
Nutrition of patients undergoing haematopoietic stem cell transplantation
Authors:
B. Kašperová 1; M. Mego 2; S. Čierniková 3; A. Ševčíková 3; S. Kašperová 4; A. Vranovský 1; L. Drgoňa 1
Authors‘ workplace:
Department of Oncohematology, Faculty of Medicine, Comenius University, Bratislava, and National Cancer Institute, Bratislava, Slovakia
1; 2nd Department of Oncology, Faculty of Medicine, Comenius University, Bratislava, and National Cancer Institute, Bratislava, Slovakia
2; Department of Genetics, Cancer Research Institute, Biomedical Research Center of the Slovak Academy of Sciences, Bratislava, Slovakia
3; 1st Department of Internal Medicine, Faculty of Medicine, Comenius University in Bratislava, and University Hospital Bratislava, Slovakia
4
Published in:
Klin Onkol 2025; 38(5): 345-357
Category:
Reviews
doi:
https://doi.org/10.48095/ccko2025345
Overview
Background: Haematopoietic stem cell transplantation is associated with increased demands for adequate caloric intake and heightened risk of macronutrient and micronutrient depletion. Carbohydrates, proteins, and fats represent a key source of energy and structural components for transplanted patients, who often have limited oral intake because of mucositis and loss of appetite and increased nutritional requirements due to catabolism, inflammation, and tissue regeneration. Deficiencies in vitamins and trace elements occurring in some patients play a crucial role in enzymatic reactions, antioxidant defense, immune function, and tissue repair. Preparative regimen also causes damage of the intestinal mucosa and, in combination with antibiotic therapy, reduces the diversity of the microbiome. According to the latest evidence, patient nutrition has an impact on the short - and long-term outcomes of transplantation. Recognition of malnutrition and catabolism in these patients is difficult in routine practice; closer analysis of body composition and early intervention by a clinical nutritionist may be helpful. Adequate nutrient replacement is an important aspect of maintaining nutritional balance and good recovery. Aim: The aim of this article is to provide an overview of nutrition, its specific components and nutritional disorders in oncology patients, as well as to summarize specific complications of aggressive treatment in patients undergoing hematopoietic stem cell transplantation and underline the need for early nutritional intervention in this group of patients.
Introduction
The hematopoietic stem-cell transplantation (HSCT) procedure has undergone a major evolution since the 1990s and, due to its therapeutic potential, has become a routine treatment modality for a wide spectrum of malignant and non-malignant diseases. It allows the use of high doses of cytotoxic agents, sometimes in combination with radiotherapy, which provide sufficient immunoablation, antitumour effect and the creation of a ‘compartment’ in the bone marrow. The severe hematological toxicity is eliminated by the administration of stem cells, which helps to restore hematopoiesis. According to the recommendations of experts, it is important for every patient undergoing a bone marrow transplant to have supervision and individualized nutritional modification, ideally provided by a clinical nutritionist, who should be part of the transplant team [1]. The nutritional status of the patient is one of the prognostic indicators of transplantation success as indicated by studies, although only obesity, diabetes mellitus and liver damage, but not malnutrition, are evaluated by the HCT-Comorbidity Index (HCT-CI) scoring system [2]. An important fact in the assessment of nutritional status is that the BMI (body mass index) is not precise. Malnutrition may also be present in many patients with normal or elevated BMI, and more detailed body composition analysis is needed [3,4]. Patients are at increased risk of malnutrition due to the toxic effect of the preparative regimen, secondary due to severe infections, or graft versus host disease (GVHD), which occurs in approximately one-third of patients and can also affect GIT. It is essential to place strong emphasis on body composition and adequate intake of calories and structural nutrients in patients undergoing HSCT; however, micronutrients, namely vitamins and trace elements, should not be overlooked, as they play a critical role in immune function, enzymatic activity, engraftment of bone marrow and tissue regeneration.
Studies of lymphoma patients undergoing autologous HSCT have shown higher morbidity and mortality in case of malnutrition, with varying results in case of overweight [5]. In a large retrospective analysis of 4,681 subjects, BMI was examined in correlation with transplant outcomes. Significantly higher risk of transplant-associated mortality (TRM) was seen in malnourished patients, which was not seen in patients with obesity or normal BMI. Overall mortality was higher in the malnourished group compared to patients with normal BMI and lower in overweight and obese patients compared to patients with normal weight. The results support the notion that obesity per se should not be a contraindication to autologous transplantation in patients with lymphoma [6]. In small retrospective studies, obesity in case of autologous transplantation was associated with a higher risk of mortality in patients with Non-Hodgkin‘s lymphoma and AML [7,8]. In 1087 multiple myeloma patients undergoing autologous HSCT with melphalan treatment, there was not negative impact of increased BMI on overall survival or mortality [9].
In case of allogeneic HSCT, weight loss and the risk of malnutrition are more frequent and more severe. This is due to the duration of neutropenia, the use of immunosuppressive therapy and the higher risk of severe infectious complications, catabolism, and the occurrence of GVHD [10]. In 2017, a new study by Baumgartner et al. published an analysis of randomized and observational studies about the role of nutrition, including a total of 18,617 patients undergoing allogeneic transplantation. Results from the most studies, including the largest ones showed a negative association between malnutrition and overall survival, a significant increase in transplant-related mortality, and a higher risk of disease relapse [11]. According to the study of 156 allogeneic transplant patients, major weight loss during hospitalization (> 7% of baseline) occurred in 15% of patients, moderate weight loss (2–7%) occurred in 58% of patients, and only 27% maintained weight. Large weight loss led to significantly higher incidence of fever, bacteremia, fungal infections, and higher in-hospital mortality or length of hospital stay [11]. According to a meta-analysis in 2014 that evaluated the incidence of acute GVHD in allogeneic HSCT patients and concurrent overall survival in relation to overweight compared to non-overweight patients, the results showed a higher risk of acute GVHD and worse overall survival in overweight patients [12]. In another study enrolling 331 allogeneic transplant patients, higher BMI in patients (> 25 kg/m2) had no impact on overall survival or progression-free survival; however, overweight and obese patients had more frequent infections and longer hospital stays compared with patients with BMI in the normal range [13]. Similar results showed a study of 2,503 patients with allogeneic HSCT, that patients with underweight condition had significantly lower early and overall survival and greater NRM. Very obese patients had increased NRM, which was associated with the intensity of conditioning regimen [14]. Also allogeneic transplanted patients with acute myeloblastic leukemia had worse OS and higher NRM when obese or occurring weight loss [15]. The different results of the studies may probably be due to the different duration of follow-up, different ethnic group of patients, as well as the different approach of the centres to dose reduction in obese patients.
It is important to maintain a good nutritional status in the post-HSCT period as dysgeusia and inappetence may persist for 1–3 months after the procedure, which has a negative impact not only on the patient‘s quality of life but also on the prognosis [16]. With a weight loss of more than 10% of baseline in the first three months after allogeneic HSCT, a retrospective study of 145 patients found a higher risk of non-relapse mortality (NRM) compared with patients with lower weight loss. About 31% of patients had a weight loss of more than 10%, another third had a weight loss of 5–10%, and only 36% of patients lost less than 5% of weight in the first three months. Cumulative NRM at 2 years from day 90 was different in the three groups (27.3 vs. 8.5 vs. 3.8%). Overall survival at 2 years after day 90 was lower in patients who had major weight loss in the early phase after HSCT compared with patients who lost less than 5% weight (55.3 vs. 73.2%) [17].
This article aims to provide a structured overview of nutrition and its specific components in cancer patients in general, including the importance of macronutrients as key energy and structural sources during the catabolic and inflammatory phases. It also discusses common nutritional disorders such as malnutrition, sarcopenia, micronutrient deficiencies, and refeeding syndrome. Specifically, in patients undergoing HSCT, it focuses on nutritional needs and describes methods for nutritional screening, including validated tools and the importance of body composition assessment. The article further explores eating-related complications frequently encountered during HSCT, such as mucositis, taste alterations, gastrointestinal toxicity, and the impact of graft-versus-host disease on nutrient absorption. It also summarizes ongoing trials in this field. In addition, it outlines current strategies for nutritional support, covering oral, enteral, and parenteral nutrition. The final section emphasizes the importance of early nutritional intervention and outlines future directions in personalized and integrative nutritional care in the transplant setting.
