
Strategie léčby žlučových kamenů u dětí: systematický přehled
Authors:
I. Shahramian 1; A. Aminisefat 2; M. Tahani 2; F. Ziyaee 1; A. Mansouri 2; G. R. Sivandzadeh 3
Authors‘ workplace:
Department of Pediatric Gastroenterology, Shiraz University of Medical Sciences, Shiraz, Iran
1; Pediatric Digestive and Hepatic Diseases Research Center, Zabol University of Medical Sciences, Zabol, Iran
2; Gastroenterohepatology Research Center, Shiraz University of Medical Sciences, Shiraz, Iran
3
Published in:
Gastroent Hepatol 2025; 79(6): 458-464
Category:
Pediatric Gastroenterology and Hepatology: Case report
doi:
https://doi.org/10.48095/ccgh2025458
Overview
Úvod: Onemocnění žlučových kamenů u dětí představuje jedinečné výzvy v léčbě. Tato systematická revize analyzuje současné léčebné strategie u dětí do 18 let. Metody: Provedli jsme rešerši literatury (2015–2025) v databázích PubMed, EMBASE a Cochrane Library zaměřenou na studie zahrnující pediatrické pacienty se žlučovými kameny léčenými kyselinou ursodeoxycholovou (UDCA), laparoskopickou cholecystektomií (LC), endoskopickou retrográdní cholangiopankreatografií (ERCP) a laparoskopickou explorací společného žlučovodu (LCBDE). Výsledky: U 758 pediatrických případů z 10 studií vykazovala LC v kombinaci s ERCP vysokou účinnost a nízkou míru komplikací. LCBDE byla účinná, ale nesla s sebou potenciálně vyšší riziko komplikací. Léčba UDCA vykazovala omezený úspěch a časté recidivy. Celková míra chirurgických komplikací byla 4,7 %. Výsledky léčby byly ovlivněny faktory specifickými pro jednotlivé pacienty (např. základní onemocnění, stav hydratace a obezita) a odbornými znalostmi lékaře provádějícího zákrok. Závěry: LC v kombinaci s ERCP se jeví jako vysoce účinný zákrok u žlučových kamenů u dětí. LCBDE je schůdnou alternativou, i když může být spojena s větším rizikem komplikací. UDCA se na základě neoptimálních dlouhodobých výsledků nedoporučuje jako primární léčba. Pro zdokonalení léčby žlučových kamenů u dětí jsou nezbytné další rozsáhlé multicentrické studie.
Klíčová slova:
žlučové kameny – cholelitiáza – choledocholitiáza – léčba – management – dítě – kojenci
Background
Gallstone disease, encompassing cholecystitis, cholelithiasis, and biliary pancreatitis, is a common condition [1]. Gallstones form primarily in the gallbladder, and less frequently in the intrahepatic or extrahepatic bile ducts. While most children with cholelithiasis are asymptomatic [2], the reported prevalence of biliary sludge and gallstones in the pediatric population is 1.46% and 1.9%, respectively, with higher rates observed in children undergoing abdominal ultrasound for pain [3].
The prevalence of gallstones in children has increased in recent years [4,5], a trend attributed to rising childhood obesity [6,7], significant calorie restriction in adolescents [7], and more frequent cholecystectomy for biliary dyskinesia [8]. The incidence of complex biliary disease in children (i.e., gallstones, cholelithiasis, and pancreatitis) is now similar to that in adults [9], raising concerns about delays in presentation and the need for effective surgical and endoscopic management [10].
Management strategies for pediatric gallstones vary. Laparoscopic cholecystectomy (LC) is the standard of care for symptomatic and complicated gallstones. For choledocholithiasis, ductal clearance can be achieved via endoscopic retrograde cholangiopancreatography (ERCP) or laparoscopic common bile duct exploration (LCBDE) [11,12]. Due to limited information on pediatric-specific treatment modalities, adult approaches are often applied, making management in children and adolescents controversial. This study aimed to systematically analyze the management of pediatric gallstone disease.
