengthen the study’s clinical relevance. The findings suggest that JZ thickness is not only a reliable marker for adenomyosis but also a potential non-invasive biomarker for identifying coexisting premalignant and malignant intrauterine lesions.
These data emphasize the enhanced clinical significance of thickness of JZ. Greater thickness of JZ, in addition to its known value in adenomyosis diagnosis, is highly correlated with endometrial polyps, hyperplasia, and atypical hyperplasia and therefore may be an epiphenomenon of intrinsic architectural changes of the endometrium. Therefore, JZ thickness measured by MRI can serve as an even non-invasive biomarker for adenomyosis as well as for identifying patients at higher risk of premalignant intrauterine lesions. This supports the value of incorporating JZ thickness in preoperative risk estimation and individualized treatment planning.
Conclusion
In conclusion, junctional zone thickness measured by MRI is a valuable diagnostic and predictive marker. It reliably indicates adenomyosis and provides additional non-invasive insight into concurrent uterine pathologies, particularly premalignant conditions such as atypical hyperplasia. Incorporating JZ thickness thresholds into routine imaging evaluation may improve risk stratification, reduce unnecessary invasive procedures, and guide personalized clinical management.
Authors’ contributions
J. E. H. (Jule Eriç Horasanlı): Conceptualization, methodology, supervision, project administration, writing – review and editing.
F. A. (Fatih Akkuş): Formal analysis, statistical analysis, data interpretation, visualization, writing – review and editing.
P. D. Y. (Pınar Diydem Yılmaz): MRI assessment, imaging methodology, validation, writing – review and editing.
C. K. (Cengiz Kadıyoran): MRI assessment, imaging methodology, validation, writing – review and editing.
E. Ç. P. (Ecenur Çetinkuş Polat): Data collection, investigation, resources, writing.
All authors have read and approved the final version of the manuscript.
Sources
1. Gordts S, Grimbizis G, Campo R. Symptoms and classification of uterine adenomyosis, including the place of hysteroscopy in diagnosis. Fertil Steril 2018; 109 (3): 380.e1–388.e1. doi: 10.1016/j.fertnstert.2018.01.006.
2. Vannuccini S, Petraglia F. Recent advances in understanding and managing adenomyosis. F1000Res 2019; 8: F1000 Faculty Rev-283. doi: 10.12688/f1000research.17242.1.
3. Guo SW. The pathogenesis of adenomyosis vis-à-vis endometriosis. J Clin Med 2020; 9 (2): 485. doi: 10.3390/jcm9020485.
4. Struble J, Reid S, Bedaiwy MA. Adenomyosis: a clinical review of a challenging gynecologic condition. J Minim Invasive Gynecol 2016; 23 (2): 164–185. doi: 10.1016/j.jmig.2015.09.018.
5. Abbott JA. Adenomyosis and abnormal uterine bleeding (AUB-A) – pathogenesis, diagnosis, and management. Best Pract Res Clin Obstet Gynaecol 2017; 40 : 68–81. doi: 10.1016/j.bpobgyn.2016.09.006.
6. Chapron C, Vannuccini S, Santulli P et al. Diagnosing adenomyosis: an integrated clinical and imaging approach. Hum Reprod Update 2020; 26 (3): 392–411. doi: 10.1093/humupd/dmz049.
7. Novellas S, Chassang M, Delotte J et al. MRI characteristics of the uterine junctional zone: from normal to the diagnosis of adenomyosis. AJR Am J Roentgenol 2011; 196 (5): 1206–1213. doi: 10.2214/AJR.10.4877.
8. Harmsen MJ, Trommelen LM, de Leeuw RA et al. Uterine junctional zone and adenomyosis: comparison of MRI, transvaginal ultrasound and histology. Ultrasound Obstet Gynecol 2023; 62 (1): 42–60. doi: 10.1002/uog.26117.
9. Bergholt T, Eriksen L, Berendt N et al. Prevalence and risk factors of adenomyosis at hysterectomy. Human Reprod 2001; 16 (11): 2418–2421. doi: 10.1093/humrep/16.11.2418.
10. Templeman C, Marshall SF, Ursin G et al. Adenomyosis and endometriosis in the California Teachers Study. Fertil Steril 2008; 90 (2): 415–424. doi: 10.1016/j.fertnstert.2007.06.027.
11. Bergholt T, Eriksen L, Berendt N et al. Prevalence and risk factors of adenomyosis at hysterectomy. Human Reprod 2001; 16 (11): 2418–2421. doi: 10.1093/humrep/16.11.2418.
12. Leyendecker G, Wildt L, Mall G. The pathophysiology of endometriosis and adenomyosis: tissue injury and repair. Arch Gynecol Obstet 2009; 280 (4): 529–538. doi: 10.1007/s00404-009-1191-0.
13. Tetikkurt S, Çelik E, Taş H et al. Coexistence of adenomyosis, adenocarcinoma, endometrial and myometrial lesions in resected uterine specimens. Mol Clin Oncol 2018; 9 (2): 231–237. doi: 10.3892/mco.2018.1660.
14. Molitor JJ. Adenomyosis: a clinical and pathologic appraisal. Am J Obstet Gynecol 1971; 110 (2): 275–284. doi: 10.1016/0002-9378 (71) 90620-x.
15. Shrestha A, Shrestha R, Sedhai LB et al. Adenomyosis at hysterectomy: prevalence, patient characteristics, clinical profile and histopatholgical findings. Kathmandu Univ Med J (KUMJ) 2012; 10 (37): 53–56. doi: 10.3126/kumj.v10i1.6915.
Labels
Paediatric gynaecology Gynaecology and obstetrics Reproduction medicineArticle was published in
Czech Gynaecology

2026 Issue 3
Most read in this issue
- Amniotic band syndrome – a case report of prenatally detected fetal upper limb amputation
- Junctional zone thickness on magnetic resonance imaging – a non-invasive diagnostic method for adenomyosis and beyond
- Lichen sclerosus – insights from a dermatologist and therapeutic approaches
- History and current possibilities of vNOTES in gynecology