Energy intake and the importance of macronutrients
Weight loss in oncology patients is primarily caused by an energy deficit, which occurs when energy expenditure exceeds intake. In cancer patients, energy demands are increased by the tumor itself and its aggressive growth, which is often accompanied by upregulated glycolysis. A greater tumor burden typically leads to greater energy losses. The body’s response to the tumor – including immune activation, systemic inflammation, B-symptoms, and inefficient metabolic cycles – also contributes to elevated energy expenditure. Meta-analyses have shown that cancer patients have an energy expenditure approximately 8–9% higher than healthy individuals [18], although values may vary significantly between individuals. Currently, predictive equations are commonly used to estimate basal energy expenditure, and when calculating total energy expenditure in cancer patients, adjustments are made for disease-related factors and physical activity levels [19]. Indirect calorimetry measures metabolic oxygen consumption and carbon dioxide output measured at rest, allowing energy expenditure to be calculated for a 24-hour period. To simplify the determination of BEV, equations have been developed that take into account age, height, weight, and gender, and have been compiled based on measurements of healthy individuals. For example, the Harris-Benedict (HB) equation, which is also recommended by the European Group for Blood and Marrow Transplantation (EBMT), is used [1]. However, in malnourished, obese or diseased patients, lower BEV values may be obtained with the HB equation, so if indirect calorimetry is possible, it should be preferred. The advantage over the HB equation is the detection of excessively high hypermetabolism and, conversely, unexpected hypometabolism. Approximately 50% of oncology patients are hypermetabolic, while around 20% are hypometabolic, suggesting that resting energy expenditure is generally elevated in this population. Despite this, studies show that physical activity levels are reduced in cancer patients, resulting in total energy expenditure similar to that of healthy individuals.
According to the European Society for Clinical Nutrition and Metabolism (ESPEN) guidelines, the recommended energy intake for cancer patients is 25–30 kcal/kg of body weight, and 30–35 kcal/kg for those with higher physical activity [20].
Compared to healthy individuals, cancer patients have increased protein requirements and a diminished ability to synthesize conditionally essential amino acids such as glutamine, cysteine, tyrosine, and arginine. Low protein intake has been associated with increased mortality and reduced performance status [21]. Therefore, during periods of metabolic stress, sufficient intake of high-biological-value protein – rich in essential amino acids and usable nitrogen – is crucial. A bolus intake of 30 g of such protein can stimulate muscle protein synthesis for 3–6 hours. Muscle protein synthesis also depends on physical activity; during immobility or bed rest, protein synthesis declines and breakdown increases within 24 hours, potentially leading to anabolic resistance within a few days, reducing the muscle’s sensitivity to dietary protein. Systemic inflammation and tumor-related catabolism further contribute to cancer cachexia. Anabolic processes can still be supported during precachexia through increased intake of protein and branched-chain amino acids, particularly leucine [22], as well as through anti-inflammatory therapy aimed at reducing systemic inflammation and oxidative stress [23].
According to professional society ESPEN, protein intake should reach at least 1 g/kg body weight, ideally 1.5 g/kg. Up to 2 g/kg in patients with immobility, systemic inflammation, or advanced age. In patients with significant deviations in BMI, weight correction should be applied when calculating protein needs, along with monitoring renal function [20].
Fat is the most energy-dense macronutrient, providing approximately 9 kcal per gram, and is well utilized in cancer patients, particularly when administered intravenously in those with significant weight loss. In patients with insulin resistance or type 2 diabetes, increasing fat intake can help reduce carbohydrate load. While healthy individuals are advised to consume 25–30% of total energy from fat, cancer patients with significant weight loss may benefit from fat intake of up to 40% of total energy [20]. Fatty acids differ in their metabolic effects depending on chain length and saturation; thus, in clinical nutrition, fat type not only contributes energy but also modulates inflammation and metabolism.
Carbohydrates primarily serve as an energy source, without providing essential nutrients. However, their absence may induce gluconeogenesis, leading to protein loss. In indigestible form – fiber, carbohydrates act as prebiotics that support microbiome diversity and promote healthy gastrointestinal transit. Carbohydrate intake should be gradual to ensure proper glucose utilization and to prevent hyperglycemia above 10 mmol/L, which is metabolically unfavorable. Hyperglycemia impairs immune function, increases infection risk, promotes oxidative stress, and has been linked to higher morbidity and mortality in critically ill patients. In healthy individuals, 45–60% of energy intake should come from carbohydrates. In cancer patients – particularly those with insulin resistance – this percentage should be reduced in favor of healthy fats, potentially to a balanced 1 : 1 ratio, meaning approximately 40% of energy from carbohydrates [24].
Nutritional disorders and their relation to HSCT
Malnutrition
Malnutrition is defined as a deficiency of energy stores, proteins and nutrients, with a negative impact on the patient‘s organ function and clinical status, such as reduced wound healing, impaired immunity, reduced muscle strength and overall functional status of the patient. Malnutrition includes the categories: disease-associated malnutrition with or without inflammation and non-disease-associated malnutrition, such as that associated with starvation. Sarcopenia and frailty has been included in a separate group of disorders frequently associated with malnutrition [25].
Sarcopenia
Sarcopenia is defined by the European Working Group on Sarcopenia in Older People (EWSOP2) as a syndrome characterized by progressive, generalized muscle disease associated with an increased risk of health complications such as falls, fractures, functional disability, etc. In sarcopenia, there is a deterioration in the quality of muscle mass associated with its loss. Primary sarcopenia is most often encountered in the aging process, preceded by a stage of frailty. Secondary sarcopenia is caused by pathological mechanisms and can be associated with disease, with reduced physical activity, with a deficiency of proteins in the diet. Muscle mass can be determined by direct precision methods such as dual X-ray absorptiometry (DXA) or imaging examinations by computed tomography (CT) or magnetic resonance imaging (MRI). These methods are among the most accurate and are considered as reference methods, but they are also costly. An option is to examine body composition on the basis of a single CT scan from reference sites, e. g. at the level of the 3rd lumbar vertebra (L3) [20]. Indirect non-invasive methods such as bioelectrical impedance analysis (BIA) are more commonly used and more affordable [26]. Overweight/obese patients with chronic or acute illness, trauma, or unbalanced diets with high energy intake and nutrient deficiencies may acquire malnutrition. Similarly, sarcopenic obesity, due to intense catabolism of muscle mass in inflammation, trauma, with or without patient inactivity [27]. A higher proportion of visceral fat and the occurrence of metabolic syndrome associated with higher inflammatory activity were observed in patients after allogeneic transplantation. Laboratory findings include higher CRP, leptin, and adiponectin decrease. Leptin increases with proportional adipose tissue representation and modifies T regulatory lymphocytes, increasing the risk of GVHD [28]. Patients who have sarcopenia before HSCT have increased risk of longer hospitalizations, worsened 2‐year overall survival, and increased risk of death because of infection or organ failure [29]. Another study showed, that sarcopenia during HSCT was affected by oral caloric intake during the preparation regimen and after transplantation [30].
Micronutrient disorders
The recommended daily allowance of nutrients is set for a healthy population and may not always meet the needs of an individual with a disease. Individual needs vary; micronutrient levels are not routinely tested. Specific deficiencies can have dramatic consequences, e. g., vitamin D deficiency can lead to osteoporosis, beri-beri or Wernicke-Korsakov syndrome caused by thiamine depletion. Micronutrient deficiencies can also lead to less pronounced problems that are not often thought of, such as poor wound healing, increased susceptibility to infection [31,32].
Patients with HSCT have impaired absorption of vitamins and trace elements, which may remain latent, unrecognized, but limiting the effect of nutritional intervention. Some standard parenteral nutrition formulations may not contain vitamins and minerals, and therefore it is necessary to supplement them according to clinical guidelines. which usually does not contain vitamins and trace elements and needs to be supplemented [20]. With stress metabolism, the deficiency of vitamins B and C develops in just a few days because of limited stores in the body. These vitamins have an important role for the successful effect of nutritional support. Manifestations of deficiency include stomatitis, cheilitis, glossitis, and psychological irritability, which are easily missed in addition to the complications of the transplantation itself. This chapter focuses on the deficiency of clinically relevant micronutrients.
Thiamine, or vitamin B1, deficiency of which may develop within 2 weeks in critically ill patients despite substitution with normal doses, possibly earlier in malnutrition patients. It can manifest as heart failure, peripheral neuropathy, lactic acidosis and is involved in the development of the ‘refeeding’ syndrome, when it needs to be replaced in high doses [33,34].
In adult patients, zinc deficiency at the time of transplant onset has been described in almost half of patients. During transplantation, zinc deficiency developes with parenteral nutrition, due to increased urinary excretion. Further depletion occurs with diarrhoea, GIT disorders, use of certain drugs (penicillamine, thiazides) and increased zinc requirements for bone marrow regeneration and infectious complications [35].