Methods
A systematic literature search was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Search strategy
Two independent researchers searched PubMed, EMBASE, and the Cochrane Library for English-language publications from January 2015 to January 2025 (see the Supplementary Material for complete search strategies). Reference lists of included studies and relevant reviews were screened for additional eligible publications.
Eligibility criteria
Studies were included if they fulfilled the following criteria:
- original research articles (prospective or retrospective), case series, or cohort studies;
- involved pediatric patients with gallstone disease (aged ≤ 18 years);
- provided sufficient data on the management and treatment of the disease.
Exclusion criteria were:
- studies including only adult patients;
- failure to separately report pediatric data when both adult and pediatric patients were involved;
- abstracts, commentaries, editorials, or expert opinions without original data;
- reviews or meta-analyses (though their reference lists were examined); or
- duplicate or overlapping data.
For multiple studies from the same institution with overlapping cohorts, the study with the most detailed methodology, the largest sample size, or the most recent publication date was selected.
Study selection and data extraction
After removing duplicates, two investigators independently screened titles and abstracts. The full text of potentially relevant articles was reviewed against the eligibility criteria. Disagreements were resolved by consensus or consultation with a third researcher. Data on study characteristics, patient demographics, predisposing factors, treatment approaches, complications, and outcomes were extracted into a standardized form.
Quality assessment
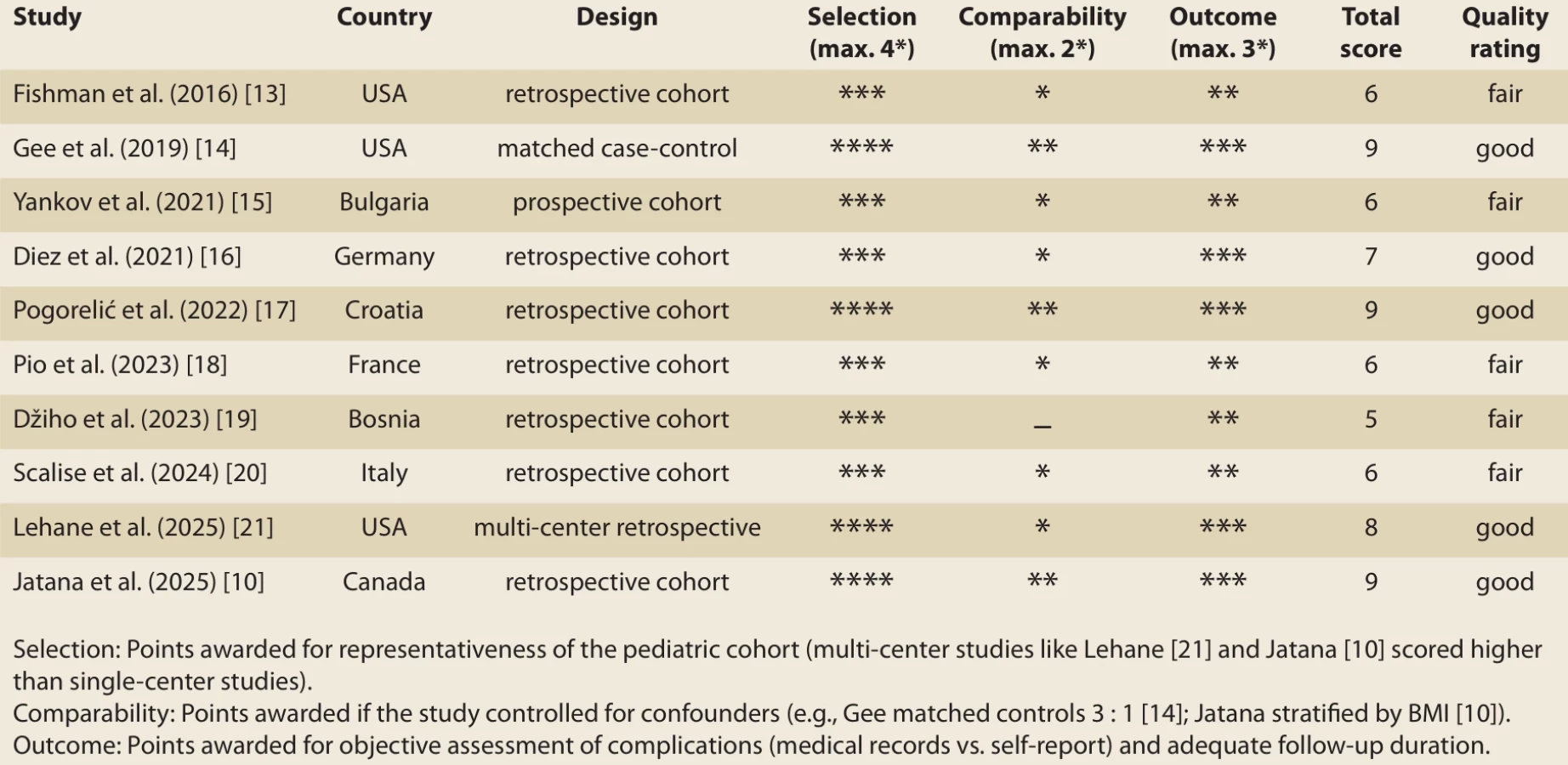
As the included studies were all non-randomized observational studies, the Newcastle-Ottawa Scale (NOS) was employed to assess methodological quality. Studies were scored across three domains: Selection (representativeness of the cohort), Comparability (control for confounding factors), and Outcome (assessment and follow-up). Studies scoring ≥ 7 stars were considered “Good” quality; 4–6 stars, “Fair”; and < 4 stars, “Poor” (Tab. 1).
Results
The PRISMA flow diagram (Scheme 1) outlines the study selection process. Ten studies [10,13–21] involving 758 pediatric patients were included.

Study characteristics
Characteristics of the included studies are summarized in Tab. 2. All but one study were retrospective. The median sample size was 45.5 (range: 32 to 210). The median age of participants across studies was 14 years (range: 1 month to 18 years). The female: male ratio was 2.4 : 1. For consistency in Tab. 2, where only the mean and standard deviation (SD) were reported, the mean was used to approximate the median, and the range was approximated as (mean – 3 × SD) to (mean + 3 × SD).

Clinical findings and predisposing factors
Pain, vomiting, fever, and jaundice were common clinical findings. More serious complications included choledocholithiasis (14.5%), acute cholecystitis (10.5%), and acute pancreatitis (6.0%). Predisposing factors are detailed in Tab. 3. Obesity was a major factor, with a prevalence of 70.0% in one study [10]. Other factors included hereditary spherocytosis, total parenteral nutrition, biliary malformations, and hematologic diseases. Yankov et al. [15] reported that UDCA was more successful in children with a history of dehydration and stones < 5 mm in diameter.

Treatment approaches
Management strategies varied across studies (Scheme 2). LC was the most common procedure. LC combined with ERCP was highly successful; Gee et al. [14] reported it as an optimal method that reduced costs without increasing anesthesia time. Pogorelić et al. [17] reported a 71.4% success rate for stone extraction via LCBDE using a Dormia basket, with laser fragmentation required in the remaining cases. UDCA treatment resulted in complete gallstone dissolution in 31.4% of patients in one study [15] and 21% in another [16].

Complications
The overall complication rate was 4.7% (36/758). Complications included bile leak, postoperative choledocholithiasis, surgical site infection, and pancreatitis [10,13,17,20]. Scalise et al. [20] reported an 18.75% rate of intraoperative complications, primarily adhesions.