In addition to bone metabolism, vitamin D is involved in reducing pro-inflammatory activity and cytokines in the body, differentiation of immune cells, blocking the proliferation of allogeneic T-lymphocytes. Because of its immunomodulatory effect, its deficiency is associated with a higher incidence of autoimmune and inflammatory diseases [36]. Some earlier studies have shown that low vitamin D levels increase the risk of GVHD, cytomegalovirus (CMV) infections, and reduce overall survival after HSCT. However, results vary. In a 2013 US study of 250 allogeneic transplant patients, low vitamin D levels (< 30 ng/mL) at day 100 post HSCT were associated with significantly higher rates of bacterial infections, intensive care unit admissions and pulmonary consolidations, but not overall infection rates. In contrast to other studies, vitamin D levels did not affect the incidence of acute and chronic GVHD. Pre-transplant levels had no effect on mortality and disease recurrence, but low levels at day 100 significantly increased the risk [37]. In contrast, a more recent 2019 retrospective study with 316 enrolled allogeneic HSCT patients reported a higher incidence of severe chronic GVHD in patients with vitamin D deficiency. There was no correlation between more frequent infections, length of hospital stay, or neutrophil attachment. A lower risk of disease relapse was found in deficient patients, which the authors attributed to a possible effect of GVHD [38]. However, the correlation between the incidence of acute or chronic GVHD with vitamin D deficiency was not confirmed by a meta-analysis including 1335 patients from 2020 [39]. In allogeneic transplantation, vitamin D could change the immune response from pro-inflammatory to more tolerant immunity [40]. Its effect on immunity cannot be refuted, but further prospective studies are needed to properly understand its effect in modifying the course of transplantation and immunotherapy. Deficiency is common in HSCT patients, most commonly due to limited sun exposure, malabsorption, impaired renal and hepatic function, medications such as corticosteroids, anticonvulsants, immunosuppressants that increase vitamin D catabolism.
Calcium is an essential mineral that plays a role in numerous physiological processes, including bone metabolism, neuromuscular signaling, blood coagulation, and cellular signaling. One of the main causes of calcium metabolism disorders in the post-transplant population is long-term corticosteroid therapy, which is a part of treatment for both acute and chronic forms of GVHD. Glucocorticoids increase bone resorption and reduce intestinal calcium absorption, leading to a negative calcium balance and accelerated bone loss. Additionally, GVHD itself may contribute to calcium malabsorption due to damage to the intestinal mucosa [16].
Patients after HSCT are at high risk of developing osteopenia and osteoporosis, which are often asymptomatic until a pathological fracture occurs – most commonly involving the vertebrae, pelvis, or proximal femur. Studies have shown that 50–70% of patients after allogeneic HSCT experience reduced bone mineral density, with the highest risk occurring during the first year [41,42]. Contributing factors include physical inactivity, malnutrition, vitamin D deficiency, and hypoestrogenic or hypogonadal states. Therefore, calcium levels should be carefully monitored and supplemented, particularly in combination with vitamin D, which enhances its intestinal absorption. According to recommendations from expert organizations (e. g., EBMT and ESPEN), bone mineral density via DXA scan should be regularly assessed in high-risk patients, and preventive measures should be considered, including calcium and vitamin supplementation, hormone replacement therapy, or administration of bisphosphonates [1,20].
Refeeding syndrome
It is characterized by a severe disturbance in the body‘s electrolyte and fluid balance, which occurs when nutritional support is rapidly initiated in malnourished patients. Clinical symptoms may include fluid retention with peripheral edema, heart failure, arrhythmias, metabolic acidosis, respiratory insufficiency, delirium, encephalopathy, and other severe organ dysfunction. It usually occurs the first 4 days after initiation of nutritional support. Laboratory hypophosphatemia develops, which is responsible for most of the symptoms, and may also be associated with hypokalemia, hypomagnesemia, hypocalcemia. Diagnostic criteria include fluid imbalance, impaired glucose metabolism, hyperlactatemia, vitamin B1 deficiency, and most commonly electrolyte deficiency [43]. In at-risk patients, nutritional support should be initiated gradually, initially up to 50% of calculated caloric intake with escalation to full doses over 4–7 days. Careful monitoring of the condition is also important, and when symptoms begin, reduction of energy intake, especially glucose, B vitamin replacement, with th most important vitamin – thiamine and electrolytes, monitoring of fluid balance [44].
Nutritional screening methods
According to the recommendations, every patient should undergo a nutritional screening before HSCT at the time of preparation for transplantation. For example, according to the Brazilian Transplant Group: if the patient has a higher risk of malnutrition, he/she should undergo follow-up examinations at intervals not exceeding 15 days; if he/she does not have a risk of malnutrition, at intervals up to 30 days. After admission to the transplant unit, a nutritional status assessment should be performed within 48 hours and every 7 days thereafter until discharge, possibly more frequently if the patient‘s condition requires it. For example, nutritional risk assessment within 24 hours of admission is a requirement for quality accreditation by the Joint Commission International (JCI) [45]. International expert groups such as ESPEN recommend that screening for malnutrition should be initiated prior to transplantation. Precise methods of determination are not defined. Among the validated screening methods, the Nutritional Risk Screening (NRS 2002), Malnutrition Universal Screening Tool (MUST), Malnutrition Screening Tool (MST), Mini Nutritional Assessment (MNA), Subjective Global Assessment (SGA) and Patient-Generated SGA (PG-SGA) questionnaires are used. For practicality, the NRS 2002 questionnaire is the most commonly used, in line with the recommendations of the EBMT [1]. This method is suitable for hospitalized patients and has been developed using evidence-based medicine – analysis of randomized control trials. The NRS 2002 screening is divided into an initial and a final assessment. If the answer to any of the questions in the initial screening is “YES,” the final questionnaire must be completed. Every patient undergoing HSCT proceeds directly to the final screening, as the sub-question regarding the presence of a severe illness is answered affirmatively. The final questionnaire takes into account age, BMI, changes in food intake over the past week, the severity of the oncological disease – which reflects the level of metabolic stress and its impact on nutritional status – and weight loss over the past three months. A score of 3 or more points indicates a nutritional risk [46]. The identification of an increased risk of malnutrition using a screening tool does not provide sufficient information to develop a comprehensive nutritional plan. ESPEN recommends a subsequent, more detailed and objective assessment to guide intervention. This includes a quantitative evaluation of food intake, muscle mass, symptoms and their impact on eating, physical activity, body composition, and the severity of any systemic inflammation. This assessment should be performed regularly [47]. Another score system – Controlling Nutritional Status (CONUT) – emerged as the most effective nutritional scoring system for predicting mortality in allo-HSCT patients [48].
Eating complications in patients with HSCT
One of the determinants of nutritional deterioration and the overall course of transplantation is the toxicity of the preparative regimen. Cytotoxic drugs act on rapidly dividing cells of GIT and cause discomforts such as: mucositis, xerostomia, dysgeusia, dysphagia, dysphagia, odynophagia, nausea and vomiting, constipation, anorexia, taste changes. The epithelial cells of the oral cavity are the first to be affected because of their rapid proliferation, which directly and most significantly affects the patient‘s food intake [49]. It has been described that symptoms can persist for up to 3 months after HSCT, and if the patient undergoes nutritional counselling prior to HSCT, better tolerance of treatment and fewer side effects are present [50]. Other factors of impaired GIT function are infectious complications (herpes simplex virus, cytomegalovirus, varicella zoster virus, mycoses, clostridial infection), GVHD, psychological factors.
Xerostomia
Subjective sensation of dryness in the oral cavity caused by lack of saliva, subjectively perceived as discomfort in the mouth – pain, burning, difficulty swallowing. Saliva is composed of water, proteins and electrolytes, and is involved in speaking, swallowing, taste production, antimicrobial function, irrigation and protection of the teeth and mucosa of the upper digestive tract. Their deficiency/dysfunction can adversely affect oral mucositis. The prevalence of xerostomia in HSCT recipients is high in comparison to the general population and can last during the first year post-HSCT [51]. According to an analysis of the saliva composition of HSCT patients, a reactive inflammatory response was demonstrated early in the HSCT phase, which persisted for months. Day 7 of transplantation saw a decrease in secretory immunoglobulin A (IgA) and antioxidant levels, with recovery by 6 months after HSCT. Conversely, salivary antimicrobials and proinflammatory cytokines increased and remained elevated 6 months after HSCT [52].
Nutritional recommendations
Frequent sipping of small amounts of fluids, including during meals; stimulation of salivation by adding mint flavoring, lemon drops, acidic foods, candies, or papaya enzymes; preparing meals in a more liquid form, reducing caffeine intake, incorporating artificial saliva products such as mouth rinses or sprays [53].
Odynophagia
Painful swallowing with typical chest pain/burning caused by inflammatory erosions or ulcerations of the larynx/pharynx, of infectious etiology (herpes virus, candida, others), in acute GVHD, in reflux, drug-induced (tetracyclines, potassium), or in mucositis after chemotherapy/radiotherapy.
Nutritional recommendations
Administer analgesic treatment before meals; avoid irritating foods such as carbonated drinks, acidic foods, very dry or tough foods; avoid foods that are excessively hot or cold; follow a light, more liquid, and less spicy diet, with additional nutritional support depending on the severity of the condition [53].
Dysgeusia
Abnormal, often unpleasant perception of taste due to impaired taste bud function. Bitter taste is the first to be affected, then sweetness, and last the perception of salty taste. Patients often complain of a metallic taste, especially if a platinum-based chemotherapeutic is in treatment [45].