Discussion
This study demonstrates that both the single-stage LCBDE and the two-stage LC with pre - or post-operative ERCP (LC + ERCP) are effective and safe for managing choledocholithiasis. Our analysis revealed no statistically significant differences in the primary success rate or overall morbidity between the two approaches. However, the single-stage LCBDE strategy was associated with a significantly shorter post-operative hospital stay, consistent with the advantage of resolving both cystic and calculous disease in a single intervention.
Comparable success rates in clearing the common bile duct (CBD) support LCBDE’s viability as a first-line therapeutic option. This aligns with current literature suggesting that, when expertise is available, LCBDE can achieve ductal clearance rates equivalent to the established ERCP-based approach [18, 19]. The primary advantage of the single-stage strategy is its efficiency in resource utilization, as evidenced by the reduced length of hospital stay. This can be attributed to eliminating the need for a separate procedure and its associated care, potentially lowering hospital costs and reducing patient inconvenience [12,22]. Furthermore, LCBDE preserves the function of the sphincter of Oddi, which may theoretically confer a long-term benefit by reducing the risk of recurrent bile duct stones and other sequelae associated with sphincterotomy, such as duodenobiliary reflux [23,24].
In contrast, the two-stage LC + ERCP approach remains a highly reliable and widely available strategy. Its principal strength lies in utilizing two highly specialized teams, allowing for a focused approach to the gallbladder and the bile duct separately. This can be particularly advantageous where advanced laparoscopic biliary surgery skills are unavailable or in cases of complex biliary anatomy. However, this strategy carries a risk of failure in the procedural sequence, such as retained stones following LC or unsuccessful ERCP cannulation, which can complicate the clinical pathway [25]. Additionally, ERCP is invasive and has its own specific complication profile, most notably post-ERCP pancreatitis, bleeding, and perforation [26].
Research indicates that UDCA does not alleviate symptoms in symptomatic gallstone disease and is therefore not recommended [27]. This is supported by evidence of poor long-term efficacy. For instance, a study of 180 Italian children with gallstones found that while UDCA led to stone dissolution in eight patients, three of them experienced a recurrence [28]. Although UDCA can be effective for small, non-calcified stones, the high recurrence rate leads to the consensus that it is not recommended for treating asymptomatic gallstones [12].
Limitations and future research
This review has several limitations. The included studies were predominantly retrospective and heterogeneous in their reporting, precluding a meta-analysis. The small sample sizes of some studies may limit the generalizability of the findings. Furthermore, the influence of surgeon and endoscopist experience on outcomes, though likely significant, could not be quantified. Finally, most studies lacked long-term follow-up to assess differences in late complications, such as stone recurrence or stenosis related to biliary-enteric dynamics after sphincterotomy [27,29]. Future research would benefit from larger, multi-institutional prospective studies or randomized controlled trials that incorporate long-term follow-up and detailed cost-effectiveness analyses. Such studies could more definitively stratify patients based on specific criteria, such as stone size, number, and CBD diameter, to determine the optimal management strategy for individual patient profiles [30,31].
Conclusion
This systematic review suggests that LC + ERCP is the preferred treatment method for pediatric gallstone disease, with high success and minimal complications. LCBDE is a successful single-stage alternative, but it may have a different complication profile. UDCA shows low treatment success and significant recurrence and is not advised as the primary therapy. Evidence indicates that factors such as underlying disease, dehydration, patient weight, and operator experience significantly influence treatment outcomes.
Sources
1. Ahmed AS, Ahmed SS, Mohamed S et al. Advancements in cholelithiasis diagnosis: a systematic review of machine learning applications in imaging analysis. Cureus 2024; 16 (8): e66453. doi: 10.7759/cureus.66453.
2. Zdanowicz K, Daniluk J, Lebensztejn DM et al. The etiology of cholelithiasis in children and adolescents – a literature review. Int J Mol Sci 2022; 23 (21): 13376. doi: 10.3390/ijms232113376.
3. Franklin AL, Qureshi FG, Nadler EP. Management of gallstones in the pediatric patient. Cham: Springer International Publishing 2015 : 197–206.
4. Pogorelic Z, Aralica M, Jukic M et al. Gallbladder disease in children: a 20-year single-center experience. Indian Pediatr 2019; 56 (5): 384–386.
5. Rothstein DH, Harmon CM. Gallbladder disease in children. Semin Pediatr Surg 2016; 25 (4): 225–231. doi: 10.1053/j.sempedsurg. 2016.05.005.
6. Fradin K, Racine AD, Belamarich PF. Obesity and symptomatic cholelithiasis in childhood: epidemiologic and case‐control evidence for a strong relation. J Pediatr Gastroenterol Nutr 2014; 58 (1): 102–106. doi: 10.1097/MPG. 0b013e3182a939cf.
7. Lacher M, Yannam GR, Muensterer OJ et al. Laparoscopic cholecystectomy for biliary dyskinesia in children: frequency increasing. J Pediatr Surg 2013; 48 (8): 1716–1721. doi: 10.1016/ j.jpedsurg.2012.08.036.
8. Orłowska A, Socha P, Szychta M et al. Management of gallstone disease in children. Polish J Paediatr 2023; 98 (3): 229–235. doi: 10.5114/polp.2023.131761.
9. Doud A, Bond L, Downard C et al. Management of complicated biliary disease in the pediatric population. Surgery 2022; 171 (3): 736–740. doi: 10.1016/j.surg.2021.09.041.
10. Jatana S, Sizov A, Jogiat U et al. Pediatric gallstone disease, postoperative outcomes, and endoscopic management: a single centre 5-year experience. Paediatr Child Health 2025; 22: pxaf051. doi: 10.1093/pch/pxaf051.
11. Gomez MK, Bosley ME. Endoscopic and surgical approaches in the management of pediatric gallstone disease: a review of associated complications. Semin Pediatr Surg 2025; 34 : 151497. doi: 10.1016/j.sempedsurg.2025. 151497.
12. European Association for the Study Of the Liver. EASL Clinical Practice Guidelines on the prevention, diagnosis and treatment of gallstones. J Hepatol 2016; 65 (1): 146–181. doi: 10.1016/j.jhep.2016.03.005.
13. Fishman DS, Chumpitazi BP, Raijman I et al. Endoscopic retrograde cholangiography for pediatric choledocholithiasis: assessing the need for endoscopic intervention. World J Gastrointest Endosc 2016; 8 (11): 425–432. doi: 10.4253/wjge.v8.i11.425.
14. Gee KM, Jones RE, Casson C et al. More is less: the advantages of performing concurrent laparoscopic cholecystectomy and endoscopic retrograde cholangiopancreatography for pediatric choledocholithiasis. J Laparoendosc Adv Surg Tech A 2019; 29 (11): 1481–1485. doi: 10.1089/lap.2019.0429.
15. Yankov I. Usefulness of ursodeoxycholic acid in management of gallstone disease in children. Central Eur J Paediatr 2022; 18 (1): 11–17. doi: 10.5457/p2005-114.310.
16. Diez S, Müller H, Weiss C et al. Cholelithiasis and cholecystitis in children and adolescents: does this increasing diagnosis require a common guideline for pediatricians and pediatric surgeons? BMC Gastroenterol 2021; 21 (1): 186. doi: 10.1186/s12876-021-01772-y.
17. Pogorelić Z, Lovrić M, Jukić M et al. The laparoscopic cholecystectomy and common bile duct exploration: a single-step treatment of pediatric cholelithiasis and choledocholithiasis. Children 2022; 9 (10): 1583. doi: 10.3390/children9101583.
18. Pio L, Tulelli B, Ali L et al. Enhanced recovery after surgery applied to pediatric laparoscopic cholecystectomy for simple cholelithiasis: feasibility and teaching insights. Children 2023; 10 (12): 1881. doi: 10.3390/children10121881.