Nutritional recommendations
Enhance flavor perception using spices and lemon; avoid overly hot foods; avoid red meat and iron-rich foods, as they may worsen metallic taste perception [24].
Diarrhoea
In HSCT patients, it most commonly occurs as a result of damage to the intestinal mucosa by radiotherapy or chemotherapy, overuse of antibiotics, clostridial or other infectious colitis, acute GVHD, drug-induced damage (e. g. mycophenolate mofetil), as a result of neutropenic enterocolitis [54].
Nutritional recommendations
Reduce the intake of lactose (yogurt is often well tolerated; alternatively, use lactose-free dairy products), sucrose, sorbitol, fatty foods, caffeine, spicy and sweet foods, and foods that are excessively hot or cold, as they may stimulate peristalsis. Avoid foods with laxative effects or high fiber content. Rehydration should preferably be done with mineral solutions. Smaller, more frequent meals are recommended. Resting in a reclined position after meals is also advised. In the case of more severe diarrhea, it is advisable to rest the bowel for several hours by avoiding solid food and consuming only fluids, then gradually reintroduce a bland diet. If the diarrhea is prolonged or severe, it is often accompanied by dehydration and nutrient malabsorption, and therefore parenteral support is necessary [55].
Constipation
It does not cause nutritional losses itself, but is an unpleasant symptom for the patient, which can lead to other symptoms, e. g. loss of appetite, abdominal pain. Also, opioids, used in the treatment of pain and dyspnea, have this adverse effect. Their receptors are found diffusely in GIT, they also act on central and peripheral receptors of the nervous system and cause inhibition of gastric, biliary and pancreatic secretion, reduce peristalsis and increase segment contractility. These effects cause longer contact of the intestinal contents with the mucosa and therefore higher absorption of water and electrolytes, thickening of the contents. Similarly, antiemetics from the setron group and reduced patient mobility may contribute to slowing peristalsis.
Nutritional recommendation
Increase fluid intake, as well as soluble and insoluble fiber, intake of vegetables and fruits, wholegrain bread, legumes, and juices with laxative properties (orange, papaya, prune). Physical activity should also be increased. In the case of severe constipation, the use of laxatives or enemas is appropriate [24].
Mucositis
This is a very common complication of HSCT occurring in up to 80% of patients, which affects the course of hospitalization, worsens the quality of life of patients, is associated with a higher incidence of infections, and increases the economic burden of the procedure. Higher administration of anti-infectives, parenteral nutrition, opioids, and prolonged hospitalization in patients with mucositis has been described [56,57]. Clinically, we know two symptom patterns, oral mucositis, which is characterized by erythematous to ulcerative lesions with edema and soreness in the oral cavity affecting speaking and eating. Another form is gastrointestinal mucositis, which affects the entire GIT and can manifest as anorexia, nausea, vomiting, diarrhea, abdominal pain. We also know the division into direct mucositis, caused by cytotoxic treatment, for example caused by the chemotherapeutic drugs methotrexate and etoposide, which are excreted in saliva, and indirect mucositis, which occurs due to infection with gram-negative bacteria or mycosis. In patients with HSCT, mucositis most often developed between days 10-21 after chemotherapy administration [57]. According to a multicenter EBMT study of 197 patients with autologous HSCT and conditioning regimens BEAM (carmustine + etoposide + cytarabine + melphalan) and high-dose melphalan, severe mucositis occurred in 44% of patients. The median peak of discomfort was experienced on day 12, at the time of the onset of neutrophil recovery [58].
Prevention and treatment
It is not clearly defined. It is important to maintain good oral hygiene and dental health. Antibiotic prophylaxis did not reduce the colonization of microorganisms in the oral cavity, which is a key aspect of the onset of mucositis, and has not been proven effective [59]. Cryotherapy has been proved to be effective in preventing oral mucositis and that it may suppress the development of dysgeusia in patients, although further studies are needed. There were used, for example, flavored ice cubes, which the patient places in his mouth 30 minutes before starting the infusion and sucks on them for at least the entire duration of the infusion. No differences in efficacy were found between 2 and 6 hours of application, and no serious adverse effects of the procedure were reported. This is a simple method of prevention that utilizes vasoconstriction of the oral mucosa and a reduction in cell metabolism during peak drug concentrations in the blood, according to the guidelines of the Multinational Association of Supportive Care in Cancer and International Society of Oral Oncology (MASCC/ISOO). Cryotherapy is recommended for patients undergoing autologous transplantation and high-dose melphalan [60]. The use of photomodulation (laser) therapy, which uses red and infrared radiation to reduce inflammation and promote regeneration, also appears promising. According to a meta-analysis of 396 patients undergoing HSCT, photobiomodulation therapy reduced the incidence of severe oral mucositis, with a protective factor 20% higher than in the control group [61]. The limiting factors are its higher price and availability. Palifermin – a recombinant human keratinocyte growth factor – is recommended by the MASCC/ISOO group for reducing the incidence of severe oral mucositis in patients undergoing autologous transplantation and a preparatory regimen in combination with radiotherapy. It has also been approved for use in patients undergoing autologous transplantation with a preparatory regimen at risk of developing severe mucositis. Disadvantages include the price and, according to meta-analyses, a mild effect on reducing the risk of mucositis in autologous transplantation and ineffectiveness in allogeneic transplantation [62].
Anorexia
Defined as early satiety or loss of appetite, the etiology of which is not fully understood, contributed to adverse effects of treatment, infections, the cancer itself, depression, and changes in food preferences. It occurs in 40% of cancer patients. Appetite is regulated by cytokines and hormones. For example, neuropeptide Y and ghrelin are orexigenic hormones, and reduced levels have been found in animal models with tumors. Melanocortin is elevated in cancer patients and has anorexigenic activity. Similarly, some cytokines cause loss of appetite, such as TNF-a, interferon gamma, interleukin 1 and 6, which are secreted by tumors and during inflammation. The occurrence of anorexia is described in transplant patients most frequently between the 2nd and 3rd week after transplantation [63]. In long-term follow-up of patients after autologous and allogeneic transplantation, 65% still reported loss of appetite on day 50, with low compliance with recommended nutritional advice [64].
Nutritional recommendations
Eat smaller portions more frequently and slowly; enhance food flavor similarly to approaches used for dysgeusia; drink fluids preferably between main meals; increase the caloric and protein content of meals; add high-calorie snacks and nutritional supplements; provide psychological support and adequate patient education, consider gestagen hormone therapy, prokinetics, corticosteroid therapy for short period of time [24].
Nutritional support for transplant patients
An overview of the studies conducted is presented in Tab. 1.

transplantation, PN – parenteral nutrition, QOL – quality of life, TGF-β2 (TE-OPF) – oral polymeric formulation enriched with trans
forming growth factor β2
The main goal of nutritional support is to bridge the period of insufficient food intake and prevent unwanted weight loss with its negative effects. Nutritional support should be initiated in malnourished patients prior to HSCT to improve survival [72]. After determining the BEV, the value is multiplied by a disease correction factor to obtain the estimated total energy requirement (e. g., 1.5 for a patient with HSCT, 1.7 for a patient with GVHD GIT). The goal of nutrition set up this way is to keep the patient‘s weight stable, and if it needs to be increased, energy intake is increased by 5 kcal/kg/day, or disease correction factor by 0.2. Enteral (EN) or parenteral nutrition (PN) should be initiated in the case of allogeneic transplantation if oral intake is less than 60% for 3 consecutive days, or earlier in malnourished patients. It can be discontinued if the patient has been receiving more than 50% of oral nutrition for 3 consecutive days, followed by supplementation with oral nutritional supplements. Along with parenteral nutrition, vitamin and trace element supplementation according to the recommended daily doses should not be forgotten. In the case of GVHD, vitamin and trace element deficiencies are common, therefore regular monitoring of their levels is also recommended [24,73].
Several expert groups agree on standard vitamin D supplementation in higher doses – EBMT or American Association of Blood Banks (AABB) from the start of transplantation. Other recommendations (AABB) include increased zinc supplementation for diarrhea, routine administration of folic acid to support hematopoiesis, and adequate thiamine intake. In addition, increased vitamin C administration is recommended for critically ill patients, although it may enhance iron absorption and thereby potentially contribute to iron overload in polytransfused patients, but there is no clear consensus about monitoring and practise quidelines in HSCT patients so far. The selenium supplementation should not be forgotten for long-term parenteral nutrition. Intravenous preparations that are available vary in their vitamin and trace element content. For patients who have undergone transplantation and are on total parenteral nutrition, it is advisable to choose preparations with lower or no iron content and higher amounts of vitamin C, thiamine, vitamin D, and zinc [74]. Due to the higher risk of infections in PV, stricter monitoring of blood glucose levels is required, maintaining them below 8 mmol/l. Glucose intake in PV should not exceed 0.24 g/kg/hour. The need for amino acids in PN or proteins in EN is high in the early phase of HSCT: 1.5–1.8 g/kg, and in GVHD of GIT or malnourished patients up to 1.8–2.5 g/kg [1]. Special substitution with glutamine is not recommended in either PV or EV, as the results of studies have been controversial [75].
Enteral versus parenteral nutrition
In routine practice, PV is preferred over EN due to concerns about tolerance of nasogastric tubes, especially in patients with vomiting and severe mucositis with diarrhea. However, EN offers the advantages of supporting the intestinal mucosa and mucosal barrier, thereby reducing the risk of bacterial translocation. Contraindications for EN include severe mucositis, vomiting and diarrhea of grade III–IV unresponsive to treatment, bleeding or obstruction of the GI tract, short bowel syndrome, and typhlitis. PN administration causes intestinal mucosal atrophy and disruption of the gastrointestinal immunity. Reduced intestinal blood flow, decreased mucosal white blood cell count, and changes in mucosal IgA secretion have been observed [76]. This condition disrupts the mucosal barrier and causes dysbiosis, more frequent colonization of the intestine by pathogenic bacteria, exudative enteropathy with higher amino acid losses. A relative contraindication to the administration of parenteral nutrition – or at least a situation requiring increased caution – includes the following: fluid overload, cardiac failure, lipid metabolism disorders, and decompensated diabetes.
According to an analysis of 121 patients after myeloablative therapy, patients with EV had lower early mortality and incidence of acute GVHD grade III–IV than patients with PN [77]. According to French authors Guize et al., 56 patients after allogeneic HSCT were administered EN through a thin nasogastric tube in half of the patients according to their preferences. EN was tolerated for 14 days by 57% of patients. No differences in nutritional status, incidence of mucositis or GVHD were found between the different types of nutrition, but patients with PN had a significantly higher incidence of fever, empirical antifungal treatment and a more frequent need for intensive care. The authors of the study recommend earlier insertion of a nasogastric tube, immediately after graft administration and before the onset of mucositis, to improve tolerance. The results of the studies suggest that, if EN nutrition is tolerated in allogeneic transplantation, it offers advantages for the patient [78].
A retrospective study of 228 pediatric patients with allogeneic HSCT showed, that patients with PN experienced severe mucositis, more frequent sinusoidal obstruction syndrome and acute GVHD in comparison with EN administered with nasogastric tube. There were no statistically significant differences in chronic GVHD, bacteremia, and patients‘ survival between both groups [79]. On the other hand, a retrospective study of 526 patients with HSCT showed that PN effectively mitigated weight loss on days 10 and 14 and the day before discharge, while also improving levels of albumin and prealbumin. In addition, there were no significant differences in bloodstream infestions incidence or liver function between the non-PN and PN groups. Furthermore, the PN group experienced a shorter length of hospital stay and lower rates of unexpected rehospitalization. These findings support the use of nutritional interventions in hematologic malignancy patients prior to transplantation [80].
In autologous transplantation, where we expect shorter duration of mucositis and limited oral intake, early nutritional intervention with high-protein oral nutritional supplements should be the basis, where the content of anti-inflammatory n-3 polyunsaturated fatty acids may be beneficial, while symptomatic treatment of feeding difficulties is administered. The options for EN are better in patients with autologous transplantation. Unless contraindicated, it should be preferred over PN. A retrospective study by American authors evaluated the effect of PN in a group of 112 patients with multiple myeloma who received short-term PN within 10–19 days of autologous HCST. Compared to the subgroup without PN, more frequent hyperglycemia, delayed graft engraftment, higher incidence of febrile neutropenia, and longer hospitalization were observed. The authors consider that the worsening of HSCT was caused by the effect of hyperglycemia after PN [81]. Another randomized study with 36 patients undergoing autologous HSCT investigated the effectiveness of EN versus PN. No significance in any of the medical or nutritional parameters between the two groups was found between groups [82].
mized controlled trial
Neutropenic diet
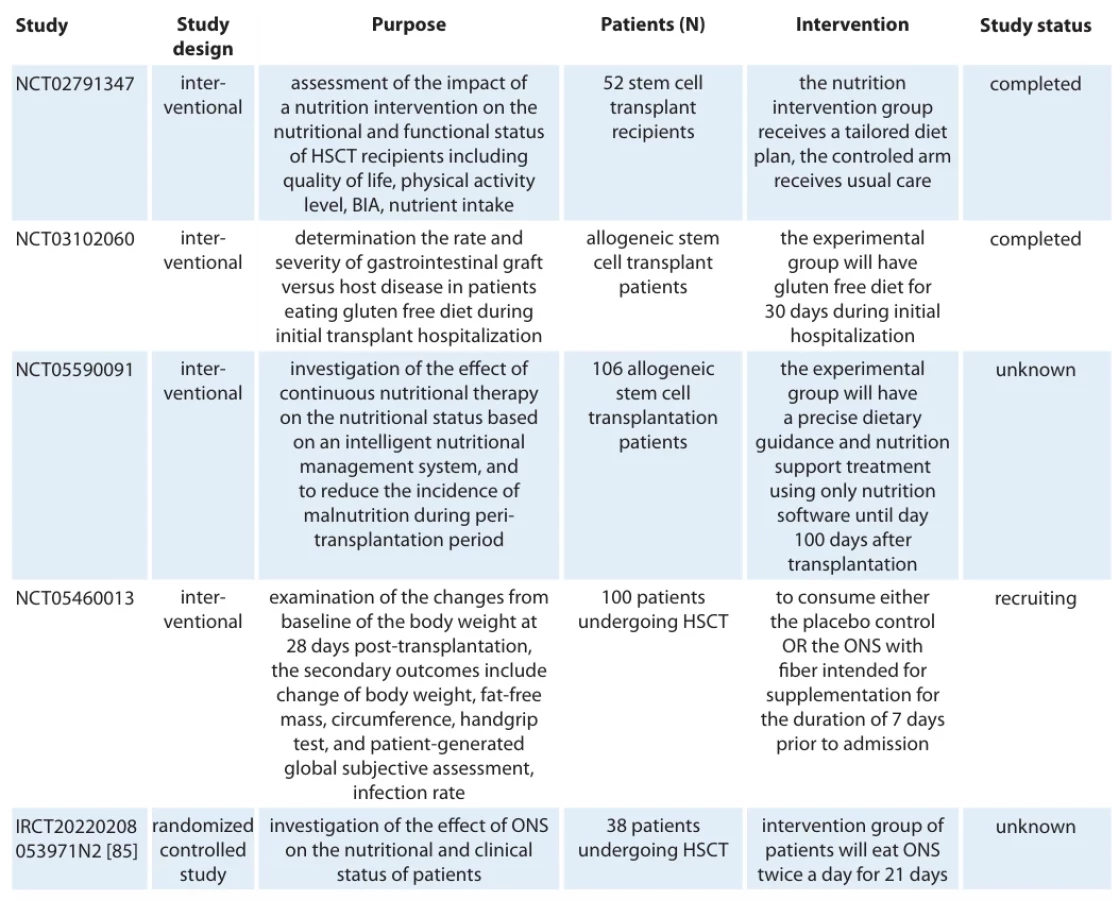
The most common source of bacterial infection in HSCT is considered to be chemotherapy-induced disruption of the gastrointestinal mucosa. Antibiotic resistance is becoming an alarming global issue, with the World Health Organization ranking it among the top ten global public health threats in 2019. Several studies have described the contamination of raw vegetables and fruit with gram-resistant bacteria (mainly producing broad-spectrum beta-lactamases ESBL, carbapenemases, enterobacteria producing cephalosporinases and colistin-resistant bacteria) [83]. When consumed, there is a concern, especially in immunocompromised patients, of colonisation of the intestine by multi-resistant strains, possibly even spreading genes for antibiotic resistance to the rest of the intestinal microbiome, translocation of bacteria into the bloodstream and the development of serious infections. Therefore, many transplant centers use so-called neutropenic diets with varying degrees of restriction to ensure that the diet is microbiologically poor during neutropenia. On the other hand, studies on the positive effects of a healthy gut microbiome in patients undergoing bone marrow transplantation are coming to the fore. It has been shown that reduced gut bacterial diversity and heavy pre-treatment with antibiotics are associated with a higher incidence of GVHD and higher patient mortality [84] Therefore, a theory is emerging that supporting a healthy gut microbiome could suppress the proliferation of resistant bacteria and positively stimulate the immune system in fighting infections during transplantation. Further studies are needed to draw a clear conclusion on whether a neutropenic diet is beneficial for transplant patients. One of the few published studies is a retrospective observational study by Trifilio et al. involving 726 patients with autologous and allogeneic bone marrow transplantation, which compared a neutropenic diet and a regular hospital diet during neutropenia because the hospital changed its dietary strategy. The neutropenic diet did not include fresh vegetables and fruits, raw and undercooked foods such as cheese, meat, grains, fish, seeds, and unpasteurized dairy products. Well-washed fruits and vegetables were allowed in the hospital diet, except for raw tomatoes; other restrictions remained similar. The authors of the study describe a higher incidence of microbiologically confirmed infections in patients on a neutropenic diet (P < 0.027), which was further accentuated after recovery in the blood count (P < 0.008) when they returned to the hospital diet. There was a trend toward more frequent diarrhea, urinary tract infections, and GIT infections caused by vancomycin-resistant enterococci, enterobacteria, and Clostridium difficile in patients on a neutropenic diet. The diet had no effect on overall mortality or length of hospital stay. Patients who tried both diets found the regular hospital diet to be more natural and easier to maintain energy intake [84]. Another meta-analysis, which included studies with a low-microbial diet in cancer patients, similarly failed to demonstrate its benefit in reducing the incidence of infections [84]. According to the EBMT working group, there is currently no evidence that a neutropenic diet is effective in preventing infections and reducing mortality. Similar to the Food and Drug Administration, it recommends increased hand hygiene and safe food handling [1]. Ongoing clinical trials assessing nutritional interventions in HSCT patients are presented in Tab. 2.