19. Džiho N, Karavdić K. Pediatric cholelithiasis single center experience results of the clinic for pediatric surgery kcu Sarajevo in period 2010–2022. J Clin Surg Res 2023; 4 (3): 2768–2757. doi: 10.31579/2768-2757/081.
20. Scalise D, Boscarelli A, Giangreco M et al. Management of childhood cholelithiasis: experience at a third-level pediatric surgical center. Spinger Science and Business Media LLC 2024.
21. Lehane A, Rauh JL, Dantes G et al. Endoscopic Retrograde Cholangiopancreatography (ERCP) findings in pediatric patients with choledocholithiasis justify a surgery-first approach: a multicenter study. J Pediatr Surg 2025; 60 (8): 162388. doi: 10.1016/j.jpedsurg.2025.162388.
22. Doud A, Bond L, Downard C et al. Management of complicated biliary disease in the pediatric population. Surgery 2022; 171 (3): 736–740. doi: 10.1016/j.surg.2021.09.041.
23. Xu ZR, Dan HL, Yu F. Risk factors, manifestations, diagnosis and treatment of cholelithiasis in children. World J Metaanal 2021; 9 (1): 54–63. doi: 10.13105/wjma.v9.i1.54.
24. Wong MC, Incerti F, Avanzini S et al. Cholelithiasis management in a third-level pediatric center: case series and literature review. Updates Surg 2022; 74 (3): 963–968. doi: 10.1007/s13304-021-01227-9.
25. Liu Y, Jin S, Li Y et al. Treatment of asymptomatic gallstones in children with hereditary spherocytosis requiring splenectomy. J Pediatr Surg 2023; 58 (4): 756–761. doi: 10.1016/j.jpedsurg.2022.11.012.
26. Gomez MK, Bosley ME. Endoscopic and surgical approaches in the management of pediatric gallstone disease: a review of associated complications. Semin Pediatr Surg 2025; 34 : 151497. doi: 10.1016/j.sempedsurg.2025.151497.
27. Wilder RT, Flick RP, Sprung J et al. Early exposure to anesthesia and learning disabilities in a population-based birth cohort. Anesthesiology 2009; 110 (4): 796–804. doi: 10.1097/01.anes.0000344728.34332.5d.
28. Della Corte C, Falchetti D, Nebbia G et al. Management of cholelithiasis in Italian children: a national multicenter study. World J Gastroenterol 2008; 14 (9): 1383–1388. doi: 10.3748/wjg.14.1383.
29. Miglioretti DL, Johnson E, Williams A et al. The use of computed tomography in pediatrics and the associated radiation exposure and estimated cancer risk. JAMA Pediatr 2013; 167 (8): 700–707. doi: 10.1001/jamapediatrics. 2013.311.
30. Rauh JL, Wood EC, Dantes G et al. Patient safety and radiation exposure in transcystic laparoscopic common bile duct exploration: A CARES working group multicenter study. J Pediatr Surg 2024; 59 (12): 161669. doi: 10.1016/j.jpedsurg.2024.08.009.
31. Venneman NG, Besselink MG, Keulemans YC et al. Ursodeoxycholic acid exerts no beneficial effect in patients with symptomatic gallstones awaiting cholecystectomy. Hepatology 2006; 43 (6): 1276–1283. doi: 10.1002/hep.21182.
Labels
Paediatric gastroenterology Gastroenterology and hepatology SurgeryArticle was published in
Gastroenterology and Hepatology

2025 Issue 6
Most read in this issue
- Swallowing disorder as the first symptom of desminopathy
- Multimodal opioid-sparing total intravenous anesthesia in bariatric surgery – initial experience
- Eosinophilic esophagitis in pediatric patients – current findings and experience from clinical practice
- Treatment strategies for pediatric gallstone disease: a systematic review