Conclusions and future directions
Nutritional management plays a pivotal role in the success of HSCT, influencing both early and long-term outcomes. Routine assessment of nutritional status, ideally including body composition analysis, is essential, as standard measures such as BMI may fail to detect sarcopenia or hidden malnutrition. Energy and protein requirements are elevated during HSCT, particularly in patients with active inflammation or GVHD, and timely intervention is associated with improved clinical outcomes and reduced transplant-related mortality. Enteral nutrition is preferred over parenteral support when feasible, given its beneficial effects on gut integrity and immune function, while parenteral nutrition should be reserved for patients unsuitable for oral or enteral feeding. Micronutrient deficiencies are common and often underestimated; supplementation with vitamins D, B1, zinc, selenium, and others is essential and should be tailored based on clinical status and treatment-related losses, and should always accompany the administration of parenteral nutrition. Nutritional complications such as mucositis, diarrhea, anorexia, and dysgeusia require individualized management to preserve nutritional intake and minimize further deterioration.
Recent studies have shown that early and structured nutritional interventions can improve quality of life, reduce infection rates, shorten hospitalization, and support better immune recovery in HSCT recipients. Furthermore, the traditionally recommended neutropenic diet has not demonstrated a clear benefit in infection prevention and may negatively affect dietary diversity and microbiome health. Therefore, current recommendations emphasize safe food handling and hygiene over restrictive dietary practices. Overall, nutritional care should be an integral, individualized component of HSCT protocols, involving clinical nutrition specialists as part of the multidisciplinary transplant team.
Supported by Vega agency, grant No. 2/0069/22.
Sources
1. Casirati A, Salcedo I, Cereda E et al. The European Society for Blood and Marrow Transplantation (EBMT) roadmap and perspectives to improve nutritional care in patients undergoing hematopoietic stem cell transplantation on behalf of the Cellular Therapy and Immunobiology Working Party (CTIWP) and the Nurses Group (NG) of the EBMT. Bone Marrow Transplant 2023; 58 (9): 965–972. doi: 10.1038/s41409-023-02018-z.
2. Sorror ML, Maris MB, Storb R et al. Hematopoietic cell transplantation (HCT) -specific comorbidity index: a new tool for risk assessment before allogeneic HCT. Blood 2005; 106 (8): 2912–2919. doi: 10.1182/blood-2005-05-2004.
3. Liu P, Zhang ZF, Cai JJ et al. NRS2002 assesses nutritional status of leukemia patients undergoing hematopoietic stem cell transplantation. Chin J Cancer Res 2012; 24 (4): 299–303. doi: 10.3978/j.issn.1000-9604.2012.09.01.
4. Mendes J, Alves P, Amaral T. Comparison of nutritional status assessment parameters in predicting length of hospital stay in cancer patients. Clin Nutr 2014; 33 (3): 466–470. doi: 10.1016/j.clnu.2013.06.016.
5. Yucel OK, Vural E, Alhan N et al. Lower body mass index and prognostic nutritional index are associated with poor posttransplant outcomes in lymphoma patients undergoing autologous stem cell transplantation. Oncology 2023; 101 (11): 753–764. doi: 10.1159/000531576.
6. Navarro WH, Loberiza FR, Bajorunaite R et al. Effect of body mass index on mortality of patients with lymphoma undergoing autologous hematopoietic cell transplantation. Biol Blood Marrow Transplant 2006; 12 (5): 541–551. doi: 10.1016/j.bbmt.2005.12.033.
7. Tarella C, Caracciolo D, Gavarotti P et al. Overweight as an adverse prognostic factor for non-Hodgkin‘s lymphoma patients receiving high-dose chemotherapy and autograft. Bone Marrow Transplant 2000; 26 (11): 1185–1191. doi: 10.1038/sj.bmt.1702692.
8. Meloni G, Proia A, Capria S et al. Obesity and autologous stem cell transplantation in acute myeloid leukemia. Bone Marrow Transplant 2001; 28 (4): 365–367. doi: 10.1038/sj.bmt.1703145.
9. Vogl DT, Wang T, Pérez WS et al. Effect of obesity on outcomes after autologous hematopoietic stem cell transplantation for multiple myeloma. Biol Blood Marrow Transplant 2011; 17 (12): 1765–1774. doi: 10.1016/j.bbmt.2011.05.005.
10. Haddadin M, Obedat A, Al-Bitar F et al. Association between malnutrition and inpatient mortality in Hematopoietic Stem Cell Transplant (HSCT) population: a Nationwide Inpatient Sample (NIS) database analysis. Blood 2024; 144 (Suppl 1): 2125–2125.
11. Baumgartner A, Bargetzi A, Zueger N et al. Revisiting nutritional support for allogeneic hematologic stem cell transplantation-a systematic review. Bone Marrow Transplant 2017; 52 (4): 506–513. doi: 10.1038/bmt.2016.310.
12. Nakao M, Chihara D, Niimi A et al. Impact of being overweight on outcomes of hematopoietic SCT: a meta-analysis. Bone Marrow Transplant 2014; 49 (1): 66–72. doi: 10.1038/bmt.2013.128.
13. Nikolousis E, Nagra S, Paneesha S et al. Allogeneic transplant outcomes are not affected by Body Mass Index (BMI) in patients with haematological malignancies. Ann Hematol 2010; 89 (11): 1141–1145. doi: 10.1007/s00277-010-1001-6.
14. Doney K, McMillen K, Buono L et al. Impact of body mass index on outcomes of hematopoietic stem cell transplantation in adults. Biol Blood Marrow Transplant 2019; 25 (3): 613–620. doi: 10.1016/j.bbmt.2018.10.006.
15. Brauer D, Backhaus D, Pointner R et al. Nutritional status at diagnosis and pre-transplant weight loss impact outcomes of acute myeloid leukemia patients following allogeneic stem cell transplantation. Hemasphere 2021; 5 (3): e532. doi: 10.1097/HS9.0000000000000532.
16. Abasaeed R, Coldwell SE, Lloid ME et al. Chemosensory changes and quality of life in patients undergoing hematopoietic stem cell transplantation. Support Care Cancer 2018; 26 (10): 3553–3561. doi: 10.1007/s00520-018-4200-7.
17. Fuji S, Einsele H, Savani BN et al. Systematic nutritional support in allogeneic hematopoietic stem cell transplant recipients. Biol Blood Marrow Transplant 2015; 21 (10): 1707–1713. doi: 10.1016/j.bbmt.2015.07.003.
18. Nguyen TY, Batterham MJ, Edwards C. Comparison of resting energy expenditure between cancer subjects and healthy controls: a meta-analysis. Nutr Cancer 2016; 68 (3): 374–387. doi: 10.1080/01635581.2016.1153667.
19. Roza AM, Shizgal HM. The Harris Benedict equation reevaluated: resting energy requirements and the body cell mass. Am J Clin Nutr 1984; 40 (1): 168–182. doi: 10.1093/ajcn/40.1.168.
20. Muscaritoli M, Arends J, Bachmann P et al. ESPEN practical guideline: clinical nutrition in cancer. Clin Nutr 2021; 40 (5): 2898–2913. doi: 10.1016/j.clnu.2021.02.005.
21. Stobäus N, Müller MJ, Küpferling S et al. Low recent protein intake predicts cancer-related fatigue and increased mortality in patients with advanced tumor disease undergoing chemotherapy. Nutr Cancer 2015; 67 (5): 818–824. doi: 10.1080/01635581.2015.1040520.
22. Deutz NE, Safar A, Schutzler S et al. Muscle protein synthesis in cancer patients can be stimulated with a specially formulated medical food. Clin Nutr 2011; 30 (6): 759–768. doi: 10.1016/j.clnu.2011.05.008.
23. Ham DJ, Caldow MK, Lynch GS et al. Leucine as a treatment for muscle wasting: a critical review. Clin Nutr 2014; 33 (6): 937–945. doi: 10.1016/j.clnu.2014.09.016.
24. Tomíška M. Výživa onkologických pacientů. Praha: Mladá fronta 2018.
25. Cederholm T, Jensen GL. To create a consensus on malnutrition diagnostic criteria: a report from the Global Leadership Initiative on Malnutrition (GLIM) meeting at the ESPEN Congress 2016. Clin Nutr 2017; 36 (1): 7–10. doi: 10.1016/j.clnu.2016.12.001.
26. Farias CL, Campos DJ, Bonfin CM et al. Phase angle from BIA as a prognostic and nutritional status tool for children and adolescents undergoing hematopoietic stem cell transplantation. Clin Nutr 2013; 32 (3): 420–425. doi: 10.1016/j.clnu.2012.09.003.
27. Stenholm S, Harris TB, Rantanen T et al. Sarcopenic obesity: definition, cause and consequences. Curr Opin Clin Nutr Metab Care 2008; 11 (6): 693–700. doi: 10.1097/MCO.0b013e328312c37d.
28. Fuji S, Kim SW, Yoshimura K et al. Possible association between obesity and posttransplantation complications including infectious diseases and acute graft-versus-host disease. Biol Blood Marrow Transplant 2009; 15 (1): 73–82. doi: 10.1016/j.bbmt.2008.10.029.
29. Armenian SH, Xiao M, Berano Teh J et al. Impact of sarcopenia on adverse outcomes after allogeneic hematopoietic cell transplantation. J Natl Cancer Inst 2019; 111 (8): 837–844. doi: 10.1093/jnci/djy231.
30. Tanaka S, Imataki O, Kitaoka A et al. Clinical impact of sarcopenia and relevance of nutritional intake in patients before and after allogeneic hematopoietic stem cell transplantation. J Cancer Res Clin Oncol 2017; 143 (6): 1083–1092. doi: 10.1007/s00432-016-2336-8.
31. Tulchinsky TH. Micronutrient deficiency conditions: global health issues. Public Health Rev 2010; 32 (1): 243–255. doi: 10.1186/s40985-017-0071-6.
32. Gdynia HJ, Müller T, Sperfeld AD et al. Severe sensorimotor neuropathy after intake of highest dosages of vitamin B6. Neuromuscul Disord 2008; 18 (2): 156–158. doi: 10.1016/j.nmd.2007.09.009.
33. Isenberg-Grzeda E, Shen MJ, Alici Y et al. High rate of thiamine deficiency among inpatients with cancer referred for psychiatric consultation: results of a single site prevalence study. Psychooncology 2017; 26 (9): 1384–1389. doi: 10.1002/pon.4155.
34. Iimura Y, Andoh S, Kawamata T et al. Thiamine deficiency and neurological symptoms in patients with hematological cancer receiving chemotherapy: a retrospective analysis. J Neurosci Rural Pract 2021; 12 (4): 726–732. doi: 10.1055/s-0041-1735825.
35. Pereira A, Juliana S, Pivocari S et al. Zinc deficiency in patients adults undergoing to hematopoietic stem cell post-transplantation. Blood 2013; 122 (21): 5500. doi: 10.1182/blood.V122.21.5500.5500.
36. Athanassiou L, Mavragani CP, Koutsilieris M. The immunomodulatory properties of vitamin D. Mediterr J Rheumatol 2022; 33 (1): 7–13. doi: 10.31138/mjr.33.1.7.
37. Beebe K, Olsen J, Chang YH et al. Impact of vitamin D level pre and post allogeneic hematopoietic stem cell transplant. Blood 2013; 122 (21): 4616.
38. Bajwa RPS, Taylor K, Hoyt AR et al. Effects of vitamin D levels on outcomes after allogeneic hematopoietic stem cell transplantation in children. Biol Blood Marrow Transplant 2019; 25 (Suppl 3): S239–S240.
39. Chiengthong K, Cheungpasitporn W, Thongprayoon C et al. Vitamin D deficiency is not associated with graft versus host disease after hematopoietic stem cell transplantation: a meta-analysis. J Evid Based Med 2020; 13 (3): 183–191. doi: 10.1111/jebm.12383.
40. Macedo R, Pasin C, Ganetsky A et al. Vitamin D deficiency after allogeneic hematopoietic cell transplantation promotes T-cell activation and is inversely associated with an EZH2-ID3 signature. Transplant Cell Ther 2022; 28 (1): 18.e1–18.e10. doi: 10.1016/j.jtct.2021.09.017.
41. Yao S, McCarthy PL, Dunford LM et al. High prevalence of early-onset osteopenia/osteoporosis after allogeneic stem cell transplantation and improvement after bisphosphonate therapy. Bone Marrow Transplant 2008; 41 (4): 393–398. doi: 10.1038/sj.bmt.1705918.
42. Savani BN, Stratton P, Shenoy A et al. Increased risk of cervical dysplasia in long-term survivors of allogeneic stem cell transplantation – implications for screening and HPV vaccination. Biol Blood Marrow Transplant 2008; 14 (9): 1072–1075. doi: 10.1016/j.bbmt.2008.07.005.
43. Crook MA. Refeeding syndrome: problems with definition and management. Nutrition 2014; 30 (11–12): 1448–1455. doi: 10.1016/j.nut.2014.03.026.
44. Szeja N, Grosicki S. Refeeding syndrome in hematological cancer patients – current approach. Expert Rev Hematol 2020; 13 (3): 201–212. doi: 10.1080/17474086. 2020.1727738.
45. Barban JB, Simões BP, Moraes B et al. Brazilian nutritional consensus in hematopoietic stem cell transplantation: adults. Einstein (Sao Paulo) 2020; 18: AE4530. doi: 10.31744/einstein_journal/2020AE4530.
46. Kondrup J, Rasmussen HH, Hamberg O et al. Nutritional risk screening (NRS 2002): a new method based on an analysis of controlled clinical trials. Clin Nutr 2003; 22 (3): 321–336. doi: 10.1016/s0261-5614 (02) 00214-5.
47. August D, Huhmann M. a. s.P.E.N. clinical guidelines: nutrition support therapy during adult anticancer treatment and in hematopoietic cell transplantation. JPEN J Parenter Enteral Nutr 2009; 33 (5): 472–500. doi: 10.1177/0148607109341804.
48. Ozkan SG, Avci S, Urusak A et al. Which nutritional scoring system best predicts transplant outcomes in allogeneic stem cell recipients? A comparison of nutritional risk index, prognostic nutritional index, and controlling nutritional status. Sisli Etfal Hastan Tip Bul 2025; 59 (1): 64–75. doi: 10.14744/SEMB.2025.74050.
49. Šachlová M. Výživa onkologických pacientů. Klin Onkol 2003; 16 (2): 77–79.
50. Paiva MDEB, Gonçalves RCC, De Campos Baldin JJCM et al. Complicações orais decorrentes da terapia antineoplásica. Arq Odontol 2010; 46 (1): 48–55.
51. Bulthuis MS, van Gennip LLA, Bronkhorst EM et al. The effect of hematopoietic stem cell transplantation on patient-reported subjective oral dryness: a systematic review focusing on prevalence, severity and distress. Support Care Cancer 2023; 31 (8): 449. doi: 10.1007/s00520-023-07921-1.
52. van Leeuwen SJM, Potting CMJ, Huysmans M et al. Salivary changes before and after hematopoietic stem cell transplantation: a systematic review. Biol Blood Marrow Transplant 2019; 25 (6): 1055–1061. doi: 10.1016/j.bbmt.2019.01.026.
53. Burns LJ. Hematopoietic stem cell transplantation: a handbook for clinicians. 2015 [online]. Available from: https: //www.aabb.org/aabb-store/product/hematopoietic-stem-cell-transplantation-a-handbook-for-clinicians-2nd-edition---digital-13102581.
54. Castillo Almeida NE, Cichon CJ, Gomez CA. How I approach diarrhea in hematological transplant patients: a practical tool. Transplant Infect Dis 2023; 25 (Suppl 1): e14184. doi: 10.1111/tid.14184.
55. Barban JB, Simões BP, Moraes BDGC et al. Brazilian nutritional consensus in hematopoietic stem cell transplantation: adults. Einstein (Sao Paulo) 2020; 18: AE4530. doi: 10.31744/einstein_journal/2020AE4530.
56. Fanning SR, Rybicki L, Kalaycio M et al. Severe mucositis is associated with reduced survival after autologous stem cell transplantation for lymphoid malignancies. Br J Haematol 2006; 135 (3): 374–381. doi: 10.1111/j.1365-2141.2006.06323.x.
57. Singh V, Singh AK. Oral mucositis. Natl J Maxillofac Surg 2020; 11 (2): 159–168. doi: 10.4103/njms.NJMS_10_20.
58. McCann S, Schwenkglenks M, Bacon P et al. The prospective oral mucositis audit: relationship of severe oral mucositis with clinical and medical resource use outcomes in patients receiving high-dose melphalan or BEAM-conditioning chemotherapy and autologous SCT. Bone Marrow Transplant 2009; 43 (2): 141–147. doi: 10.1038/bmt.2008.299.
59. Lövenich H, Schütt-Gerowitt H, Keulertz C et al. Failure of anti-infective mouth rinses and concomitant antibiotic prophylaxis to decrease oral mucosal colonization in autologous stem cell transplantation. Bone Marrow Transplant 2005; 35 (10): 997–1001. doi: 10.1038/sj.bmt.1704933.
60. Elad S, Cheng KKF, Lalla RV et al. MASCC/ISOO clinical practice guidelines for the management of mucositis secondary to cancer therapy. Cancer 2020; 126 (19): 4423–4431. doi: 10.1002/cncr.33100.
61. da Silva BM, Prosdócimo ML, Gasparini LR et al. Most used photobiomodulation dosimetry parameters to treat oral mucositis after preconditioning for hematopoietic stem cell transplantation: systematic review and meta-analysis. Support Care Cancer 2022; 30 (5): 3721–3732. doi: 10.1007/s00520-022-06817-w.
62. Riley P, Glenny AM, Worthington HV et al. Interventions for preventing oral mucositis in patients with cancer receiving treatment: cytokines and growth factors. Cochrane Database Syst Rev 2017; 11 (11): CD011990. doi: 10.1002/14651858.CD011990.pub2.
63. Malone FR, Leisenring WM, Storer BE et al. Prolonged anorexia and elevated plasma cytokine levels following myeloablative allogeneic hematopoietic cell transplant. Bone Marrow Transplant 2007; 40 (8): 765–772. doi: 10.1038/sj.bmt.1705816.
64. Iestra JA, Fibbe WE, Zwinderman AH et al. Body weight recovery, eating difficulties and compliance with dietary advice in the first year after stem cell transplantation: a prospective study. Bone Marrow Transplant 2002; 29 (5): 417–424. doi: 10.1038/sj.bmt.1703375.
65. Sheean PM, Freels SA, Helton WS et al. Adverse clinical consequences of hyperglycemia from total parenteral nutrition exposure during hematopoietic stem cell transplantation. Biol Blood Marrow Transplant 2006; 12 (6): 656–664. doi: 10.1016/j.bbmt.2006. 01.010.
66. Zama D, Gori D, Muratore E et al. Enteral versus parenteral nutrition as nutritional support after allogeneic hematopoietic stem cell transplantation: a systematic review and meta-analysis. Transplant Cell Ther 2021; 27 (2): 180.e1–180.e8. doi: 10.1016/j.jtct.2020.11.006.
67. Inden A, Tsukahara T, Tachibana E et al. Effect of early nutritional support on quality of life by EORTC QLQ-C30 in allogeneic hematopoietic stem cell transplantation. Blood Cell Ther 2022; 5 (4): 107–115. doi: 10.31547/bct-2022-007.
68. Morello E, Arena F, Malagola M et al. Malnutrition prevention after allogeneic Hematopoietic Stem Cell Transplantation (alloHSCT): a prospective explorative interventional study with an oral polymeric formulation enriched with transforming growth factor beta 2 (TGF-b2). Nutrients 2022; 14 (17): 3589. doi: 10.3390/nu14173589.
69. Baena-Gómez MA, Aguilar MJ, Mesa MD et al. Changes in antioxidant defense system using different lipid emulsions in parenteral nutrition in children after hematopoietic stem cell transplantation. Nutrients 2015; 7 (9): 7242–7255. doi: 10.3390/nu7095335.
70. Geng M, Sun Z. Beneficial effect of integrated nutritional interventions in patients with hematological diseases undergoing hematopoietic stem cell transplant. Acta Haematol 2025; 148 (4): 398–407. doi: 10.1159/000541154.
71. Aoyama T, Yoshitsugu K, Fukaya M et al. Benefit of reducing body weight loss with a nutritional support pathway in patients undergoing allogeneic hematopoietic stem cell transplantation. Med Sci Monit Basic Res 2019; 25 : 187–198. doi: 10.12659/MSMBR.917329.
72. Sauls R, Buro AW, Montgomery L et al. Nutritional status and body mass index before hematopoietic stem cell transplantation (HSCT) and associated outcomes: a rapid review. Support Care Cancer 2023; 32 (1): 50. doi: 10.1007/s00520-023-08238-9.
73. Bezděk K, Maňásek V. Parenterální výživa v onkologii. Onkologie 2021; 15 (1): 15–20. doi: 10.36290/xon.2021.003.
74. Wingard JR, Gastineau DA, Leather HL et al. Hematopoietic stem cell transplantation: a handbook for clinicians. 2015 [online]. Available from: https: //catalog.nlm.nih.gov/discovery/fulldisplay/alma9916467663406676/01 NLM_INST: 01NLM_INST.
75. Uderzo C, Rebora P, Marrocco E et al. Glutamine-enriched nutrition does not reduce mucosal morbidity or complications after stem-cell transplantation for childhood malignancies: a prospective randomized study. Transplantation 2011; 91 (12): 1321–1325. doi: 10.1097/TP.0b013e31821ab959.
76. Renegar KB, Kudsk KA, Dewitt RC et al. Impairment of mucosal immunity by parenteral nutrition: depressed nasotracheal influenza-specific secretory IgA levels and transport in parenterally fed mice. Ann Surg 2001; 233 (1): 134–138. doi: 10.1097/00000658-200101000-00019.
77. Seguy D, Duhamel A, Rejeb MB et al. Better outcome of patients undergoing enteral tube feeding after myeloablative conditioning for allogeneic stem cell transplantation. Transplantation 2012; 94 (3): 287–294. doi: 10.1097/TP.0b013e3182558f60.
78. Guièze R, Lemal R, Cabrespine A et al. Enteral versus parenteral nutritional support in allogeneic haematopoietic stem-cell transplantation. Clin Nutr 2014; 33 (3): 533–538. doi: 10.1016/j.clnu.2013.07.012.
79. Alsalamah S, Alramyan R, Alakel R et al. The outcome and complications of total parenteral nutrition in pediatric hematopoietic stem cell transplantation. Pediatr Transplant 2022; 26 (3): e14198. doi: 10.1111/petr.14198.
80. Yang L, Wu D, Dai J et al. Clinical impacts of total parenteral nutrition in hematopoietic stem cell transplantation patients with high nutritional risk. Front Nutr 2024; 11 : 1495640. doi: 10.3389/fnut.2024.1495640.
81. Sheean PM, Kilkus JM, Liu D et al. Incident hyperglycemia, parenteral nutrition administration and adverse outcomes in patients with myeloma admitted for initial auto-SCT. Bone Marrow Transplant 2013; 48 (8): 1117–1122. doi: 10.1038/bmt.2013.11.
82. Madill J, Hartman B, Resvick H et al. Medical and nutritional outcomes are similar among autologous transplant patients on enteral nutrition when compared to parenteral nutrition. A randomized pilot study. Eur J Haematol 2025; 115 (2): 117–124. doi: 10.1111/ejh.14428.
83. Chelaghma W, Loucif L, Bendahou M et al. Vegetables and fruit as a reservoir of b-lactam and colistin-resistant gram-negative bacteria: a review. Microorganisms 2021; 9 (12): 2534. doi: 10.3390/microorganisms9122534.
84. Trifilio S, Helenowski I, Giel M et al. Questioning the role of a neutropenic diet following hematopoetic stem cell transplantation. Biol Blood Marrow Transplant 2012; 18 (9): 1385–1390. doi: 10.1016/j.bbmt.2012. 02.015.
85. Habibi S, Ghoreishy SM, Imani H et al. The effect of Oral Nutrition Supplement (ONS) on the nutritional and clinical status of patients undergoing autologous hematopoietic stem cell transplantation: study protocol for a randomized controlled clinical trial. BMC Nutr 2024; 10 (1): 83. doi: 10.1186/s40795-024-00893-3.
Labels
Paediatric clinical oncology Surgery Clinical oncologyArticle was published in
Clinical Oncology

2025 Issue 5
Most read in this issue
- Monoclonal gammopathy of clinical significance – a group name for diseases caused by monoclonal immunoglobulin and/ or free light chains. A change in the approach to non-malignant gammopathies
- Changes in the approach to the analysis and evaluation of inherited pathogenic TP53 variants
- Nutrition of patients undergoing haematopoietic stem cell transplantation
- Precision medicine in hemato-oncology – treatment of refractory multiple myeloma with massive extramedullary involvement using BRAF/ MEK inhibitors